Exploring Harms Experienced by Children Aged 7 to 11 Using Ambulance Attendance Data: A 6-Year Comparison with Adolescents Aged 12–17



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Ambulance Attendance Coding
2.2. Data for Inclusion
2.3. Mental Health Symptomology
2.4. Self-Injurious Behaviour
2.5. Ingestion of Pharmaceuticals or other Substances
2.6. Statistical Analysis
3. Results
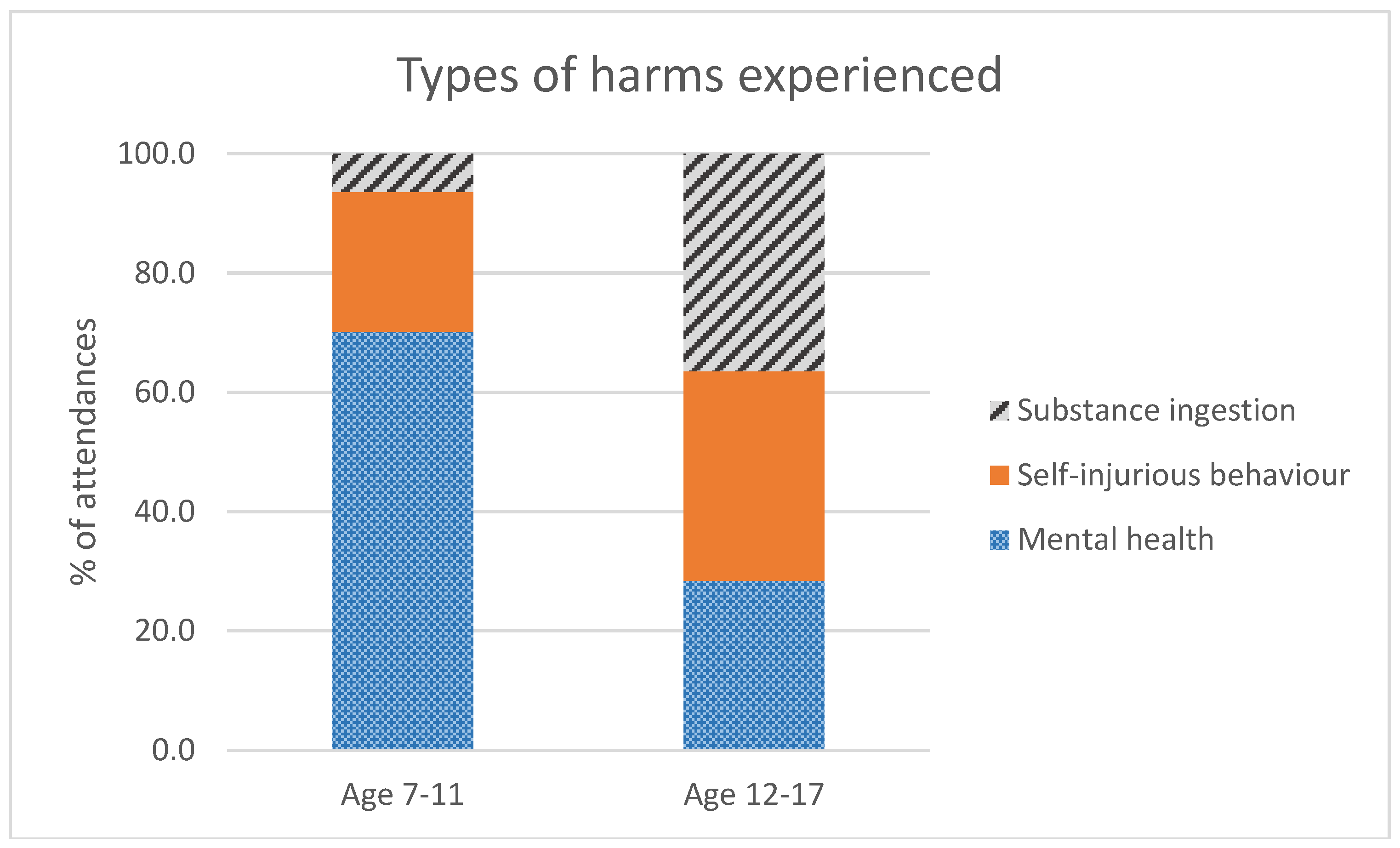
3.1. What Harms Are Experienced by Younger Children and Adolescents
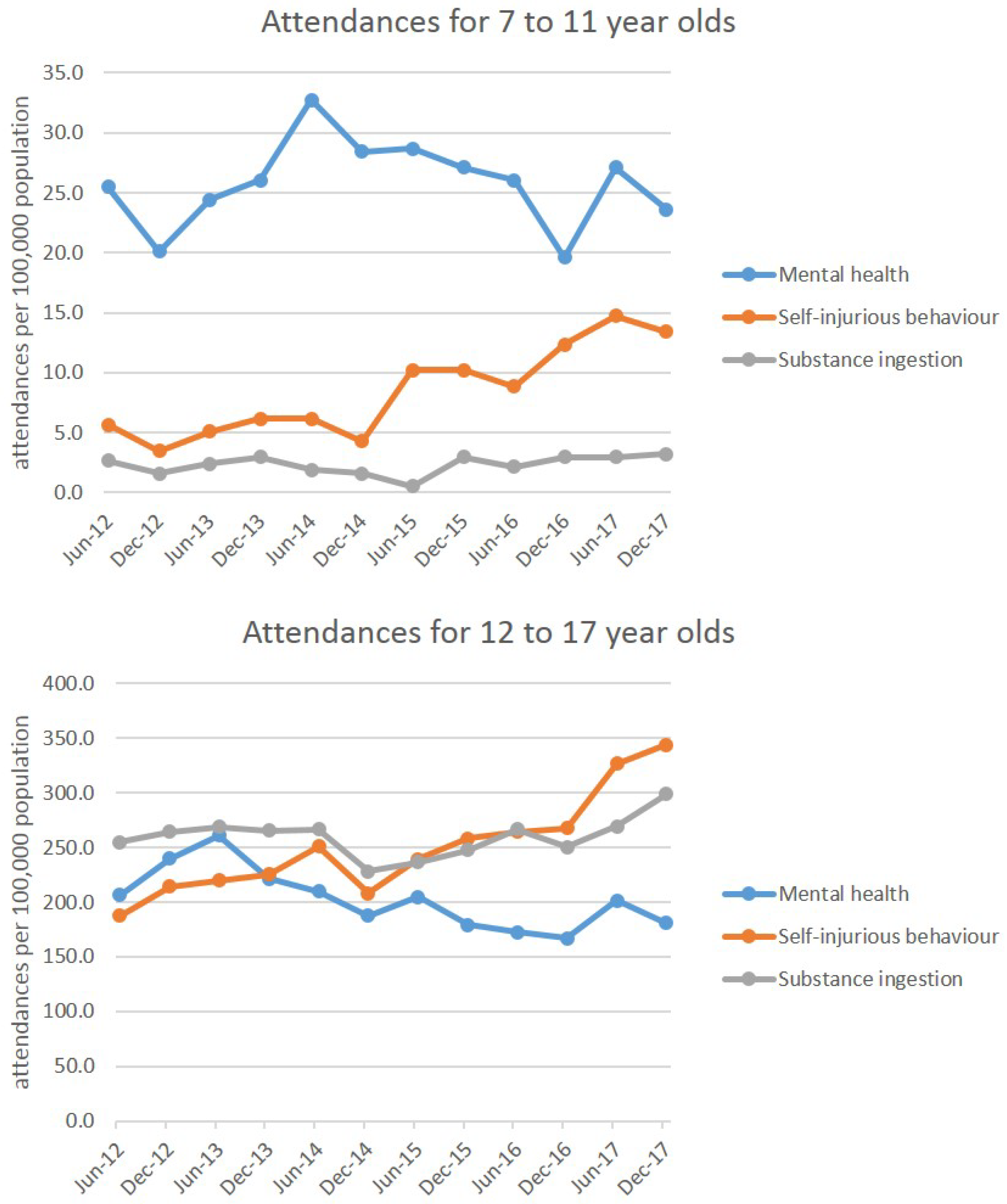
3.2. Are Rates of Ambulance Attendances Changing over Time?
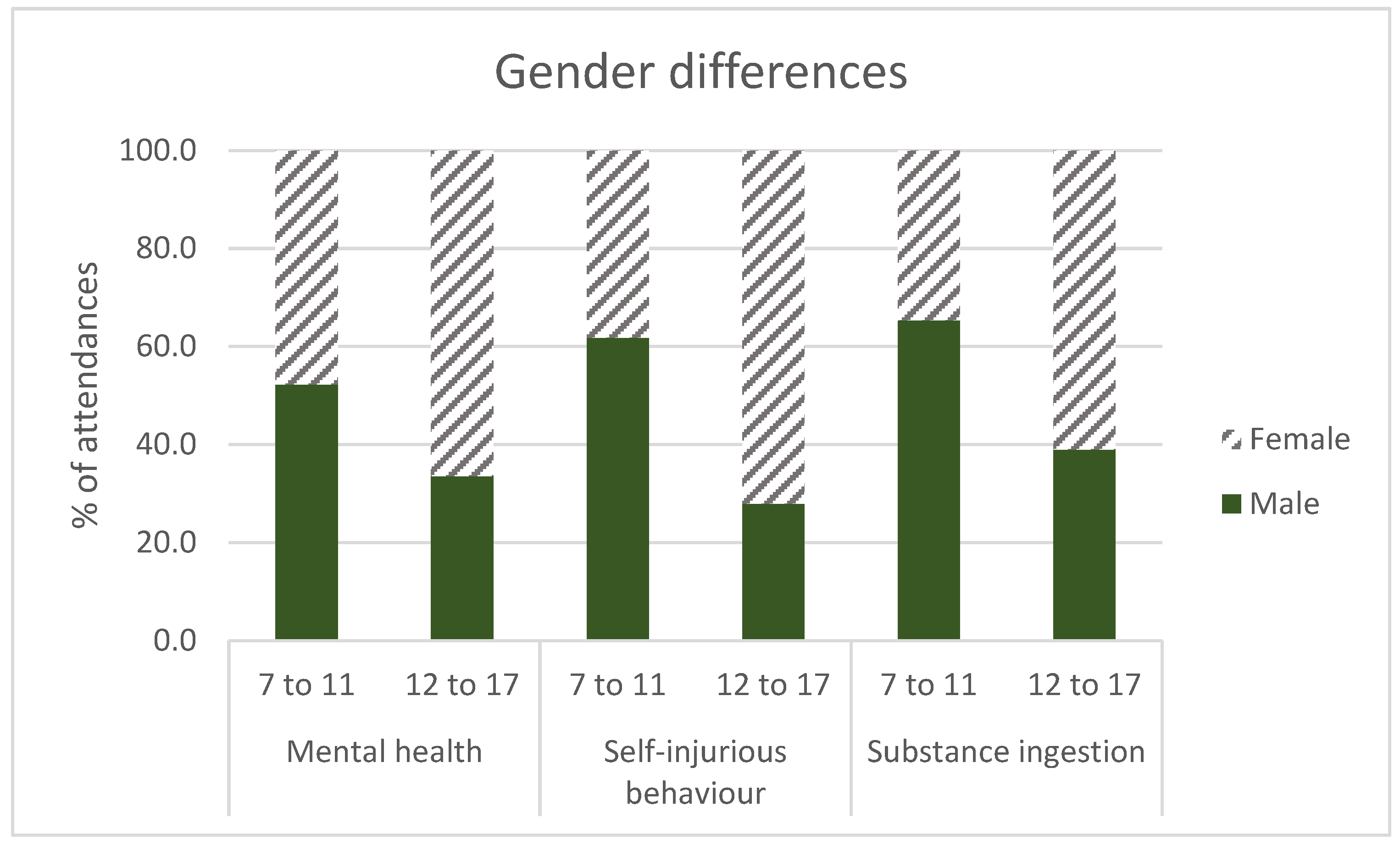
3.3. Are Gender Patterns Similar between Young and Older Adolescents?
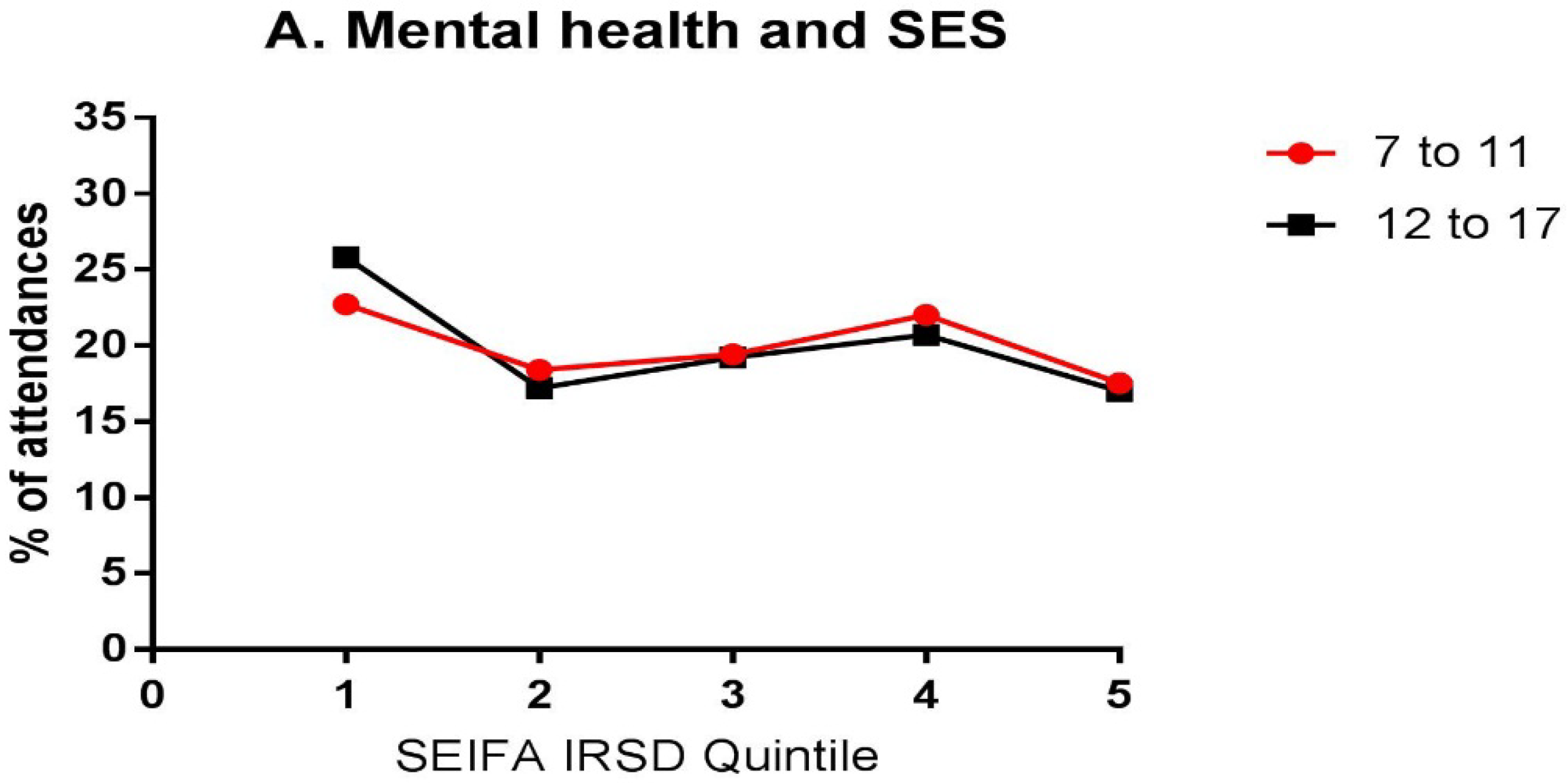
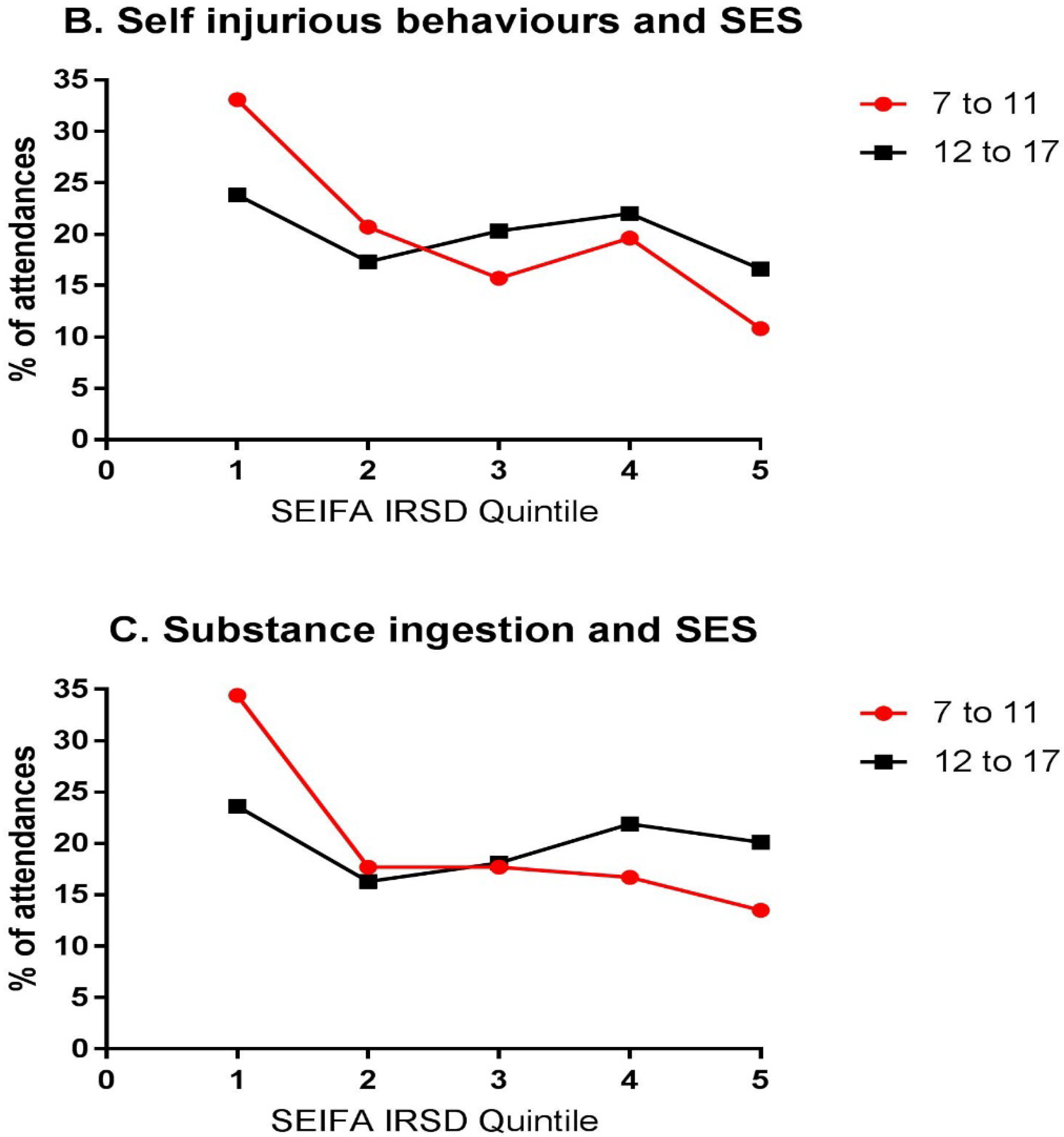
3.4. Is the Influence of Socio-Economic Status the Same between Age Groups?
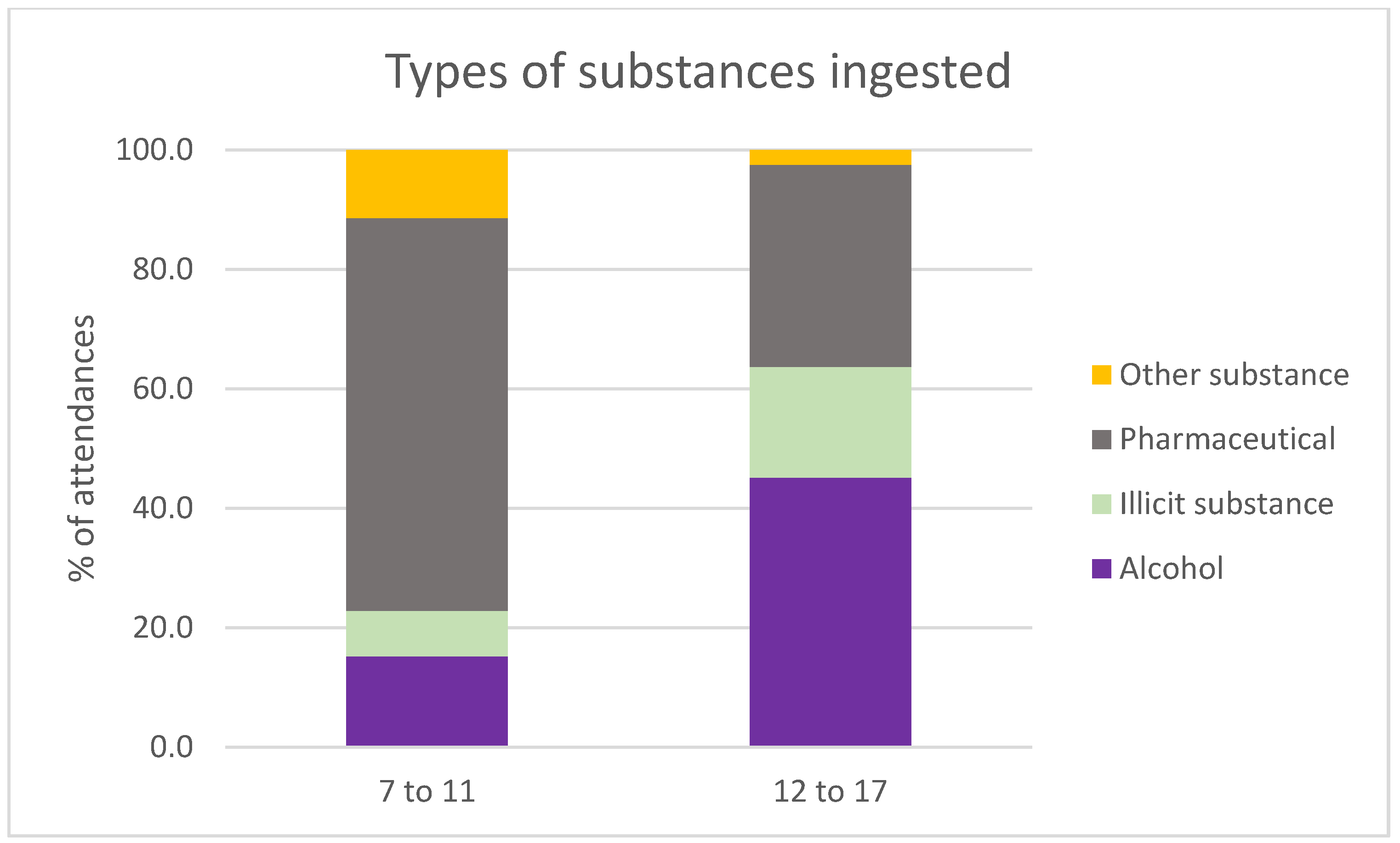
3.5. Do the Two Age Groups Have Similar Patterns in the Types of Substances Ingested?
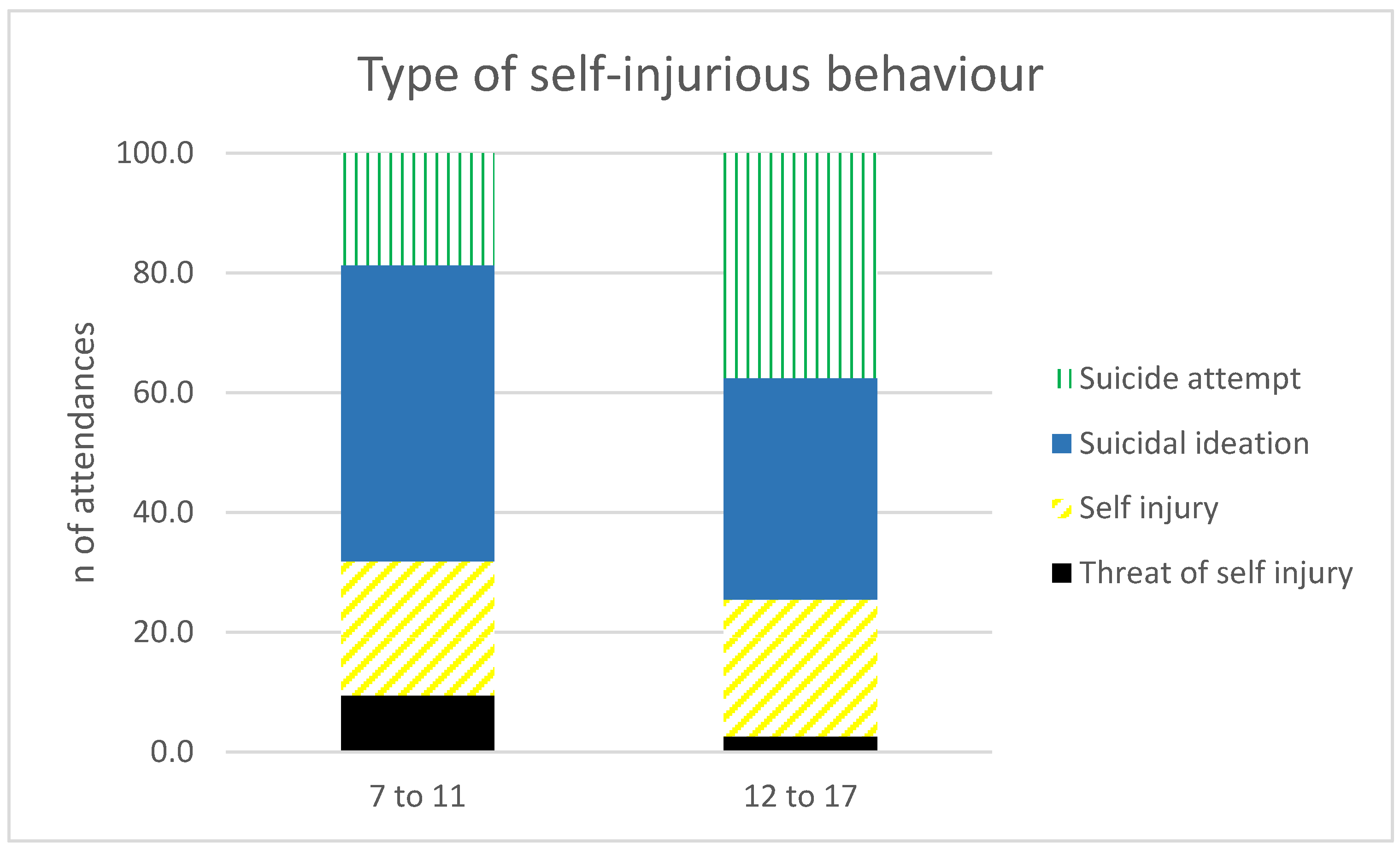
3.6. Do patterns of Self-Injurious Behaviour Differ between Age Groups?
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burke, K.C.; Burke, J.D.; Regier, D.A.; Rae, D.S. Age at onset of selected mental disorders in five community populations. Arch. Gen. Psychiatry 1990, 47, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.; He, J.; Burstein, M.; Swanson, S.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.H.; Dewa, C.S.; Phare, S. The suicidal process: Age of onset and severity of suicidal behaviour. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- McGorry, P.D.; Purcell, R.; Goldstone, S.; Amminger, G.P. Age of onset and timing of treatment for mental and substance use disorders: Implications for preventive intervention strategies and models of care. Curr. Opin. Psychiatry 2011, 24, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.; Johnson, S.; Hafekost, J.; de Haan, K.B.; Sawyer, M.; Ainley, J.; Zubrick, S.R. The Mental Health of Children and Adolescents; Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing; Department of Health: Canberra, Australia, 2015.
- White, V.; Williams, T. Australian Secondary School Students’ Use of Tobacco, Alcohol, and Over-the-Counter and Illicit Substances in 2014; Cancer Council Victoria: Melbourne, Australia, 2016. [Google Scholar]
- Fisher, C.B. Adolescent and parent perspectives on ethical issues in youth drug use and suicide survey research. Ethics Behav. 2003, 13, 303–332. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.L.; Webb, S.A.; Bioethics, C.O. Informed consent in decision-making in pediatric practice. Pediatrics 2016, 138, e20161485. [Google Scholar] [CrossRef] [PubMed]
- Gillett-Swan, J.K. Time to Tell: The Complexity of Wellbeing from the Perspective of Tweens; Australian Catholic University: Brisbane, Australia, 2013. [Google Scholar]
- Pasch, K.E.; Perry, C.L.; Stigler, M.H.; Komro, K.A. Sixth grade students who use alcohol: Do we need primary prevention programs for “tweens”? Health Educ. Behav. 2009, 36, 673–695. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustun, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Stoep, A.V.; McCauley, E.; Flynn, C.; Stone, A. Thoughts of death and suicide in early adolescence. Suicide Life Threat. Behav. 2009, 39, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Goldston, D.B.; Molock, S.D.; Whitbeck, L.B.; Murakami, J.L.; Zayas, L.H.; Hall, G.C.N. Cultural considerations in adolescent suicide prevention and psychosocial treatment. Am. Psychol. 2008, 63, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Tishler, C.L.; Reiss, N.S.; Rhodes, A.R. Suicidal behavior in children younger than twelve: A diagnostic challenge for emergency department personnel. Acad. Emerg. Med. 2007, 14, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, C.R. Childhood suicidal behavior: A developmental perspective. Psychiatr. Clin. 1997, 20, 551–562. [Google Scholar] [CrossRef]
- Jacobsen, L.K.; Rabinowitz, I.; Popper, M.S.; Solomon, R.J.; Sokol, M.S.; Pfeffer, C.R. Interviewing prepubertal children about suicidal ideation and behavior. J. Am. Acad. Child Adolesc. Psychiatry 1994, 33, 439–452. [Google Scholar] [CrossRef] [PubMed]
- Crossin, R.; Cairney, S.; Lawrence, A.J.; Duncan, J.R. Adolescent inhalant abuse leads to other drug use and impaired growth; implications for diagnosis. Aust. N. Z. J. Public Health 2017, 41, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hiscock, H.; Neely, R.J.; Lei, S.; Freed, G. Paediatric mental and physical health presentations to emergency departments, Victoria, 2008–2015. Med. J. Aust. 2018, 208, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Perera, J.; Wand, T.; Bein, K.J.; Chalkley, D.; Ivers, R.; Steinbeck, K.S.; Shields, R.; Dinh, M.M. Presentations to nsw emergency departments with self-harm, suicidal ideation, or intentional poisoning, 2010–2014. Med. J. Aust. 2018, 208, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Patton, G.C. Why are so many more adolescents presenting to our emergency departments with mental health problems? Med. J. Aust. 2018, 208, 339–340. [Google Scholar] [CrossRef] [PubMed]
- Buntsma, D.; Lithgow, A.; O’neill, E.; Palmer, D.; Morris, P.; Acworth, J.; Babl, F.E. Patterns of paediatric emergency presentations to a tertiary referral centre in the northern territory. Emerg. Med. Australas. 2017, 29, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, B. Trends in Alcohol and Drug Related Ambulance Attendances in Victoria: 2011–12; Department of Health: Melbourne, Victoria, Australia, 2013. [Google Scholar]
- Lloyd, B.K.; Mcelwee, P. Trends over time in characteristics of pharmaceutical drug-related ambulance attendances in Melbourne. Drug Alcohol Rev. 2011, 30, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Hall, W.; Adelstein, B.A. Ambulance calls to suspected overdoses: New South Wales patterns July 1997 to June 1999. Aust. N. Z. J. Public Health 2001, 25, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, B.; Gao, C.X.; Heilbronn, C.; Lubman, D.I. Self Harm and Mental Health-Related Ambulance Attendances in Australia; Turning Point: Melbourne, Victoria, Australia, 2013. [Google Scholar]
- Dietze, P.; Cvetkovski, S.; Rumbold, G.; Miller, P. Non-Fatal Heroin Overdose in Melbourne: Establishment and Analysis of a Database of Ambulance Service Records; Project Report 1997/1998; Turning Point Alcohol and Drug Centre: Melbourne, Victoria, Australia, 1998. [Google Scholar]
- Dietze, P.M.; Cvetkovski, S.; Rumbold, G.; Miller, P. Ambulance attendance at heroin overdose in Melbourne: The establishment of a database of ambulance service records. Drug Alcohol Rev. 2000, 19, 27–33. [Google Scholar]
- Australian Bureau of Statistics. Australian Demographic Statistics, March 2017; Australian Bureau of Statistics: Canberra, Australia, 2017.
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas 2016; Australian Bureau of Statistics: Canberra, Australia, 2017.
- Stewart, C.; Spicer, M.; Babl, F.E. Caring for adolescents with mental health problems: Challenges in the emergency department. J. Paediatr. Child Health 2006, 42, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Fahimi, J.; Aurrecoechea, A.; Anderson, E.; Herring, A.; Alter, H. Substance abuse and mental health visits among adolescents presenting to us emergency departments. Pediatr. Emerg. Care 2015, 31, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Page, A.; Morrell, S.; Carter, G.; Harrison, J. Socio-economic differentials in mental disorders and suicide attempts in Australia. Br. J. Psychiatry 2004, 185, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Matthews, K.A.; Boyce, W.T. Socioeconomic differences in children’s health: How and why do these relationships change with age? Psychol. Bull. 2002, 128, 295–329. [Google Scholar] [CrossRef] [PubMed]
- Patton, G.C.; Coffey, C.; Sawyer, S.M.; Viner, R.M.; Haller, D.M.; Bose, K.; Vos, T.; Ferguson, J.; Mathers, C.D. Global patterns of mortality in young people: A systematic analysis of population health data. Lancet 2009, 374, 881–892. [Google Scholar] [CrossRef]
- Reinherz, H.Z.; Tanner, J.L.; Berger, S.R.; Beardslee, W.R.; Fitzmaurice, G.M. Adolescent suicidal ideation as predictive of psychopathology, suicidal behavior, and compromised functioning at age 30. Am. J. Psychiatry 2006, 163, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Brent, D.A.; Baugher, M.; Bridge, J.; Chen, T.; Chiappetta, L. Age-and sex-related risk factors for adolescent suicide. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1497–1505. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. World Report on Child Injury Prevention; World Health Organisation: Geneva, Switzerland, 2008. [Google Scholar]
- Bronfenbrenner, U. Ecological Systems Theory; Jessica Kingsley Publishers: London, UK, 1992. [Google Scholar]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, D.; Crossin, R.; Ogeil, R.; Smith, K.; Lubman, D.I. Exploring Harms Experienced by Children Aged 7 to 11 Using Ambulance Attendance Data: A 6-Year Comparison with Adolescents Aged 12–17. Int. J. Environ. Res. Public Health 2018, 15, 1385. https://doi.org/10.3390/ijerph15071385
Scott D, Crossin R, Ogeil R, Smith K, Lubman DI. Exploring Harms Experienced by Children Aged 7 to 11 Using Ambulance Attendance Data: A 6-Year Comparison with Adolescents Aged 12–17. International Journal of Environmental Research and Public Health. 2018; 15(7):1385. https://doi.org/10.3390/ijerph15071385
Chicago/Turabian StyleScott, Debbie, Rose Crossin, Rowan Ogeil, Karen Smith, and Dan I. Lubman. 2018. "Exploring Harms Experienced by Children Aged 7 to 11 Using Ambulance Attendance Data: A 6-Year Comparison with Adolescents Aged 12–17" International Journal of Environmental Research and Public Health 15, no. 7: 1385. https://doi.org/10.3390/ijerph15071385
APA StyleScott, D., Crossin, R., Ogeil, R., Smith, K., & Lubman, D. I. (2018). Exploring Harms Experienced by Children Aged 7 to 11 Using Ambulance Attendance Data: A 6-Year Comparison with Adolescents Aged 12–17. International Journal of Environmental Research and Public Health, 15(7), 1385. https://doi.org/10.3390/ijerph15071385