Short-Term Effects of Carbonaceous Components in PM2.5 on Pulmonary Function: A Panel Study of 37 Chinese Healthy Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Design
2.2. Measurement
2.2.1. Lung Function Measurement
2.2.2. Environmental Measurement
2.2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics of Participants, Pollutants, and Meteorology Variables
3.2. Correlation Matrix between Indoor/Outdoor Pollutants
3.3. Estimated Effects of Carbonaceous Components on Lung Function
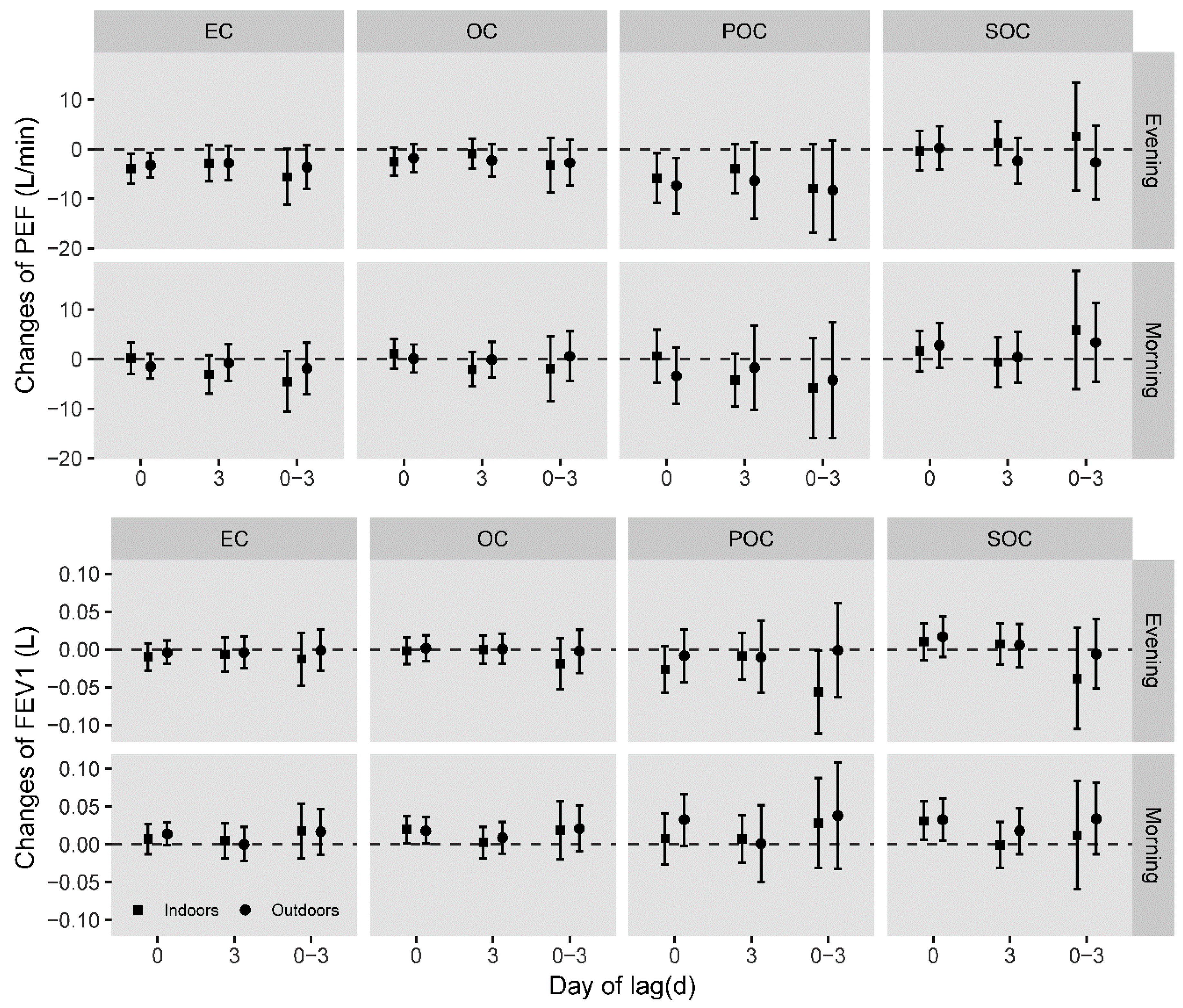
3.3.1. Global Analysis of Health Effects of Carbonaceous Components
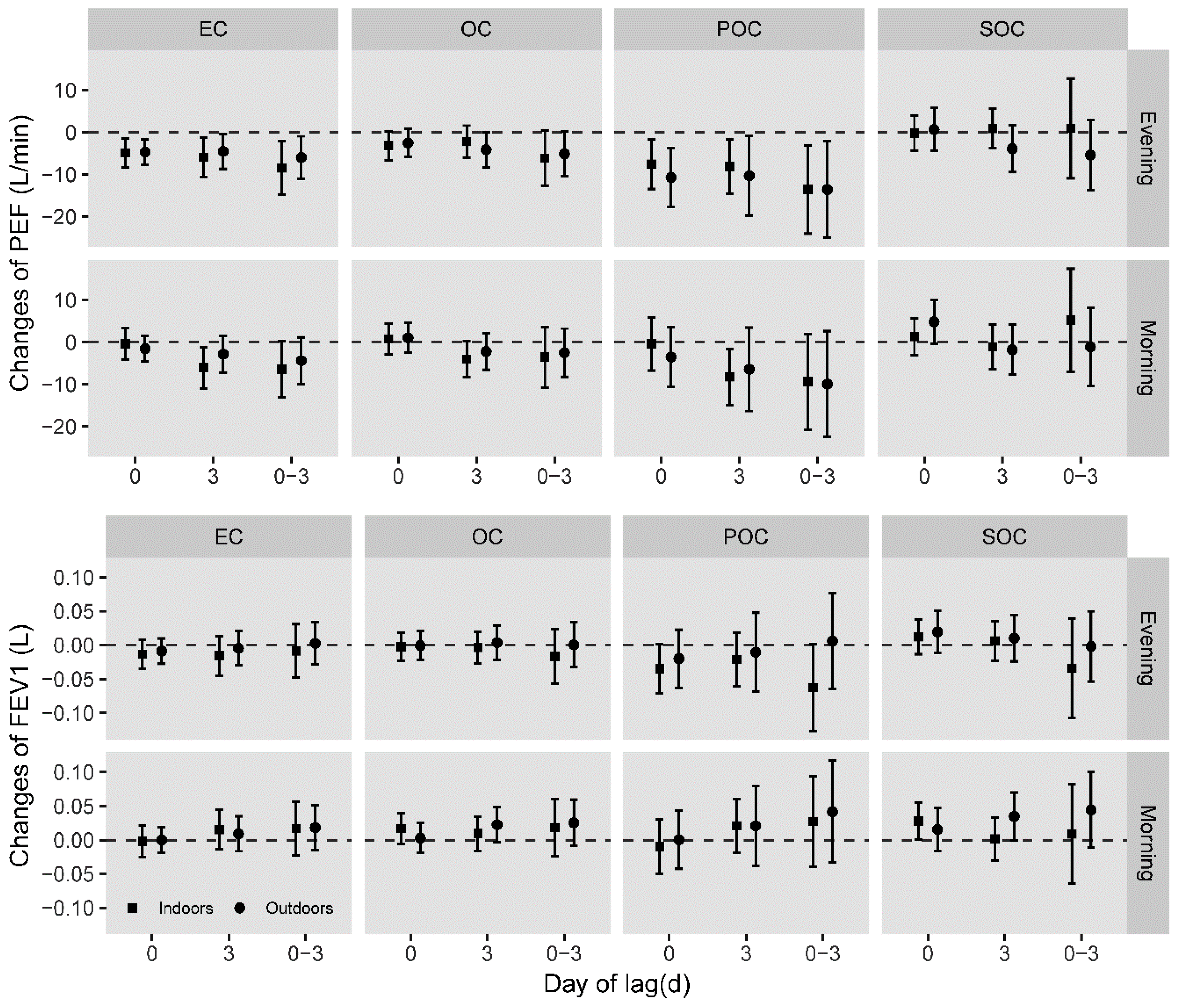
3.3.2. Seasonal Analysis of Health Effects of Carbonaceous Components
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dockery, D.W.; Stone, P.H. Cardiovascular risks from fine particulate air pollution. N. Engl. J. Med. 2007, 356, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Ren, M.; Fang, X.; Li, M.; Sun, S.; Pei, L.; Xu, Q.; Ye, X.; Cao, Y. Concentration-Response Relationship between PM2.5 and Daily Respiratory Deaths in China: A Systematic Review and Metaregression Analysis of Time-Series Studies. Biomed. Res. Int. 2017, 2017, 5806185. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Liu, Q.; Deng, F.; Wang, X.; Lin, H.; Guo, X.; Wu, S. Association between particulate matter air pollution and risk of depression and suicide: Systematic review and meta-analysis. Br. J. Psychiatry 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D. Evaluating the effects of ambient air pollution on life expectancy. N. Engl. J. Med. 2009, 360, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Ye, B.; Feng, H.; Ren, F.; Huang, S.; Zhang, X.; Zhang, Y.; Du, Q.; Ma, L. Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016. Int. J. Environ. Res. Public Health 2017, 14, 1321. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Deng, F.; Hao, Y.; Wang, X.; Zheng, C.; Lv, H.; Lu, X.; Wei, H.; Huang, J.; Qin, Y.; et al. Fine particulate matter, temperature, and lung function in healthy adults: Findings from the HVNR study. Chemosphere 2014, 108, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Li, C.; Li, Y.; Liu, J.; Meng, C.; Han, J.; Zhang, Y.; Xu, D. Short-term effects of ambient air pollution exposure on lung function: A longitudinal study among healthy primary school children in China. Sci. Total Environ. 2018, 645, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Hulo, S.; Cherot-Kornobis, N.; Matran, R.; Amouyel, P.; Edme, J.L.; Giovannelli, J. Short-term exposure to air pollution: Associations with lung function and inflammatory markers in non-smoking, healthy adults. Environ. Int. 2018, 121, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.B.; Ljungman, P.L.; Wilker, E.H.; Dorans, K.S.; Gold, D.R.; Schwartz, J.; Koutrakis, P.; Washko, G.R.; O’Connor, G.T.; Mittleman, M.A. Long-term exposure to traffic emissions and fine particulate matter and lung function decline in the Framingham heart study. Am. J. Respir. Crit. Care Med. 2015, 191, 656–664. [Google Scholar] [CrossRef]
- Mu, L.; Deng, F.; Tian, L.; Li, Y.; Swanson, M.; Ying, J.; Browne, R.W.; Rittenhouse-Olson, K.; Zhang, J.J.; Zhang, Z.F.; et al. Peak expiratory flow, breath rate and blood pressure in adults with changes in particulate matter air pollution during the Beijing Olympics: A panel study. Environ. Res. 2014, 133, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Gu, Y.; Qiao, L.; Wang, C.; Song, Y.; Bai, C.; Sun, Y.; Ji, H.; Zhou, M.; Wang, H.; et al. Fine Particulate Constituents and Lung Dysfunction: A Time-Series Panel Study. Environ. Sci. Technol. 2017, 51, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- McCreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.K.; Ohman-Strickland, P.; et al. Respiratory effects of exposure to diesel traffic in persons with asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Dong, W.; Li, H.; Miller, M.R.; Chen, Y.; Loh, M.; Wu, S.; Xu, J.; Yang, X.; Shima, M.; et al. Association patterns for size-fractioned indoor particulate matter and black carbon and autonomic function differ between patients with chronic obstructive pulmonary disease and their healthy spouses. Environ. Pollut. 2018, 236, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Arhami, M.; Polidori, A.; Gillen, D.L.; George, S.C.; Shafer, M.M.; Schauer, J.J.; Sioutas, C. Associations of primary and secondary organic aerosols with airway and systemic inflammation in an elderly panel cohort. Epidemiology 2010, 21, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, J.; Vonwiller, M.; Liu, D.; Cheng, H.; Shen, K.; Salazar, G.; Agrios, K.; Zhang, Y.; He, Q.; et al. The importance of non-fossil sources in carbonaceous aerosols in a megacity of central China during the 2013 winter haze episode: A source apportionment constrained by radiocarbon and organic tracers. Atmos. Environ. 2016, 144, 60–68. [Google Scholar] [CrossRef]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Gillen, D.; Kleinman, M.T.; Sioutas, C.; Cooper, D. Personal and ambient air pollution exposures and lung function decrements in children with asthma. Environ. Health Perspect. 2008, 116, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.J.; Lee, S.C.; Chow, J.C.; Cheng, Y.; Ho, K.F.; Fung, K.; Liu, S.X.; Watson, J.G. Indoor/outdoor relationships for PM2.5 and associated carbonaceous pollutants at residential homes in Hong Kong—Case study. Indoor Air 2005, 15, 197–204. [Google Scholar] [CrossRef]
- Jansen, K.L.; Larson, T.V.; Koenig, J.Q.; Mar, T.F.; Fields, C.; Stewart, J.; Lippmann, M. Associations between health effects and particulate matter and black carbon in subjects with respiratory disease. Environ. Health Perspect. 2005, 113, 1741–1746. [Google Scholar] [CrossRef]
- Zhang, Y.; Mo, J.; Weschler, C.J. Reducing health risks from indoor exposures in rapidly developing urban China. Environ. Health Perspect. 2013, 121, 751–755. [Google Scholar] [CrossRef]
- Rivas, I.; Viana, M.; Moreno, T.; Bouso, L.; Pandolfi, M.; Alvarez-Pedrerol, M.; Forns, J.; Alastuey, A.; Sunyer, J.; Querol, X. Outdoor infiltration and indoor contribution of UFP and BC, OC, secondary inorganic ions and metals in PM2.5 in schools. Atmos. Environ. 2015, 106, 129–138. [Google Scholar] [CrossRef]
- Grady, S.T.; Koutrakis, P.; Hart, J.E.; Coull, B.A.; Schwartz, J.; Laden, F.; Zhang, J.J.; Gong, J.; Moy, M.L.; Garshick, E. Indoor black carbon of outdoor origin and oxidative stress biomarkers in patients with chronic obstructive pulmonary disease. Environ. Int. 2018, 115, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Soppa, V.J.; Schins, R.P.; Hennig, F.; Hellack, B.; Quass, U.; Kaminski, H.; Kuhlbusch, T.A.; Hoffmann, B.; Weinmayr, G. Respiratory effects of fine and ultrafine particles from indoor sources--a randomized sham-controlled exposure study of healthy volunteers. Int. J. Environ. Res. Public Health 2014, 11, 6871–6889. [Google Scholar] [CrossRef] [PubMed]
- Rohr, A.C. The health significance of gas- and particle-phase terpene oxidation products: A review. Environ. Int. 2013, 60, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; He, M.; Wu, S.; Zhu, Y.; Wang, S.; Shima, M.; Tamura, K.; Ma, L. Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China. Int. J. Environ. Res. Public Health 2015, 12, 7777–7793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319. [Google Scholar] [CrossRef]
- Castro, L.M.; Pio, C.A.; Harrison, R.M.; Smith, D. Carbonaceous aerosol in urban and rural European atmospheres: Estimation of secondary organic carbon concentrations. Atmos. Environ. 1999, 33, 2771–2781. [Google Scholar] [CrossRef]
- Feng, Y.; Chen, Y.; Guo, H.; Zhi, G.; Xiong, S.; Li, J.; Sheng, G.; Fu, J. Characteristics of organic and elemental carbon in PM2.5 samples in Shanghai, China. Atmos. Res. 2009, 92, 434–442. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Hao, Y.; Shima, M.; Wang, X.; Zheng, C.; Wei, H.; Lv, H.; Lu, X.; Huang, J.; et al. Chemical constituents of fine particulate air pollution and pulmonary function in healthy adults: The Healthy Volunteer Natural Relocation study. J. Hazard. Mater. 2013, 260, 183–191. [Google Scholar] [CrossRef]
- Ho, K.F.; Cao, J.J.; Harrison, R.M.; Lee, S.C.; Bau, K.K. Indoor/outdoor relationships of organic carbon (OC) and elemental carbon (EC) in PM2.5 in roadside environment of Hong Kong. Atmos. Environ. 2004, 38, 6327–6335. [Google Scholar] [CrossRef]
- Ji, D.; Zhang, J.; He, J.; Wang, X.; Pang, B.; Liu, Z.; Wang, L.; Wang, Y. Characteristics of atmospheric organic and elemental carbon aerosols in urban Beijing, China. Atmos. Environ. 2016, 125, 293–306. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Wang, X.; Wei, H.; Shima, M.; Huang, J.; Lv, H.; Hao, Y.; Zheng, C.; Qin, Y.; et al. Association of lung function in a panel of young healthy adults with various chemical components of ambient fine particulate air pollution in Beijing, China. Atmos. Environ. 2013, 77, 873–884. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Oberdorster, G.; Oberdorster, E.; Oberdorster, J. Nanotoxicology: An emerging discipline evolving from studies of ultrafine particles. Environ. Health Perspect. 2005, 113, 823–839. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, W.; Fierens, F.; Trimpeneers, E.; Janssen, S.; Van de Vel, K.; Deutsch, F.; Viaene, P.; Vankerkom, J.; Dumont, G.; Vanpoucke, C.; et al. Modeling the effects of a speed limit reduction on traffic-related elemental carbon (EC) concentrations and population exposure to EC. Atmos. Environ. 2011, 45, 197–207. [Google Scholar] [CrossRef]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Gillen, D.L.; Polidori, A.; Arhami, M.; Kleinman, M.T.; Vaziri, N.D.; Longhurst, J.; Sioutas, C. Air Pollution Exposures and Circulating Biomarkers of Effect in a Susceptible Population: Clues to Potential Causal Component Mixtures and Mechanisms. Environ. Health Perspect. 2009, 117, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Tjoa, T.; Gillen, D.L.; Staimer, N.; Polidori, A.; Arhami, M.; Jamner, L.; Sioutas, C.; Longhurst, J. Traffic-related air pollution and blood pressure in elderly subjects with coronary artery disease. Epidemiology 2010, 21, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Spengler, C.M.; Shea, S.A. Endogenous circadian rhythm of pulmonary function in healthy humans. Am. J. Respir. Crit. Care Med. 2000, 162, 1038–1046. [Google Scholar] [CrossRef]
- Strak, M.; Boogaard, H.; Meliefste, K.; Oldenwening, M.; Zuurbier, M.; Brunekreef, B.; Hoek, G. Respiratory health effects of ultrafine and fine particle exposure in cyclists. Occup. Environ. Med. 2010, 67, 118–124. [Google Scholar] [CrossRef]
- Giles, L.V.; Brandenburg, J.P.; Carlsten, C.; Koehle, M.S. Physiological responses to diesel exhaust exposure are modified by cycling intensity. Med. Sci. Sports Exerc. 2014, 46, 1999–2006. [Google Scholar] [CrossRef]
- Tainio, M.; de Nazelle, A.J.; Gotschi, T.; Kahlmeier, S.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; de Sa, T.H.; Kelly, P.; Woodcock, J. Can air pollution negate the health benefits of cycling and walking? Prev. Med. 2016, 87, 233–236. [Google Scholar] [CrossRef] [Green Version]
- Kelly, P.; Kahlmeier, S.; Gotschi, T.; Orsini, N.; Richards, J.; Roberts, N.; Scarborough, P.; Foster, C. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 132. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450–451, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Lin, H.M.; Stewart, W.F.; Kong, L.; Xu, F.; Zhou, D.; Zhu, Z.; Liang, S.; Chen, W.; Shah, N.; et al. Seasonal pattern of the acute mortality effects of air pollution. J. Air Waste Manag. Assoc. 2010, 60, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.A.; Yin, F.; Song, Y.; Ming-Quan, H.E.; Masayuki, S.; Kenji, T. Indoor and Outdoor Pollutant Characteristics of Particulate Matter and OC, EC in Autumn and Winter in Wuhan. Urban Environ. Urban Ecol. 2011, 24, 25–28. [Google Scholar]
- Liu, D.; Deng, Q.; Zhou, Z.; Lin, Y.; Tao, J. Variation Trends of Fine Particulate Matter Concentration in Wuhan City from 2013 to 2017. Int. J. Environ. Res. Public Health 2018, 15, 1847. [Google Scholar] [CrossRef] [PubMed]
- Johan, D.H.J.; Boogaard, H.; Nijland, H.; Hoek, G. Do the health benefits of cycling outweigh the risks? Environ. Health Perspect. 2010, 118, 1109–1116. [Google Scholar]
- Kubesch, N.J.; de Nazelle, A.; Westerdahl, D.; Martinez, D.; Carrasco-Turigas, G.; Bouso, L.; Guerra, S.; Nieuwenhuijsen, M.J. Respiratory and inflammatory responses to short-term exposure to traffic-related air pollution with and without moderate physical activity. Occup. Environ. Med. 2015, 72, 284–293. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | All Subjects (n = 37) | Male (n = 18) | Female (n = 19) |
|---|---|---|---|
| Age, years | 20.70 ± 0.80 | 21.00 ± 0.90 | 20.50 ± 0.60 |
| Height, cm | 164.95 ± 8.16 | 171.67 ± 5.87 | 158.58 ± 3.67 |
| Weight, kg | 54.7 ± 7.0 | 59.1 ± 5.62 | 50.6 ± 5.61 |
| Body mass index, kg/m2 | 20.08 ± 1.84 | 20.03 ± 1.51 | 20.13 ± 2.1 |
| N | Mean | SD | Min | P25 | Median | P75 | Max | |
|---|---|---|---|---|---|---|---|---|
| Pulmonary function | ||||||||
| Morning FEV1 (L) | 1646 | 2.99 | 0.78 | 1.22 | 2.44 | 2.85 | 3.49 | 5.14 |
| Evening FEV1 (L) | 1682 | 2.99 | 0.77 | 1.01 | 2.44 | 2.84 | 3.42 | 5.24 |
| Morning PEF (L/min) | 1758 | 474.70 | 128.13 | 226.00 | 367.00 | 447.00 | 561.00 | 894.00 |
| Evening PEF (L/min) | 1780 | 476.70 | 125.15 | 250.00 | 374.00 | 445.00 | 562.00 | 838.00 |
| Pollutant & meteorology | ||||||||
| Indoor | ||||||||
| PM2.5 (μg/m3) | 54 | 80.47 | 39.93 | 23.07 | 48.46 | 65.40 | 107.52 | 189.42 |
| OC (μg/m3) | 54 | 14.11 | 10.24 | 1.35 | 7.25 | 9.75 | 18.30 | 42.43 |
| EC (μg/m3) | 54 | 10.88 | 8.65 | 1.12 | 5.81 | 8.05 | 12.98 | 55.37 |
| SOC (μg/m3) | 54 | 5.92 | 5.86 | 0.48 | 2.34 | 3.77 | 7.27 | 32.73 |
| POC (μg/m3) | 54 | 7.97 | 6.34 | 0.82 | 4.26 | 5.90 | 9.51 | 40.58 |
| Temperature (°C) | 54 | 20.85 | 8.31 | 9.18 | 13.38 | 18.43 | 29.99 | 37.18 |
| Humidity (%) | 54 | 61.45 | 9.20 | 36.28 | 55.71 | 62.80 | 67.60 | 77.89 |
| Outdoor | ||||||||
| PM2.5 (μg/m3) | 54 | 96.77 | 49.10 | 29.06 | 59.21 | 80.48 | 125.67 | 228.91 |
| OC (μg/m3) | 54 | 14.74 | 11.55 | 1.34 | 6.70 | 10.42 | 20.56 | 52.01 |
| EC (μg/m3) | 54 | 12.54 | 10.79 | 1.10 | 6.11 | 8.78 | 15.40 | 69.00 |
| SOC (μg/m3) | 54 | 8.92 | 7.73 | 0.58 | 3.63 | 5.79 | 12.87 | 33.27 |
| POC (μg/m3) | 54 | 5.50 | 4.73 | 0.48 | 2.68 | 3.85 | 6.75 | 30.25 |
| Temperature (°C) | 54 | 18.90 | 9.55 | 4.97 | 10.47 | 16.37 | 29.66 | 36.13 |
| Humidity (%) | 54 | 62.27 | 10.71 | 39.63 | 55.32 | 63.28 | 70.31 | 83.76 |
| Components | Lag | β (95%CI) | ||||
|---|---|---|---|---|---|---|
| Overall | Spring | Summer | Autumn | Winter | ||
| OC | ||||||
| 0 | −3.15 (−6.59, 0.30) | −20.43 (−68.89, 28.04) | −18.77 (−76.7, 39.17) | −1.25 (−16.47, 13.97) | −16.78 (−32.16, −1.40) * | |
| 3 | −2.21 (−6.00, 1.58) | −2.21 (−188.26, 119.55) | 4.54(−54.67, 63.75) | −10.46 (−31.69, 10.78) | −16.36 (−96.91, 64.20) | |
| 0-3 | −6.14 (−12.63, 0.35) | −37.62 (−245.38, 170.14) | −48.39 (−184.19, 87.42) | 15.45 (−61.85, 92.75) | −98.02 (−216.65, −20.60) * | |
| EC | ||||||
| 0 | −4.88 (−8.34, −1.42) * | −23.08 (−78.72, 32.55) | −93.39 (−166.93, −19.85) * | −6.41 (−15.63, 2.81) | −3.08 (−12.14, 5.97) | |
| 3 | −5.95 (−10.66, −1.23) * | −156.25 (−527.36, 214.86) | −13.22 (−90.22, 63.79) | −2.88 (−11.27, 5.50) | 16.69 (−34.68, 68.05) | |
| 0-3 | −8.47 (−14.83, −2.11) * | −160.30 (−679.83, 359.23) | −87.54 (−255.52, 80.44) | −24.26 (−60.82, 12.30) | −53.01 (−250.37, 144.34) | |
| SOC | ||||||
| 0 | −0.19 (−4.36, 3.98) | −43.15 (−159.15, 72.84) | 36.67 (−36.00, 109.33) | 5.86 (−4.99, 16.71) | −18.95 (−50.54, 12.65) | |
| 3 | 0.90 (−3.78, 5.58) | −23.05 (−215.99, 169.90) | 14.63 (−68.14, 97.40) | 1.76 (−14.21, 17.73) | −13.93 (−58.04, 30.18) | |
| 0-3 | 0.94 (−10.91, 12.80) | −27.74 (−318.44, 262.97) | −29.08 (−316.27, 258.10) | 44.52 (−8.25, 97.28) | −112.76 (−257.20, 31.68) | |
| POC | ||||||
| 0 | −7.56 (−13.43, −1.69) * | −31.51 (−107.45, 44.43) | −127.43 (−227.77, −27.09) * | −8.75 (−21.33, 3.83) | −13.51 (−29.50, 2.48) | |
| 3 | −8.11 (−14.55, −1.67) * | −213.20 (−719.60, 293.19) | −18.06 (−123.30, 87.19) | −3.94 (−15.38, 7.51) | 22.77 (−47.31, 92.85) | |
| 0-3 | −13.56 (−24.02, −3.10) * | −218.73 (−927.63, 490.17) | −119.40 (−348.35, 109.55) | −33.11 (−82.99, 16.78) | −53.85 (−136.23, 28.53) | |
| Components | Lag | β (95%CI) | ||||
|---|---|---|---|---|---|---|
| Overall | Spring | Summer | Autumn | Winter | ||
| OC | ||||||
| 0 | −2.50 (−5.89, 0.90) | 16.42 (−34.70, 67.55) | −53.46 (−115.36, 8.43) | −13.12 (−87.38, 61.15) | −9.38 (−22.33, 3.57) | |
| 3 | −4.11 (−8.24, 0.02) | −0.55 (−57.01, 55.91) | 0.89 (−39.08, 40.85) | 4.02 (−30.04, 38.07) | −15.17 (−29.65, −0.69) * | |
| 0-3 | −5.09 (−10.42, 0.23) | 150.43 (−18.46, 319.32) | 177.62 (−28.14, 383.38) | −31.56 (−123.76, 60.65) | −35.86 (−69.12, −2.61) * | |
| EC | ||||||
| 0 | −4.69 (−7.72, 1.67) * | 35.18 (−32.10, 102.47) | −57.12 (−130.31, 16.08) | 1.81 (−12.74, 16.37) | −4.96 (−10.74, 1.57) | |
| 3 | −4.51 (−8.64, −0.38) * | −74.06 (−148.49, 0.36) | 15.22 (−40.73, 71.18) | 13.62 (−22.73, 49.97) | −9.78 (−19.63, 0.07) | |
| 0-3 | −5.95 (−10.98, −0.93) * | −10.42 (−172.92, 151.07) | 85.09 (−72.04, 242.22) | −13.00 (−83.35, 57.35) | −28.18 (−60.02, 3.65) | |
| SOC | ||||||
| 0 | 0.67 (−4.44, 5.77) | 10.90 (−50.61, 72.41) | −67.75 (−153.26, 17.76) | −3.89 (−29.05, 21.28) | −4.82 (−19.36, 9.71) | |
| 3 | −3.87 (−9.43, 1.70) | 26.81 (−42.23, 95.85) | −5.08 (−62.29, 52.14) | −2.56 (−51.92, 46.80) | −17.65 (−42.80, 7.5) | |
| 0-3 | −5.40 (−13.78, 3.00) | 285.81 (58.50, 513.13) * | 396.14 (−12.91, 805.20) | −87.18 (−271.56, 97.20) | −24.01 (−58.69, 10.67) | |
| POC | ||||||
| 0 | −10.69 (−17.60, −3.79) * | 80.19 (−73.29, 233.67) | −135.14 (−307.95, 37.68) | 4.14 (−29.05, 37.33) | −10.47 (−24.51, 3.58) | |
| 3 | −10.29 (−19.71, −0.87) * | −168.94 (−338.70, 0.81) | 34.63 (−92.88, 162.15) | 31.07 (−51.85, 113.99) | −22.31 (−44.78, 0.15) | |
| 0-3 | −13.58 (−25.04, −2.11) * | −23.66 (−393.03, 344.70) | 193.58 (−159.19, 546.36) | −29.66 (−190.14, 130.83) | −64.29 (−136.91, 8.32) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.; Feng, H.; Zuo, S.; Liao, J.; He, M.; Shima, M.; Tamura, K.; Li, Y.; Ma, L. Short-Term Effects of Carbonaceous Components in PM2.5 on Pulmonary Function: A Panel Study of 37 Chinese Healthy Adults. Int. J. Environ. Res. Public Health 2019, 16, 2259. https://doi.org/10.3390/ijerph16132259
Huang S, Feng H, Zuo S, Liao J, He M, Shima M, Tamura K, Li Y, Ma L. Short-Term Effects of Carbonaceous Components in PM2.5 on Pulmonary Function: A Panel Study of 37 Chinese Healthy Adults. International Journal of Environmental Research and Public Health. 2019; 16(13):2259. https://doi.org/10.3390/ijerph16132259
Chicago/Turabian StyleHuang, Shichun, Huan Feng, Shanshan Zuo, Jingling Liao, Mingquan He, Masayuki Shima, Kenji Tamura, Yang Li, and Lu Ma. 2019. "Short-Term Effects of Carbonaceous Components in PM2.5 on Pulmonary Function: A Panel Study of 37 Chinese Healthy Adults" International Journal of Environmental Research and Public Health 16, no. 13: 2259. https://doi.org/10.3390/ijerph16132259