Quantitative Microbial Risk Assessment for Workers Exposed to Bioaerosol in Wastewater Treatment Plants Aimed at the Choice and Setup of Safety Measures

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hazard Identification and Exposure Assessment
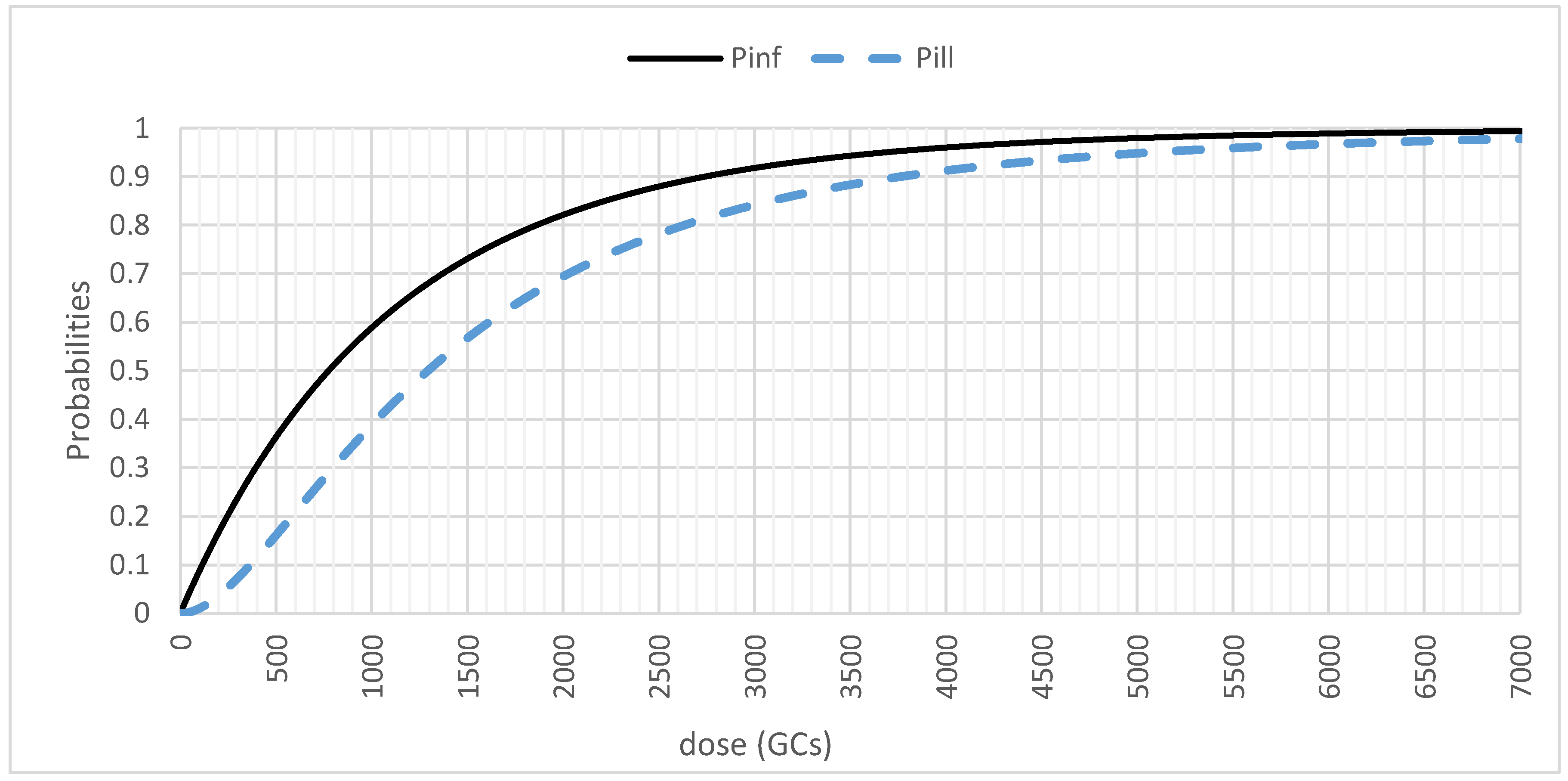
2.2. Dose–Response Assessment and Risk Characterization
2.3. Model Implementation
3. Results
- For the sewage influent, a lognormal distribution with µ = 7.7968 and σ = 1.5946;
- For the biological oxidation tank, a lognormal distribution with µ = 7.4005 and σ = 1.7299;
- For the sludge treatment, a uniform distribution in the range [306.67, 1664.9];
- For the side-entrance manhole, a uniform distribution in the range [306.67, 1664.9]. With the side-entrance manhole, we refer to the area of access to the manholes for inspection operations.
- 60.45 TCID50 or 42,315 GC at the biological oxidation tank;
- 72 TCID50 or 50,400 GC at the sewage entrance;
- 8.15 TCID50 or 5705 GC at the sludge treatment;
- 5.8 TCID50 or 4060 GC at the side entrance manhole.
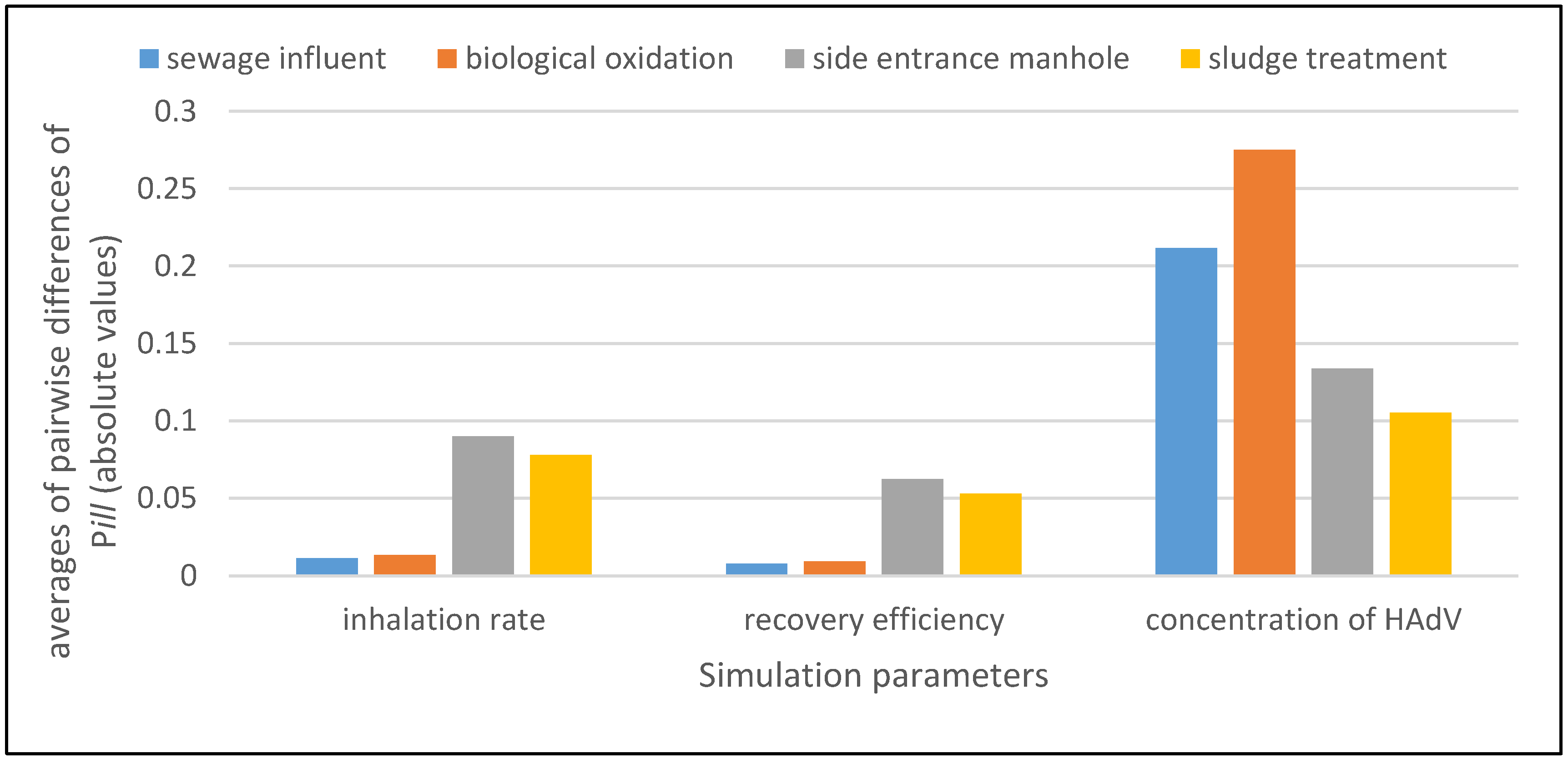
3.1. Sensitivity Analysis
3.2. Application of Quantitative Microbial Risk Assessment to Support Risk Management
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Douwes, J.; Thorne, P.; Pearce, N.; Heederik, D. Bioaerosol health effects and exposure assessment: Progress and prospects. Ann. Occup. Hyg. 2003, 47, 187–200. [Google Scholar] [PubMed]
- Corrao, C.; Mazzotta, A.; La Torre, G.; De Giusti, M. Biological risk and occupational health. Ind. Health 2012, 50, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Sykes, P.; Morris, R.H.; Allen, J.A.; Wilsmith, J.D.; Jones, K.P. Workers’ exposure to dust, endotoxin and beta-(1-3) glucan at four large scale composting facilities. Waste Manag. 2011, 31, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Neumann, H.D.; Balfanz, J.; Becker, G.; Lohmeyer, M.; Mathys, W.; Raulf-Heimsoth, M. Bioaerosol exposure during refuse collection: Results of field studies in the real-life situation. Sci. Total Environ. 2002, 293, 219–231. [Google Scholar] [CrossRef]
- Carducci, A.; Federigi, I.; Verani, M. Virus occupational exposure in solid waste processing facilities. Ann. Occup. Hyg. 2013, 57, 1115–1127. [Google Scholar] [PubMed]
- Vimercati, L.; Baldassarre, A.; Gatti, M.F.; De Maria, L.; Caputi, A.; Dirodi, A.A.; Cuccaro, F.; Bellino, R.M. Respiratory health in waste collection and disposal workers. Int. J. Environ. Res. Public Health 2016, 13, 631. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Directive 2000/54/EC of the European Parliament and of the Council of 18 September 2000 on the Protection of Workers from Risks Related to Exposure to Biological Agents at Work (Seventh Individual Directive within the Meaning of Article 16(1) of Directive. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32000L0054&from=EN (accessed on 4 January 2018).
- European Agency for Safety and Health at Work. E-fact 53: Risk Assessment for Biological Agents. Available online: https://osha.europa.eu/en/tools-and-publications/publications/e-facts/efact53/view (accessed on 4 January 2018).
- European Agency for Safety and Health at Work. Report—Expert Forecast on Emerging Biological Risks Related to Occupational Safety and Health. Available online: https://osha.europa.eu/it/tools-and-publications/publications/reports/7606488 (accessed on 4 January 2018).
- World Health Organization. Quantitative Microbial Risk Assessment: Application for Water Safety Management. Available online: http://www.who.int/water_sanitation_health/publications/qmra/en/ (accessed on 4 January 2018).
- Pang, H.; Lambertini, E.; Buchanan, R.; Schaffner, D. Quantitative microbial risk assessment for Escherichia coli O157:H7 in fresh-cut lettuce. J. Food Prot. 2017, 80, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.; Barker, G.; Gorris, L.; Tian, M.; Song, X.; Malakar, P. Status and future of quantitative microbiological risk assessment in China. Trends Food Sci. Technol. 2015, 42, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Carducci, A.; Donzelli, G.; Cioni, L.; Verani, M. Quantitative microbial risk assessment in occupational settings applied to the airborne human adenovirus infection. Int. J. Environ. Res. Public Health 2016, 13, 733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Chapter 6—Viruses. In Water Recreation and Disease. Plausibility of Associated Infections: Acute Effects, Sequelae and Mortality; Pond, K., Ed.; IWA Publishing: London, UK, 2005; pp. 191–219. ISBN 9241563052. [Google Scholar]
- Teunis, P.; Schijven, J.; Rutjes, S. A generalized dose-response relationship for adenovirus infection and illness by exposure pathway. Epidemiol. Infect. 2016, 144, 3461–3473. [Google Scholar] [CrossRef] [PubMed]
- Allard, A.; Vantarakis, A. Adenoviruses. In Global Water Pathogens Project; Rose, J.B., Jiménez-Cisneros, B., Eds.; Michigan State University: East Lansing, MI, USA, 2017; pp. 3–30. [Google Scholar]
- Carducci, A.; Morici, P.; Pizzi, F.; Battistini, R.; Rovini, E.; Verani, M. Study of the viral removal efficiency in an urban wastewater treatment plant. Water Sci. Technol. 2008, 58, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Masclaux, F.; Hotz, P.; Gashi, D.; Savova-Bianchi, D.; Oppliger, A. Assessment of airborne virus contamination in wastewater treatment plants. Environ. Res. 2014, 133, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Pascual, L.; Pérez-Luz, S.; Yàñez, M.; Santamarìa, A.; Gibert, K.; Salgot, M.; Apraiz, D.; Catalàn, V. Bioaerosol emission from wastewater treatment plant. Aerobiologia 2003, 19, 261–270. [Google Scholar] [CrossRef]
- Haas, C.; Rose, J.; Gerba, C. Risk assessment paradigms. In Quantitative Microbial Risk Assessment, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 63–89. ISBN 9781118145296. [Google Scholar]
- Carducci, A.; Arrighi, S.; Ruschi, A. Detection of coliphages and enteroviruses in sewage and aerosol from an activated sludge wastewater treatment plant. Lett. Appl. Microbiol. 1995, 21, 207–209. [Google Scholar] [CrossRef] [PubMed]
- McBride, G.; Stott, R.; Miller, W.; Bambic, D.; Wuertz, S. Discharge-based QMRA for estimation of public health risks from exposure to stormwater-borne pathogens in recreational waters in the United States. Water Res. 2013, 47, 5282–5297. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Exposure Factors Handbook: Chapter 6—Inhalation Rates. 2011. Available online: https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=236252 (accessed on 4 January 2018).
- Ventana Systems, Inc. User Guide—Vensim Introduction & Tutorials. Available online: https://www.vensim.com/documentation/index.html?users_guide.htm (accessed on 4 January 2018).
- Gan, Y.; Duan, Q.; Gong, W.; Tong, C.; Sun, Y.; Chu, W.; Ye, A.; Miao, C.; Di, Z. A comprehensive evaluation of various sensitivity analysis methods: A case study with a hydrological model. Environ. Model. Softw. 2014, 51, 269–285. [Google Scholar] [CrossRef]
- Thorn, J.; Kerekes, E. Health effects among employees in sewage treatment plants: A literature survey. Am. J. Ind. Med. 2001, 40, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Douwes, J.; Mannetje, A.; Heederik, D. Work-related symptoms in sewage treatment workers. Ann. Agric. Environ. Med. 2001, 8, 39–45. [Google Scholar] [PubMed]
- Guo, X.; Wu, P.; Ding, W.; Zhang, W.; Li, L. Reduction and characterization of bioaerosols in a wastewater treatment station via ventilation. J. Environ. Sci. 2014, 26, 1575–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, J.; Cloutier, Y.; Lara, J.; Marchand, G. Guide on Respiratory Protection Against Bioaerosols—Recommendations on Its Selection and Use; Technical Guide RG-501.IRSST—Chemical Substances and Biological Agents, Studies and Research Project; IRSST Communications Division: Montréal, QC, USA, 2007; Available online: http://www.irsst.qc.ca/media/documents/PubIRSST/RG-501.pdf (accessed on 10 January 2018).
- Tanner, B.D.; Brooks, J.P.; Gerba, C.P.; Haas, C.N.; Josephson, K.L.; Pepper, I.L. Estimated occupational risk from bioaerosols generated during land application of Class B biosolids. J. Environ. Qual. 2008, 37, 2311–2321. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.P.; McLaughlin, M.R.; Gerba, C.P.; Pepper, I.L. Land application of manure and Class B biosolids: An occupational and public quantitative microbial risk assessment. J. Environ. Qual. 2012, 41, 2009–2023. [Google Scholar] [CrossRef] [PubMed]
- Jahne, M.A.; Rogers, S.A.; Holsen, T.M.; Grimberg, S.J. Quantitative microbial risk assessment of bioaerosols from a manure application site. Aerobiologia 2015, 31, 73–87. [Google Scholar] [CrossRef]
- Carducci, A.; Tozzi, E.; Rubulotta, E.; Casini, B.; Cantiani, L.; Muscillo, M. Assessing airborne biological hazard from urban wastewater treatment. Water Res. 2000, 34, 1173–1178. [Google Scholar] [CrossRef]
- Vieira, C.; Baptista, J. Bioaerosol in hospital environment: A short review. In Occupational Safety and Hygiene II; Arezes, P., Baptista, J.S., Barroso, M.P., Carneiro, P., Cordeiro, P., Costa, N., Melo, R.B., Miguel, S.A., Perestrelo, G., Eds.; CRC Press: London, UK, 2014; Chapter 22; ISBN 9781138001442. [Google Scholar]
- Karra, S.; Katsivela, E. Microorganisms in bioaerosol emissions from wastewater treatment plants during summer at a Mediterranean site. Water Res. 2007, 41, 1355–1365. [Google Scholar] [CrossRef] [PubMed]
- Chigor, V.; Sibanda, T.; Okoh, A. Assessment of the risks for human health of adenoviruses, hepatitis A virus, rotaviruses and enteroviruses in the Buffalo River and three source water dams in the Eastern Cape. Food Environ. Virol. 2014, 6, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Corsi, S.; Borchardt, M.; Carvin, R.; Burch, T.; Spencer, S.; Lutz, M.; McDermott, C.; Busse, K.; Kleinheinz, G.; Feng, X.; et al. Human and bovine viruses and bacteria at three great lakes beaches: Environmental variable associations and health risk. Environ. Sci. Technol. 2016, 50, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Cui, Q.; Fang, T.; Huang, Y.; Dong, P.; Wang, W. Evaluation of bacterial pathogen diversity, abundance and health risks in urban recreational water by amplicon next-generation sequencing and quantitative PCR. J. Environ. Sci. 2017, 57, 137–149. [Google Scholar] [CrossRef] [PubMed]
- WHO. Quantitative Microbial Risk Assessment: Application for Water Safety Management; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Eregno, F.E.; Tryland, I.; Tjomsland, T.; Myrmel, M.; Robertson, L.; Heistad, A. Quantitative microbial risk assessment combined with hydrodynamic modelling to estimate the public health risk associated with bathing after rainfall events. Sci. Total Environ. 2016, 548–549, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Fuhrimann, S.; Winkler, M.; Stalder, M.; Niwagaba, C.; Babu, M.; Kabatereine, N.; Halage, A.; Utzinger, J.; Cissé, G.; Nauta, M. Disease burden due to gastrointestinal pathogens in a wastewater system in Kampala, Uganda. Microb. Risk Anal. 2016, 4, 16–28. [Google Scholar] [CrossRef] [Green Version]
- Seidu, R.; Heistad, A.; Amoah, P.; Drechsel, P.; Jenssen, P.D.; Stenström, T.A. Quantification of the health risk associated with wastewater reuse in Accra, Ghana: A contribution toward local guidelines. J. Water Health 2008, 6, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Mara, D.; Sleigh, A. Estimation of norovirus infection risks to consumers of wastewater-irrigated food crops eaten raw. J. Water Health 2008, 8, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Stellacci, P.; Liberti, L.; Notarnicola, M.; Haas, C.N. Hygienic sustainability of site location of wastewater treatment plants. A case study. II. Estimating airborne biological hazard. Desalination 2010, 253, 106–111. [Google Scholar] [CrossRef]
- Lim, K.Y.; Hamilton, A.J.; Jiang, S.C. Assessment of public health risk associated with viral contamination in harvested urban stormwater for domestic applications. Sci. Total Environ. 2015, 523, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Linnemann, C.; Gartside, P.; Phair, J.; Blacklow, N.; Zeiss, C. Serologic survey of rotavirus, norwalk agent and prototheca wickerhamii in wastewater workers. Am. J. Public Health 1985, 75, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, P.; Roudot-Thoraval, F. Seroprevalence of hepatitis A virus infection among sewage workers. Eur. J. Epidemiol. 1996, 12, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Montuori, P.; Negrone, M.; Cacace, G.; Triassi, M. Wastewater workers and hepatitis A virus infection. Occup. Med. 2009, 59, 506–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Rosa, G.; Pourshaban, M.; Iaconelli, M.; Muscillo, M. Quantitative real-time PCR of enteric viruses in influent and effluent samples from wastewater treatment plants in Italy. Annali dell’Istituto Superiore di Sanita 2010, 46, 266–273. [Google Scholar] [PubMed]
- Carducci, A.; Verani, M. Effects of bacterial, chemical, physical and meteorological variables on virus removal by a wastewater treatment plant. Food Environ. Virol. 2013, 5, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Masclaux, F.G.; Hotz, P.; Friedli, D.; Savova-Bianchi, D.; Oppliger, A. High occurrence of hepatitis E virus in samples from wastewater treatment plants in Switzerland and comparison with other enteric viruses. Water Res. 2013, 47, 5101–5109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myrmel, M.; Lange, H.; Rimstad, E. A 1-year quantitative survey of noro-, adeno-, human boca-, and hepatitis E viruses in raw and secondarily treated sewage from two plants in Norway. Food Environ. Virol. 2015, 7, 213–223. [Google Scholar] [CrossRef] [PubMed]





© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carducci, A.; Donzelli, G.; Cioni, L.; Federigi, I.; Lombardi, R.; Verani, M. Quantitative Microbial Risk Assessment for Workers Exposed to Bioaerosol in Wastewater Treatment Plants Aimed at the Choice and Setup of Safety Measures. Int. J. Environ. Res. Public Health 2018, 15, 1490. https://doi.org/10.3390/ijerph15071490
Carducci A, Donzelli G, Cioni L, Federigi I, Lombardi R, Verani M. Quantitative Microbial Risk Assessment for Workers Exposed to Bioaerosol in Wastewater Treatment Plants Aimed at the Choice and Setup of Safety Measures. International Journal of Environmental Research and Public Health. 2018; 15(7):1490. https://doi.org/10.3390/ijerph15071490
Chicago/Turabian StyleCarducci, Annalaura, Gabriele Donzelli, Lorenzo Cioni, Ileana Federigi, Roberto Lombardi, and Marco Verani. 2018. "Quantitative Microbial Risk Assessment for Workers Exposed to Bioaerosol in Wastewater Treatment Plants Aimed at the Choice and Setup of Safety Measures" International Journal of Environmental Research and Public Health 15, no. 7: 1490. https://doi.org/10.3390/ijerph15071490