Larger Workplaces, People-Oriented Culture, and Specific Industry Sectors Are Associated with Co-Occurring Health Protection and Wellness Activities

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Sampling and Recruitment
2.3. Measures
2.3.1. Independent Variables: Workplace Demographic Characteristics
2.3.2. Occupational Health and Safety and Wellness Activities
2.3.3. Outcome Variable: Co-Occurrence of Occupational Health and Safety and Wellness Activities
2.4. Analyses
3. Results
3.1. Descriptive Statistics
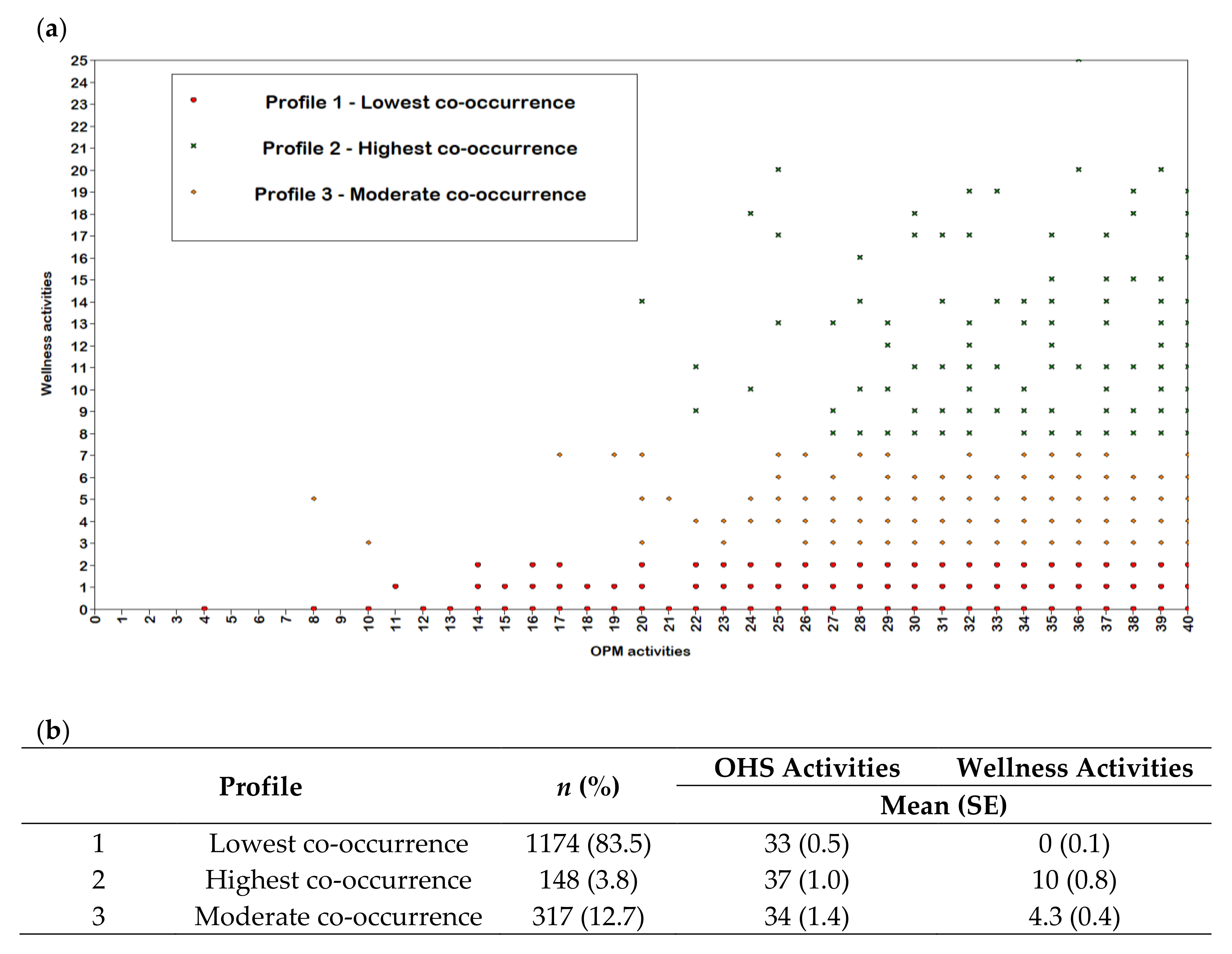
3.2. Co-Occurrence of Occupational Health and Safety and Wellness Activities
3.3. Asociations between Workplace Demographic Characteristics and the Co-Occurrence of Occupational Health and Safety and Wellness Activities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raphael, D. Social Determinants of Health: Canadian Perspectives; Canadian Scholars’ Press and Women’s Press: Toronto, ON, Canada, 2009; pp. 150–191. [Google Scholar]
- Solar, O.; Irwin, A. A conceptual framework for action on the social determinants of health. In Social Determinants of Health Discussion Paper 2 (Policy and Practice); WHO Press: Geneva, Switzerland, 2010; pp. 32–33. [Google Scholar]
- Schulte, P.A.; Pandalai, S.; Wulsin, V.; Chun, H. Interaction of occupational and personal risk factors in workforce health and safety. Am. J. Public Health 2012, 102, 434–448. [Google Scholar] [CrossRef] [PubMed]
- Ljungblad, C.; Granström, F.; Dellve, L.; Åkerlind, I. Workplace health promotion and working conditions as determinants of employee health. Int. J. Workplace Health Manag. 2014, 7, 89–104. [Google Scholar] [CrossRef]
- Musich, S.; Napier, D.; Edington, D.W. The association of health risks with workers’ compensation costs. J. Occup. Environ. Med. 2001, 43, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Trogdon, J.; Finkelstein, E.; Hylands, T.; Dellea, P.; Kamal-Bahl, S. Indirect costs of obesity: A review of the current literature. Obes. Rev. 2008, 9, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Hafdahl, A.R.; Cooper, P.S.; Brown, L.M.; Lusk, S.L. Meta-analysis of workplace physical activity interventions. Am. J. Prev. Med. 2009, 37, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Noblet, A.; LaMontagne, A.D. The role of workplace health promotion in addressing job stress. Health Promot. Int. 2006, 21, 346–353. [Google Scholar] [CrossRef]
- Hymel, P.A.; Loeppke, R.R.; Baase, C.M.; Burton, W.N.; Hartenbaum, N.P.; Hudson, T.W.; McLellan, R.K.; Mueller, K.L.; Roberts, M.A.; Yarborough, C.M. Workplace health protection and promotion: A new pathway for a healthier—And safer—Workforce. J. Occup. Environ. Med. 2011, 53, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Stoddard, A.M.; LaMontagne, A.D.; Emmons, K.; Hunt, M.K.; Youngstrom, R.; McLellan, D.; Christiani, D.C. A comprehensive worksite cancer prevention intervention: Behavior change results from a randomized controlled trial (United States). Cancer Causes Control 2002, 13, 493–502. [Google Scholar] [CrossRef]
- Cooklin, A.; Joss, N.; Husser, E.; Oldenburg, B. Integrated approaches to occupational health and safety: A systematic review. Am. J. Health Promot. 2017, 31, 401–412. [Google Scholar] [CrossRef]
- World Health Organization. Healthy Workplaces: A WHO Global Model for Action. For Employers, Workers, Policy-Makers and Practitioners; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- International Labour Organization. The SOLVE Training Package: Integrating Health Promotion into Workplace OSH Policies. Available online: http://www.ilo.org/safework/info/instr/WCMS_178438/lang--en/index.htm (accessed on 21 November 2018).
- Schill, A.L.; Chosewood, L.C. The NIOSH Total Worker Health™ program: An overview. J. Occup. Environ. Med. 2013, 55, S8–S11. [Google Scholar] [CrossRef] [PubMed]
- Hannon, P.A.; Garson, G.; Harris, J.R.; Hammerback, K.; Sopher, C.J.; Clegg-Thorp, C. Workplace health promotion implementation, readiness, and capacity among mid-sized employers in low-wage industries: A national survey. J. Occup. Environ. Med. 2012, 54, 1337–1343. [Google Scholar] [CrossRef]
- Sinclair, R.C.; Cunningham, T.R. Safety activities in small businesses. Saf. Sci. 2014, 64, 32–38. [Google Scholar] [CrossRef] [PubMed]
- McLellan, D.L.; Cabán-Martinez, A.J.; Nelson, C.C.; Pronk, N.P.; Katz, J.N.; Allen, J.D.; Davis, K.L.; Wagner, G.R.; Sorensen, G. Organizational characteristics influence implementation of worksite health protection and promotion programs: Evidence from smaller businesses. J. Occup. Environ. Med. 2015, 57, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, P.A.; Nobrega, S.; Davis, L.; Erck, E.; Punnett, L. Healthy workplaces? A survey of Massachusetts employers. Am. J. Health Promot. 2013, 27, 390–400. [Google Scholar] [CrossRef] [PubMed]
- McLellan, D.L.; Williams, J.A.; Katz, J.N.; Pronk, N.P.; Wagner, G.R.; Cabán-Martinez, A.J.; Nelson, C.C.; Sorensen, G. Key organizational characteristics for integrated approaches to protect and promote worker health in smaller enterprises. J. Occup. Environ. Med. 2017, 59, 289–294. [Google Scholar] [CrossRef]
- McCoy, M.K.; Stinson, M.K.; Scott, M.K.; Tenney, M.L.; Newman, L.S. Health promotion in small business: A systematic review of factors influencing adoption and effectiveness of worksite wellness programs. J. Occup. Environ. Med. 2014, 56, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Institute for Work & Health. Measures in the Ontario Leading Indicators Project (OLIP) Survey. Available online: https://www.iwh.on.ca/sites/iwh/files/iwh/reports/iwh_project_olip_about_the_measures_august_2013.pdf (accessed on 21 November 2018).
- Workplace Safety and Insurance Board of Ontario. 2017 Highlights: By the Numbers. Available online: http://www.wsibstatistics.ca/S2/Workplaces%20%20WSIB%20By%20The%20Numbers_P.php (accessed on 21 November 2018).
- Sorensen, G.; McLellan, D.; Dennerlein, J.T.; Pronk, N.P.; Allen, J.D.; Boden, L.I.; Okechukwu, C.A.; Hashimoto, D.; Stoddard, A.; Wagner, G.R. Integration of health protection and health promotion: Rationale, indicators, and metrics. J. Occup. Environ. Med. 2013, 55, S12. [Google Scholar] [CrossRef]
- Leung, D.; Rispoli, L.; Chan, R. Small, Medium-Sized, and Large Businesses in the Canadian Economy: Measuring Their Contribution to Gross Domestic Product from 2001 to 2008. Available online: https://www150.statcan.gc.ca/n1/en/pub/11f0027m/11f0027m2012082-eng.pdf (accessed on 21 November 2018).
- Amick, B.C.; Habeck, R.V.; Hunt, A.; Fossel, A.H.; Chapin, A.; Keller, R.B.; Katz, J.N. Measuring the impact of organizational behaviors on work disability prevention and management. J. Occup. Rehabil. 2000, 10, 21–38. [Google Scholar] [CrossRef]
- Hunt, H.A.; Habeck, R.V.; VanTol, B.; Scully, S.M. Disability Prevention among Michigan Employers, 1988–1993; Report No. 93-004; W.E. Upjohn Institute for Employment Research: Kalamazoo, MI, USA, 1993. [Google Scholar]
- Shea, T.; De Cieri, H.; Donohue, R.; Cooper, B.; Sheehan, C. Leading indicators of occupational health and safety: An employee and workplace level validation study. Saf. Sci. 2016, 85, 293–304. [Google Scholar] [CrossRef]
- Institute for Work & Health. Benchmarking Organizational Leading Indicators for the Prevention and Management of Injuries and Illnesses: Final Report. Available online: https://www.iwh.on.ca/sites/iwh/files/iwh/reports/iwh_report_benchmarking_organizational_leading_indicators_2011.pdf (accessed on 21 November 2018).
- Centers for Disease Control and Prevention. Workplace Health Model. Available online: https://www.cdc.gov/workplacehealthpromotion/pdf/WorkplaceHealth-model-update.pdf (accessed on 21 November 2018).
- Goetzel, R.Z.; Henke, R.M.; Tabrizi, M.; Pelletier, K.R.; Loeppke, R.; Ballard, D.W.; Grossmeier, J.; Anderson, D.R.; Yach, D.; Kelly, R.K. Do workplace health promotion (wellness) programs work? J. Occup. Environ. Med. 2014, 56, 927–934. [Google Scholar] [CrossRef]
- SAS Institute. Base SAS 9.4 Procedures Guide; SAS Institute: Cary, NC, USA, 2015. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Oberski, D. Mixture models: Latent profile and latent class analysis. In Modern Statistical Methods for Human-Computer Interaction; Springer: Geneva, Switzerland, 2016; pp. 275–287. [Google Scholar]
- Aldana, S.G.; Anderson, D.R.; Adams, T.B.; Whitmer, R.W.; Merrill, R.M.; George, V.; Noyce, J. A review of the knowledge base on healthy worksite culture. J. Occup. Environ. Med. 2012, 54, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.; Allen, C. Chapter 26: A culture of health: Creating and sustaining supportive organizational environments for health. In ACSM’s Worksite Health Handbook. A Guide to Building Healthy and Productive Companies, 2nd ed.; Pronk, N., Ed.; Human Kinetics Publishers: Champaign, IL, USA, 2009; pp. 224–230. [Google Scholar]
- Feltner, C.; Peterson, K.; Weber, R.P.; Cluff, L.; Coker-Schwimmer, E.; Viswanathan, M.; Lohr, K.N. The effectiveness of Total Worker Health interventions: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2016, 165, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Anger, W.K.; Elliot, D.L.; Bodner, T.; Olson, R.; Rohlman, D.S.; Truxillo, D.M.; Kuehl, K.S.; Hammer, L.B.; Montgomery, D. Effectiveness of Total Worker Health interventions. J. Occup. Health Psychol. 2015, 20, 226–247. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.J.; Grossman, D.C.; Hubbard, R.A.; Ortega, A.N.; Curry, S.J. Integrated interventions for improving Total Worker Health: A panel report from the National Institutes of Health Pathways to Prevention Workshop: Total Worker Health—What’s Work Got to Do with It? Ann. Intern. Med. 2016, 165, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Rohlman, D.S.; Campo, S.; Hall, J.; Robinson, E.L.; Kelly, K.M. What could Total Worker Health® look like in small enterprises? Ann. Work Expo. Health 2018, 62, S34–S41. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n | % or M | SD |
|---|---|---|---|
| Workplace size | |||
| Small (<100 employees) without a JHSC | 171 | 53.2 | 4.1 |
| Small (<100 employees) with a JHSC | 511 | 28.3 | 3.3 |
| Medium (100 to 499 employees) | 267 | 8.0 | 1.8 |
| Large (>500 employees) | 81 | 1.9 | 0.8 |
| Union status | |||
| Non-unionized | 964 | 90.1 | 1.9 |
| Unionized | 304 | 5.9 | 0.9 |
| Don’t know | 10 | 4.1 | 4.2 |
| Industry sector | |||
| Manufacturing | 440 | 30.4 | 1.4 |
| Service | 412 | 53.6 | 2.9 |
| Healthcare | 197 | 4.4 | 0.6 |
| Agriculture | 161 | 10.2 | 1.4 |
| Education | 81 | 0.8 | 0.1 |
| Municipal | 62 | 0.4 | 0.1 |
| Pulp and paper | 24 | 0.1 | <0.1 |
| Electrical and utilities | 13 | 0.1 | <0.1 |
| Occupational health & safety performance (IWH-OPM, range: 1 to 5) | |||
| Formal safety audits at regular intervals | 3.3 | 15.3 | |
| Organization values ongoing safety improvement | 4.3 | 9.4 | |
| Safety as important as work production and quality | 4.4 | 9.5 | |
| Workers and supervisors have information to work safely | 4.5 | 8.5 | |
| Employees always involved in health and safety decisions | 4.3 | 9.3 | |
| Those in charge of safety have authority to make necessary changes | 4.5 | 9.1 | |
| Positive recognition for those who act safely | 4.0 | 11.9 | |
| Everyone has the tools and/or equipment to complete work safely | 4.6 | 7.9 | |
| Workplace wellness activities | |||
| Flexible work hours for wellness | 484 | 39.8 | 2.2 |
| Have onsite shower facilities | 365 | 15.0 | 2.2 |
| Employee assistance programs | 394 | 14.6 | 2.5 |
| Physical activity and/or fitness programs | 272 | 14.2 | 2.4 |
| Programs to prevent/reduce stress | 226 | 12.6 | 2.4 |
| Self-care books/tools | 210 | 11.9 | 2.1 |
| Nutrition education | 221 | 11.7 | 2.4 |
| Education on balancing work and family | 164 | 11.4 | 2.2 |
| Provide or encourage fitness breaks | 158 | 8.1 | 1.7 |
| Have fitness or walking trails on site | 133 | 6.4 | 1.5 |
| Health risk assessment | 87 | 5.8 | 1.9 |
| Smoking cessation classes/counselling | 184 | 5.7 | 1.5 |
| Weight management classes/counselling | 115 | 5.2 | 1.9 |
| Screenings for high blood pressure | 83 | 5.2 | 1.6 |
| Alcohol or drug abuse support programs | 173 | 4.3 | 0.9 |
| Cholesterol reduction education | 68 | 4.1 | 1.4 |
| Screenings for cholesterol level | 35 | 3.2 | 1.6 |
| Screening for diabetes | 30 | 2.4 | 1.3 |
| Chronic disease management programs | 66 | 2.3 | 0.9 |
| Promotions/discounts to encourage health food choices | 158 | 2.2 | 0.9 |
| Label health food choices in cafeteria | 76 | 2.2 | 1.0 |
| Nurse advice line | 41 | 1.9 | 0.8 |
| Screenings for any form of cancer | 24 | 1.7 | 0.9 |
| Have signage to encourage people to use the stairs | 41 | 1.7 | 0.9 |
| HIV/AIDS education | 22 | 0.4 | 0.1 |
| Characteristic | Profile 2 | Profile 3 |
|---|---|---|
| Highest Co-Occurrence | Moderate Co-Occurrence | |
| OR (95% CI) | ||
| Workplace size | ||
| Small (<100 employees) without a JHSC | Reference | Reference |
| Small (<100 employees) with a JHSC | 0.32 (0.05–2.19) | 1.48 (1.15–4.25) |
| Medium (100 to 499 employees) | 2.76 (0.43–3.59) | 4.71 (1.42–8.74) |
| Large (>500 employees) | 3.22 (1.15–5.89) | 2.22 (1.05–4.52) |
| Union status | ||
| Non-unionized | Reference | Reference |
| Unionized | 1.52 (0.48–4.88) | 1.03 (0.33–3.27) |
| Industry sector | ||
| Manufacturing | Reference | Reference |
| Agriculture | 1.00 (0.11–9.20) | 0.78 (0.46–1.50) |
| Pulp and paper | 0.50 (0.11–2.21) | 0.51 (0.10–2.70) |
| Education | 0.74 (0.15–3.67) | 4.90 (0.28–8.77) |
| Electrical and utilities | 5.57 (2.24–8.35) | 7.97 (2.46–10.50) |
| Municipal | 5.52 (0.91–8.43) | 6.97 (1.80–9.06) |
| Healthcare | 1.76 (0.68–4.56) | 2.12 (0.72–6.28) |
| Service | 0.13 (0.03–0.59) | 1.87 (0.73–4.80) |
| Health and safety leadership | ||
| 1 (low) | Reference | Reference |
| 2 | 1.77 (0.25–2.66) | 0.52 (0.12–2.24) |
| 3 | 5.19 (0.95–7.52) | 0.50 (0.15–1.69) |
| 4 (high) | 4.77 (0.73–5.99) | 0.60 (0.21–1.74) |
| People-oriented culture | ||
| 1 (low) | Reference | Reference |
| 2 | 1.63 (0.96–2.40) | 3.59 (0.77–6.88) |
| 3 | 1.73 (2.20–4.41) | 4.63 (0.93–6.02) |
| 4 (high) | 4.70 (1.59–5.26) | 2.77 (0.62–5.42) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biswas, A.; Severin, C.N.; Smith, P.M.; Steenstra, I.A.; Robson, L.S.; Amick, B.C., III. Larger Workplaces, People-Oriented Culture, and Specific Industry Sectors Are Associated with Co-Occurring Health Protection and Wellness Activities. Int. J. Environ. Res. Public Health 2018, 15, 2739. https://doi.org/10.3390/ijerph15122739
Biswas A, Severin CN, Smith PM, Steenstra IA, Robson LS, Amick BC III. Larger Workplaces, People-Oriented Culture, and Specific Industry Sectors Are Associated with Co-Occurring Health Protection and Wellness Activities. International Journal of Environmental Research and Public Health. 2018; 15(12):2739. https://doi.org/10.3390/ijerph15122739
Chicago/Turabian StyleBiswas, Aviroop, Colette N. Severin, Peter M. Smith, Ivan A. Steenstra, Lynda S. Robson, and Benjamin C. Amick, III. 2018. "Larger Workplaces, People-Oriented Culture, and Specific Industry Sectors Are Associated with Co-Occurring Health Protection and Wellness Activities" International Journal of Environmental Research and Public Health 15, no. 12: 2739. https://doi.org/10.3390/ijerph15122739
APA StyleBiswas, A., Severin, C. N., Smith, P. M., Steenstra, I. A., Robson, L. S., & Amick, B. C., III. (2018). Larger Workplaces, People-Oriented Culture, and Specific Industry Sectors Are Associated with Co-Occurring Health Protection and Wellness Activities. International Journal of Environmental Research and Public Health, 15(12), 2739. https://doi.org/10.3390/ijerph15122739