Active Tobacco Smoke Exposure in Utero and Concentrations of Hepcidin and Selected Iron Parameters in Newborns

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Blood Sampling and Biochemical Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. The Global Prevalence of Anemia in 2011; WHO: Geneva, Switzerland, 2015; Available online: www.who.int/nutrition/publications/micronutrients/global_prevalence_anaemia_2011/en/ (accessed on 19 May 2015).
- Cao, C.; O’Brien, K.O. Pregnancy and iron homeostasis: An update. Nutr. Rev. 2013, 71, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Wojtyła, C.; Głuszek, Ł.; Biliński, P.; Paprzycki, P.; Warzocha, K. Smoking during pregnancy-hematological observations in pregnant women and their newborns after delivery. Ann. Agric. Environ. Med. 2012, 19, 836–841. [Google Scholar] [PubMed]
- Koenig, M.D.; Tussing-Humphreys, L.; Day, J.; Cadwell, B.; Nemeth, E. Hepcidin and iron homeostasis during pregnancy. Nutrients 2014, 6, 3062–3083. [Google Scholar] [CrossRef] [PubMed]
- Haider, B.A.; Olofin, I.; Wang, M.; Spigelman, D.; Ezzati, M.; Fawzii, W.W.; Nutrition Impact Model Study Group. Anaemia prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346, F3443. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.L.; Nemeth, E. Iron homeostasis during pregnancy. Am. J. Clin. Nutr. 2017, 106 (Suppl. 6), 1567S. [Google Scholar] [CrossRef] [PubMed]
- Berglund, S.; Lonnerdal, B.; Westrup, B.; Domellof, M. Effects of iron supplementation on serum hepcidin and serum erythropoietin in low-birth-weight infants. Am. J. Clin. Nutr. 2011, 94, 1553–1561. [Google Scholar] [CrossRef]
- Nicolas, G.; Chauvet, C.; Viatte, L.; Danna, J.L.; Bigard, X.; Devaux, I.; Beaumont, C.; Kahn, A.; Vaulont, S. The gene encoding the iron regulatory peptide hepcidin is regulated by anemia, hypoxia, and inflammation. J. Clin. Investig. 2002, 110, 1037–1044. [Google Scholar] [CrossRef]
- Young, M.F.; Griffin, I.; Pressman, E.; McIntyre, A.W.; Cooper, E.; McNanley, T.; Harris, Z.L.; Westerman, M.; O’Brien, K.O. Maternal hepcidin is associated with placental transfer of iron derived from dietary heme and nonheme sources. J. Nutr. 2012, 142, 33–39. [Google Scholar] [CrossRef]
- Lee, S.; Guillet, R.; Cooper, E.M.; Westerman, M.; Orlando, M.; Kent, T.; Pressman, E.; O’Brien, K.O. Prevalence of anemia and associations between neonatal iron status, hepcidin, and maternal iron status among neonates born to pregnant adolescents. Pediatr. Res. 2016, 79, 42–48. [Google Scholar] [CrossRef]
- Briana, D.D.; Boutsikou, T.; Baka, S.; Boutsikou, M.; Stamati, L.; Hassiakos, D.; Gourgiotis, D.; Malamitsi-Puchner, A. Perinatal role of hepcidin and iron homeostasis in full-term intrauterine growth-restricted infants. Eur. J. Haematol. 2012, 90, 37–44. [Google Scholar] [CrossRef]
- Teramo, K.A.; Widness, J.A. Increased fetal plasma and amniotic fluid erythropoietin concentrations: Markers of intrauterine hypoxia. Neonatology 2009, 95, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Sokołowska, E.; Klimek, J. Hepcidin-hormone taking part in the regulation of iron metabolism in the body. Postepy Biol. Kom. 2007, 1, 15. [Google Scholar]
- Dallalio, G.; Law, E.; Means, R.T., Jr. Hepcidin inhibits in vitro erythroid colony formation and reduced erythropoietin concentrations. Blood 2006, 107, 2702–2704. [Google Scholar] [CrossRef] [PubMed]
- Kulik-Rechberger, B.; Szponar, E.; Kościesza, A.; Furmaga-Jabłońska, W. Soluble transferrin receptor as a marker of iron stores in full term and preterm newborns and infants. Acta Haematol. Pol. 2010, 41, 551–556. [Google Scholar]
- Sweet, D.G.; Savage, G.; Tubman, T.R.; Lappin, T.R.; Halliday, H.L. Study of maternal influences on fetal iron status at term using cord blood transferrin receptors. Arch. Dis. Child Fetal Neonatal. Ed. 2001, 84, F40–F43. [Google Scholar] [CrossRef] [PubMed]
- Begiun, Y. Soluble transferrin receptor for the evaluation of erythropoiesis and iron status. Clin. Chim. Acta 2003, 329, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Chełchowska, M.; Ambroszkiewicz, J.; Gajewska, J.; Jabłońska-Głąb, E.; Maciejewski, T.M.; Ołtarzewski, M. Hepcidin and iron metabolism in pregnancy: Correlation with smoking and birth weight and length. Biol. Trace Elem. Res. 2016, 173, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Ingvarsson, R.F.; Bjarnason, A.O.; Dagbjartsson, A.; Hardardottir, H.; Haraldsson, A.; Thorkelsson, T. The effects of smoking in pregnancy on factors influencing fetal growth. Acta Paediatr. 2007, 96, 383–386. [Google Scholar] [CrossRef]
- Rehu, M.; Punnonen, K.; Ostland, V.; Heinonen, S.; Westerman, M.; Pulkki, K.; Sankilampi, U. Maternal serum hepcidin is slow at term and independent of cord blood iron status. Eur. J. Haematol. 2010, 85, 345–352. [Google Scholar] [CrossRef]
- Laskowska-Klita, T.; Chełchowska, M.; Ołtarzewski, M.; Gajewska, J.; Ambroszkiewicz, J. The effect of tobacco smoking during pregnancy on birth mass on the basis of population study-preliminary results. Przegl. Lek. 2010, 67, 830–834. [Google Scholar]
- Polanska, K.; Krol, A.; Kaluzny, P.; Ligocka, D.; Mikolajewska, K.; Shaheen, S.; Walton, R.; Hanke, W. Estimation of cut-off points for active and passive smoking during pregnancy-polish mother and child cohort (REPRO_PL). Int. J. Environ. Res. Public Health 2016, 13, 1216. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M.J.; Tunstall-Pedoe, H.; Feyerabend, C.; Vesey, C.; Saloojee, Y. Comparison of tests used to distinguish smokers from non-smokers. Am. J. Public Health 1987, 77, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Sazak, S.; Kayiran, S.M.; Paksoy, Y. Umbilical cord serum erythropoietin levels and maternal smoking during pregnancy. Sci. World J. 2012, 2012, 420763. [Google Scholar] [CrossRef] [PubMed]
- Sekovanić, A.; Jurasović, J.; Piasek, M.; Pašalić, D.; Orct, T.; Grgec, A.S.; Stasenko, S.; Čakanić, K.B.; Jazbec, A. Metallothionein 2A gene polymorphism and trace elements in mother-newborn pairs in the Croatian population. J. Trace Elem. Med. Biol. 2018, 45, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Sochaczewska, D.; Czeszyńska, M.B.; Konefał, H.; Elster, T.; Baryła-Pankiewicz, E. Assessment of relationship between cord blood cotinine levels and some factors of perinatal hypoxia. Ginekol. Pol. 2009, 80, 920–926. [Google Scholar] [PubMed]
- Metryka, E.; Chibowska, K.; Gutowska, I.; Falkowska, A.; Kupnicka, P.; Barczak, K.; Chlubek, D.; Baranowska-Bosiacka, I. Lead (Pb) exposure enhances expression of factors associated with inflammation. Int. J. Mol. Sci. 2018, 19, 1813. [Google Scholar] [CrossRef]
- Pateva, I.B.; Kerling, E.H.; Reddy, M.; Chen, D.; Carlson, S.E.; Tancabelic, J. Effect of maternal cigarette smoking on newborn iron stores. Clin. Res. Trials 2015, 1, 4–7. [Google Scholar] [PubMed]
- Eslami, Z.; Ghilian, R.; Abbasi, F. Evaluation of haemoglobin concentration of cord, capillary and venous sampling in neonates. Iran. J. Pediatr. Hematol. Oncol. 2012, 2, 159–163. [Google Scholar]
- Delaney, K.M.; Guillet, R.; Fleming, R.E.; Ru, Y.; Pressman, E.K.; Vermeylen, F.; Nemeth, E.; O’Brien, K.O. Umbilical cord serum ferritin concentration is inversely associated with umbilical cord hemoglobin in neonates born to adolescents carrying singletons and women carrying multiples. J. Nutr. 2019, 149, 406–415. [Google Scholar] [CrossRef]
- Rasmussen, S.; Bergsjo, P.; Jacobsen, G.; Haram, K.; Bakketeig, L.S. Haemoglobin and serum ferritin in pregnancy-correlation with smoking and body mass index. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 123, 27–34. [Google Scholar] [CrossRef]
- Zafar, J.; Mohammad, K.N.; Nisar, M.; Rashida, M.; Assadullah, S.B.; Shumaila, B.; Mohammad, S.A. Effect of cigarette smoking on erythrocytes, leukocytes and haemoglobin. J. Med. Sci. 2003, 3, 245–250. [Google Scholar]
- Habek, D.; Habek, J.C.; Ivanisevic, M.; Djelmis, J. Fetal tobacco syndrome and perinatal outcome. Fetal Diagn. Ther. 2002, 17, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Gruslin, A.; Perkins, S.L.; Manchanda, R.; Fleming, N.; Clinch, J.J. Maternal smoking and fetal erythropoietin levels. Obstet. Gynecol. 2000, 95, 561–564. [Google Scholar] [PubMed]
- Van Santen, S.; de Mast, Q.; Luty, A.J.F.; Wiegerinck, E.T.; Van der Ven, A.J.; Swinkels, DW. Iron homeostasis in mother and child during placental malaria infection. Am. J. Trop. Med. Hyg. 2011, 84, 148–151. [Google Scholar] [CrossRef]
- Basu, S.; Kumar, N.; Srivastava, R.; Kumar, A. Maternal and cord blood hepcidin concentrations in severe iron deficiency anemia. Pediatr. Neonat. 2016, 57, 413–419. [Google Scholar] [CrossRef]
- Lorenz, L.; Herbst, J.; Engel, C.; Peter, A.; Abele, H.; Poets, C.F.; Westerman, M.; Franz, A.R. Gestational age-specific reference ranges of hepcidin in cord blood. Neonatology 2014, 106, 133–139. [Google Scholar] [CrossRef]
- Ichinomiya, K.; Maruyama, K.; Inoue, T.; Koizumi, A.; Inoue, F.; Fukuda, K.; Yamazaki, Y.; Arakawa, H. Perinatal factors affecting serum hepcidin levels in low-birth-weight infants. Neonatology 2017, 112, 180–186. [Google Scholar] [CrossRef]
- Marshall, T. What is a case-control study? Int. J. Epidemiol. 2004, 33, 612–613. [Google Scholar] [CrossRef]
- Hoppe, M.; Hulthén, L.; Samuelson, G. Is cord blood hepcidin influenced by the low-grade acute-phase response occurring during delivery? A small-scale longitudinal study. J. Matern. Fetal Neonatal. Med. 2019, 32, 2166–2172. [Google Scholar] [CrossRef]
- Ru, Y.; Pressman, E.K.; Guillet, R.; Katzman, P.J.; Vermeylen, F.; O’Brien, K.O. Umbilical cord hepcidin concentrations are positively associated with the variance in iron status among multiple birth neonates. J. Nutr. 2018, 48, 1716–1722. [Google Scholar] [CrossRef]
- Yang, A.; Zhao, J.; Lu, M.; Gu, Y.; Zhu, Y.; Chen, D.; Fu, J. Expression of hepcidin and ferroportin in the placenta, and ferritin and transferrin receptor 1 levels in maternal and umbilical cord blood in pregnant women with and without gestational diabetes. Int. J. Environ. Res. Public Health 2016, 13, 766. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Smokers (n = 40) | Non-Smokers (n = 40) | p-Value |
|---|---|---|---|
| Newborn Characteristics | |||
| Gestational age, weeks | 39.0 ± 1.0 | 39.3 ± 0.9 | 0.384 |
| Apgar 1th min score | 10 (9–10) | 10 (10–10) | 0.511 |
| Apgar 5th min score | 10 (10–10) | 10 (10–10) | 0.576 |
| Male/Female, % | 46/54 | 38/62 | 0.420 |
| Birth weight, g | 3124 ± 427 | 3517 ± 446 | <0.001 |
| Birth body length, cm | 54.5 ± 2.7 | 55.9 ± 2.5 | 0.009 |
| Head circumference, cm | 34.0 ± 1.7 | 35.0 ± 1.1 | <0.001 |
| Cotinine, µg/L | 84.5 (56.3–112.1) | 0 | - |
| Maternal Characteristics | |||
| Age, years | 28.8 ± 4.5 | 30.3 ± 4.8 | 0.120 |
| Race: Caucasian, % | 100 | 100 | - |
| Mode of delivery: vaginal, % | 100 | 100 | - |
| Pre-gravid BMI, kg/m2 | 23.4 ± 1.3 | 24.1 ± 1.4 | 0.073 |
| Hemoglobin, g/dL | 12.2 ± 1.1 | 12.7 ±1.1 | 0.049 |
| Smoking habit smokers/non-smokers, % | 50 | 50 | - |
| Number of cigarettes, day | 10 (5–10) | - | - |
| Time of smoking before conception, year | 8 (5–12) | - | - |
| Cord Iron Status Parameters | Newborns of Smoking Mothers (n = 40) | Newborns of Non-Smoking Mothers (n = 40) | p-Value |
|---|---|---|---|
| Hepcidin, ng/mL | 36.8 ± 7.8 | 49.1 ± 9.6 | <0.001 |
| Erythropoietin, mIU/mL | 46.6 ± 14.6 | 22.2 ± 8.4 | <0.001 |
| Ferritin, ng/mL | 137.7 ± 26.2 | 150.1 ± 27.7 | 0.042 |
| Iron, µmol/L | 15.5 ± 4.0 | 17.3 ± 3.8 | 0.043 |
| Haemoglobin, g/dL | 16.3 (16.2–16.9) | 16.0 (15.8–16.4) | 0.063 |
| Soluble transferrin receptor, μg/mL | 5.5 ± 1.3 | 4.9 ± 1.0 | 0.011 |
| Cord Iron Status Parameters | Cotinine Level | Number of Cigarettes/Day | Time of Smoking Before Conception | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Hepcidin a | −0.334 | 0.033 | −0.320 | 0.041 | −0.128 | 0.425 |
| Erythropoietin a | 0.474 | 0.002 | 0.456 | 0.003 | 0.045 | 0.778 |
| Ferritin a | −0.250 | 0.115 | 0.064 | 0.692 | −0.087 | 0.589 |
| Iron a | −0.262 | 0.099 | −0.055 | 0.731 | −0.332 | 0.034 |
| Hemoglobin b | 0.185 | 0.247 | 0.226 | 0.155 | −0.018 | 0.912 |
| Soluble transferrin receptor a | 0.192 | 0.228 | 0.646 | 0.000 | 0.023 | 0.883 |
| Parameter | All Newborns (n = 80) | Newborns of Smoking Mothers (n = 40) | Newborns of Non-Smoking Mothers (n = 40) | |||
|---|---|---|---|---|---|---|
| β | p-Value | β | p-Value | β | p-Value | |
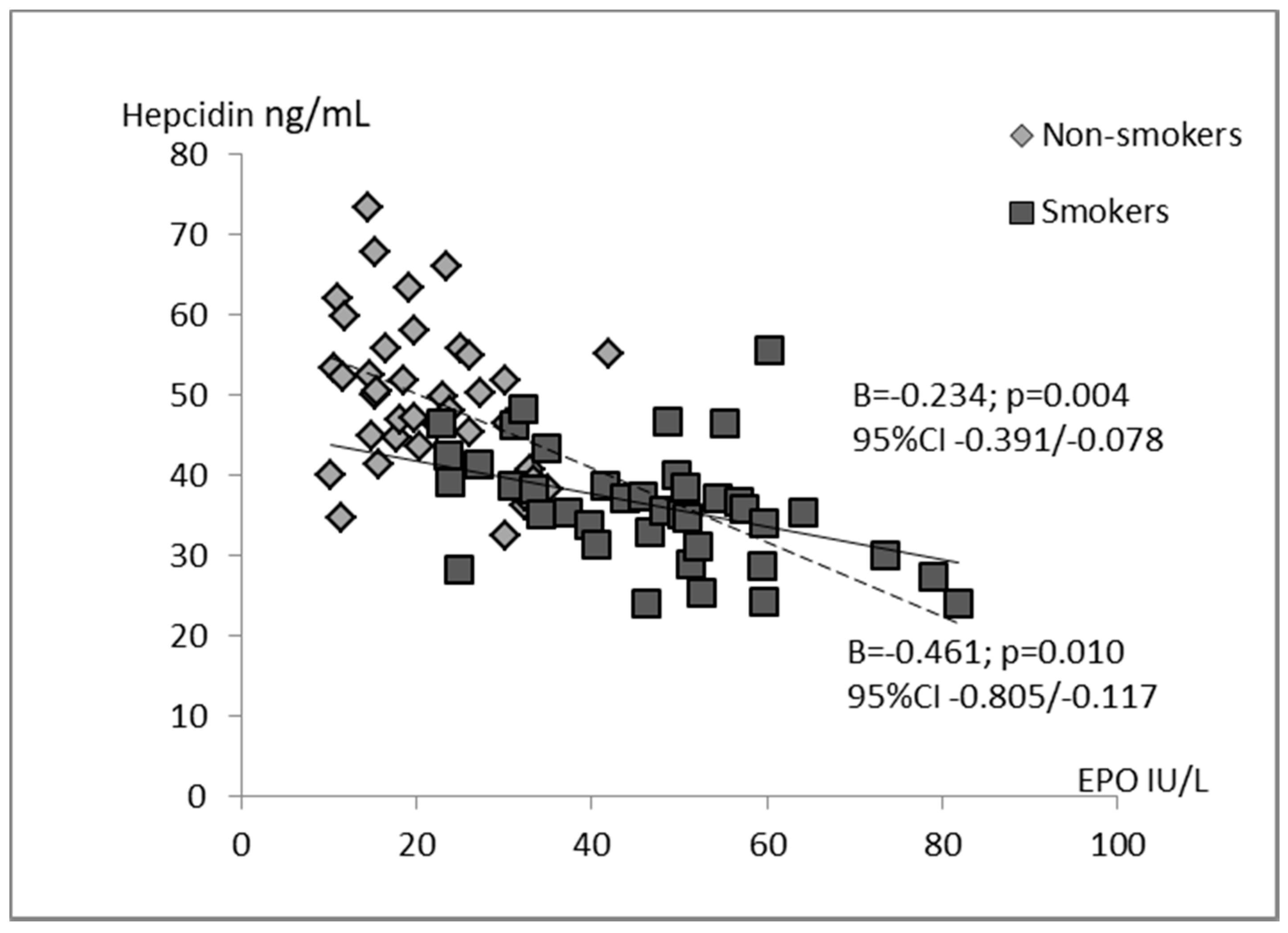
| Erythropoietin | −0.531 | 0.001 | −0.565 | 0.011 | −0.316 | 0.101 |
| Ferritin | 0.123 | 0.212 | 0.205 | 0.231 | 0.085 | 0.629 |
| Iron | −0.049 | 0.645 | −0.098 | 0.601 | 0.017 | 0.925 |
| Hemoglobin | 0.115 | 0.288 | 0.323 | 0.103 | −0.028 | 0.873 |
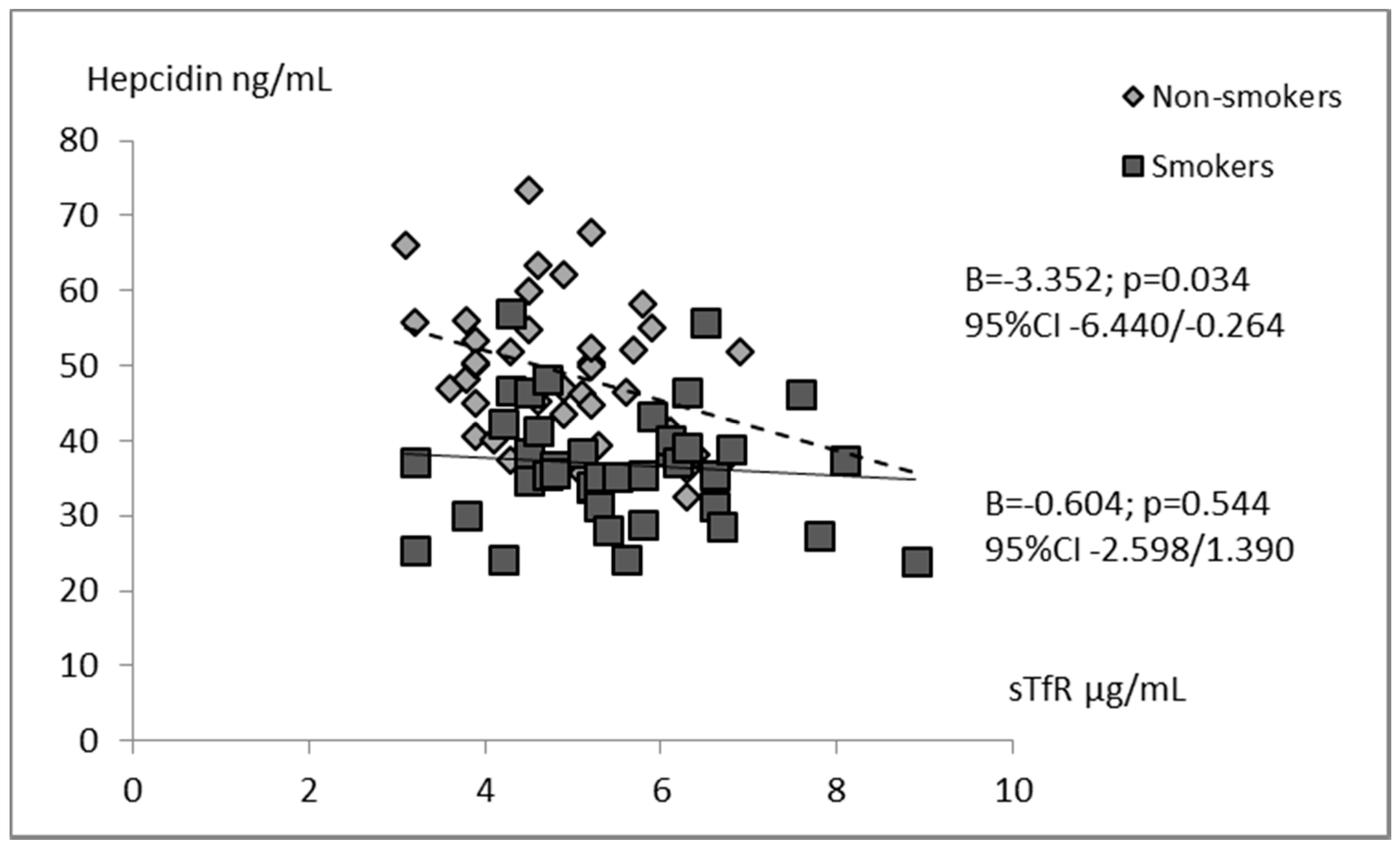
| Soluble transferrin receptor | −0.100 | 0.277 | 0.129 | 0.526 | −0.227 | 0.165 |
| Smoking status (no = 0; yes = 1) | 0.178 | 0.073 | - | - | - | - |
| Cotinine | - | - | 0.007 | 0.972 | - | - |
| Number of cigarettes/day | - | - | −0.242 | 0.350 | - | - |
| R2% | 46.6 | 31.9 | 22.5 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chełchowska, M.; Maciejewski, T.M.; Mazur, J.; Gajewska, J.; Zasimovich, A.; Ołtarzewski, M.; Ambroszkiewicz, J. Active Tobacco Smoke Exposure in Utero and Concentrations of Hepcidin and Selected Iron Parameters in Newborns. Int. J. Environ. Res. Public Health 2019, 16, 1996. https://doi.org/10.3390/ijerph16111996
Chełchowska M, Maciejewski TM, Mazur J, Gajewska J, Zasimovich A, Ołtarzewski M, Ambroszkiewicz J. Active Tobacco Smoke Exposure in Utero and Concentrations of Hepcidin and Selected Iron Parameters in Newborns. International Journal of Environmental Research and Public Health. 2019; 16(11):1996. https://doi.org/10.3390/ijerph16111996
Chicago/Turabian StyleChełchowska, Magdalena, Tomasz M. Maciejewski, Joanna Mazur, Joanna Gajewska, Anastasiya Zasimovich, Mariusz Ołtarzewski, and Jadwiga Ambroszkiewicz. 2019. "Active Tobacco Smoke Exposure in Utero and Concentrations of Hepcidin and Selected Iron Parameters in Newborns" International Journal of Environmental Research and Public Health 16, no. 11: 1996. https://doi.org/10.3390/ijerph16111996