Development of a Cumulative Exposure Index (CEI) for Manganese and Comparison with Bone Manganese and Other Biomarkers of Manganese Exposure


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cumulative Exposure Index
2.3. Biological Samples and Determination of Mn Biomarkers
2.4. Statistical Analyses
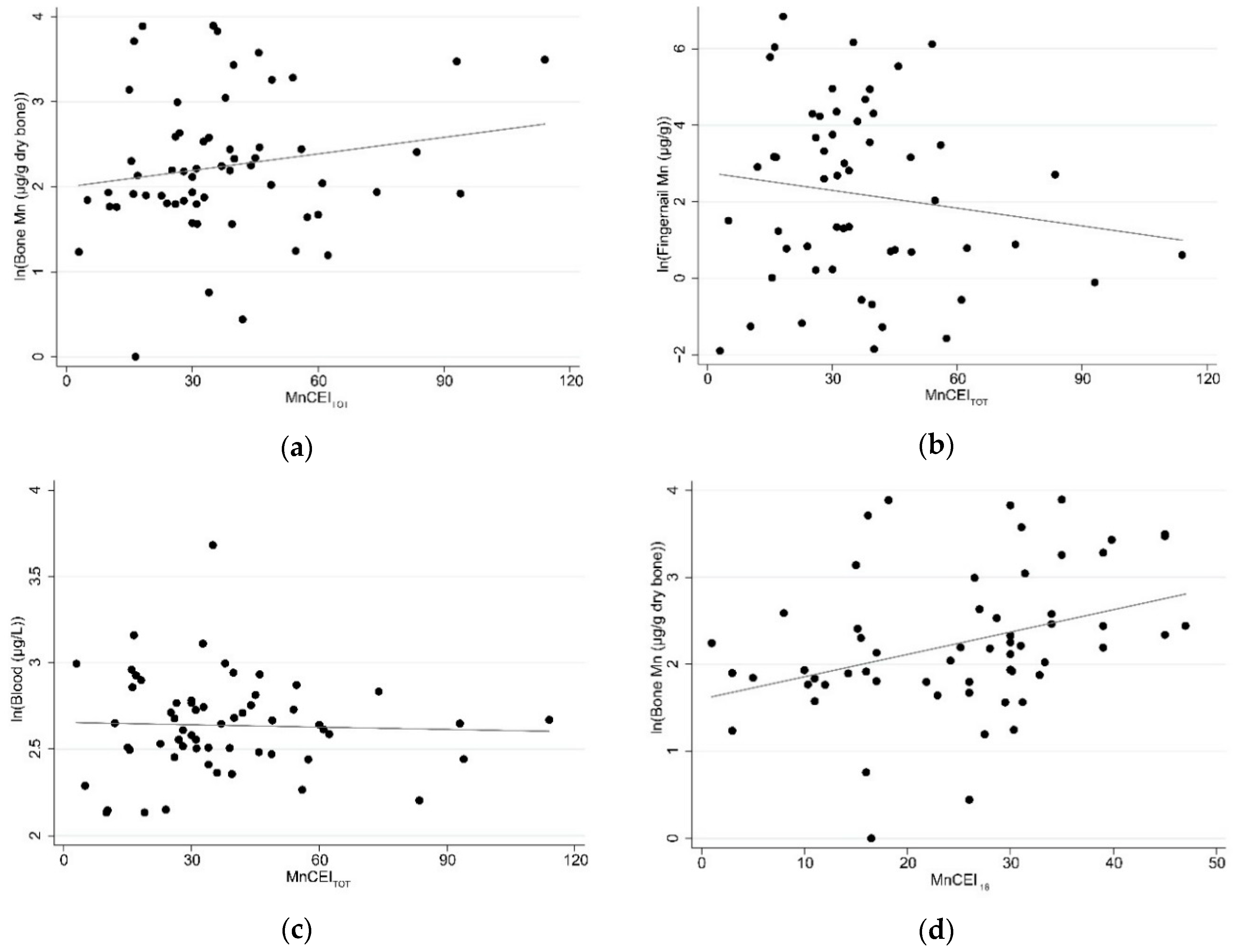
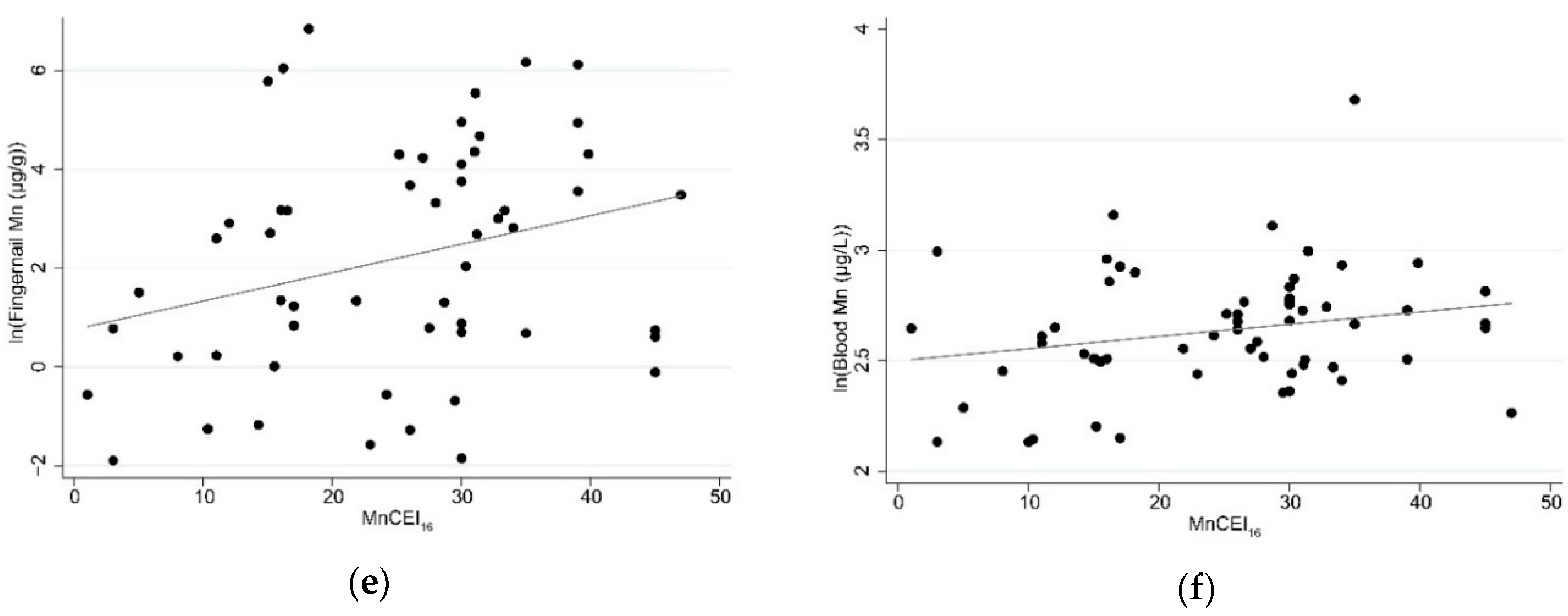
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Job Title 1 | Occupational Category 2 | Air Mn 3 | Exposure Rank |
|---|---|---|---|
| Welder/arc welder | Metal ore processing | Welders: 0.01 to 2.13 mg/m3 [40]; Ferroalloy workers: 0.098 to 0.374 mg/m3 [13] | 3: high (direct exposure) |
| Smelter | |||
| Ore combustion | |||
| Ore extraction | |||
| Manganese ore processing | |||
| Underground Mn ore mining | |||
| Manganese electrolysis | |||
| Director | Management (ferroalloy) | Ferroalloy workers (indirect exposure) = 0.01–0.11 mg/m3 [13]; Mining = 0.21 mg/m3 [41]; Die-casting foundry = up to 0.14 mg/m3 [43] | 2: medium (indirect exposure) |
| Manager/Project manager | |||
| Ore production manager | |||
| Equipment management | |||
| Driver | Transportation and material moving (Ferroalloy) | ||
| Driver: ore transporting | |||
| Trainman | |||
| Metal product assembler | Assemblers and fabricators | ||
| Maintenance | Installation maintenance and repair (Ferroalloy) | ||
| Equipment repair | |||
| Machine repair | |||
| Cleaner | Building grounds and cleaning (Ferroalloy) | ||
| Machine operator | Non-ferrous metal production and processing | ||
| Miner | Mining | ||
| Die-casting hardware | Molding | ||
| Refinery | Metal-refining furnace operators and tenders | ||
| Lime processing | Lime product manufacturing | ||
| Factory/general worker | Other occupations (ferroalloy) 4 | ||
| Wireman | |||
| Advertisement | Advertisement and marketing | Auto repair: 0.00045 mg/m3 [38]; Administrative Support: 0.001 mg/m3 [44] | 1: low (low/no exposure) |
| Marketing | |||
| Driver | Transportation and material moving (manufacturing) | ||
| Stevedore | |||
| Secretary | Administrative support | ||
| Security guard/personnel | Protective services | ||
| Machine repair | Installation, maintenance, and repair (manufacturing) | ||
| Weeding | Building and grounds cleaning (manufacturing) | ||
| Designer | Industrial designers | ||
| Car repair | Automotive repair and maintenance | ||
| Cement factory worker | Construction | ||
| Construction worker | |||
| Road construction/roadman | |||
| Brick carrier | |||
| Manager | Management (manufacturing) | ||
| Vegetable storage manager | Other occupations (manufacturing/other employer) 4 | ||
| General/other worker | |||
| Private business | |||
| Wireman |
References
- Ferraz, H.B.; Bertolucci, P.H.; Pereira, J.S.; Lima, J.G.; Andrade, L.A. Chronic exposure to the fungicide maneb may produce symptoms and signs of CNS manganese intoxication. Neurology 1988, 38, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Chia, S.E.; Foo, S.C.; Gan, S.L.; Jeyaratnam, J.; Tian, C.S. Neurobehavioral functions among workers exposed to manganese ore. Scand. J. Work. Environ. Health 1993, 19, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Bowler, R.M.; Gysens, S.; Diamond, E.; Nakagawa, S.; Drezgic, M.; Roels, H.A. Manganese exposure: Neuropsychological and neurological symptoms and effects in welders. Neurotoxicology 2006, 27, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, R.; Apostoli, P.; Perrone, C.; Placidi, D.; Albini, E.; Migliorati, P.; Mergler, D.; Sassine, M.P.; Palmi, S.; Alessio, L. Long-term exposure to “low levels” of manganese oxides and neurofunctional changes in ferroalloy workers. Neurotoxicology 1999, 20, 287–297. [Google Scholar] [PubMed]
- Bowler, R.M.; Roels, H.A.; Nakagawa, S.; Drezgic, M.; Diamond, E.; Park, R.; Koller, W.; Bowler, R.P.; Mergler, D.; Bouchard, M.; et al. Dose-effect relationships between manganese exposure and neurological, neuropsychological and pulmonary function in confined space bridge welders. Occup. Environ. Med. 2007, 64, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.M.; Zheng, W.; Zou, Y.; Shi, X.; Chen, J.; Rosenthal, F.S.; Fan, Q. Manganese exposure among smelting workers: Relationship between blood manganese-iron ratio and early onset neurobehavioral alterations. Neurotoxicology 2009, 30, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, S.L.; Zheng, W. Manganese Toxicity Upon Overexposure: A Decade in Review. Curr. Environ. Health Rep. 2015, 2, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Racette, B.A.; Aschner, M.; Guilarte, T.R.; Dydak, U.; Criswell, S.R.; Zheng, W. Pathophysiology of manganese-associated neurotoxicity. Neurotoxicology 2012, 33, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Dietz, M.C.; Ihrig, A.; Wrazidlo, W.; Bader, M.; Jansen, O.; Triebig, G. Results of magnetic resonance imaging in long-term manganese dioxide-exposed workers. Environ. Res. 2001, 85, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, M.; Mergler, D.; Baldwin, M.E.; Panisset, M. Manganese cumulative exposure and symptoms: A follow-up study of alloy workers. Neurotoxicology 2008, 29, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Bowler, R.M.; Nakagawa, S.; Drezgic, M.; Roels, H.A.; Park, R.M.; Diamond, E.; Mergler, D.; Bouchard, M.; Bowler, R.P.; Koller, W. Sequelae of fume exposure in confined space welding: A neurological and neuropsychological case series. Neurotoxicology 2007, 28, 298–311. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, R.; Selis, L.; Folli, D.; Apostoli, P.; Mutti, A.; Vanoni, O.; Iregren, A.; Alessio, L. Neurobehavioral effects of manganese in workers from a ferroalloy plant after temporary cessation of exposure. Scand. J. Work. Environ. Health 1995, 21, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.M.; Fan, Q.; Zou, Y.; Shi, X.; Chen, J.; Aschner, M.; Rosenthal, F.S.; Zheng, W. Manganese exposure among smelting workers: Blood manganese-iron ratio as a novel tool for manganese exposure assessment. Biomarkers 2009, 14, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Laohaudomchok, W.; Lin, X.; Herrick, R.F.; Fang, S.C.; Cavallari, J.M.; Christiani, D.C.; Weisskopf, M.G. Toenail, blood, and urine as biomarkers of manganese exposure. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2011, 53, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Järvisalo, J.; Olkinuora, M.; Kiilunen, M.; Kivistö, H.; Ristola, P.; Tossavainen, A.; Aitio, A. Urinary and blood manganese in occupationally nonexposed populations and in manual metal arc welders of mild steel. Int. Arch. Occup. Environ. Health 1992, 63, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Kim, H.; Zhao, Q. Comparative toxicokinetics of manganese chloride and methylcyclopentadienyl manganese tricarbonyl (MMT) in Sprague-Dawley rats. Toxicol. Sci. Off. J. Soc. Toxicol. 2000, 54, 295–301. [Google Scholar] [CrossRef]
- Apostoli, P.; Lucchini, R.; Alessio, L. Are current biomarkers suitable for the assessment of manganese exposure in individual workers? Am. J. Ind. Med. 2000, 37, 283–290. [Google Scholar] [CrossRef]
- Ellingsen, D.G.; Dubeikovskaya, L.; Dahl, K.; Chashchin, M.; Chashchin, V.; Zibarev, E.; Thomassen, Y. Air exposure assessment and biological monitoring of manganese and other major welding fume components in welders. J. Environ. Monit. 2006, 8, 1078–1086. [Google Scholar] [CrossRef] [PubMed]
- Long, Z.; Jiang, Y.-M.; Li, X.-R.; Fadel, W.; Xu, J.; Yeh, C.-L.; Long, L.-L.; Luo, H.-L.; Harezlak, J.; Murdoch, J.B.; et al. Vulnerability of welders to manganese exposure—A neuroimaging study. Neurotoxicology 2014, 45, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Hassani, H.; Golbabaei, F.; Ghahri, A.; Hosseini, M.; Shirkhanloo, H.; Dinari, B.; Eskandari, D.; Fallahi, M. Occupational exposure to manganese-containing welding fumes and pulmonary function indices among natural gas transmission pipeline welders. J. Occup. Health 2012, 54, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Eastman, R.R.; Jursa, T.P.; Benedetti, C.; Lucchini, R.G.; Smith, D.R. Hair as a biomarker of environmental manganese exposure. Environ. Sci. Technol. 2013, 47, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Reiss, B.; Simpson, C.D.; Baker, M.G.; Stover, B.; Sheppard, L.; Seixas, N.S. Hair Manganese as an Exposure Biomarker among Welders. Ann. Occup. Hyg. 2016, 60, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.J.; Edmondson, D.A.; Nour, M.M.; Snyder, S.; Rosenthal, F.S.; Dydak, U. Toenail Manganese: A Sensitive and Specific Biomarker of Exposure to Manganese in Career Welders. Ann. Work Expo. Health 2018, 62, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.; Dietz, M.C.; Ihrig, A.; Triebig, G. Biomonitoring of manganese in blood, urine and axillary hair following low-dose exposure during the manufacture of dry cell batteries. Int. Arch. Occup. Environ. Health 1999, 72, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Fu, S.X.; Dydak, U.; Cowan, D.M. Biomarkers of manganese intoxication. Neurotoxicology 2011, 32, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Gwiazda, R.; Bowler, R.; Roels, H.; Park, R.; Taicher, C.; Lucchini, R. Biomarkers of Mn exposure in humans. Am. J. Ind. Med. 2007, 50, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Lauwerys, R.; Hoet, P. Industrial Chemical Exposure: Guidelines for Biological Monitoring, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2001; ISBN 1-56670-545-2. [Google Scholar]
- Andersen, M.E.; Gearhart, J.M.; Clewell, H.J. Pharmacokinetic data needs to support risk assessments for inhaled and ingested manganese. Neurotoxicology 1999, 20, 161–171. [Google Scholar] [PubMed]
- O’Neal, S.L.; Hong, L.; Fu, S.; Jiang, W.; Jones, A.; Nie, L.H.; Zheng, W. Manganese accumulation in bone following chronic exposure in rats: Steady-state concentration and half-life in bone. Toxicol. Lett. 2014, 229, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.L.; McNeill, F.E.; Stronach, I.M.; Pejovic-Milic, A.; Chettle, D.R.; Waker, A. An accelerator based system for in vivo neutron activation analysis measurements of manganese in human hand bones. Med. Phys. 2002, 29, 2718–2724. [Google Scholar] [CrossRef] [PubMed]
- Pejović-Milić, A.; Aslam; Chettle, D.R.; Oudyk, J.; Pysklywec, M.W.; Haines, T. Bone manganese as a biomarker of manganese exposure: A feasibility study. Am. J. Ind. Med. 2009, 52, 742–750. [Google Scholar] [CrossRef]
- Liu, Y.; Koltick, D.; Byrne, P.; Wang, H.; Zheng, W.; Nie, L.H. Development of a transportable neutron activation analysis system to quantify manganese in bone in vivo: Feasibility and methodology. Physiol. Meas. 2013, 34, 1593–1609. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Mostafaei, F.; Sowers, D.; Hsieh, M.; Zheng, W.; Nie, L.H. Customized compact neutron activation analysis system to quantify manganese (Mn) in bone in vivo. Physiol. Meas. 2017, 38, 452–465. [Google Scholar] [CrossRef] [PubMed]
- Wells, E.M.; Liu, Y.; Rolle-McFarland, D.; Mostafaei, F.; Zheng, W.; Nie, L.H. In vivo measurement of bone manganese and association with manual dexterity: A pilot study. Environ. Res. 2018, 160, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Rolle-McFarland, D.; Mostafaei, F.; Zhou, Y.; Li, Y.; Zheng, W.; Wells, E.; Nie, L.H. In vivo neutron activation analysis of bone manganese in workers. Physiol. Meas. 2018, 39, 035003. [Google Scholar] [CrossRef] [PubMed]
- Ramlow, J.M.; Spadacene, N.W.; Hoag, S.R.; Stafford, B.A.; Cartmill, J.B.; Lerner, P.J. Mortality in a cohort of pentachlorophenol manufacturing workers, 1940–1989. Am. J. Ind. Med. 1996, 30, 180–194. [Google Scholar] [CrossRef]
- Fayerweather, W.E.; Karns, M.E.; Nuwayhid, I.A.; Nelson, T.J. Case-control study of cancer risk in tetraethyl lead manufacturing. Am. J. Ind. Med. 1997, 31, 28–35. [Google Scholar] [CrossRef]
- O’Neal, S.L.; Lee, J.-W.; Zheng, W.; Cannon, J.R. Subacute manganese exposure in rats is a neurochemical model of early manganese toxicity. Neurotoxicology 2014, 44, 303–313. [Google Scholar] [CrossRef] [PubMed]
- US Department of Labor Occupational Outlook Handbook. Available online: https://www.bls.gov/ooh/occupation-finder.htm (accessed on 8 June 2017).
- Hedmer, M.; Karlsson, J.-E.; Andersson, U.; Jacobsson, H.; Nielsen, J.; Tinnerberg, H. Exposure to respirable dust and manganese and prevalence of airways symptoms, among Swedish mild steel welders in the manufacturing industry. Int. Arch. Occup. Environ. Health 2014, 87, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.E.; Thompson, M.L.; Ramushu, S.; Young, T.; Jeebhay, M.F.; London, L.; Esswein, E.; Renton, K.; Spies, A.; Boulle, A.; et al. The nervous system effects of occupational exposure on workers in a South African manganese smelter. Neurotoxicology 2003, 24, 885–894. [Google Scholar] [CrossRef]
- Sierra, P.; Loranger, S.; Kennedy, G.; Zayed, J. Occupational and environmental exposure of automobile mechanics and nonautomotive workers to airborne manganese arising from the combustion of methylcyclopentadienyl manganese tricarbonyl (MMT). Am. Ind. Hyg. Assoc. J. 1995, 56, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Westberg, H.B.; Seldén, A.I.; Bellander, T. Exposure to chemical agents in Swedish aluminum foundries and aluminum remelting plants--a comprehensive survey. Appl. Occup. Environ. Hyg. 2001, 16, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Zayed, J.; Mikhaïl, M.; Loranger, S.; Kennedy, G.; L’Espérance, G. Exposure of taxi drivers and office workers to total and respirable manganese in an urban environment. Am. Ind. Hyg. Assoc. J. 1996, 57, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Zhu, C.; Liu, D.; Dong, M.; Zhang, A.; Pan, Y.; Yan, H. [Inductively coupled plasma mass spectrometry for the simultaneous determination of thirty metals and metalloids elements in blood samples]. Zhonghua Yu Fang Yi Xue Za Zhi 2012, 46, 745–749. [Google Scholar] [PubMed]
- Zhang, L.-L.; Lu, L.; Pan, Y.-J.; Ding, C.-G.; Xu, D.-Y.; Huang, C.-F.; Pan, X.-F.; Zheng, W. Baseline blood levels of manganese, lead, cadmium, copper, and zinc in residents of Beijing suburb. Environ. Res. 2015, 140, 10–17. [Google Scholar] [CrossRef] [PubMed]
- De Sousa Viana, G.F.; de Carvalho, C.F.; Nunes, L.S.; Rodrigues, J.L.G.; Ribeiro, N.S.; de Almeida, D.A.; Ferreira, J.R.D.; Abreu, N.; Menezes-Filho, J.A. Noninvasive biomarkers of manganese exposure and neuropsychological effects in environmentally exposed adults in Brazil. Toxicol. Lett. 2014, 231, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Kile, M.L.; Houseman, E.A.; Breton, C.V.; Quamruzzaman, Q.; Rahman, M.; Mahiuddin, G.; Christiani, D.C. Association between total ingested arsenic and toenail arsenic concentrations. J. Environ. Sci. Health Part A 2007, 42, 1827–1834. [Google Scholar] [CrossRef] [PubMed]
- Succop, P.A.; Clark, S.; Chen, M.; Galke, W. Imputation of data values that are less than a detection limit. J. Occup. Environ. Hyg. 2004, 1, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Wells, E.M.; Herbstman, J.B.; Lin, Y.H.; Jarrett, J.; Verdon, C.P.; Ward, C.; Caldwell, K.L.; Hibbeln, J.R.; Witter, F.R.; Halden, R.U.; et al. Cord Blood Methylmercury and Fetal Growth Outcomes in Baltimore Newborns: Potential Confounding and Effect Modification by Omega-3 Fatty Acids, Selenium, and Sex. Environ. Health Perspect. 2016, 124, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Mukherjee, B.; Xia, X.; Sparrow, D.; Weisskopf, M.G.; Nie, H.; Hu, H. Bone lead level prediction models and their application to examine the relationship of lead exposure and hypertension in the Third National Health and Nutrition Examination Survey. J. Occup. Environ. Med. 2009, 51, 1422–1436. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.; Aro, A.; Rotnitzky, A.; Amarasiriwardena, C.; Hu, H. K X-ray fluorescence measurements of bone lead concentration: The analysis of low-level data. Phys. Med. Biol. 1995, 40, 1475–1485. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, A.C. Plots, Transformations, and Regression: An Introduction to Graphical Methods of Diagnostic Regression Analysis; Oxford Statistical Science Series; Oxford University Press: Oxford, UK, 1987; ISBN 0-19-853371-3. [Google Scholar]
- Baker, M.G.; Simpson, C.D.; Stover, B.; Sheppard, L.; Checkoway, H.; Racette, B.A.; Seixas, N.S. Blood manganese as an exposure biomarker: State of the evidence. J. Occup. Environ. Hyg. 2014, 11, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Grashow, R.; Zhang, J.; Fang, S.C.; Weisskopf, M.G.; Christiani, D.C.; Cavallari, J.M. Toenail metal concentration as a biomarker of occupational welding fume exposure. J. Occup. Environ. Hyg. 2014, 11, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, M.; Chan, H.M.; Domingo, J.L.; Oliveira, R.B.; Kawakami, S.; Murata, K. Significance of fingernail and toenail mercury concentrations as biomarkers for prenatal methylmercury exposure in relation to segmental hair mercury concentrations. Environ. Res. 2015, 136, 289–294. [Google Scholar] [CrossRef] [PubMed]


| Characteristic | Manufacturing Factory (N = 30) | Ferroalloy Factory (N = 30) | Total Population (N = 60) |
|---|---|---|---|
| Age, years | 48.2 (9.4) | 46.7 (6.1) | 47.3 (7.9) |
| Education, years | 10.9 (4.0) | 9.1 (3.6) | 10.0 (3.9) |
| Duration of current job, years | 9.5 (8.7) | 8.4 (4.1) | 9.0 (6.8) |
| MnCEITOT, no units | 41.2 (28.1) | 33.9 (13.0) | 37.5 (22.0) |
| MnCEI16, no units | 21.2 (12.5) * | 28.7 (8.7) * | 25.0 (11.3) |
| Blood manganese, µg/L | 13.4 (3.1) *,1 | 15.2 (5.9) *,1 | 14.1 (4.0) 1 |
| Fingernail manganese, µg/g | 1.5 (1.9) *,1,2 | 42.8 (116.2) *,2,3 | 13.5 (58.5) 1,4 |
| Bone manganese, µg/g | 0.9 (4.5) 1 | 3.0 (16.3) 1 | 2.6 (7.2) 1 |
| Variable | Blood Mn | Fingernail Mn | Bone Mn | MnCEITOT | MnCEI16 |
|---|---|---|---|---|---|
| Blood Mn | 1.00 (1.00) | -- | -- | -- | -- |
| Fingernail Mn | 0.23 (0.09) 1 | 1.00 (1.00) 1 | -- | -- | -- |
| Bone Mn | 0.16 (0.23) | 0.45 (<0.01) 1 | 1.00 (1.00) | -- | -- |
| MnCEITOT | −0.01 (0.97) | −0.13 (0.35) 1 | 0.16 (0.22) | 1.00 (1.00) | -- |
| MnCEI16 | 0.22 (0.09) | 0.32 (0.02) 1 | 0.43 (<0.01) | 0.66 (<0.01) | 1.00 (1.00) |
| Mn Biomarker | Model 1 | MnCEITOT | MnCEI16 |
|---|---|---|---|
| Blood Mn | Continuous | −0.0003 (−0.004, 0.003) | 0.002 (−0.005, 0.009) |
| Ordinal | −0.0008 (−0.02, 0.02) | 0.008 (−0.04, 0.05) | |
| Fingernail Mn 2 | Continuous | −0.007 (−0.03, 0.01) | 0.004 (−0.03, 0.04) |
| Ordinal | −0.008 (−0.04, 0.02) | 0.009 (−0.05, 0.06) | |
| Bone Mn | Continuous | 0.007 (−0.003, 0.02) | 0.03 (0.001, 0.05) * |
| Ordinal | 0.02 (−0.0003 , 0.05) | 0.08 (0.03, 0.14) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rolle-McFarland, D.; Liu, Y.; Zhou, J.; Mostafaei, F.; Zhou, Y.; Li, Y.; Fan, Q.; Zheng, W.; Nie, L.H.; Wells, E.M. Development of a Cumulative Exposure Index (CEI) for Manganese and Comparison with Bone Manganese and Other Biomarkers of Manganese Exposure. Int. J. Environ. Res. Public Health 2018, 15, 1341. https://doi.org/10.3390/ijerph15071341
Rolle-McFarland D, Liu Y, Zhou J, Mostafaei F, Zhou Y, Li Y, Fan Q, Zheng W, Nie LH, Wells EM. Development of a Cumulative Exposure Index (CEI) for Manganese and Comparison with Bone Manganese and Other Biomarkers of Manganese Exposure. International Journal of Environmental Research and Public Health. 2018; 15(7):1341. https://doi.org/10.3390/ijerph15071341
Chicago/Turabian StyleRolle-McFarland, Danelle, Yingzi Liu, Jieqiong Zhou, Farshad Mostafaei, Yuanzhong Zhou, Yan Li, Quiyan Fan, Wei Zheng, Linda H. Nie, and Ellen M. Wells. 2018. "Development of a Cumulative Exposure Index (CEI) for Manganese and Comparison with Bone Manganese and Other Biomarkers of Manganese Exposure" International Journal of Environmental Research and Public Health 15, no. 7: 1341. https://doi.org/10.3390/ijerph15071341
APA StyleRolle-McFarland, D., Liu, Y., Zhou, J., Mostafaei, F., Zhou, Y., Li, Y., Fan, Q., Zheng, W., Nie, L. H., & Wells, E. M. (2018). Development of a Cumulative Exposure Index (CEI) for Manganese and Comparison with Bone Manganese and Other Biomarkers of Manganese Exposure. International Journal of Environmental Research and Public Health, 15(7), 1341. https://doi.org/10.3390/ijerph15071341