Development of Ahmedabad’s Air Information and Response (AIR) Plan to Protect Public Health

 ,
,
Abstract
:1. Introduction
1.1. Air Pollution as A Public Health Concern in India
1.2. Economic Growth and Climate Change
1.3. Ahmedabad’s Leadership on Extreme Heat Preparedness
1.4. Objectives
2. Methods
2.1. Planning and Conceptual Model Development
2.2. Community Needs Assessment
2.3. Baseline Data
2.3.1. India’s Air Quality Standards
2.3.2. Ahmedabad’s Air Pollution Monitoring
2.3.3. Health Impacts of Air Pollution in Ahmedabad
2.3.4. Best Practices from Other AQI Systems
2.4. Coalition Building and Outreach
3. Results
3.1. Planning
3.2. Community Needs Assessment
3.3. Baseline Data
3.3.1. India’s Air Quality Standards
3.3.2. Ahmedabad’s Air Pollution Monitoring
3.3.3. Health Impacts of Air Pollution in Ahmedabad
3.3.4. Best Practices from Other AQI Systems
3.4. Intervention Implementation
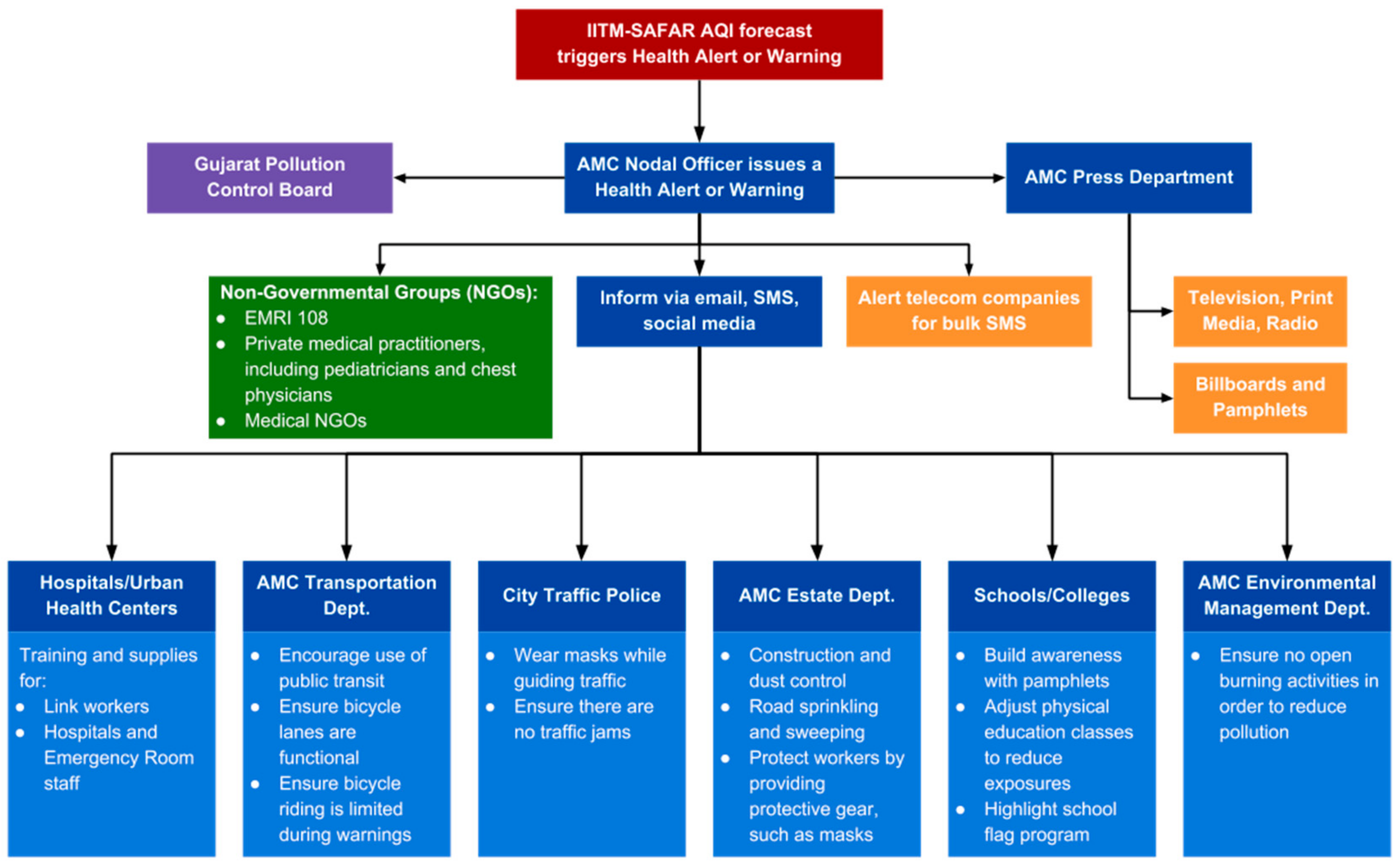
- Pilot Health-Based AQI Warning and Interagency Coordination—robust interagency coordination to pilot a color-coded AQI alert system that makes air quality data from new IITM-SAFAR air quality stations in Ahmedabad available to the public.
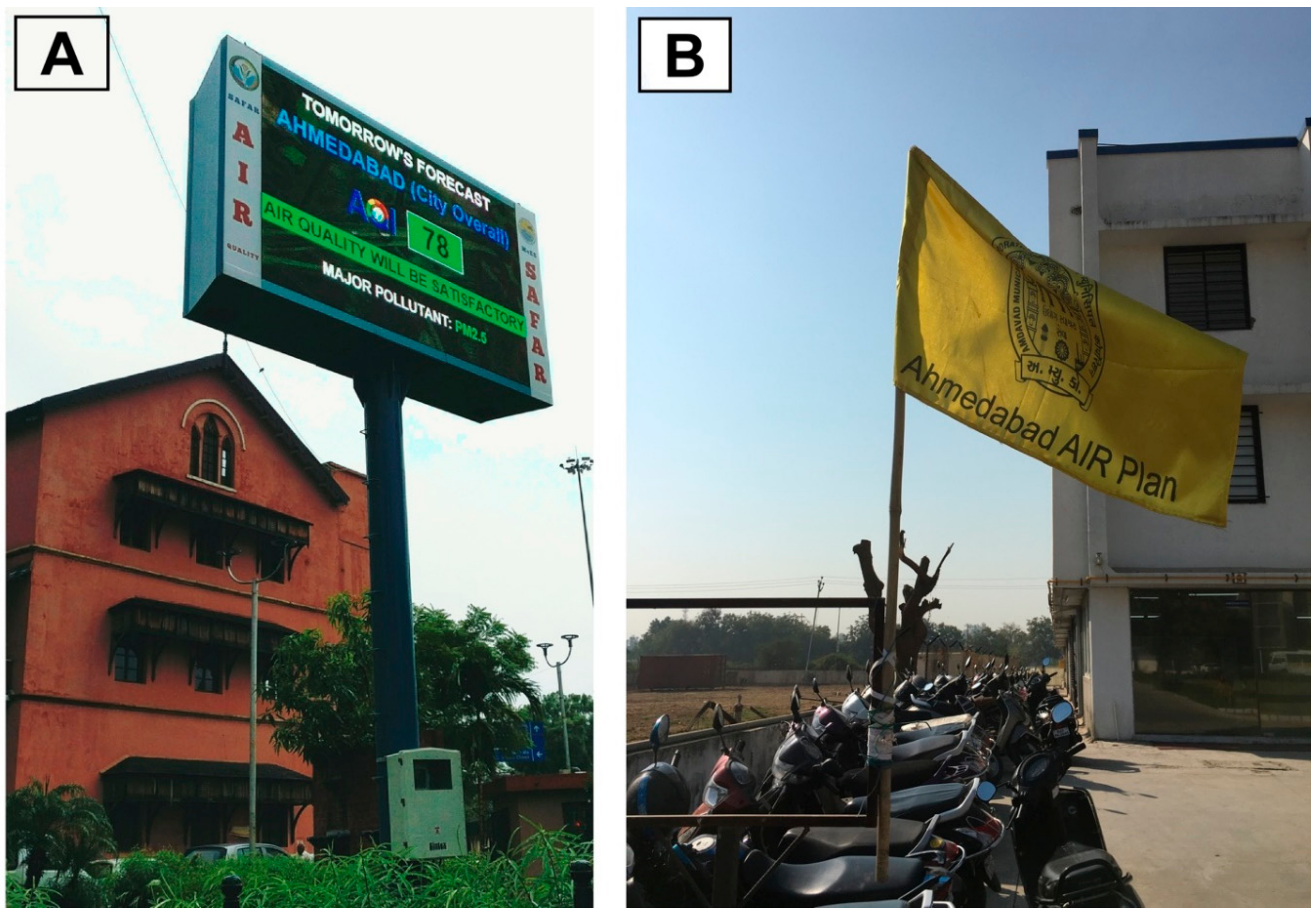
- Enhanced Public Awareness and Communication Outreach—an expansive program that communicates the AQI and protection strategies to local communities through a range of tools, including 12 new LED light board displays, hoardings and billboards; the IITM-SAFAR web portal; cellular phone text messages (SMS) and smartphone mobile application; traditional media engagement; and information, education and communication (IEC) materials translated into the local language (Gujarati).
- Targeted Capacity Building for Medical Professionals—engagement with private and public medical professionals to build awareness of the AQI and promote protection strategies on air pollution [66].
- Supporting Research on Future Exposure Reduction and Mitigation Pathways—application of the AQI for identification of exposure mitigation and pollution source reduction measures by key academic partners from leading local institutes [152].
3.4.1. Piloting a Health-Based AQI through Streamlined Interagency Coordination
3.4.2. Conducting Effective Communication Outreach to Enhance Public Awareness
3.4.3. Activities Focused on Vulnerable Groups
3.4.4. Capacity Building Among Medical Professionals
3.4.5. Initiate Research on Future Exposure Reduction and Mitigation Pathways
3.5. Project Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIR | Ahmedabad Air Information and Response Plan |
| AMC | Ahmedabad Municipal Corporation |
| AQI | Air quality index |
| CPCB | Central Pollution Control Board |
| GPCB | Gujarat Pollution Control Board |
| HAP | Heat Action Plan |
| IEC | Information, education, and communication materials |
| IIPH-G | Indian Institute of Public Health-Gandhinagar |
| IITM-SAFAR | Indian Institute of Tropical Meteorology System of Air Quality and Weather Forecasting and Research |
| IMD | India Meteorological Department |
| MOEFCC | Ministry of Environment, Forests, and Climate Change |
| NAAQS | National Ambient Air Quality Standards |
| NRDC | Natural Resources Defense Council |
| NO2 | Nitrogen dioxide |
| O3 | Ozone |
| PM | Particulate matter |
| PM2.5 | Fine particulate matter, aerodynamic diameter ≤2.5 microns |
| PM10 | Coarse particulate matter, aerodynamic diameter ≤10 microns |
| SO2 | Sulfur dioxide |
| SPCB | State Pollution Control Board |
| U.S. EPA | U.S. Environmental Protection Agency |
| VOCs | Volatile organic compounds |
| WHO | World Health Organization |
References
- Health Effects Institute. State of Global Air. 2018. Available online: https://www.stateofglobalair.org/sites/default/files/soga-2018-report.pdf (accessed on 25 April 2018).
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Lvovsky, K. Economic costs of air pollution with special reference to India. In Proceedings of the National Conference on Health and Environment, Delhi, India, 7–9 July 1998. [Google Scholar]
- Cohen, A.; Anderson, H.R.; Ostro, B.; Pandey, K.; Krzyanowski, M.; Kunzli, N.; Gutschmidt, K.; Pope, C.A.; Romieu, I.; Samet, J.M.; et al. Urban Air Pollution; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Smith, K.R. National burden of disease in India from indoor air pollution. Proc. Natl. Acad. Sci. USA 2000, 97, 13286–13293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brauer, M.; Amann, M.; Burnett, R.T.; Cohen, A.; Dentener, F.; Ezzati, M.; Henderson, S.B.; Krzyzanowski, M.; Martin, R.V.; Van Dingenen, R.; et al. Exposure Assessment for Estimation of the Global Burden of Disease Attributable to Outdoor Air Pollution. Environ. Sci. Technol. 2012, 46, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Effects Institute. Burden of Disease Attributable to Major Air Pollution Sources in India. 2018. Available online: https://www.healtheffects.org/publication/gbd-air-pollution-india (accessed on 28 April 2018).
- World Health Organization. Ambient and Household Air Pollution and Health. 2018. Available online: http://www.who.int/airpollution/data/cities/en/ (accessed on 28 May 2018).
- Health Effects Institute. Burden of Disease: Outdoor Air Pollution among Top Killers. 2013. Available online: https://static01.nyt.com/news/health.pdf (accessed on 22 May 2018).
- Balakrishnan, K.; Cohen, A.; Smith, K.R. Addressing the burden of disease attributable to air pollution in India: The need to integrate across household and ambient air pollution exposures. Environ. Health Perspect. 2014, 122, A6–A7. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Krewski, D.; Burnet, R.T.; Goldberg, M.S.; Hoover, K.; Siemiatycki, J.; Jerrett, M.; Abrahamowicz, M.; White, W.H. Re-Analysis of the Harvard Six-Cities Study and the American Cancer Society Study of Air Pollution and Mortality; Health Effects Institute: Cambridge, MA, USA, 2000. [Google Scholar]
- Samoli, E.; Peng, R.; Ramsay, T.; Pipikou, M.; Touloumi, G.; Dominici, F.; Burnett, R.; Cohen, A.; Krewski, D.; Samet, J.; et al. Acute Effects of Ambient Particulate Matter on Mortality in Europe and North America: Results from the APHENA Study. Environ. Health Perspect. 2008, 116, 1480–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glad, J.A.; Brink, L.L.; Talbott, E.O.; Lee, P.C.; Xu, X.; Saul, M.; Rager, J. The Relationship of Ambient Ozone and PM2. 5 Levels and Asthma Emergency Department Visits: Possible Influence of Gender and Ethnicity. Arch. Environ. Occup. Health 2012, 67, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Burnett, R.T.; Krewski, D.; Jerrett, M.; Shi, Y.; Calle, E.E.; Thun, M.J. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke. Circulation 2009, 120, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Burnett, R.T.; Turner, M.C.; Cohen, A.; Krewski, D.; Jerrett, M.; Gapstur, S.M.; Thun, M.J. Lung Cancer and Cardiovascular Disease Mortality Associated with Ambient Air Pollution and Cigarette Smoke: Shape of the Exposure–Response Relationships. Environ. Health Perspect. 2011, 119, 1616–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krewski, D.; Burnett, R.; Goldberg, M.; Hoover, B.K.; Siemiatycki, J.; Jerrett, M.; Abrahamowicz, M.; White, W. Overview of the reanalysis of the Harvard six cities study and American Cancer Society study of particulate air pollution and mortality. J. Toxicol. Environ. Health Part A 2003, 66, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Davila, S.; Ilić, J.P.; Bešlić, I. Real-time dissemination of air quality information using data streams and Web technologies: Linking air quality to health risks in urban areas/Izvješćivanje o kvaliteti zraka u stvarnom vremenu kontinuiranim prijenosom podataka i web tehnologijama-povezivanje kvalitete zraka sa zdravstvenim rizicima u urbanim sredinama. Arch. Ind. Hyg. Toxicol. 2015, 66, 171–180. [Google Scholar]
- Varghese, K.; Mohan, M.P.R. Air Quality Data Dissemination. Econ. Polit. Wkly. 2017, LII, 25–27. [Google Scholar]
- Natural Resources Defense Council. Clearing the Air: Highlighting Actions on Fighting Air Pollution in India. 2018. Available online: https://www.nrdc.org/sites/default/files/air_pollution_factsheet_final_0.pdf (accessed on 14 March 2018).
- Shooter, D.; Brimblecombe, P. Air quality indexing. Int. J. Environ. Pollut. 2008, 36, 305–323. [Google Scholar] [CrossRef]
- Mintz, D. Technical Assistance Document for the Reporting of Daily Air Quality-the Air Quality Index (AQI); U.S. Environmental Protection Agency, Office of Air Quality Planning and Standards: Research Triangle Park, NC, USA, 2009. [Google Scholar]
- Chen, H.; Li, Q.; Kaufman, J.S.; Wang, J.; Copes, R.; Su, Y.; Benmarhnia, T. Effect of air quality alerts on human health: A regression discontinuity analysis in Toronto, Canada. Lancet Planet. Health 2018, 2, e19–e26. [Google Scholar] [CrossRef]
- Ministry of Health and Family Welfare. Report of the Steering Committee on Air Pollution and Health-Related Issues. 2015. Available online: https://mohfw.gov.in/sites/default/files/5412023661450432724_0.pdf (accessed on 20 March 2018).
- Gujarat Pollution Control Board (GPCB). About Board. 2014. Available online: http://www.gpcb.gov.in/About-Board1.htm (accessed on 30 April 2018).
- Ministry of Environment, Forests, and Climate Change (MOEFCC). National Clean Air Programme (NCAP)—India. 2018. Available online: http://envfor.nic.in/sites/default/files/NCAP%20with%20annex-ilovepdf-compressed.pdf (accessed on 8 May 2018).
- Pal, S. This Indian City Is Taking Huge Steps to Protect Its Residents From Dangerous Air Pollution Levels. Available online: https://www.thebetterindia.com/91336/ahmedabad-air-information-response-plan-pollution/ (accessed on 25 June 2018).
- Patil, M. India’s First Early Warning System in Ahmedabad Aims to Reduce Health Impact of Air Pollution. Available online: https://www.hindustantimes.com/india-news/india-s-first-early-warning-system-in-ahmedabad-aims-to-reduce-health-impact-of-air-pollution/story-P3pvXMd9BmWmYF4M53yxuI.html (accessed on 25 June 2018).
- Beinecke, F. How One Indian City is Taking on air Pollution. Available online: https://www.greenbiz.com/article/how-one-indian-city-taking-air-pollution (accessed on 25 June 2018).
- Purohit, P.; Amann, M.; Mathur, R.; Gupta, I.; Marwah, S.; Verma, V.; Bertok, I.; Borken-Kleefeld, J.; Chambers, A.; Cofala, J.; et al. GAINS-Asia. Scenarios for Cost-Effective Control of Air Pollution and Greenhouse Gases in India; International Institute for Applied Systems Analysis (IIASA): Laxenburg, Austria, 2010. [Google Scholar]
- Smith, K.R.; Frumkin, H.; Balakrishnan, K.; Butler, C.D.; Chafe, Z.A.; Fairlie, I.; Kinney, P.; Kjellstrom, T.; Mauzerall, D.L.; McKone, T.E.; et al. Energy and Human Health. Annu. Rev. Public Health 2013, 34, 159–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Environmental Protection Agency. The Clean Air Act and the Economy. Available online: https://www.epa.gov/clean-air-act-overview/clean-air-act-and-economy (accessed on 25 June 2018).
- Zhao, Y.; Wang, S.; Duan, L.; Lei, Y.; Cao, P.; Hao, J. Primary air pollutant emissions of coal-fired power plants in China: Current status and future prediction. Atmos. Environ. 2008, 42, 8442–8452. [Google Scholar] [CrossRef]
- Kandlikar, M.; Ramachandran, G. The causes and consequences of particulate air pollution in urban India: A synthesis of the science. Annu. Rev. Energy Environ. 2000, 25, 629–684. [Google Scholar] [CrossRef]
- Patz, J.A.; West, J.J. The Paris Agreement could saves lives in China. Lancet Planet. Health 2018, 2, e147–e148. [Google Scholar] [CrossRef]
- Pucher, J.; Korattyswaropam, N.; Mittal, N.; Ittyerah, N. Urban transport crisis in India. Transp. Policy 2005, 12, 185–198. [Google Scholar] [CrossRef]
- Pucher, J.; Peng, Z.; Mittal, N.; Zhu, Y.; Korattyswaroopam, N. Urban transport trends and policies in China and India: Impacts of rapid economic growth. Transp. Rev. 2007, 27, 379–410. [Google Scholar] [CrossRef]
- Verma, M. Growing car ownership and dependence in India and its policy implications. Case Stud. Transp. Policy 2015, 3, 304–310. [Google Scholar] [CrossRef]
- Health Effects Institute. Traffic-Related Air Pollution: A Critical Review of the Literature on Emissions, Exposure, and Health Effects; Panel on the Health Effects of Traffic-Related Air Pollution; Health Effects Institute: Cambridge, MA, USA, 2010. [Google Scholar]
- York Bigazzi, A.; Rouleau, M. Can traffic management strategies improve urban air quality? A review of the evidence. J. Transp. Health 2017, 7, 111–124. [Google Scholar] [CrossRef]
- Pandey, A.; Venkataraman, C. Estimating emissions from the Indian transport sector with on-road fleet composition and traffic volume. Atmos. Environ. 2014, 98, 123–133. [Google Scholar] [CrossRef]
- Chaturvedi, V.; Kim, S.H. Long term energy and emission implications of a global shift to electricity-based public rail transportation system. Energy Policy 2015, 81, 176–185. [Google Scholar] [CrossRef]
- Tiwari, G. Urban transport priorities: Meeting the challenge of socio-economic diversity in cities, a case study of Delhi, India. Cities 2002, 19, 95–103. [Google Scholar] [CrossRef]
- Woodcock, J.; Edwards, P.; Tonne, C.; Armstrong, B.G.; Ashiru, O.; Banister, D.; Beevers, S.; Chalabi, Z.; Chowdhury, Z.; Cohen, A. Public health benefits of strategies to reduce greenhouse-gas emissions: Urban land transport. Lancet 2009, 374, 1930. [Google Scholar] [CrossRef]
- Singh, S.K. Review of urban transportation in India. J. Public Transp. 2005, 8, 5. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Horowitz, L.W.; Tong, D.Q.; West, J.J. An Estimate of the Global Burden of Anthropogenic Ozone and Fine Particulate Matter on Premature Human Mortality Using Atmospheric Modeling. Environ. Health Perspect. 2010, 118, 1189–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Ozone and short-term mortality in 95 US urban communities, 1987–2000. JAMA J. Am. Med. Assoc. 2004, 292, 2372–2378. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Walker, J.; Samet, J.M.; Zeger, S.L.; Dominici, F. Seasonal and regional short-term effects of fine particles on hospital admissions in 202 US counties, 1999–2005. Am. J. Epidemiol. 2008, 168, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Jacob, D.J.; Winner, D.A. Effect of climate change on air quality. Atmos. Environ. 2009, 43, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Central Pollution Control Board (CPCB). About National Air Quality Index. Available online: http://cpcb.nic.in/About_AQI.pdf (accessed on 24 April 2018).
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar] [PubMed]
- Snider, G.; Carter, E.; Clark, S.; Yang, X.; Ezzati, M.; Schauer, J.J.; Wiedinmyer, C.; Baumgartner, J. Impacts of stove use patterns and outdoor air quality on household air pollution and cardiovascular mortality in southwestern China. Environ. Int. 2018, 117, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Azhar, G.S.; Mavalankar, D.; Nori-Sarma, A.; Rajiva, A.; Dutta, P.; Jaiswal, A.; Sheffield, P.; Knowlton, K.; Hess, J.J. Heat-related mortality in India: Excess all-cause mortality associated with the 2010 Ahmedabad heat wave. PLoS ONE 2014, 9, e91831. [Google Scholar] [CrossRef] [PubMed]
- Luber, G.; McGeehin, M. Climate Change and Extreme Heat Events. Am. J. Prev. Med. 2008, 35, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, K. National Energy Map for India: Technology Vision 2030 Summary for Policy-Makers; The Energy and Resources Institute (TERI): New Delhi, India, 2003. [Google Scholar]
- Abel, D.W.; Holloway, T.; Harkey, M.; Meier, P.; Ahl, D.; Limaye, V.S.; Patz, J.A. Air-quality-related health impacts from climate change and from adaptation of cooling demand for buildings in the eastern United States: An interdisciplinary modeling study. PLoS Med. 2018, 15, e1002599. [Google Scholar] [CrossRef] [PubMed]
- Dahl, R. Cooling concepts: Alternatives to air conditioning for a warm world. Environ. Health Perspect. 2013, 121, a18. [Google Scholar] [CrossRef] [PubMed]
- Sivak, M. Potential energy demand for cooling in the 50 largest metropolitan areas of the world: Implications for developing countries. Energy Policy 2009, 37, 1382–1384. [Google Scholar] [CrossRef]
- Knowlton, K.; Kulkarni, S.P.; Azhar, G.S.; Mavalankar, D.; Jaiswal, A.; Connolly, M.; Nori-Sarma, A.; Rajiva, A.; Dutta, P.; Deol, B. Development and implementation of South Asia’s first heat-health action plan in Ahmedabad (Gujarat, India). Int. J. Environ. Res. Public. Health 2014, 11, 3473–3492. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.K. Heat Wave (A Silent Disaster); National Disaster Management Authority (NDMA): New Delhi, India, 2017. [Google Scholar]
- Jaiswal, A. Air Pollution & Health: Preparing for Ahmedabad’s AQI. 2016. Available online: https://www.nrdc.org/experts/anjali-jaiswal/air-pollution-health-preparing-ahmedabads-aqi (accessed on 24 April 2018).
- Jaiswal, A. It’s Not Just Delhi, Air Pollution Is a Threat across India. 2017. Available online: https://www.nrdc.org/experts/anjali-jaiswal/its-not-just-delhi-air-pollution-threat-across-india (accessed on 24 April 2018).
- Natural Resources Defense Council. Issue Brief: Protecting Health from Increasing Air Pollution in Ahmedabad. 2017. Available online: https://www.nrdc.org/sites/default/files/ahmedabad_aqi_-_final.pdf (accessed on 24 April 2018).
- Guttikunda, S.K.; Goel, R.; Pant, P. Nature of air pollution, emission sources, and management in the Indian cities. Atmos. Environ. 2014, 95, 501–510. [Google Scholar] [CrossRef]
- Wen, X.-J.; Balluz, L.; Mokdad, A. Association between Media Alerts of Air Quality Index and Change of Outdoor Activity Among Adult Asthma in Six States, BRFSS, 2005. J. Community Health 2009, 34, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Suresh, Y.; Devi, M.M.S.; Manjari, V.; Das, U.N. Oxidant stress, antioxidants and nitric oxide in traffic police of Hyderabad, India. Environ. Pollut. 2000, 109, 321–325. [Google Scholar] [CrossRef]
- Apte, J.S.; Kirchstetter, T.W.; Reich, A.H.; Deshpande, S.J.; Kaushik, G.; Chel, A.; Marshall, J.D.; Nazaroff, W.W. Concentrations of fine, ultrafine, and black carbon particles in auto-rickshaws in New Delhi, India. Atmos. Environ. 2011, 45, 4470–4480. [Google Scholar] [CrossRef]
- Bateson, T.F.; Schwartz, J. Children’s response to air pollutants. J. Toxicol. Environ. Health A 2007, 71, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Khafaie, M.A.; Salvi, S.S.; Yajnik, C.S.; Ojha, A.; Khafaie, B.; Gore, S.D. Air pollution and respiratory health among diabetic and non-diabetic subjects in Pune, India—Results from the Wellcome Trust Genetic Study. Environ. Sci. Pollut. Res. 2017, 24, 15538–15546. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, K.; Ghosh, S.; Thangavel, G.; Sambandam, S.; Mukhopadhyay, K.; Puttaswamy, N.; Sadasivam, A.; Ramaswamy, P.; Johnson, P.; Kuppuswamy, R. Exposures to fine particulate matter (PM 2.5) and birthweight in a rural-urban, mother-child cohort in Tamil Nadu, India. Environ. Res. 2018, 161, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, A. Back to Basics: Clean Air in India. 2017. Available online: https://www.nrdc.org/experts/anjali-jaiswal/back-basics-clean-air-india (accessed on 24 April 2018).
- Beinecke, F. Ahmedabad, India: Protecting the Most Vulnerable from Dangerous Air Pollution. 2017. Available online: https://www.nrdc.org/experts/frances-beinecke/ahmedabad-india-protecting-most-vulnerable-dangerous-air-pollution (accessed on 24 April 2018).
- World Health Organization. Health and Environment: Communicating the Risks. 2013. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/233759/e96930.pdf (accessed on 25 April 2018).
- US Environmental Protection Agency. Air Quality Index: A Guide to Air Quality and Your Health. Available online: https://www3.epa.gov/airnow/aqi_brochure_02_14.pdf (accessed on 3 March 2018).
- Indian Ministry of Environment, Forests, and Climate Change (MOEFCC). The Air (Prevention and Control of Pollution) Act. 1981. Available online: http://www.moef.nic.in/legis/air/air1.html (accessed on 2 March 2018).
- Indian Ministry of Environment, Forests, and Climate Change (MOEFCC). Consideration of Projects for Environmental Clearance Based on Comprehensive Environmental Pollution Index; MOEFCC: New Delhi, India, 2010.
- Central Pollution Control Board (CPCB). Annual Report. Available online: http://cpcbnicin/upload/AnnualReports/AnnualReport_55_Annual_Report_2014-15pdf (accessed on 29 April 2018).
- Central Pollution Control Board (CPCB). Comprehensive Industry Document with Emission Standards, Guidelines and Stack Height Regulation for Vertical Shaft Brick Kilns (VSBK) vis-à-vis Pollution Control Measures; Central Pollution Control Board (CPCB): New Delhi, India, 2007. [Google Scholar]
- Central Pollution Control Board (CPCB). Air Quality Monitoring, Emission Inventory and Source Apportionment Study for Indian Cities: National Summary Report; Central Pollution Control Board (CPCB): New Delhi, India, 2011; Available online: http://www.moef.nic.in/downloads/public-information/Rpt-air-monitoring-17-01-2011.pdf (accessed on 25 May 2018).
- Central Pollution Control Board (CPCB). National Ambient Air Quality Status & Trends in India-2010; Central Pollution Control Board (CPCB): New Delhi, India, 2012; Available online: http://cpcb.nic.in/openpdffile.php?id=UHVibGljYXRpb25GaWxlLzYyOF8xNDU3NTA1MzkxX1B1YmxpY2F0aW9uXzUyMF9OQUFRU1RJLnBkZg== (accessed on 25 May 2018).
- Central Pollution Control Board (CPCB). Ambient Air Quality Data at various locations in the country. Available online: http://www.cpcb.gov.in/CAAQM/frmUserAvgReportCriteria.aspx (accessed on 25 May 2018).
- Guttikunda, S.K.; Jawahar, P. Application of SIM-air Modeling Tools to Assess Air Quality in Indian Cities. Atmos. Environ. 2012, 62, 551–561. [Google Scholar] [CrossRef]
- Kumar, R.; Nagar, J.K.; Kumar, H.; Kushwah, A.S.; Meena, M.; Kumar, P.; Raj, N.; Singhal, M.K.; Gaur, S.N. Association of Indoor and Outdoor Air Pollutant Level With Respiratory Problems Among Children in an Industrial Area of Delhi, India. Arch. Environ. Occup. Health 2007, 62, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Hansen, M.L.; Long, R.W.; Nielsen, K.R.; Eatough, N.L.; Wilson, W.E.; Eatough, D.J. Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ. Health Perspect. 2004, 112, 339. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M. South Asians and Cardiovascular Risk: What Clinicians Should Know. Circulation 2006, 113, e924–e929. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.; Dey, S. Cause-specific premature death from ambient PM2.5 exposure in India: Estimate adjusted for baseline mortality. Environ. Int. 2016, 91, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Gong Jr, H.; Bailar, J.C.; Ford, J.G.; Gold, D.R.; Lambert, W.E.; Utell, M.J. Air pollution health risks: Do class and race matter? Toxicol. Ind. Health 1993, 9, 843–878. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, P.; Smith, K.R.; Joffe, M.; Haines, A. A global perspective on energy: Health effects and injustices. The Lancet 2007, 370, 965–978. [Google Scholar] [CrossRef]
- Ingle, S.T.; Pachpande, B.G.; Wagh, N.D.; Patel, V.S.; Attarde, S.B. Exposure to vehicular pollution and respiratory impairment of traffic policemen in Jalgaon City, India. Ind. Health 2005, 43, 656–662. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency. Air Quality Index (AQI) Basics. Available online: https://airnow.gov/index.cfm?action=aqibasics.aqi (accessed on 3 March 2018).
- US Environmental Protection Agency. Risk Communication in Action: Environmental Case Studies; US Environmental Protection Agency: Washington, DC, USA, 2002. Available online: https://cfpub.epa.gov/si/si_public_record_Report.cfm?dirEntryID=64244 (accessed on 4 March 2018).
- Oltra, C.; Sala, R. Communicating the risks of urban air pollution to the public. A study of urban air pollution information services. Rev. Int. Contam. Ambient. 2015, 31, 361–375. [Google Scholar]
- World Meteorological Organization. GAW Report No. 217, System of Air Quality and Weather Forecasting and Research (SAFAR-India); World Meteorological Organization: Geneva, Switzerland, 2015. [Google Scholar]
- SAFAR. System of Air Quality and Weather Forecasting and Research in metropolitan cities like Delhi. Available online: http://niti.gov.in/writereaddata/files/bestpractices/SAFAR%20System%20of%20Air%20quality%20Forecasting%20And%20Research%20in%20metropolitan%20cities%20like%20Delhi.pdf (accessed on 2 March 2018).
- Millman, A.; Tang, D.; Perera, F.P. Air pollution threatens the health of children in China. Pediatrics 2008, 122, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Siddique, S.; Ray, M.R.; Lahiri, T. Effects of air pollution on the respiratory health of children: A study in the capital city of India. Air Qual. Atmosphere Health 2011, 4, 95–102. [Google Scholar] [CrossRef]
- Central Pollution Control Board (CPCB). Study on Ambient Air Quality, Respiratory Symptoms and Lung Function of Children in Delhi; CPCB: Delhi, India, 2012. Available online: http://cpcb.nic.in/openpdffile.php?id=UmVwb3J0RmlsZXMvMzNfMTQ1ODEyNzM4OV9OZXdJdGVtXzE5MV9TdHVkeUFpclF1YWxpdHkucGRm (accessed on 24 April 2018).
- Shendell, D.G.; Rawling, M.-M.; Bohlke, A.; Edwards, B.; Rico, S.A.; Felix, J.; Eaton, S.; Moen, S.; Roberts, E.M.; Love, M.M. The outdoor air quality flag program in central California: A school-based educational intervention to potentially help reduce children’s exposure to environmental asthma triggers. J. Environ. Health 2007, 70, 28. [Google Scholar] [PubMed]
- Kaur, N. Flagging Air Pollution for School Children in Ahmedabad. 2017. Available online: https://www.nrdc.org/experts/nehmat-kaur/flagging-air-pollution-school-children-ahmedabad (accessed on 24 April 2018).
- Chen, R.; Wang, X.; Meng, X.; Hua, J.; Zhou, Z.; Chen, B.; Kan, H. Communicating air pollution-related health risks to the public: An application of the Air Quality Health Index in Shanghai, China. Environ. Int. 2013, 51, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Tushar Sheth, J.; Patel, K.; Shah, D. Solid Waste Management: A Case Study of Ahmedabad. In Proceedings of the Habitat Conclave 2016, Ahmedabad, India, 18–21 February 2016. [Google Scholar]
- Dutta, S. Nearing 35 Years, Ahmedabad’s Pirana Landfill Is Infamous for Its Garbage Mountains and Frequent Fires. Available online: https://swachhindia.ndtv.com/nearing-35-years-ahmedabads-pirana-landfill-is-infamous-for-its-garbage-mountains-and-frequent-fires-11855/ (accessed on 25 June 2018).
- Central Pollution Control Board (CPCB). National Ambient Air Quality Standards. Available online: http://cpcb.nic.in/air-quality-standard/ (accessed on 7 March 2018).
- US Environmental Protection Agency. National Ambient Air Quality Standards for Particulate Matter. Fed. Regist. 2012, 78, 3086–3274. [Google Scholar]
- World Health Organization. Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide; World Health Organization: Copenhagen, Denmark, 2006; ISBN 978-92-890-2192-0. [Google Scholar]
- Dey, S.; Di Girolamo, L.; van Donkelaar, A.; Tripathi, S.; Gupta, T.; Mohan, M. Variability of outdoor fine particulate (PM 2.5) concentration in the Indian subcontinent: A remote sensing approach. Remote Sens. Environ. 2012, 127, 153–161. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Urban Ambient Air Pollution Database (Update 2016). Available online: http://www.who.int/phe/health_topics/outdoorair/databases/cities/en/ (accessed on 24 April 2018).
- World Health Organization. Global Health Observatory Data Repository: Ambient (Outdoor) Air Pollution Database, by Country and City; WHO: Geneva, Switzerland, 2014. Available online: http://www.who.int/phe/health_topics/outdoorair/databases/cities-2014/en/ (accessed on 25 April 2018).
- Health Effects Institute. International Scientific Oversight Committee Outdoor Air Pollution and Health in the Developing Countries of Asia: A Comprehensive Review; Special Report 18; Health Effects Institute: Cambridge, MA, USA, 2010. [Google Scholar]
- Central Pollution Control Board (CPCB). NAQI Status of Indian Cities in 2015-16. 2016. Available online: http://cpcb.nic.in/cpcbold/upload/Latest/Latest_119_NAQI-StatusIndianCities-2015-16.pdf (accessed on 26 April 2018).
- Guttikunda, S. It’s About Time We Got Smarter about Monitoring Our Air Pollution. Available online: https://thewire.in/environment/air-pollution-monitoring-diwali-pm2-5-pm10-cpcb-namp (accessed on 25 June 2018).
- Gujarat Pollution Control Board (GPCB). Ambient Air Quality Monitoring Programmes. Available online: https://gpcb.gujarat.gov.in/webcontroller/page/ambient-air-quality-monitoring-programmes (accessed on 24 April 2018).
- Gujarat Pollution Control Board (GPCB). Ambient Air Quality Monitoring Programme (AAQM). Available online: https://www.gpcb.gov.in/ambient-air-quality-monitoring-programme.htm#link1 (accessed on 24 April 2018).
- Central Pollution Control Board (CPCB). About NAMP. Available online: http://cpcb.nic.in/about-namp/ (accessed on 27 June 2018).
- Central Pollution Control Board (CPCB). Guidelines for the Measurement of Ambient Air Pollutants, Volume-I (National Ambient Air Quality Series: NAAQMS/36/2012-13). Available online: http://cpcb.nic.in/openpdffile.php?id=UmVwb3J0RmlsZXMvMjdfMTQ1ODExMDQyNl9OZXdJdGVtXzE5Nl9OQUFRTVNfVm9sdW1lLUkucGRm (accessed on 27 June 2018).
- Gujarat Pollution Control Board (GPCB). Annual Report 2014-15. Available online: https://gpcb.gov.in/pdf/AR_2014_15_ENG.PDF (accessed on 27 June 2018).
- Central Pollution Control Board (CPCB). Current Air Pollution Levels. Available online: http://www.cpcb.gov.in/caaqm/frmCurrentDataNew.aspx?StationName=Maninagar&StateId=8&CityId=337 (accessed on 27 June 2018).
- Central Pollution Control Board (CPCB). Real-time Air Quality Data. Available online: http://cpcb.nic.in/real-time-air-quality-data/ (accessed on 27 June 2018).
- Mukherjee, S.; Chakraborty, D. Environmental Scenario in India: Successes and Predicaments; Routledge: New York, NY, USA, 2013; ISBN 1-136-48866-9. [Google Scholar]
- Guttikunda, S.K.; Goel, R. Health impacts of particulate pollution in a megacity—Delhi, India. Environ. Dev. 2013, 6, 8–20. [Google Scholar] [CrossRef]
- Amann, M.; Bertok, I.; Borken, J.; Chambers, A.; Cofala, J.; Dentener, F.; Heyes, C.; Kejun, J.; Klimont, Z.; Makowski, M.; et al. GAINS-Asia. A Tool to Combat Air Pollution and Climate Change Simultaneously; International Institute for Applied Systems Analysis (IIASA): Laxenburg, Austria, 2008. [Google Scholar]
- World Bank. What is Causing Particulate Air Pollution? Evidence from Delhi, Kolkata, and Mumbai; South Asia Urban Air Quality Management Briefing Note No. 14; World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Lepeule, J.; Laden, F.; Dockery, D.; Schwartz, J. Chronic Exposure to Fine Particles and Mortality: An Extended Follow-up of the Harvard Six Cities Study from 1974 to 2009. Environ. Health Perspect. 2012, 120, 965–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dholakia, H.H.; Purohit, P.; Rao, S.; Garg, A. Impact of current policies on future air quality and health outcomes in Delhi, India. Atmos. Environ. 2013, 75, 241–248. [Google Scholar] [CrossRef]
- Kushwaha, R.; Lal, H.; Srivastava, A.; Jain, V.K. Human Exposure to Particulate Matter and Their Risk Assessment over Delhi, India. Natl. Acad. Sci. Lett. 2012, 35, 497–504. [Google Scholar] [CrossRef]
- Magsumbol, M.S.; Singh, A.; Ghosh, A.; Kler, N.; Garg, P. Association of air pollution on birth outcomes in New Delhi—A pilot study on the potential of HMIS data for environmental public health tracking. Indian J. Med. Inform. 2016, 8, 52–56. [Google Scholar]
- Jain, V.; Dey, S.; Chowdhury, S. Ambient PM 2.5 exposure and premature mortality burden in the holy city Varanasi, India. Environ. Pollut. 2017, 226, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Maji, S.; Ahmed, S.; Siddiqui, W.A.; Ghosh, S. Short term effects of criteria air pollutants on daily mortality in Delhi, India. Atmos. Environ. 2017, 150, 210–219. [Google Scholar] [CrossRef]
- Samiksha, S.; Sunder Raman, R.; Nirmalkar, J.; Kumar, S.; Sirvaiya, R. PM 10 and PM 2.5 chemical source profiles with optical attenuation and health risk indicators of paved and unpaved road dust in Bhopal, India. Environ. Pollut. 2017, 222, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Tonne, C.; Salmon, M.; Sanchez, M.; Sreekanth, V.; Bhogadi, S.; Sambandam, S.; Balakrishnan, K.; Kinra, S.; Marshall, J.D. Integrated assessment of exposure to PM 2.5 in South India and its relation with cardiovascular risk: Design of the CHAI observational cohort study. Int. J. Hyg. Environ. Health 2017, 220, 1081–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Jayaraman, G.; Anand, S.; Marimuthu, P. Assessing respiratory morbidity through pollution status and meteorological conditions for Delhi. Environ. Monit. Assess. 2006, 114, 489–504. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Mangal, A.; Satsangi, A.; Lakhani, A.; Maharaj Kumari, K. Characterization, sources and health risk analysis of PM 2.5 bound metals during foggy and non-foggy days in sub-urban atmosphere of Agra. Atmospheric Res. 2017, 197, 121–131. [Google Scholar] [CrossRef]
- Joshi, P.; Islam, S.; Pais, P.; Reddy, S.; Dorairaj, P.; Kazmi, K.; Pandey, M.R.; Haque, S.; Mendis, S.; Rangarajan, S. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA J. Am. Med. Assoc. 2007, 297, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Duong, M.; Islam, S.; Rangarajan, S.; Teo, K.; O’Byrne, P.M.; Schünemann, H.J.; Igumbor, E.; Chifamba, J.; Liu, L.; Li, W.; et al. Global differences in lung function by region (PURE): An international, community-based prospective study. Lancet Respir. Med. 2013, 1, 599–609. [Google Scholar] [CrossRef]
- Fulambarker, A. Comparison of Pulmonary Function in Immigrant vs US-Born Asian Indians. CHEST J. 2010, 137, 1398. [Google Scholar] [CrossRef] [PubMed]
- Environnement SA. MP101M—Continuous, Automatic PM10, PM2.5, PM1, TSP Particulate Monitor. Available online: http://www.environnement-sa.com/products-page/en/air-quality-monitoring-en/mp101m-continuous-automatic-pm10-pm2-5-pm1-tsp-particulate-monitor/ (accessed on 30 May 2018).
- International Organization for Standardization. ISO 10473:2000—Ambient Air—Measurement of the Mass of Particulate Matter on a Filter Medium—Beta-ray Absorption Method. Available online: https://www.iso.org/standard/32943.html (accessed on 30 May 2018).
- SAFAR—India. Forecast Modelling and Supercomputing. Available online: http://safar.tropmet.res.in/FORECASTING-46-4-Details (accessed on 2 April 2018).
- State Department of the United States. Air Quality Data Information. Available online: https://in.usembassy.gov/air-quality-data-information/ (accessed on 22 April 2018).
- State Department of the United States. Air Quality Awareness Week: Using Data and Partnerships. Available online: https://blogs.state.gov/stories/2018/05/02/en/air-quality-awareness-week-using-data-and-partnerships (accessed on 22 April 2018).
- State Department of the United States. Air Quality Data | U.S. Embassy & Consulates in India. Available online: https://in.usembassy.gov/embassy-consulates/new-delhi/air-quality-data/ (accessed on 23 April 2018).
- Li, S.; Feng, K.; Li, M. Identifying the main contributors of air pollution in Beijing. J. Clean. Prod. 2017, 163, S359–S365. [Google Scholar] [CrossRef]
- Fang, M.; Chan, C.K.; Yao, X. Managing air quality in a rapidly developing nation: China. Atmos. Environ. 2009, 43, 79–86. [Google Scholar] [CrossRef]
- Cai, H.; Xie, S. Traffic-related air pollution modeling during the 2008 Beijing Olympic Games: The effects of an odd-even day traffic restriction scheme. Sci. Total Environ. 2011, 409, 1935–1948. [Google Scholar] [CrossRef] [PubMed]
- South Coast Air Quality Management District. Current Air Quality Data and Forecasts. Available online: http://www.aqmd.gov/home/air-quality/air-quality-data-studies (accessed on 26 May 2018).
- World Health Organization. Urban Air Pollution in Megacities of the World; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Davis, L.W. The effect of driving restrictions on air quality in Mexico City. J. Polit. Econ. 2008, 116, 38–81. [Google Scholar] [CrossRef]
- Jaiswal, A. Health First: Ahmedabad’s Groundbreaking AIR Plan. 2017. Available online: https://www.nrdc.org/experts/anjali-jaiswal/health-first-ahmedabads-groundbreaking-air-plan (accessed on 24 April 2018).
- Natural Resources Defense Council. Ahmedabad Information and Response (AIR) Plan. 2017. Available online: https://www.nrdc.org/sites/default/files/ahmedabad_air_plan_feb_2017_final_pdf.pdf (accessed on 24 April 2018).
- Limaye, V.S. Ahmedabad’s AIR Plan, from Classrooms to the Community. 2018. Available online: https://www.nrdc.org/experts/vijay-limaye/ahmedabads-air-plan-classrooms-community (accessed on 18 April 2018).
- Sagar, A.; Balakrishnan, K.; Guttikunda, S.; Roychowdhury, A.; Smith, K.R. India Leads the Way: A Health-Centered Strategy for Air Pollution. Environ. Health Perspect. 2016, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.; Maheshwari, M.; Sengupta, B.; Shukla, B. Design of a website for dissemination of air quality index in India. Environ. Model. Softw. 2003, 18, 405–411. [Google Scholar] [CrossRef]
- World Bank. World Development Report 2016; World Dev. Rep. 359; World Bank: Washington, DC, USA, 2016. [Google Scholar]
- Kakkad, K.; Barzaga, M.L.; Wallenstein, S.; Azhar, G.S.; Sheffield, P.E. Neonates in Ahmedabad, India, during the 2010 heat wave: A climate change adaptation study. J. Environ. Public Health 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Gulia, S.; Shiva Nagendra, S.M.; Khare, M.; Khanna, I. Urban air quality management-A review. Atmospheric Pollut. Res. 2015, 6, 286–304. [Google Scholar] [CrossRef]
- Indian Institute of Tropical Meteorology. Emission Inventory of Ahmedabad (SAFAR-India). 2017. Available online: http://assets.nrdc.org/sites/default/files/media-uploads/safar-ahmedabad-ei-2017-full_report.pdf (accessed on 5 April 2018).
- Limaye, V.; Sarkar, S. Ahmedabad’s New Air Quality Monitors Advance Public Health. 2018. Available online: https://www.nrdc.org/experts/vijay-limaye/new-monitoring-air-quality-ahmedabad-protects-health (accessed on 27 May 2018).
- Mohan, M.; Kandya, A. An analysis of the annual and seasonal trends of air quality index of Delhi. Environ. Monit. Assess. 2007, 131, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Gurjar, B.R.; Ravindra, K.; Nagpure, A.S. Air pollution trends over Indian megacities and their local-to-global implications. Atmos. Environ. 2016, 142, 475–495. [Google Scholar] [CrossRef]
- Patel, L. With 18 New ‘Green Lungs’, Amdavadis to Breathe Easy. Available online: https://ahmedabadmirror.indiatimes.com/ahmedabad/cover-story/with-18-new-green-lungs-amdavadis-to-breathe-easy/articleshow/64714989.cms (accessed on 26 June 2018).
- Grote, R.; Samson, R.; Alonso, R.; Amorim, J.H.; Cariñanos, P.; Churkina, G.; Fares, S.; Thiec, D.L.; Niinemets, Ü.; Mikkelsen, T.N. Functional traits of urban trees: Air pollution mitigation potential. Front. Ecol. Environ. 2016, 14, 543–550. [Google Scholar] [CrossRef]
- Fusaro, L.; Marando, F.; Sebastiani, A.; Capotorti, G.; Blasi, C.; Copiz, R.; Congedo, L.; Munafò, M.; Ciancarella, L.; Manes, F. Mapping and Assessment of PM10 and O3 Removal by Woody Vegetation at Urban and Regional Level. Remote Sens. 2017, 9, 791. [Google Scholar] [CrossRef]
- Stone, B.; Hess, J.J.; Frumkin, H. Urban Form and Extreme Heat Events: Are Sprawling Cities More Vulnerable to Climate Change Than Compact Cities? Environ. Health Perspect. 2010, 118, 1425–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, K.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of Wisconsin. Int. J. Environ. Res. Public. Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public. Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Curtis, A.; Helmig, D.; Baroch, C.; Daly, R.; Davis, S. Biogenic volatile organic compound emissions from nine tree species used in an urban tree-planting program. Atmos. Environ. 2014, 95, 634–643. [Google Scholar] [CrossRef]
- Dholakia, H.H.; Bhadra, D.; Garg, A. Short term association between ambient air pollution and mortality and modification by temperature in five Indian cities. Atmos. Environ. 2014, 99, 168–174. [Google Scholar] [CrossRef]
- Central Pollution Control Board (CPCB). Epidemiological Study on Effect of Air Pollution on Human Health (Adults) in Delhi; CPCB: Delhi, India, 2012; Available online: http://cpcb.nic.in/openpdffile.php?id=UmVwb3J0RmlsZXMvMzRfMTQ1ODEyOTEzMV9OZXdJdGVtXzE4OF9FcGlkZW1pb2xvZ2ljYWxfc3R1ZHlfQVBfUmVwb3J0LnBkZg== (accessed on 24 April 2018).
- Kumar, N.; Chu, A.; Foster, A. An empirical relationship between PM2.5 and aerosol optical depth in Delhi Metropolitan. Atmos. Environ. 2007, 41, 4492–4503. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Sharma, S.K.; Thakur, J.; Lakshmi, P.; Sharma, M.; Singh, T. Association of air pollution and mortality in the Ludhiana city of India: a time-series study. Indian J. Public Health 2010, 54, 98. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Dockery, D.W. Health Effects of Fine Particulate Air Pollution: Lines that Connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šrám, R.J.; Binková, B.; Dejmek, J.; Bobak, M. Ambient air pollution and pregnancy outcomes: A review of the literature. Environ. Health Perspect. 2005, 113, 375. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Perera, F. Pollution from Fossil-Fuel Combustion is the Leading Environmental Threat to Global Pediatric Health and Equity: Solutions Exist. Int. J. Environ. Res. Public. Health 2017, 15, 16. [Google Scholar] [CrossRef] [PubMed]
- Gupta, U. Valuation of urban air pollution: A case study of Kanpur City in India. Environ. Resour. Econ. 2008, 41, 315–326. [Google Scholar] [CrossRef]
- Etchie, T.O.; Sivanesan, S.; Adewuyi, G.O.; Krishnamurthi, K.; Rao, P.S.; Etchie, A.T.; Pillarisetti, A.; Arora, N.K.; Smith, K.R. The health burden and economic costs averted by ambient PM 2.5 pollution reductions in Nagpur, India. Environ. Int. 2017, 102, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Spears, D. Health externalities of India’s expansion of coal plants: Evidence from a national panel of 40,000 households. J. Environ. Econ. Manag. 2017, 86, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Beig, G.; Chate, D.M.; Ghude, S.D.; Mahajan, A.; Srinivas, R.; Ali, K.; Sahu, S.; Parkhi, N.; Surendran, D.; Trimbake, H. Quantifying the effect of air quality control measures during the 2010 Commonwealth Games at Delhi, India. Atmos. Environ. 2013, 80, 455–463. [Google Scholar] [CrossRef]
- Kumar, P.; Gulia, S.; Harrison, R.M.; Khare, M. The influence of odd–even car trial on fine and coarse particles in Delhi. Environ. Pollut. 2017, 225, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Williams, G.M.; Morawska, L.; Mengersen, K.; Tong, S. Ozone modifies associations between temperature and cardiovascular mortality: Analysis of the NMMAPS data. Occup. Environ. Med. 2008, 65, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, C.; Williams, G.M.; Mengersen, K.; Morawska, L.; Tong, S. Does temperature modify short-term effects of ozone on total mortality in 60 large eastern US communities?—An assessment using the NMMAPS data. Environ. Int. 2008, 34, 451–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainham, D. The role of air pollution in the relationship between a heat stress index and human mortality in Toronto. Environ. Res. 2003, 93, 9–19. [Google Scholar] [CrossRef]
- Stafoggia, M.; Schwartz, J.; Forastiere, F.; Perucci, C.A. The SISTI Group Does Temperature Modify the Association between Air Pollution and Mortality? A Multicity Case-Crossover Analysis in Italy. Am. J. Epidemiol. 2008, 167, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S. Children First: Frontlines of India’s Air Pollution Crisis. 2018. Available online: https://www.nrdc.org/experts/anjali-jaiswal/children-first-frontlines-indias-air-pollution-crisis (accessed on 24 April 2018).
- Ostrom, E.; Dietz, T.; Dolsak, N.; Stern, P.C.; Stonich, S.; Weber, E.U. Hidden Costs of Energy: Unpriced Consequences of Energy Production and Use; National Academies Press: Washington, DC, USA, 2002. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Air Quality Descriptor | AQI Value | PM2.5 (μg/m3) 24-hr Average | PM10 (μg/m3) 24-hr Average | O3 (ppb) 8-hr Average | NO2 (ppb) 24-hr Average | CO (ppm) 24-hr Average |
|---|---|---|---|---|---|---|
| Good | 0–100 | 0–60 | 0–100 | 0–50 | 0–43 | 0–1.7 |
| Moderate | 101–200 | 61–90 | 101–250 | 51–84 | 44–96 | 1.8–8.7 |
| Poor | 201–300 | 91–120 | 251–350 | 85–104 | 97–149 | 8.8–14.8 |
| Very Poor | 301–400 | 121–250 | 351–430 | 105–374 | 150–213 | 14.9–29.7 |
| Severe | 401–500 | 251–350 | 431–550 | 375–450 | 214–750 | 29.8–40 |
| AIR Plan Aim [151] | Evaluation Method |
|---|---|
| 1. Health-Based AQI Warning and Interagency Coordination | Meetings with AMC and IITM-SAFAR staff and development of a draft internal AIR Plan User Guide and Standard Operating Procedures to standardize and strengthen interagency coordination practices. |
| 2. Communication and Outreach | Community roundtable meetings to qualitatively gauge the success of communication and outreach efforts. Development additional public outreach materials and engagement of local media on the AQI and AIR Plan. |
| 3. Focused Activities for Vulnerable Groups | Roundtable discussions with school administrators participating in the school flag program to assess student understanding and engagement [152]. |
| 4. Capacity Building of Medical Professionals | Conversations with leading medical professionals [152,186]. |
| 5. Research on Exposure Reduction and Mitigation Pathways | Local expert working group discussions of IITM-SAFAR AQI data and the Emissions Inventory to inform emission reduction efforts [24,152,158]. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limaye, V.S.; Knowlton, K.; Sarkar, S.; Ganguly, P.S.; Pingle, S.; Dutta, P.; M., S.L.; Tiwari, A.; Solanki, B.; Shah, C.; et al. Development of Ahmedabad’s Air Information and Response (AIR) Plan to Protect Public Health. Int. J. Environ. Res. Public Health 2018, 15, 1460. https://doi.org/10.3390/ijerph15071460
Limaye VS, Knowlton K, Sarkar S, Ganguly PS, Pingle S, Dutta P, M. SL, Tiwari A, Solanki B, Shah C, et al. Development of Ahmedabad’s Air Information and Response (AIR) Plan to Protect Public Health. International Journal of Environmental Research and Public Health. 2018; 15(7):1460. https://doi.org/10.3390/ijerph15071460
Chicago/Turabian StyleLimaye, Vijay S., Kim Knowlton, Sayantan Sarkar, Partha Sarthi Ganguly, Shyam Pingle, Priya Dutta, Sathish L. M., Abhiyant Tiwari, Bhavin Solanki, Chirag Shah, and et al. 2018. "Development of Ahmedabad’s Air Information and Response (AIR) Plan to Protect Public Health" International Journal of Environmental Research and Public Health 15, no. 7: 1460. https://doi.org/10.3390/ijerph15071460
APA StyleLimaye, V. S., Knowlton, K., Sarkar, S., Ganguly, P. S., Pingle, S., Dutta, P., M., S. L., Tiwari, A., Solanki, B., Shah, C., Raval, G., Kakkad, K., Beig, G., Parkhi, N., Jaiswal, A., & Mavalankar, D. (2018). Development of Ahmedabad’s Air Information and Response (AIR) Plan to Protect Public Health. International Journal of Environmental Research and Public Health, 15(7), 1460. https://doi.org/10.3390/ijerph15071460