We describe the status of and factors associated with the use of basic water and sanitation services based on data from a combined WaSH and nutrition intervention programme in Ethiopia. Region, intervention and control area, socioeconomic status, multiple use of the main water source, sanitary hygiene, sanitation sensitisation and training, educational background and health risk perceptions determined the use of basic services.
4.1. Factors Associated with Basic Water and Sanitation Services
The use of basic sanitation services was associated with the region (SNNPR had higher odds than Amhara), while basic water services was not. The four regions where the community-based nutrition programme was implemented are very diverse in terms of environment, topography, hydrology, regional climate and occurrence of extreme weather events, and they are inhabited by different ethnic, cultural and linguistic population groups that settle in different population densities and have different lifestyles, all of which are factors that may explain these differences [
2,
12,
13].
Households that had electricity were positively associated with basic water services as compared to households who lacked electricity. No respective association was found regarding the use of basic sanitation services. In this study, the presence of electricity was used as a proxy for socioeconomic status. Consequently, the interpretation of these results would point to a better socioeconomic status increasing the use of basic water services, but not of basic sanitation services. While the presence of electricity surely points to a better socioeconomic situation as compared to households who lack electricity, the findings may suggest that electricity alone is not an entirely robust indicator. In a rural setting, as in the programme area, electricity may be present in certain villages and absent in others; thus, it is a rather weak indicator for wealth as compared to wealth indices that, in addition to electricity, include the possession of other additional asset items [
30,
31].
Household heads who used their main drinking water source for multiple purposes other than drinking (including cooking, hygiene, washing) were less likely to use basic services as compared to those only using the main drinking water source for drinking only. This may suggest that households who drew their combined water needs from just only one source were forced to use an unimproved service, possibly because the basic services could not produce the quantities needed to address all water needs in the water-scarce rural area. This finding underlines the need for actors and researchers to not only focus on, but also encourage the use of multiple water sources for different purposes [
32].
Households whose latrine had been emptied at least once before were more likely to use basic sanitation services that were not shared with others. This underlines that besides presence, sanitary hygiene matters in terms of use.
4.2. Differences in Basic Services between the Intervention and Control Areas
In the programme area, where 86% of the households rely on agriculture as their livelihoods, but where chronic malnutrition is widespread, the use of basic services is vitally important. Ensuring that sufficient water is available not only for WaSH and domestic purposes, but also for irrigation has a substantial impact on food availability; it improves nutritional status, and thus human health. The use of unsafely managed water supply (for both domestic and local productive use), inadequate access to sanitation, and poor hygiene practices, however, exacerbates food insecurity and malnutrition, while at the same time decreasing work productivity further.
This programme evaluation revealed no significant difference in the use of basic water services between intervention and control areas, which suggests that the households in the control areas perform as well as do the households in the intervention area.
The use of basic sanitation services was significantly higher in intervention than in control areas. Moreover, the respondents from the intervention area were more likely to link latrine use to health benefits, which suggests that sanitation sensitisation in the intervention may have been successful.
The data of this programme implementation was collected two years after completion of the WaSH intervention. Thus, assuming a positive effect on WaSH behaviour and on WaSH-related knowledge and risk perceptions as entirely owing to the intervention may not suffice, as a substantial amount of time has passed since.
4.3. The Implications of Education on Basic Water and Sanitation Services
Education levels were low in the programme area; about 51% of the household heads never went to school, and 8% received only informal or pre-school education. Thus, only about 40% ever went to primary or higher schools. Households with heads who had received any education were significantly more likely to use basic water services as opposed to those who received no education at all, as shown in the bivariate analyses. Education did not show any significant association with the use of basic sanitation services. The household head’s education was not significantly associated with either the use of basic water or sanitation services in the multivariable models. Thus, formal education plays a limited role in terms for the use of basic services, contradicting studies from similar settings [
2,
13,
33].
In the programme area, education was measured by years spent at school. However, knowledge can be acquired elsewhere, e.g., via the radio, newspapers or internet broadcast, at health centres, through community health workers and family members, and is not necessarily measurable or quantifiable.
The fact that household heads in the programme area who had received sanitation sensitisation or training before were more likely to use basic sanitation service than those who had not, underlines this statement, and indicates that the education component of the intervention may have been successful. This becomes visible due to the high level of risk knowledge and perception related to diarrhoea in the programme area, the low overall education level notwithstanding. These findings also acknowledge the importance of strengthening all health educators, i.e., community health workers’ role in the implementation of WaSH [
34,
35].
4.4. The Role of Risk Perceptions for WaSH-Related Behaviour
Despite the low level of formal education, the awareness on risk factors related to WaSH and diarrhoea was high in the programme area. The disease was believed to be linked to faeces, the presence of flies, poor food hygiene, ‘dirty spaces’ and unsafe drinking water.
The household members’ perceptions adequately reflect the real WaSH-related risks, as described in the framework on faecal-oral disease transmission (‘F-diagram’) on transmission routes of excreta-related pathogens that cause disease [
36,
37], thus supporting evidence from Kenya, where the risk perceptions from the grassroots level corresponded to real health risks [
34,
38].
The study from Ethiopia may go one step beyond: In this study, household heads attributed numerous benefits, such as better health or cleanliness of the compound, and disadvantages, such as construction and maintenance cost, to the use of latrines. Believing that unsafe drinking water was the main cause for diarrhoea, for example, proved to be positively associated with the use of basic water service (OR 1.48; CI 1.20–1.81;
p ≤ 0.001). The perception of ‘dirty spaces’ causing diarrhoea was associated with the use of basic sanitation service (OR 1.81; CI 1.50–2.19;
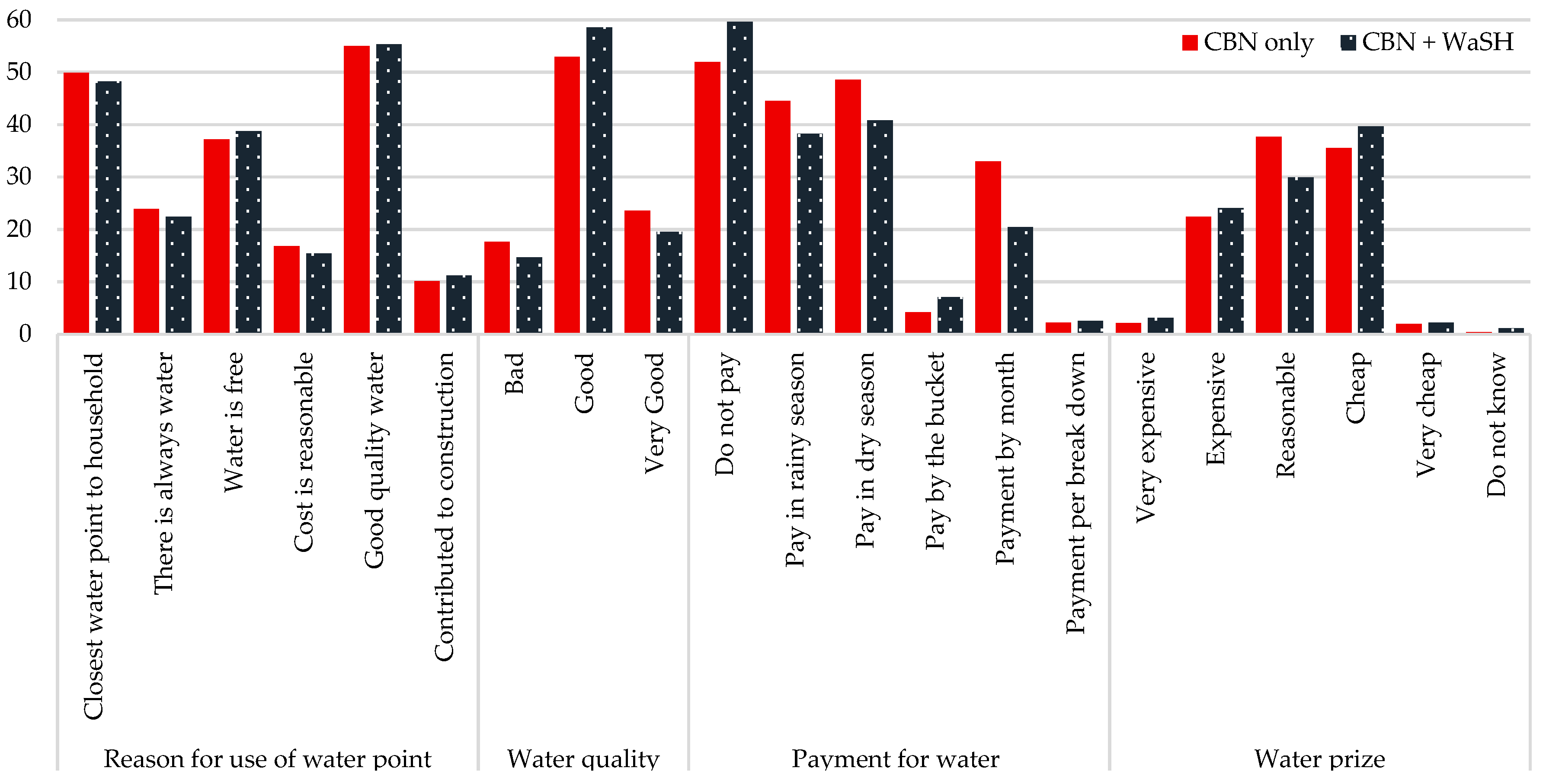
p ≤ 0.001). Moreover, household heads perceiving the water quality of the main drinking water source as good was positively associated with the use of basic water service as opposed to those perceiving the water quality to be poor (OR 3.94; CI 3.06–5.08;
p ≤ 0.001). Believing that the quality was good therefore animated the household heads to make use of a particular water point. While this does not prove that the water quality free of contamination based on microbial or chemical water testing, it indicates that health risk perceptions matter. Both findings point to risk perceptions being closely linked to and potentially motivating the application of positive WaSH-related and health-protective behaviour—the use of basic services. These results confirm findings from a qualitative study in Malawi that found risk communication on the need for domestic water treatment effecting behaviour change [
39].
Although the benefits of safely managed sanitation were clear to the respondents, only about 20% of the observed sanitation facilities were clean, and about 30% had never emptied. This could mean that many of the latrines were relatively new and had therefore never been emptied. This could also mean, as is common in some rural areas, that latrines were not emptied, but topped off, and the slab and infrastructure moved to a new pit. So, do risk perception and health beliefs thus not translate into practice?
Some household heads’ risk perceptions were positively or negatively associated with the use of basic sanitation service. Those, for example, who believed that the main benefits of latrines included improved privacy were more likely to use a basic sanitation service, whereas those who believed that the main disadvantage of a latrine was its maintenance cost were less likely to use basic sanitation services. Thus, some of the risk perceptions are put in practice, while others are not.
Although risk perceptions may act as triggers for precautionary action [
40], it should be noted that the engagement in preventive health behaviours is not merely determined by the awareness of objective health risks, but is also greatly influenced by health beliefs and specific health cognitions [
41]. Thus, risk perceptions do not necessarily translate into practice and the engagement in preventive health behaviours [
17,
18]. Practising healthy behaviour is dependent upon a variety of social, cultural and economic factors, and not limited to infrastructure development and education [
13,
41,
42]. According to Curtis et al. [
17,
18] and following social and evolutionary psychology and neuroscience, health and WaSH-related behaviour can be assigned to three types of interacting causes. These are cognitive or executive control producing ‘planned’ behaviour, aimed at preventing disease, achieving long-term health goals, and adequate socialisation. Moreover, there is the reward system stimulating ‘motivated’ behaviour, with drivers of motivation being disgust, status and social standing, and attraction, as well as fear of WaSH-related diseases. Additionally, there is the automatic or reflexive control, which is responsible for ‘habitual’ behaviour, learnt at an early age, automated and regularly triggered by a particular cue. Considering that 80% of respondents had taken part in sanitation training or sensitisation activity, which was positively associated with use of basic sanitation service, and given that risk perception is a major motivator for behaviour change [
43], well-designed communication strategies and health messaging could speak to a highly effective form to engage households to accept and use basic services [
33,
39,
44].
4.5. Limitations
A limitation lies in the cross-sectional design of the survey, which was useful for providing a snapshot of the situation and for associating the use of basic water and sanitation services with different explanatory factors, but, however, could not account for behaviours at different points of time. Originally, this study was supposed to compare not only the intervention and control areas, but also baseline data with post-intervention data. Due to major quality issues with the baseline data, no proper comparison was possible. Such would have allowed uncovering cause-effect relationships, e.g., in terms of seasonal differences in terms of use of services [
45].
Qualitative data, collected through open-ended questions as part of the household survey, in-depth interviews and focus group discussions, or through anthropological techniques such as photovoice [
14], would have added vital value to the findings of this study. Particularly in terms of health risk perceptions [
34] related to WaSH, which can only partly be captured by quantitative research, such approaches should be included in future studies for the sake of triangulation of findings [
12,
13]. Risk perceptions and health beliefs are complex, multi-dimensional and influenced by cultural practices and social factors [
2,
14,
33,
46,
47]. They can motivate the application of positive WaSH-related choices and health-related behaviours, inform health-related management [
34] and should therefore play a more prominent role in the design of WaSH programmes and evaluations.
This study included households that were mainly headed by males (91%). The small number of female-headed households detected prevented sex-disaggregation. The burden of limited or unimproved water and sanitation services, however, falls disproportionately on women, who bear responsibility for all related domestic tasks [
39], while caring for the children and the sick. Thus, viewing WaSH in the programme areas through a gender lens by comparing male- with female-headed households may have uncovered differences in terms of risk perceptions, as well as additional explanatory factors to the use of basic services.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}