Out-Of-Pocket Expenditures on Dental Care for Schoolchildren Aged 6 to 12 Years: A Cross-Sectional Estimate in a Less-Developed Country Setting

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
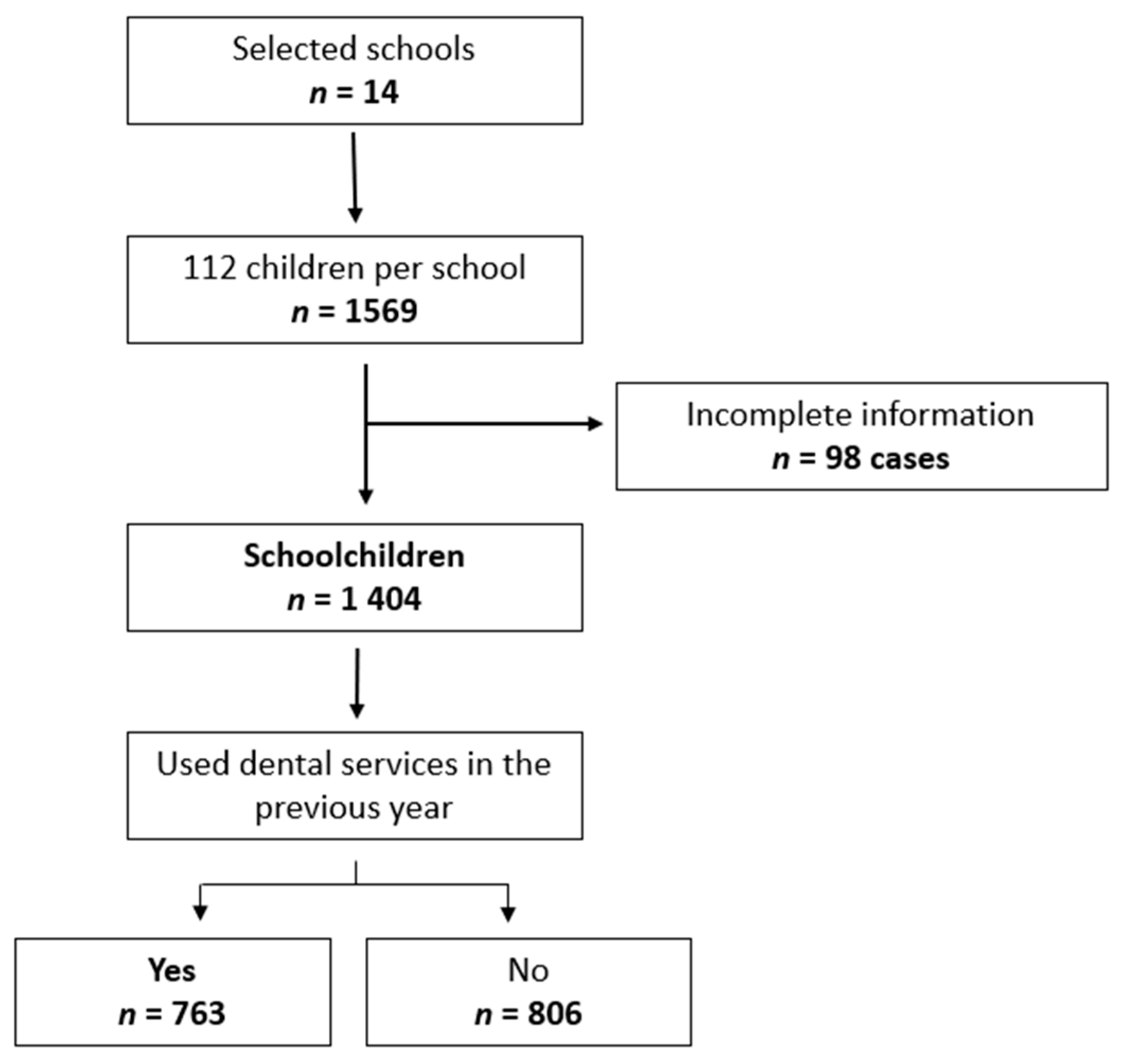
2.1. Design and Study Sample
2.2. Data Collection, Variables and Conformation Variables
2.3. Statistical Analysis
2.4. Ethical Considerations
2.5. Data Availability Statement
2.6. The Mexican Dental Health Care System
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Guizar, J.M.; Muñoz, N.; Amador, N.; Garcia, G. Association of Alimentary Factors and Nutritional Status with Caries in Children of Leon, Mexico. Oral. Health Prev. Dent. 2016, 14, 563–569. [Google Scholar] [CrossRef] [PubMed]
- López-Gómez, S.A.; Villalobos-Rodelo, J.J.; Ávila-Burgos, L.; Casanova-Rosado, J.F.; Vallejos-Sánchez, A.A.; Lucas-Rincón, S.E.; Patiño-Marín, N.; Medina-Solís, C.E. Relationship between premature loss of primary teeth with oral hygiene, consumption of soft drinks, dental care, and previous caries experience. Sci. Rep. 2016, 6, 21147. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, A.; Irigoyen-Camacho, M.E.; Borges-Yáñez, A. Fluorosis and dental caries in Mexican schoolchildren residing in areas with different water fluoride concentrations and receiving fluoridated salt. Caries Res. 2013, 47, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Taboada-Aranza, O.; Rodríguez-Nieto, K. Prevalence of plaque and dental decay in the first permanent molar in a school population of south Mexico City. Bol. Med. Hosp. Infant Mex. 2018, 75, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Secretaría de Salud. Encuesta Nacional de Caries 2001; Secretaría de Salud: Mexico City, Mexico, 2006.
- Guido, J.A.; Martinez-Mier, E.A.; Soto, A.; Eggertsson, H.; Sanders, B.J.; Jones, J.E.; Weddell, J.A.; Villanueva Cruz, I.; Anton de la Concha, J.L. Caries prevalence and its association with brushing habits, water availability, and the intake of sugared beverages. Int. J. Paediatr. Dent. 2011, 21, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Reisine, S.T. Theoretical considerations in formulating sociodental indicators. Soc. Sci. Med. A 1981, 15, 745–750. [Google Scholar] [CrossRef]
- Pérez-Núñez, R.; Medina-Solís, C.E.; Maupomé, G.; Vargas-Palacios, A. Factors associated with dental health care coverage in Mexico: Findings from the National Performance Evaluation Survey 2002–2003. Community Dent. Oral. Epidemiol. 2006, 34, 387–397. [Google Scholar] [CrossRef]
- Medina-Solís, C.E.; Casanova-Rosado, A.J.; Casanova-Rosado, J.F.; Vallejos-Sánchez, A.A.; Maupomé, G.; Ávila-Burgos, L. Socioeconomic and dental factors associated with the use of dental services in schoolchildren in Campeche, Mexico. Bol. Med. Hosp. Infant Mex. 2004, 61, 324–333. [Google Scholar]
- Medina-Solís, C.E.; Maupomé, G.; Ávila-Burgos, L.; Casanova-Rosado, J.F.; Vallejos-Sánchez, A.A.; Segovia-Villanueva, A. Use of dental health services for children under 5 years of age with social security. Rev. Mex. Pediatr. 2004, 71, 222–228. [Google Scholar]
- Medina-Solís, C.E.; Maupomé, G.; Ávila-Burgos, L.; Hijar-Medina, M.; Segovia-Villanueva, A.; Pérez-Núñez, R. Factors influencing the use of dental health services by preschool children in Mexico. Pediatr. Dent. 2006, 28, 285–592. [Google Scholar]
- Medina-Solís, C.E.; Villalobos-Rodelo, J.J.; Márquez-Corona, M.L.; Vallejos-Sánchez, A.A.; López-Portillo-Núñez, C.; Casanova-Rosado, A.J. Socioeconomic inequalities in the use of oral health services: Study in Mexican schoolchildren from 6 to 12 years of age. Cad. Saude Publica 2009, 25, 2621–2631. [Google Scholar] [CrossRef] [PubMed]
- Pontigo-Loyola, A.P.; Medina-Solís, C.E.; Márquez-Corona, M.L.; Vallejos-Sánchez, A.A.; Minaya-Sánchez, M.; Escoffié-Ramírez, M. Influence of predisposing, enabling, and health care need variables on the use of dental health services among Mexican adolescents from a semi-rural location. Gac. Med. Mex. 2012, 148, 218–226. [Google Scholar] [PubMed]
- Jiménez-Gayosso, S.I.; Medina-Solís, C.E.; Lara-Carrillo, E.; Scougal-Vilchis, R.J.; de la Rosa-Santillana, R.; Márquez-Rodríguez, S.; Mendoza-Rodríguez, M.; de Jesús Navarrete-Hernández, J. Socioeconomic inequalities in oral health service utilization any time in their lives for Mexican schoolchildren from 6 to 12 years old. Gac. Med. Mex. 2015, 151, 27–33. [Google Scholar] [PubMed]
- Comisión Nacional de Protección en Salud. Catálogo Universal de Servicios de Salud Causes 2016. Available online: http://www.documentos.seguro-popular.gob.mx/dgss/CAUSES2016.pdf (accessed on 2 April 2019).
- Gutiérrez, J.P.; Rivera-Dommarco, J.; Shamah-Levy, T.; Villalpando-Hernández, S.; Franco, A.; Cuevas-Nasu, L.; Romero-Martínez, M.; Hernández-Ávila, M. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. Instituto Nacional de Salud Pública (MX): Cuernavaca, México, 2012. Available online: https://ensanut.insp.mx/informes/ENSANUT2012ResultadosNacionales.pdf (accessed on 2 April 2019).
- Frenk, J.; Gómez Dantés, O. El sistema de Salud Mexicano; Editorial Nostra: Mexico City, Mexico, 2015. [Google Scholar]
- Ávila-Burgos, L.; Serván-Mori, E.; Wirtz, V.J.; Sosa-Rubí, S.G.; Salinas-Rodríguez, A. Efectos del Seguro Popular sobre el gasto en salud en hogares mexicanos a diez años de su implementación. Salud Publica Mex. 2013, 55 (Suppl. 2), S91–S99. [Google Scholar]
- Chemor-Ruiz, A.; Ochmann-Ratsch, A.E.; Alamilla-Martínez, G.A. Mexico’s Seguro Popular: Achievements and Challenges. Health Syst. Reform. 2018, 4, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Government of the Republic. Social Protection in Health System: Results Report January–December 2017; Government of the Republic: México City, México, 2018. Available online: http://www.transparencia.seguro-popular.gob.mx/contenidos/archivos/transparencia/planesprogramaseinformes/informes/2017/InformedeResultadosdelSPSSenero-diciembre2017.pdf (accessed on 25 November 2018).
- Sosa-Rubí, S.G.; Galárraga, O.; Harris, J.E. Heterogeneous impact of the “Seguro Popular” program on the utilization of obstetrical services in Mexico, 2001-2006: A multinomial probit model with a discrete endogenous variable. J. Health Econ. 2009, 28, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Escoffié-Ramirez, M.; Ávila-Burgos, L.; Baena-Santillan, E.S.; Aguilar-Ayala, F.; Lara-Carrillo, E.; Minaya-Sánchez, M.; Mendoza-Rodríguez, M.; de Lourdes Márquez-Corona, M.; Medina-Solís, C.E. Factors associated with dental pain in Mexican schoolchildren aged 6 to 12 years. Biomed. Res. Int. 2017, 2017, 7431301. [Google Scholar] [CrossRef]
- Medina-Solís, C.E.; Pontigo-Loyola, A.P.; Maupomé, G.; Lamadrid-Figueroa, H.; Loyola-Rodriguez, J.P.; Hernández-Romano, J.; Villalobos-Rodelo, J.J.; Márquez-Corona, M.L. Dental fluorosis prevalence and diagnostic test using Dean’s index based on 6 teeth, and on 28 teeth. Clin. Oral. Investig. 2008, 12, 197–202. [Google Scholar] [CrossRef] [PubMed]
- INSP. El Consumo de Azúcar en México y la Nueva Directriz de la OMS para su Reducción Global. Available online: https://www.insp.mx/epppo/blog/3609-consumo-azucar-mexico-nueva-directriz-oms.html (accessed on 2 April 2019).
- WHO. Chapter 1: Organization of a Basic Oral Health Survey. In Oral Health Survey—Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997; pp. 4–9. [Google Scholar]
- National Institute of Statistic and Geography (INEGI). Inflation Calculator. Available online: http://www.inegi.org.mx/sistemas/indiceprecios/CalculadoraInflacion.aspx (accessed on 25 November 2018).
- OECD. Data. Purchasing Power Parities. Available online: http://www.imf.org/external/np/fin/data/param_rms_mth.aspx (accessed on 9 September 2018).
- World Bank. Data. Purchasing Power Parities. Available online: https://datos.bancomundial.org/indicador/PA.NUS.PPP?view=map (accessed on 25 November 2018).
- Sun, G.W.; Shook, T.L.; Kay, G.L. Inappropriate use of bivariable analysis to screen risk factors for use in multivariable analysis. J. Clin. Epidemiol. 1996, 49, 907–916. [Google Scholar] [CrossRef]
- Bagley, S.C.; White, H.; Golomb, B.A. Logistic regression in the medical literature: Standards for use and reporting, with particular attention to one medical domain. J. Clin. Epidemiol. 2001, 54, 979–985. [Google Scholar] [CrossRef]
- Williams, R.L. A note on robust variance estimation for cluster-correlated data. Biometrics 2000, 56, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Barrera, M.Á.; Medina-Solís, C.E.; Casanova-Rosado, J.F.; Mendoza-Rodríguez, M.; Escoffié-Ramírez, M.; Casanova-Rosado, A.J.; de Jesús Navarrete-Hernández, J.; Maupomé, G. Contribution of prosthetic treatment considerations for dental extractions of permanent teeth. PeerJ 2016, 4, e2015. [Google Scholar] [CrossRef] [PubMed]
- Alkenbrack, S.; Lindelow, M. The impact of community-based health insurance on utilization and out-of-pocket expenditures in Lao People’s Democratic Republic. Health Econ. 2015, 24, 379–399. [Google Scholar] [CrossRef] [PubMed]
- Villalobos-Rodelo, J.J.; Medina-Solís, C.E.; Maupomé, G.; Vallejos-Sánchez, A.A.; Lau-Rojo, L.; de León-Viedas, M.V. Socioeconomic and sociodemographic variables associated with oral hygiene status in Mexican schoolchildren aged 6 to 12 years. J. Periodontol. 2007, 78, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Medina-Solís, C.E.; Galan-Vidal, C.A.; Navarrete-Hernández, J.J.; Escoffié-Ramirez, M.; Maupome, G. Salivary Parameters (Salivary Flow, pH and Buffering Capacity) in Stimulated Saliva of Mexican Elders 60 Years Old and Older. West Indian Med. J. 2014, 63, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Medina-Solís, C.E.; Maupomé, G.; Pelcastre-Villafuerte, B.; Avila-Burgos, L.; Vallejos-Sánchez, A.A.; Casanova-Rosado, A.J. Socioeconomic inequalities in oral health: Dental caries in 6 to 12 year-old children. Rev. Investig. Clin. 2006, 58, 296–304. [Google Scholar]
- Herrera, M.S.; Medina-Solís, C.E.; Robles-Bermeo, N.L.; Minaya-Sánchez, M.; Alonso-Sánchez, C.C.; Lara-Carrillo, E.; Mendoza-Rodríguez, M.; Bayardo-González, R.A. Consultation for dental extraction in Nicaraguan children: An approach to oral care needs. Pediatr 2017, 44, 239–244. [Google Scholar] [CrossRef]
- van der Tas, J.T.; Kragt, L.; Elfrink, M.E.C.; Bertens, L.C.M.; Jaddoe, V.W.V.; Moll, H.A.; Ongkosuwito, E.M.; Wolvius, E.B. Social inequalities and dental caries in six-year-old children from the Netherlands. J. Dent. 2017, 62, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.S. Social gradients in oral health status in Korea population. Arch. Oral. Biol. 2018, 95, 89–94. [Google Scholar] [CrossRef]
- Andrade, F.B.; Antunes, J.L.F.; Souza Junior, P.R.B.; Lima-Costa, M.F.; Oliveira, C. Life course socioeconomic inequalities and oral health status in later life: ELSI-Brazil. Rev. Saude Publica 2018, 52 (Suppl. 2), S7. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.M.; Martins, C.C.; Pinto, M.Q.C.; Vasconcelos, M.; Abreu, M.H.N.G. Socioeconomic factors and caries in people between 19 and 60 years of age: An update of a systematic review and meta-analysis of observational studies. Int. J. Environ. Res. Public Health 2018, 15, 1775. [Google Scholar] [CrossRef] [PubMed]
- Kailembo, A.; Preet, R.; Stewart-Williams, J. Socioeconomic inequality in self-reported unmet need for oral health services in adults aged 50 years and over in China, Ghana, and India. Int. J. Equity Health 2018, 17, 99. [Google Scholar] [CrossRef] [PubMed]
- Kailembo, A.; Quiñonez, C.; Lopez-Mitnik, G.V.; Weintraub, J.A.; Stewart-Williams, J.; Preet, R.; Iafolla, T.; Dye, B.A. Income and wealth as correlates. Of socioeconomic disparity in dentist visits among adults aged 20 years and over in the United States, 2011–2014. BMC Oral. Health. 2018, 18, 147. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Yang, B. Relationship between catastrophic health expenditures and household incomes and expenditure patterns in South Korea. Health Policy 2011, 100, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Bernabe, E.; Liu, X.; Gallagher, J.E.; Zheng, S. Determinants of Catastrophic Dental Health Expenditure in China. PLoS ONE 2016, 11, e0168341. [Google Scholar] [CrossRef] [PubMed]
- Knaul, F.M.; Frenk, J. Health insurance in Mexico: Achieving universal coverage through structural reform. Health Aff. 2005, 24, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at Glance; OECD: Paris, France, 2013; Available online: https://www.oecd.org/els/health-systems/Health-at-a-Glance-2013.pdf (accessed on 25 November 2018).
- Bernabé, E.; Masood, M.; Vujicic, M. The impact of out-of-pocket payments for dental care on household finances in low and middle income countries. BMC Public Health 2017, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Health Ministry. DGIS. Financial Resources. Expenditure on Health in the National Health System. Available online: http://www.dgis.salud.gob.mx/contenidos/sinais/gastoensalud_gobmx.html (accessed on 25 November 2018).
- González, E. Salaries in Hidalgo. Milenio. 23 August 2016. Available online: http://www.milenio.com/opinion/eduardo-gonzalez/intelecto-opuesto/salarios-en-hidalgo (accessed on 25 November 2018).
- Quiroz, V.; Reinero, D.; Hernández, P.; Contreras, J.; Vernal, R.; Carvajal, P. Development of a self-report questionnaire designed for population-based surveillance of gingivitis in adolescents: Assessment of content validity and reliability. J. Appl. Oral. Sci. 2017, 25, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.M.; Thomson, W.M.; McGee, R. An assessment of the validity and reliability of dental self-report items used in a National Child Nutrition Survey. Community Dent. Oral. Epidemiol. 2004, 32, 49–54. [Google Scholar] [CrossRef]
- Schluter, P.J.; Durward, C.; Cartwright, S.; Paterson, J. Maternal self-report of oral health in 4-year-old Pacific children from South Auckland, New Zealand: Findings from the Pacific Islands Families Study. J. Public Health Dent. 2007, 67, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Blizniuk, A.; Ueno, M.; Zaitsu, T.; Kawaguchi, Y. Association between self-reported and clinical oral health status in Belarusian adults. J. Investig. Clin. Dent. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, Á.; Borges-Yáñez, S.A.; Jiménez-Corona, A.; Jiménez-Corona, M.E.; Ponce-de-León, S. Self-report of gingival problems and periodontitis in indigenous and non-indigenous populations in Chiapas, Mexico. Int. Dent. J. 2016, 66, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Abbood, H.M.; Hinz, J.; Cherukara, G.; Macfarlane, T.V. Validity of self-reported periodontal disease: A systematic review and meta-analysis. J. Periodontol. 2016, 87, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Shpigel, I.; Peretz, B. The use of a self-report questionnaire for dental health status assessment: A preliminary study. Br. Dent. J. 2013, 214, E15. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.E.; Menezes, A.M.; Assunção, M.C.; Gonçalves, H.; Demarco, F.; Vargas-Ferreira, F.; Peres, M. Validation of self-reported information on dental caries in a birth cohort at 18 years of age. PLoS ONE 2014, 9, e106382. [Google Scholar] [CrossRef] [PubMed]
- Haugejorden, O.; Klock, K.S.; Trovik, T.A. Incidence and predictors of self-reported tooth loss in a representative sample of Norwegian adults. Community Dent. Oral. Epidemiol. 2003, 31, 261–268. [Google Scholar] [CrossRef]
- Gilbert, G.H.; Chavers, L.S.; Shelton, B.J. Comparison of two methods of estimating 48-month tooth loss incidence. J. Public Health Dent. 2002, 62, 163–169. [Google Scholar] [CrossRef]
- Matsui, D.; Yamamoto, T.; Nishigaki, M.; Miyatani, F.; Watanabe, I.; Koyama, T.; Ozaki, E.; Kuriyama, N.; Kanamura, N.; Watanabe, Y. Validity of self-reported number of teeth and oral health variables. BMC Oral. Health 2016, 17, 17. [Google Scholar] [CrossRef]
- Ueno, M.; Shimazu, T.; Sawada, N.; Tsugane, S.; Kawaguchi, Y. Validity of self-reported tooth counts and masticatory status study of a Japanese adult population. J. Oral. Rehabil. 2018, 45, 393–398. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Frequencies | Percentages |
|---|---|---|
| Age (children) | ||
| 6/7 years | 221 | 29.0 |
| 8/9 years | 237 | 31.0 |
| 10/12 years | 305 | 40.0 |
| Sex | ||
| Boys | 374 | 49.0 |
| Girls | 389 | 51.0 |
| Number of household members | ||
| <3 | 178 | 23.3 |
| <5 | 456 | 59.8 |
| ≥6 | 129 | 16.9 |
| Dental visits in the last year | ||
| 1 | 297 | 38.9 |
| 2 | 247 | 32.4 |
| ≥3 | 219 | 28.7 |
| Dental pain in the last year | ||
| No | 238 | 31.2 |
| Yes | 525 | 68.8 |
| Reason for the last dental visit | ||
| Curative | 501 | 65.6 |
| Preventive | 205 | 26.9 |
| Specialty treatment | 57 | 7.5 |
| Report of oral disease | ||
| No | 591 | 77.5 |
| Yes | 172 | 22.5 |
| Oral health perception | ||
| Very poor/poor | 85 | 11.1 |
| Regular | 309 | 40.5 |
| Good/Very good | 369 | 48.4 |
| Frequency of tooth brushing | ||
| Less than once a day | 135 | 17.7 |
| At least once a day | 628 | 82.3 |
| Oral health knowledge | ||
| Low | 257 | 33.7 |
| Medium | 288 | 37.7 |
| High | 218 | 28.6 |
| Variables | Frequencies | Percentages |
|---|---|---|
| Educational level of mother | ||
| Lower than elementary | 58 | 7.6 |
| Lower than middle | 299 | 39.2 |
| Lower than high school | 249 | 32.6 |
| High school and beyond | 157 | 20.6 |
| Educational level of father | ||
| Lower than elementary | 75 | 10.0 |
| Lower than middle | 221 | 29.5 |
| Lower than high school | 203 | 27.0 |
| High school and beyond | 251 | 33.5 |
| Health insurance | ||
| None | 230 | 30.1 |
| Social Security | 368 | 48.2 |
| SEDENA/SEMAR/PEMEX * | 47 | 6.2 |
| Private insurance | 31 | 4.1 |
| Seguro Popular | 87 | 11.4 |
| SEP (housing features) | ||
| 1st tertile | 260 | 34.1 |
| 2nd tertile | 265 | 34.7 |
| 3rd tertile | 238 | 31.2 |
| SEP (ownership of household appliances) | ||
| 1st tertile | 255 | 33.4 |
| 2nd tertile | 256 | 33.6 |
| 3rd tertile | 252 | 33.0 |
| Household car ownership | ||
| No | 279 | 36.8 |
| Yes | 480 | 63.2 |
| Expenditure Items | PPP US$ Mean ± sd * | Mexican Pesos Mean ± sd |
|---|---|---|
| Transportation | 2.97 ± 7.12 | 27.38 ± 65.72 |
| Consultations | 24.48 ± 37.68 | 225.92 ± 347.79 |
| Treatments | 31.89 ± 87.38 | 294.39 ± 806.48 |
| Medications | 6.23 ± 26.11 | 57.51 ± 240.99 |
| Laboratory tests and radiographic studies | 2.67 ± 12.31 | 24.65 ± 113.65 |
| Others | 1.63 ± 23.29 | 15.06 ± 214.97 |
| Total average expenditure | 70.17 ± 123.72 | 647.65 ± 1141.95 |
| Variables | PPP US$ Mean ± sd | Mexican Pesos Mean ± sd | p Value |
|---|---|---|---|
| Age (children) | |||
| 6/7 years | 52.81 ± 75.80 | 487.45 ± 699.68 | |
| 8/9 years | 75.95 ± 129.51 | 701.05 ± 1195.35 | |
| 10/12 years | 78.18 ± 144.34 | 721.59 ± 1332.27 | 0.0794 * |
| Sex | |||
| Boys | 71.21 ± 132.03 | 657.24 ± 1,218.62 | |
| Girls | 69.13 ± 115.12 | 638.07 ± 1062.53 | 0.6230 † |
| Number of household members | |||
| <3 | 50.29 ± 77.88 | 464.17 ± 718.85 | |
| <5 | 77.29 ± 133.66 | 713.37 ± 1,233.69 | |
| ≥6 | 72.24 ± 135.74 | 666.82 ± 1,252.85 | 0.0792 † |
| Dental visits in the last year | |||
| 1 | 47.32 ± 70.76 | 436.79 ± 653.13 | |
| 2 | 60.08 ± 82.78 | 554.54 ± 764.04 | 0.0002 † |
| ≥3 | 112.45 ± 190.48 | 1037.88 ± 1758.1 | <0.001 ‡ |
| Dental pain in the last year | |||
| No | 70.02 ± 145.23 | 646.28 ± 1,340.49 | |
| Yes | 70.17 ± 112.59 | 647.65 ± 1,039.25 | <0.0001 * |
| Reason for the last dental visit | |||
| Curative | 55.19 ± 73.43 | 509.36 ± 677.77 | |
| Preventive | 70.32 ± 166.30 | 649.02 ± 1534.92 | |
| Specialty treatment | 201.31 ± 199.23 | 1858.06 ± 1838.89 | 0.0001 † |
| Report of oral disease | |||
| No | 64.09 ± 107.11 | 591.51 ± 988.59 | |
| Yes | 91.08 ± 167.33 | 840.71 ± 1544.5 | 0.6439 * |
| Oral health perception | |||
| Very poor/poor | 98.80 ± 141.97 | 911.91 ± 1310.36 | |
| Regular | 62.16 ± 139.00 | 573.71 ± 1282.98 | |
| Good/Very good | 70.17 ± 103.25 | 647.65 ± 952.99 | 0.0001 † |
| Frequency of tooth brushing | |||
| Less than once a day | 76.84 ± 124.46 | 709.27 ± 1148.79 | |
| At least once a day | 68.68 ± 123.57 | 633.96 ± 1140.58 | 0.5433 * |
| Oral health knowledge | |||
| Low | 52.22 ± 71.06 | 481.97 ± 655.87 | |
| Medium | 97.17 ± 127.43 | 896.85 ± 1176.18 | |
| High | 97.91 ± 158.43 | 903.7 ± 1462.35 | 0.0065 † |
| Variables | PPP US Mean ± sd | Mexican Pesos Mean ± sd | p Value |
|---|---|---|---|
| Educational level of mother | |||
| Lower than elementary | 31.60 ± 35.31 | 291.65 ± 325.88 | |
| Lower than middle | 81.89 ± 136.33 | 755.82 ± 1258.33 | |
| Lower than high school | 62.16 ± 92.42 | 573.71 ± 853.04 | |
| High school and beyond | 74.77 ± 155.47 | 690.10 ± 1434.96 | 0.0617 † |
| Educational level of father | |||
| Lower than elementary | 94.79 ± 145.82 | 874.94 ± 1345.96 | |
| Lower than middle | 60.08 ± 93.46 | 554.54 ± 862.62 | |
| Lower than high school | 57.85 ± 118.08 | 534.00 ± 1089.91 | 0.026 ‡ |
| High school and beyond | 84.71 ± 143.30 | 781.84 ± 1322.69 | 0.0080 † |
| Health insurance 1 | |||
| None | 85.15 ± 149.38 | 785.94 ± 1378.82 | |
| Social Security | 74.32 ± 127.87 | 685.99 ± 1180.28 | |
| SEDENA/SEMAR/PEMEX | 48.51 ± 48.66 | 447.74 ± 449.11 | |
| Private insurance | 49.40 ± 40.65 | 455.96 ± 375.17 | |
| Seguro Popular | 32.04 ± 43.32 | 295.76 ± 399.82 | 0.0034 † |
| SEP (housing features) | |||
| 1st tertile | 64.98 ± 109.93 | 599.73 ± 1014.61 | |
| 2nd tertile | 61.12 ± 94.79 | 564.13 ± 874.94 | 0.028 ‡ |
| 3rd tertile | 85.74 ± 159.92 | 791.42 ± 1476.04 | 0.0007 † |
| SEP (ownership of household goods) | |||
| 1st tertile | 65.57 ± 104.73 | 605.2 ± 966.68 | |
| 2nd tertile | 60.67 ± 102.95 | 560.02 ± 950.25 | 0.048 ‡ |
| 3rd tertile | 84.41 ± 155.62 | 779.10 ± 1436.33 | 0.0001 † |
| Household car ownership | |||
| No | 44.21 ± 60.97 | 408.03 ± 562.76 | |
| Yes | 85.45 ± 146.72 | 788.68 ± 1354.18 | 0.0001 * |
| Variables | Linear Regression Coefficient | 95% CI | Logistic Regression Odds Ratio | 95% CI |
|---|---|---|---|---|
| Age (children) | ||||
| 6/7 years | 1 * | 1 | ||
| 8/9 years | 155.21 † | 36.81–273.61 | 1.18 n/s | 0.76–1.86 |
| 10/12 years | 229.89 ‡ | 77.53–382.25 | 1.05 n/s | 0.70–1.55 |
| Dental visits in the last year | ||||
| 1 | 1 * | |||
| 2 | 48.83 n/s | −107.60–205.28 | ||
| ≥3 | 311.11 † | 85.57–536.66 | not included | |
| Dental pain in the last year | ||||
| No | 1 * | |||
| Yes | not included | 2.25 § | 1.49–3.39 | |
| Reason for the last dental visit | ||||
| Curative | −783.38 ‡ | −1187.1–−235.1 | 2.48 ‡ | 1.37–4.47 |
| Preventive | −711.15 § | −1146.9–−419.8 | 1 * | |
| Specialty treatment | 1 * | 2.69 n/s | 0.63–11.48 | |
| Educational level of mother | ||||
| Lower than elementary | 1 * | |||
| Lower than middle | 265.76 § | 159.21–372.32 | ||
| Lower than high school | 129.68 ‡ | 36.08–223.28 | ||
| High school and beyond | 116.61 † | 9.96–223.26 | not included | |
| Health insurance 1 | ||||
| None | 1 * | 1 * | ||
| Social Security | −23.96 n/s | −124.69–76.75 | 0.67 n/s | 0.43–1.05 |
| SEDENA/SEMAR/PEMEX | −234.92 n/s | −479.05–9.21 | 1.11 n/s | 0.45–2.69 |
| Private insurance | −81.27 n/s | −211.87–49.31 | 1.23 n/s | 0.45–3.38 |
| Seguro Popular | −210.27 ‡ | −315.09–−105.45 | 0.38§ | 0.26–0.53 |
| SEP (housing features) | ||||
| 1st tertile | 1 * | |||
| 2nd tertile | 4.91 § | 2.21–10.94 | ||
| 3rd tertile | not included | 2.47 ‡ | 1.23–4.95 | |
| Household car ownership | ||||
| No | 1 * | |||
| Yes | 179.85 ‡ | 65.12–294.58 | not included |
| Variables | Coefficient | 95% CI |
|---|---|---|
| Age (children) | ||
| 6/7 years | 1 * | |
| 8/9 years | 170.32 † | 28.79–311.85 |
| 10/12 years | 315.55 ‡ | 120.76–510.34 |
| Dental visits in the last year | ||
| 1 | 1 * | |
| 2 | 63.92 n/s | −104.84–232.69 |
| ≥3 | 359.38 ‡ | 133.01–585.74 |
| Reason for the last dental visit | ||
| Curative | −914.72 § | −1123.70–−705.74 |
| Preventive | −713.92 ‡ | −1071.62–−356.23 |
| Specialty treatment | 1 * | |
| Educational level of mother | ||
| Lower than elementary | 1 * | |
| Lower than middle | 313.93 ‡ | 166.36–461.50 |
| Lower than high school | 122.10 † | 8.80–235.39 |
| High school and beyond | 310.53 ‡ | 153.83–467.23 |
| Health insurance 1 | ||
| None | 1 * | |
| Social Security | 8.16 n/s | −143.68–160.01 |
| SEDENA/SEMAR/PEMEX | −270.95 † | −501.05–−40.86 |
| Private insurance | 46.97 n/s | −201.46–107.52 |
| Seguro Popular | −221.93 † | −388.46–−55.39 |
| Household car ownership | ||
| No | 1 * | |
| Yes | 144.64 ‡ | 9.25–280.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medina-Solís, C.E.; Ávila-Burgos, L.; Márquez-Corona, M.d.L.; Medina-Solís, J.J.; Lucas-Rincón, S.E.; Borges-Yañez, S.A.; Fernández-Barrera, M.Á.; Pontigo-Loyola, A.P.; Maupomé, G. Out-Of-Pocket Expenditures on Dental Care for Schoolchildren Aged 6 to 12 Years: A Cross-Sectional Estimate in a Less-Developed Country Setting. Int. J. Environ. Res. Public Health 2019, 16, 1997. https://doi.org/10.3390/ijerph16111997
Medina-Solís CE, Ávila-Burgos L, Márquez-Corona MdL, Medina-Solís JJ, Lucas-Rincón SE, Borges-Yañez SA, Fernández-Barrera MÁ, Pontigo-Loyola AP, Maupomé G. Out-Of-Pocket Expenditures on Dental Care for Schoolchildren Aged 6 to 12 Years: A Cross-Sectional Estimate in a Less-Developed Country Setting. International Journal of Environmental Research and Public Health. 2019; 16(11):1997. https://doi.org/10.3390/ijerph16111997
Chicago/Turabian StyleMedina-Solís, Carlo Eduardo, Leticia Ávila-Burgos, María de Lourdes Márquez-Corona, June Janette Medina-Solís, Salvador Eduardo Lucas-Rincón, Socorro Aida Borges-Yañez, Miguel Ángel Fernández-Barrera, América Patricia Pontigo-Loyola, and Gerardo Maupomé. 2019. "Out-Of-Pocket Expenditures on Dental Care for Schoolchildren Aged 6 to 12 Years: A Cross-Sectional Estimate in a Less-Developed Country Setting" International Journal of Environmental Research and Public Health 16, no. 11: 1997. https://doi.org/10.3390/ijerph16111997