1. Introduction
The use of gardens in healthcare has a long history [
1,
2], and today there is an increasing interest in, prevalence and use of therapy gardens as health facilities [
3]. An increasing body of research spanning multiple fields indicates that participation in nature-based therapy (NBT) in therapy gardens [
3,
4,
5,
6,
7,
8] result in positive health outcomes. In Scandinavia this has raised political awareness of the benefits of using nature areas in healthcare and as treatment facilities. In Denmark, several municipalities currently run or are planning therapy gardens. Hitherto, Danish therapy gardens have mostly been private initiatives. Currently, there is a demand across the municipal health authorities in Denmark for efficient and evidence-based treatment in general, including NBT [
9]. An evidence-based approach has the potential to provide suitable measures for bringing about improvements to the health outcome of a range of patient groups. With respect to NBT, an evidence-based approach has the potential to increase the likelihood of the effectiveness of this form of treatment. For this reason, several municipalities have sought support in the evidence-based health design in landscape architecture (EBHDL) for arguments put forward at governmental level for therapy garden projects. Over the course of the past decade, evidence-based design has evolved into health design, which is a branch of both architecture and landscape architecture. In Denmark, an often cited definition of health design in landscape architecture is: the conscious design of green spaces and gardens such that they in some way support health processes (and nature-based treatment programmes) and result in improved health outcomes [
10]. The design of the therapy garden is of great significance, and there are examples of gardens which have negative effects on patients. For instance, a survey found that 22% percent of patients at a care unit overlooking a garden which featured abstract design components reported an overall negative reaction to the garden [
2]. Accordingly, health design in landscape architecture may benefit from an evidence-based design approach.
Evidence-based health design in landscape architecture (EBHDL) has evolved from other disciplines that have used evidence-based models to guide decisions and practices in their respective fields [
11], e.g., evidence-based medicine (EBM) and evidence-based clinical practice (EBCP), in which clinical practitioners make decisions concerning the treatment, care and practice of individual patients based on current best evidence from research (EBM) and practice (EBCP) [
12,
13,
14]. The Center for Health Design defines evidence-based design (EBD) as: “
The process of basing decisions about the built environment on credible research to achieve the best possible outcomes” [
15]. EBHDL is based on definitions of EBD, although EBHDL specifically focuses on the design of landscapes, gardens or other natural environments with the aim of maximizing positive outcomes in terms of clients’ health and well-being. However, the process of EBHDL does not end when the design has been realised, since systematic and efficient evaluations are required in order to secure, maintain, and enhance positive health outcomes [
3,
10,
16,
17].
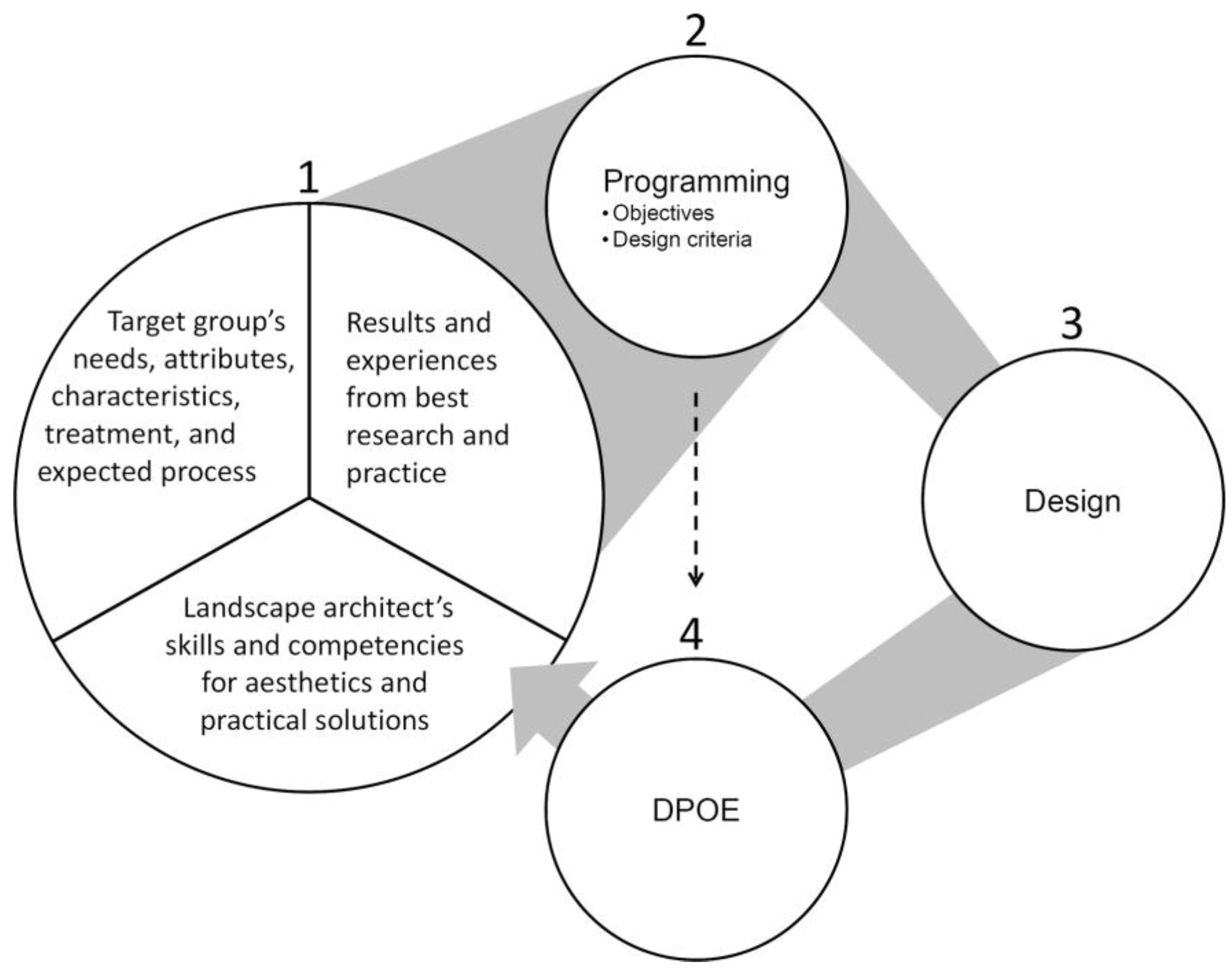
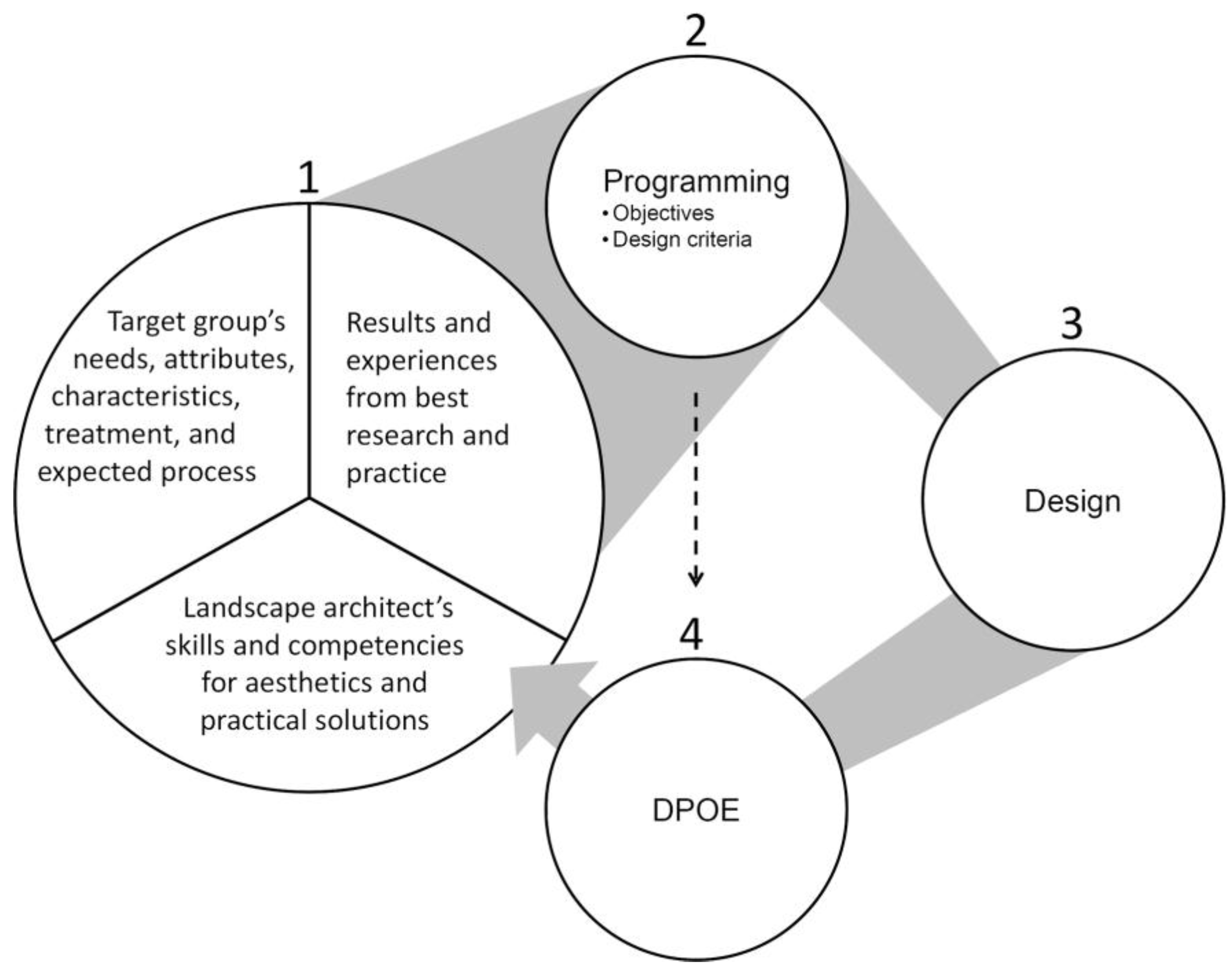
EBHDL is regarded as continuously explorative, evolving, and cyclical process of gaining experience, knowledge, and evidence from a current case in order to enhance patients’ health and well-being during treatment. An EBHDL model (
Figure 1) developed by the University of Copenhagen aims to describe the process transparently [
10]. The model consists of four parts. The first part comprises three equally important main components which must initially be considered: (1) Aesthetic and practical expertise with and experience of landscape architecture; (2) the specific user, patient or target group’s special needs, wishes and preferences; with respect to treatment, the treatment programme and the patient’s expected rehabilitation process must be taken into consideration; and (3) research evidence and relevant practical experience. These basic elements constitute the foundation for the next part of the model (part 2), which consists of the programming that guides the subsequent design. Here, the desired health outcomes and the objectives of the garden should be stated, together with details of how they will be achieved by means of the design (design criteria), as well as evidence to support the decisions on which the design is based. Evidence-based health design is, however, a process. A key aspect of this model is that the process does not stop when the design (part 3) has been realized. The idea is that the garden is continuously evaluated. This is achieved by means of part 4, which is a diagnostic post-occupancy evaluation (DPOE), which evaluates whether the design has fulfilled its aims and objectives (part 2).
Regarding post-occupancy evaluations (POE) of therapy gardens, Marcus and Sachs [
3] recommend making use of a diagnostic POE (DPOE), which should be conducted over a longitudinal time span using triangulation of mixed method and multiple sources of data to provide strong and reliable findings for a comprehensive and reflective evidence-based design process [
3].
The DPOE will illuminate the thinking behind the design decisions in order to clarify the aims and objectives of the design, determine the appropriate core area of examination for the specific site, and facilitate an evaluation based on the original aims and objectives of the case.
Different types of DPOEs are presented in the literature published on the subject. Guinther et al. [
16] describe DPOEs in relation to healthcare settings in general, while in Hopper [
17] and Marcus and Sachs [
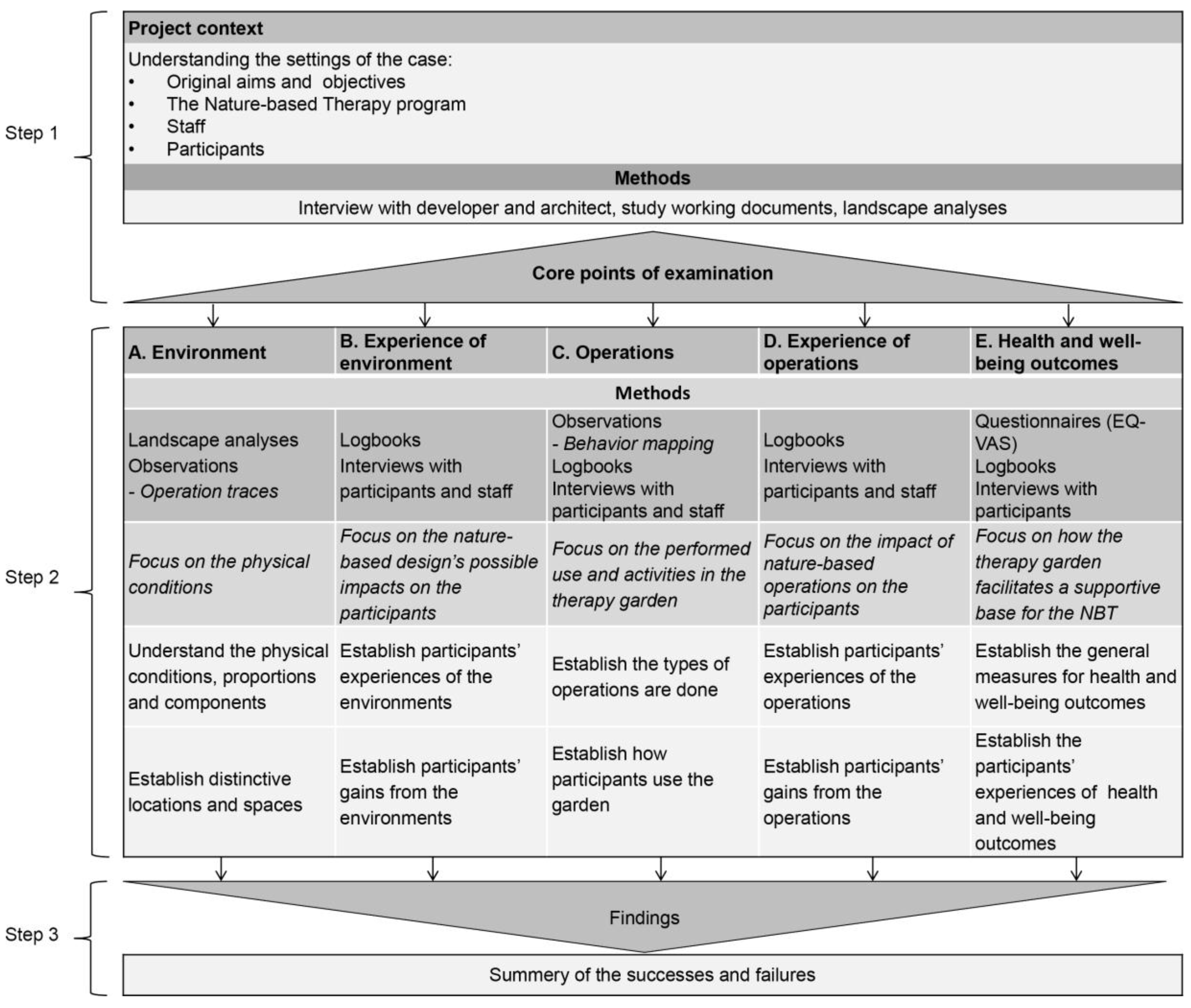
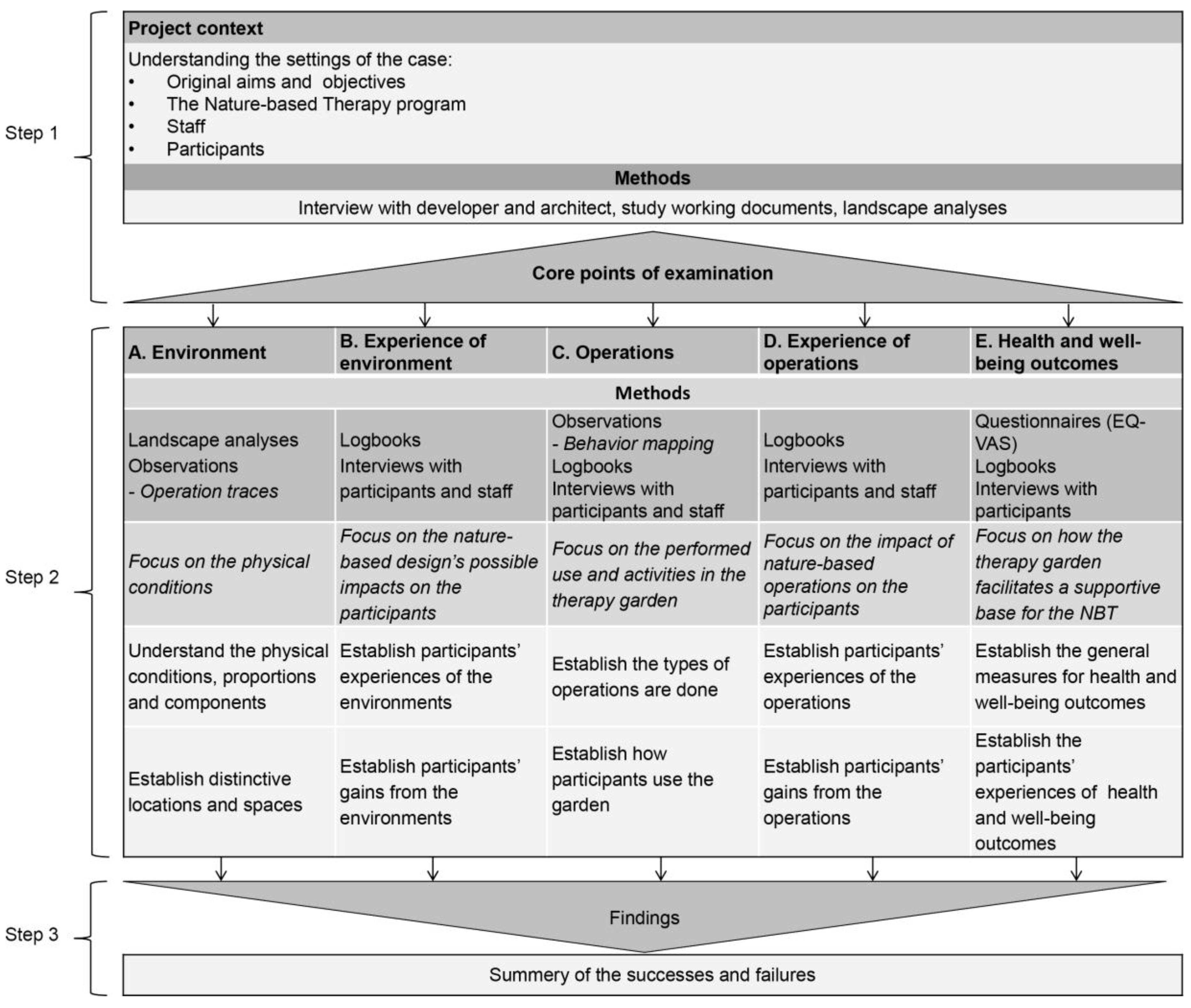
3], DPOEs are described in the context of landscape architecture and nature-based therapeutic settings, respectively. The DPOE in the current study is designated for therapy gardens and, for this purpose, a new form has been conceptualized (
Figure 2) which draws inspiration from the above-mentioned DPOEs. This is motivated by the definition of the concept of therapy gardens, according to which the design of the garden and the nature-based therapy programme are closely related [
18]. For this reason the DPOE utilised in the present study (
Figure 2) places an increased focus on patients’ experiences of and opinions and reflections on the garden environment, the different operations, and the potential impact on their health outcomes. The similarities and differences between the DPOEs employed in the present study and the aforementioned DPOEs are presented in
Table 1. The differences are motivated by the current DPOE, which is designated as a therapy garden, and according to which the number of participants and the operations are predefined in the NBT program. For example, Hopper’s [
17] DPOE is designated as landscape architecture in general, Guinther’s DPOE [
16] examines built healthcare settings in general, including all possible user groups, and Marcus and Sachs’ DPOE [
3] examines healing gardens, which do not have a specific patient group or NBT programme.
The aim of the current DPOE is to assess the initial design decisions in therapy garden projects by examining the effect of a therapy garden, and subsequently a nature-based therapy programme, on a specific patient group’s health outcomes. The DPOE consists of the following steps: (1) Project context; (2) examination of the five core points: Environment, Experiences of the environment, Operations, Experience of operations, and Health and well-being outcomes; and (3) findings (
Figure 2).
1.1. Presentation of the Case
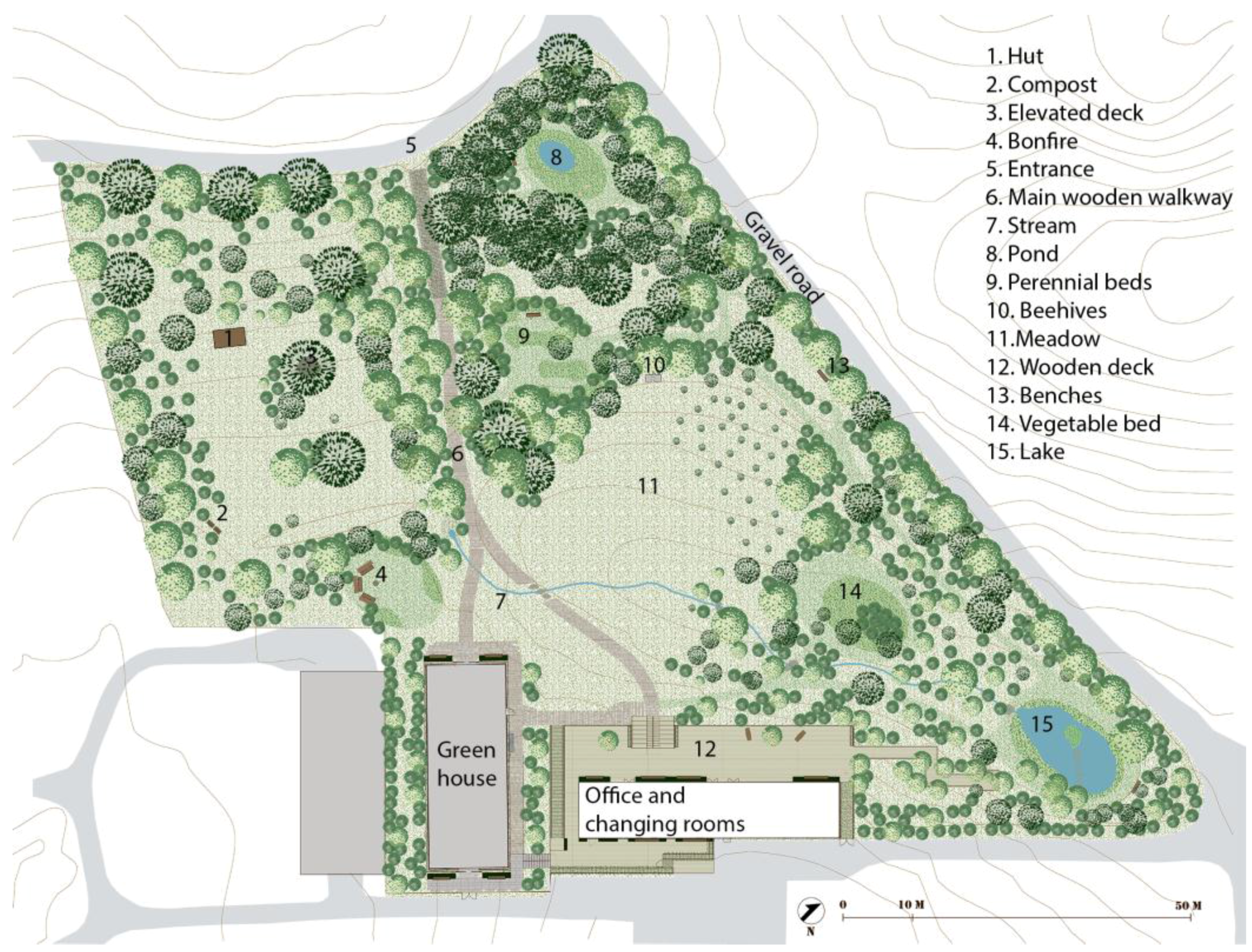
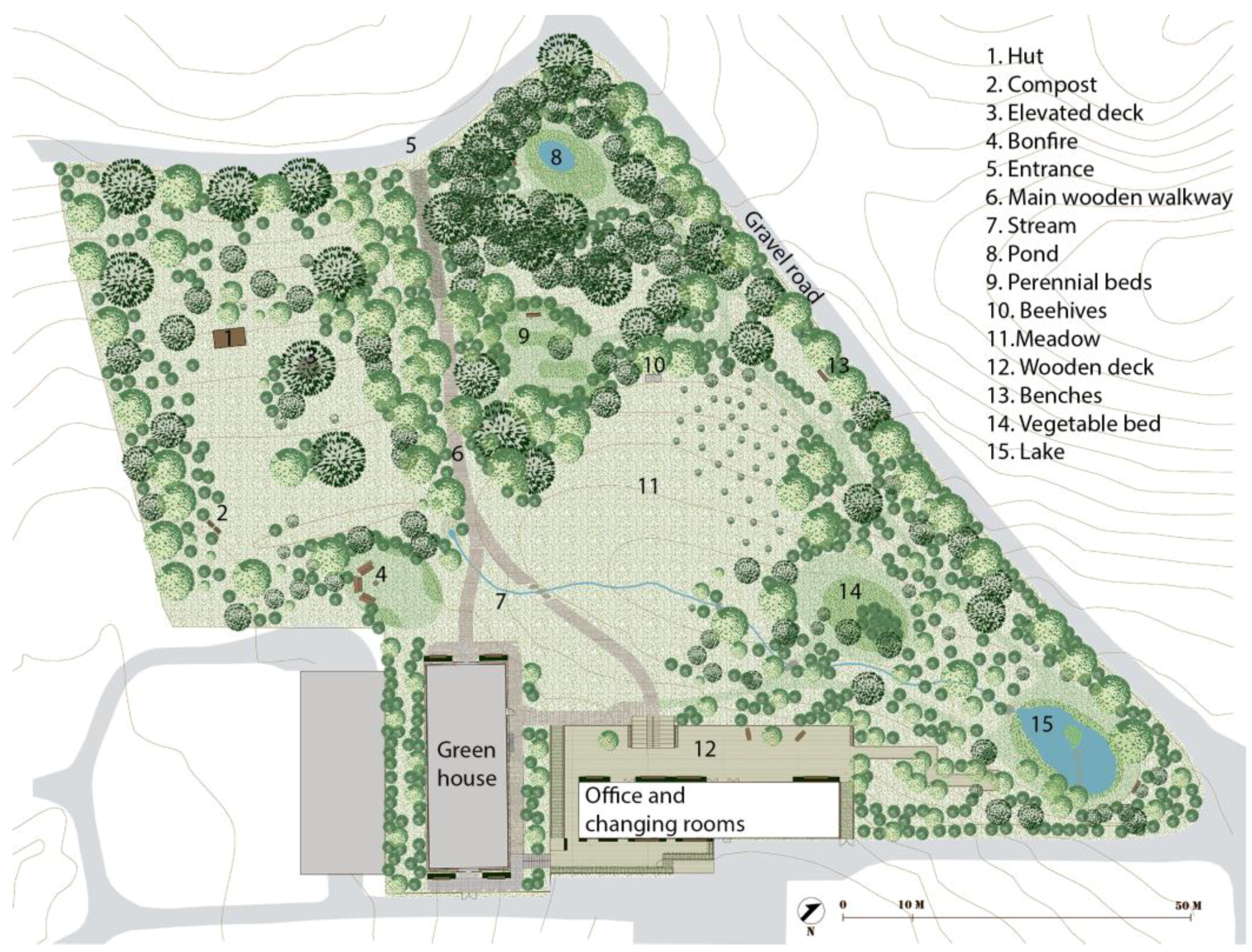
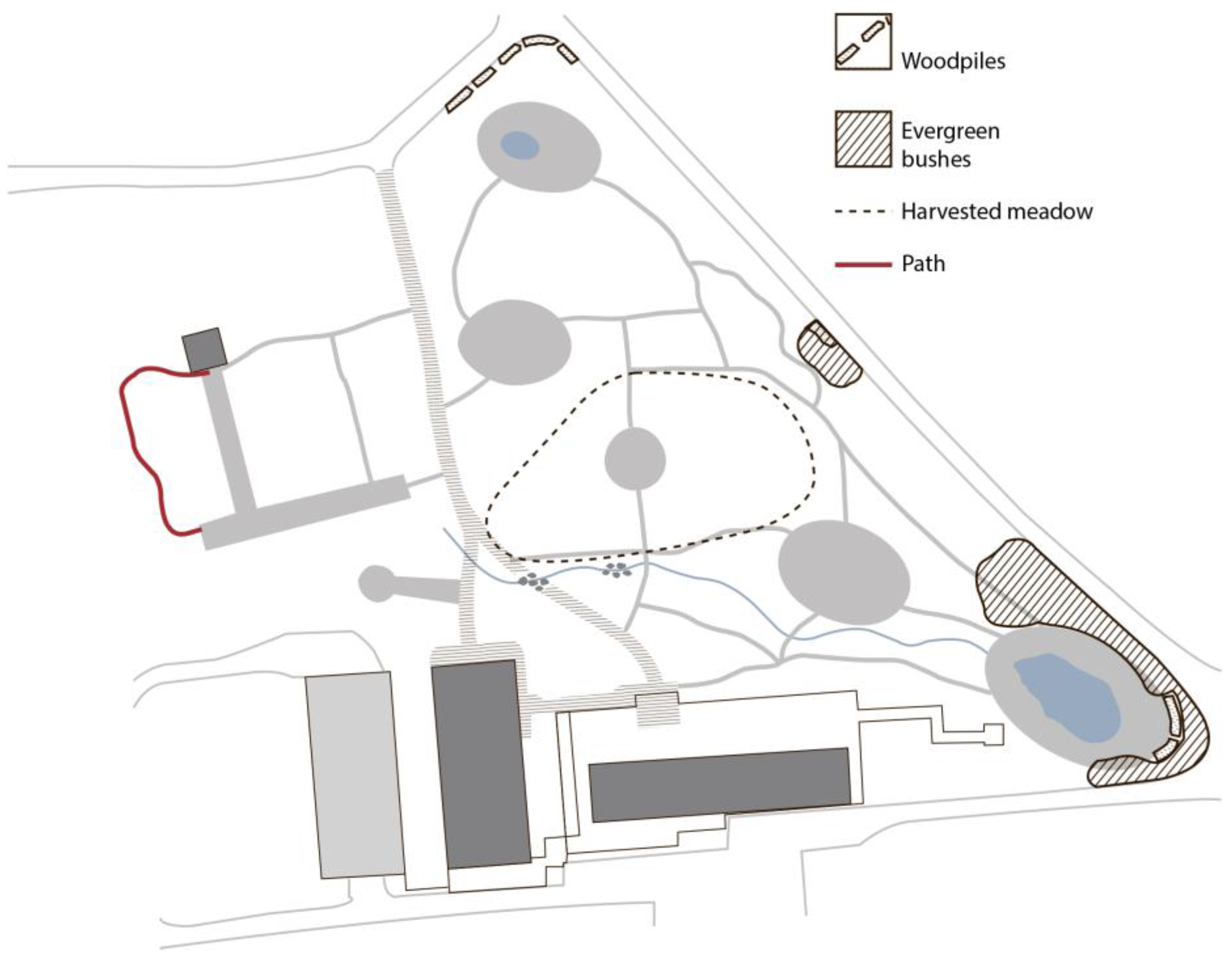
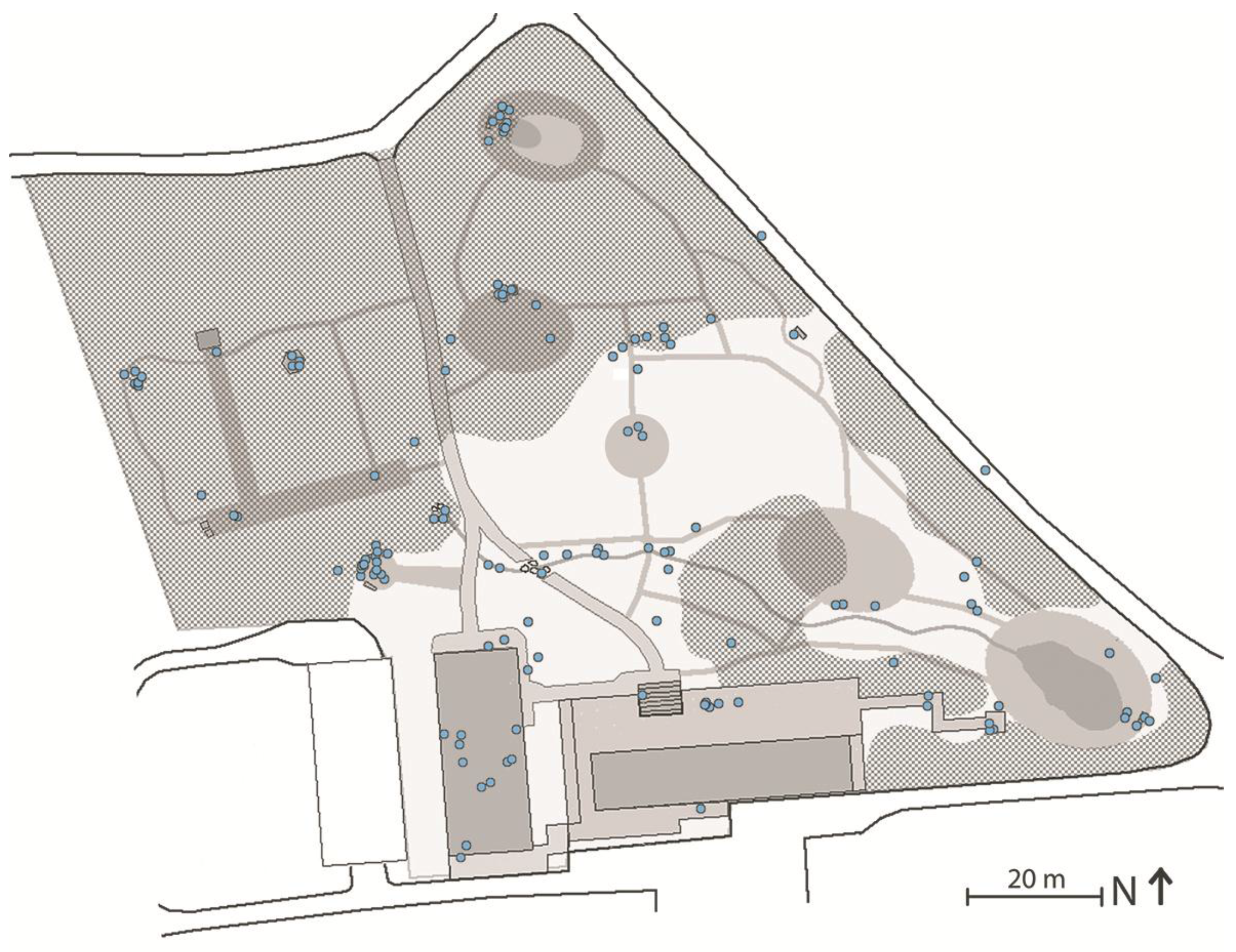
This study is a DPOE of the University of Copenhagen’s therapy garden, Nacadia®, which is located in the Arboretum in Hoersholm, approximately 30 km north of Copenhagen. The garden was designed according to the above-mentioned EBHDL model and was opened in 2011. It covers an area of 1.4 hectares and is located in the section of the arboretum that is home to a collection of trees and shrubs from North America. The terrain is slightly sloping from the highest point in the northern end to the lowest point in the south-eastern corner, lending it a slightly parabolic form. Nacadia® has a forest-like appearance.
The design of the garden is targeted at individuals who are suffering from stress-related illnesses. In the design phase, an NBT programme was developed [
18]. The NBT consists of the following five components: Individual conversational therapy, which is based on mindfulness cognitive therapy; Garden activities; Awareness exercises; Participants’ ‘own time’, and; Homework, the aim of which is for the participants to apply some of the experiences acquired in the therapeutic setting to their everyday situations [
18,
19]. The participants were divided into seven groups of 4–7 individuals for a 10-week NBT program, which ran from August 2013 to March 2015. The NBT programme was managed by two therapists who were assisted by a gardener.
1.2. Aim
The aim of this study is to apply the DPOE model (
Figure 2) to the design of the therapy garden, Nacadia
®. In comparison with the original aim and objectives of Nacadia
®, the current DPOE aims to assess the possible impact of the environment and the operations which comprise the NBT programme on patients’ wellbeing in order to identify possible successes and failures of the design.
The original aims and objectives of Nacadia
® were identified by applying step 1, ‘project context’, of the DPOE model (
Figure 2), which will resulted in the identification of the ‘core points of examination’. This was followed by step 2, examining the five core points. In step 3 ‘successes and failures’ were identified on the basis of the examinations.
4. Discussion
4.1. Results
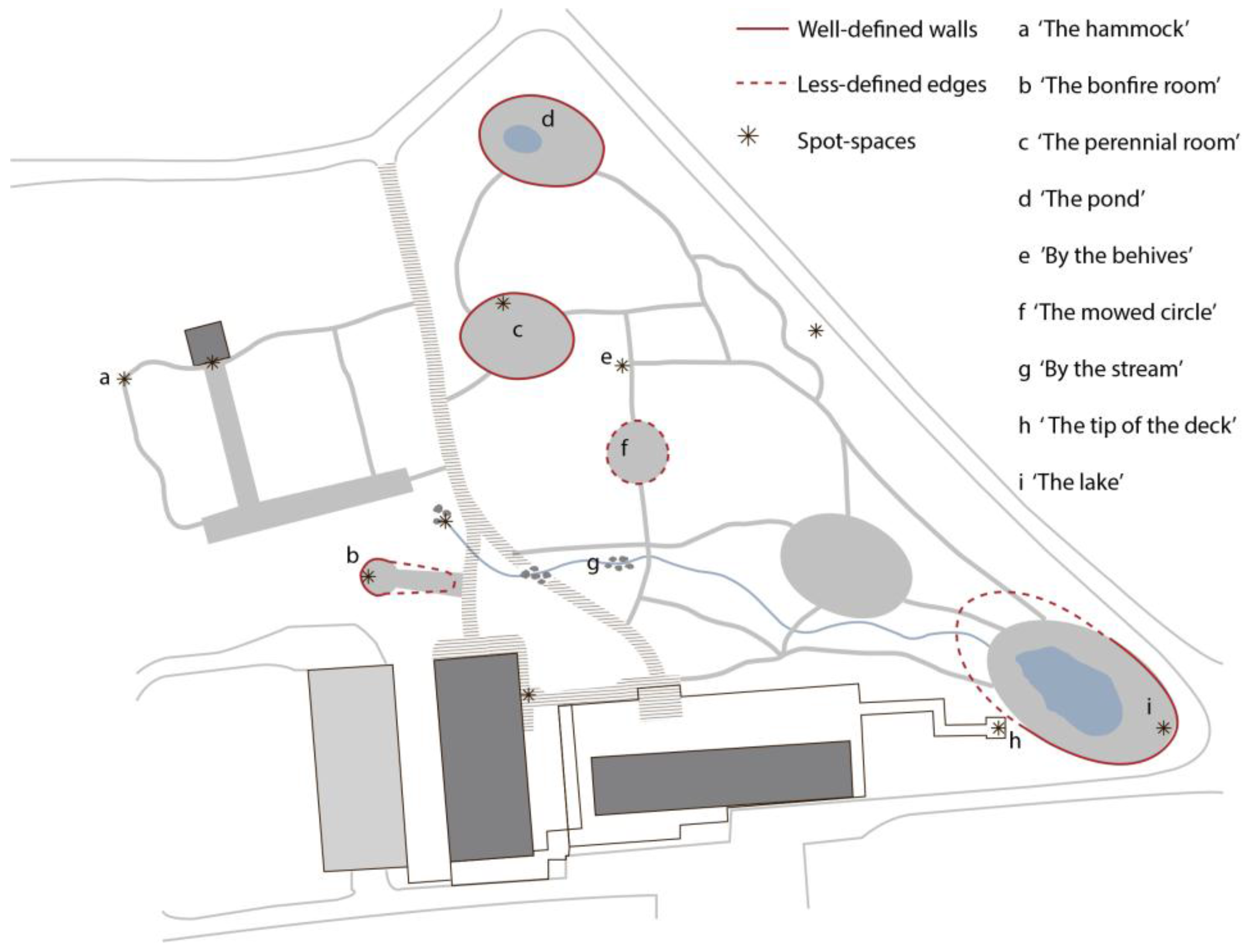
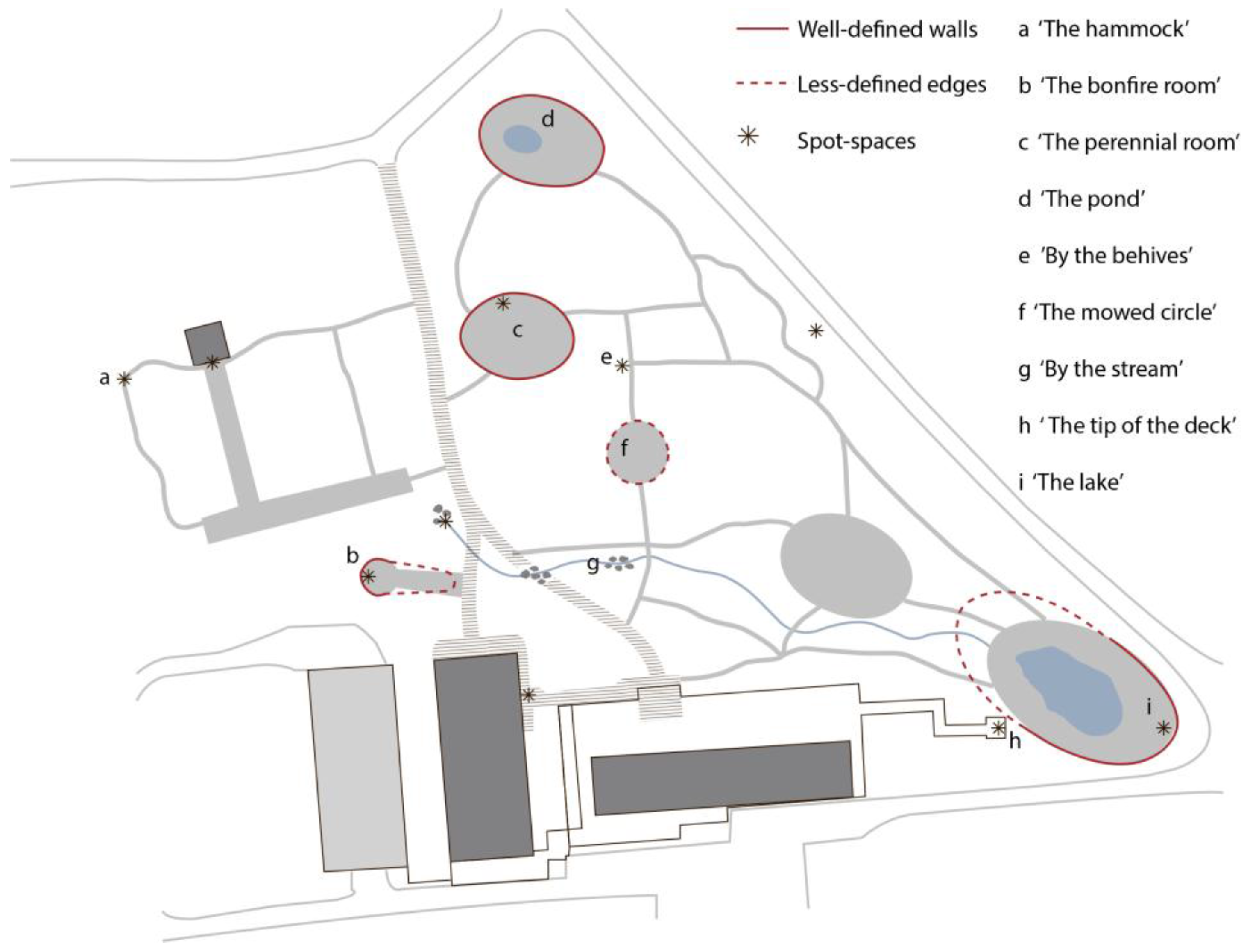
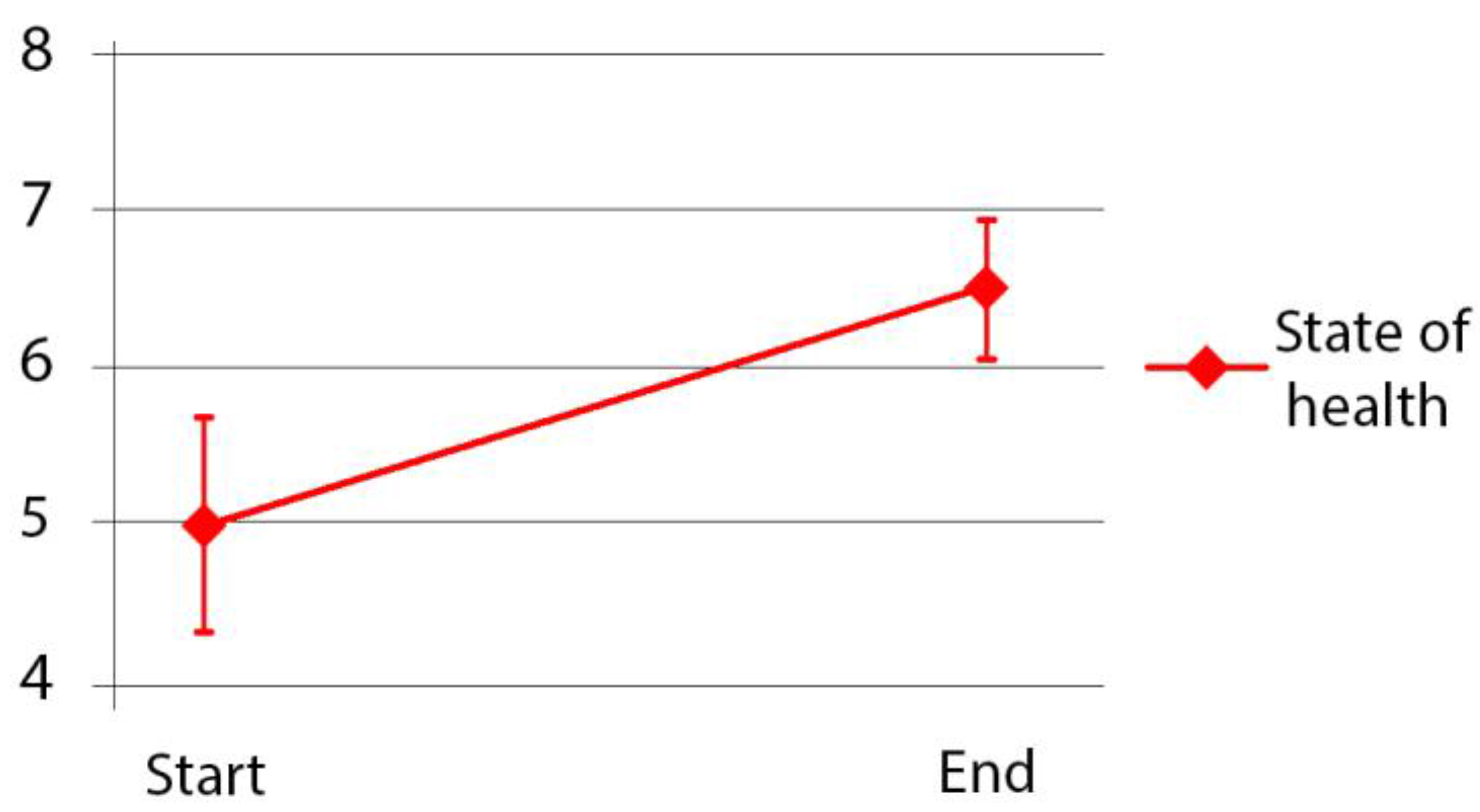
A number of successes and failures have been identified in relation to the original aims and objectives of Nacadia®. The original aim and objectives of Nacadia® appear to have been fulfilled. The participants experienced the setting as a safe and protective frame for the operations. This experience gave the participants a feeling of being free to engage, explore and even challenge themselves. Several distinctive spaces have been identified which are suitable for all the operations which comprise the NBT programme (‘awareness exercises’, ‘individual therapeutic conversations’, ‘garden activities’ and ‘own time’) which made it possible for the participants to find meaningful spaces and activities throughout the NBTN programme and in all four seasons of the year. The participants experienced improved memory, fewer cognitive problems, greater energy levels, and a significant improvement in self-assessed general health over the course of the NBTN programme.
Natural environments can promote health by allowing individuals to recuperate from mental fatigue [
35]. According to the Attention Restoration Theory (ART) proposed by Kaplan and Kaplan [
36] it is important to restore ‘directed attention’, while natural environments are considered good places in which to practice ‘effortless attention’, thereby providing a break from directed attention [
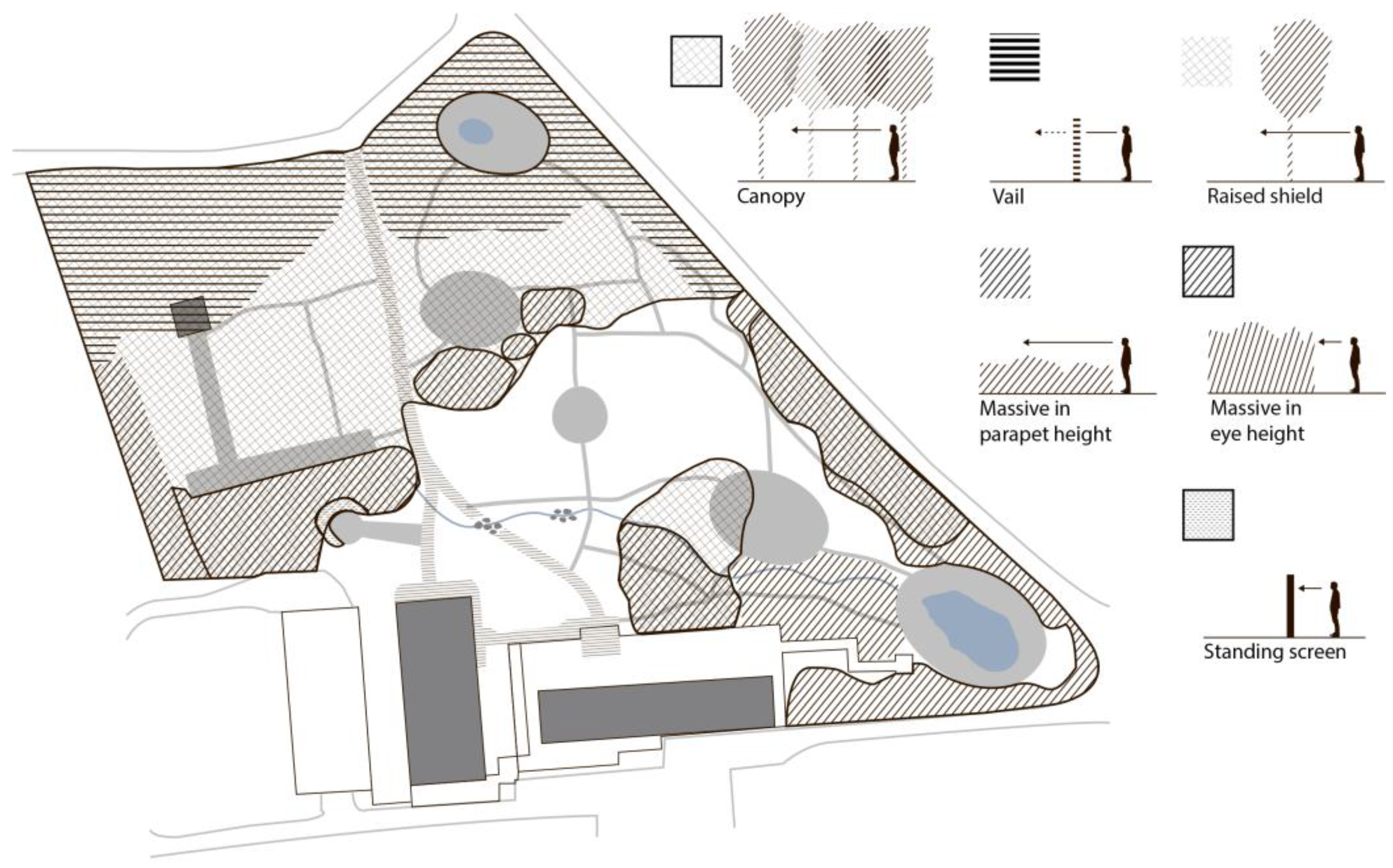
36]. In relation to the positive health impact of natural environments, some recent studies have attempted to identify and describe important spatial features of natural spaces with the goal of supporting psychological restoration [
37,
38]. These studies conclude that such spaces should be: enclosed at the sides and back as well as incorporating a canopy roof, while at the same time being open and providing a view. Furthermore, the plants in the space should have varied textures and shapes, and comfortable seating should be provided, as well as diverse sensory experiences [
37,
38]. The participants’ descriptions of the spatial conditions of the distinctive spaces in Nacadia of which they had the most positive experiences confirm these findings. These results can be related to Prospect-Refuge Theory [
39]. From an evolutionary perspective, Appleton [
39] proposed that people instinctively seek places in nature that have served a fundamental role in human survival in the earlier times [
39]. This theory states that enclosed spatial conditions (refuge) with an outlook (prospect) are experienced by humans as safe.
However, the findings from the current study stress that it is important that a therapy garden does not merely function as a safe room for psychological restoration. As is confirmed by the participants’ experiences of the environment, a prerequisite for an effective therapy garden design is that it constitutes an overall protective and safe environment that hosts a variety of distinctive spaces that can facilitate different operations and natural experiences of varying character, presenting varying challenges. The design will thus relate closely to the various operations of an NBT programme: it will engage a broad spectrum of individuals with various backgrounds, preferences and capabilities and it will match individual participants’ treatment processes by both supporting and challenging them over the course of the treatment. Nacadia
® constitutes such a protective and safe overall environment, for instance by being visually shielded and blocking out the ‘real world’. This leads participants to experience the overall environment as “fascinating” and makes them feel that they are “in another world”. Such experiences accord with ART [
36,
40], which states that a restorative environment should include the following four experiences: ‘Fascination’ (does not require the expenditure of mental effort and involves stimuli and processes of exploration); ‘Being away’ (the feeling, either psychological or physical, of being distant from daily routines and demands, where directed attention capacity is utilised); ‘Extent’ (the capacity of an environment to provide scope for exploration and a sense of coherence); ‘Compatibility’ (the correlation between what a person wants to do, what activities the environment supports and what the person is expected to do in the environment) [
40]. The participants’ sense of fascination and being away in another world promotes calmness and encourages them to explore and find ‘compatibility’ and ‘extent’ in accordance with their individual current needs and capabilities.
With respect to ART, the NBTN programme provides ‘fascination’ and ‘being away’ by providing the experience of being in an overall protective and safe environment distanced from day-to-day worries. The NBTN programme facilitates a spectrum of both concrete and symbolic opportunities, which is of crucial importance for the participants to find ‘extent’ and ‘compatibility’, which thereby provide a sense of meaning and support their treatment process and positive development.
On a number of occasions the participants shared stories of how, over the course of the treatment process, Nacadia® gave them opportunities to find spaces and operations that match their current capabilities, e.g., to get support to help them cope with their fears. For this reason it is important that the garden features various opportunities for the participants to select different spaces (environments) and operations and that the participants are made fully aware that is it possible and fully acceptable to seek to escape the space and engage in other activities more suited to their current needs and capabilities.
4.2. DPOE—A Key Element of the EBHDL Model
The EBHDL model (
Figure 1) was originally developed with the aim of strengthening the design process of therapy gardens in order to fulfil the design intentions of such gardens with respect to positive health outcomes. The first part of the model has been developed, applied and adjusted over a period of years, while part 4 has yet to be fully developed, and when planning the present study it was difficult to locate a satisfactory model of a POE to apply to the therapy garden. A need for such a POE was thus identified.
The literature describes three different types of POE: Indicative, Investigative, and Diagnostic, with the latter being the most comprehensive type [
3,
16,
41]. Guinther et al. [
16] conclude that no DPOE model fits all interventions, and that the methods applied must be tailored to the specific aims and objectives of the design in question [
16]. Three different versions of DPOE, proposed by Guither, Hopper, and Marcus and Sachs, respectively, have been previously described. However, since these did not cover the full examination of a therapy garden, it was necessary to develop version new model inspired by the aforementioned work. Previous research on Nacadia
® [
16,
42,
43] highlighted the importance of using mixed method triangulation in order to fully understand the impact of the garden environment and the NBT on the participants. Consequently, the current DPOE places an enhanced focus on the participants’ own experiences of, opinions of and reflections on the environment, the operations and the health outcomes. In contrast to the other DPOEs, there is less focus is on the staff’s use of and experiences of the environment. The staff’s role in managing the NBTN programme and guiding certain operations is examined via interviews.
Some key findings of the current study would have been difficult or impossible to discover without the enhanced focus on participants’ own experiences, their opinions of and reflections on their interactions with the environment and activities. These findings are: that the participants experienced the environment as safe and protective; that the participants felt free to explore and challenge themselves; that the participants found meaningful spaces and activities throughout all seasons of the year; that the participants increasingly experienced improved memory, fewer cognitive problems, and increased energy levels. Further, the fact that the DPOE was conducted over a long period of time, and included beginning- and end measures, made it possible to trace developments in and changes to the environment, and most importantly how the participants experienced benefits over time from participation in various operations, through the various seasons of the year, and in the varying physical conditions that the changing seasons brought with them.
The current DPOE model is considered suitable for evaluation of care environments that aim to motivate users to feel safe, and to have a positive impact on users’ wellbeing. In particular it is considered appropriate for care settings to implement natural environment and nature-based activities in which synergistic interaction between users, environments and operations are considered key success factors. Use of the current DPOE model may contribute to providing a rich understanding of interactions between users and environments and may thereby provide a deeper understanding of how to reconsider and adjust potential design failures in order to transform them into successes in relation to the specific user group, and in particular with respect to care settings.
In order to render the DPOE model user-friendly, it is presented as a generic and step-wise model, which means that it can be applied in a range of therapy gardens. The generic DPOE model can be tailored to suit the aim and objectives of the therapy garden, the therapy programme and patient groups. This is of relevance to all steps of the DPOE model, although the methods for measuring health outcomes in particular can vary depending on specific patient groups and intended health outcomes.
According to the EBHDL model, consideration should be given to the DPOE from the very beginning of the project. Clearly stating aims and objectives as early as the programming phase facilitates the DPOE process and may help to strengthen the results. The costs of carrying out the DPOE and any potential design modifications should be taken into account in the full budget for the therapy garden project.
The internal operational impacts of the DPOE process in Nacadia® have been on the design as well as on the NBT programme. Adjustments to the design have been made in Nacadia®, e.g., the woodpiles were built to resolve the problem of exposure and to enhance the participants’ feeling of safety. The various findings regarding the environment, the activities, and the participants’ interactions with these aspects are currently and will continuously be used for developing NBT programmes for future projects.
Furthermore the operational impact has an external dimension: the experiences and knowledge acquired from the DPOE have been used in the EBHDL process of the ‘Møllebæk’ therapy garden in Kolding municipality.
In general a well-implemented DPOE may be said to have a continuing and dynamic operational impact in that the data, findings, and knowledge acquired can be used for modifications to the design and in developing the NBT programme, thus enabling continuous alignment with the most up-to-date internal and external evidence in order to meet the needs of a specific user group in the most optimal manner.
4.3. Methods
Drawing on a triangulation approach, mixed methods are employed in the current DPOE as recommended by Guinther et al. [
16], Marcus and Sachs [
3], Stigsdotter et al. [
44], and Taylor and Francis [
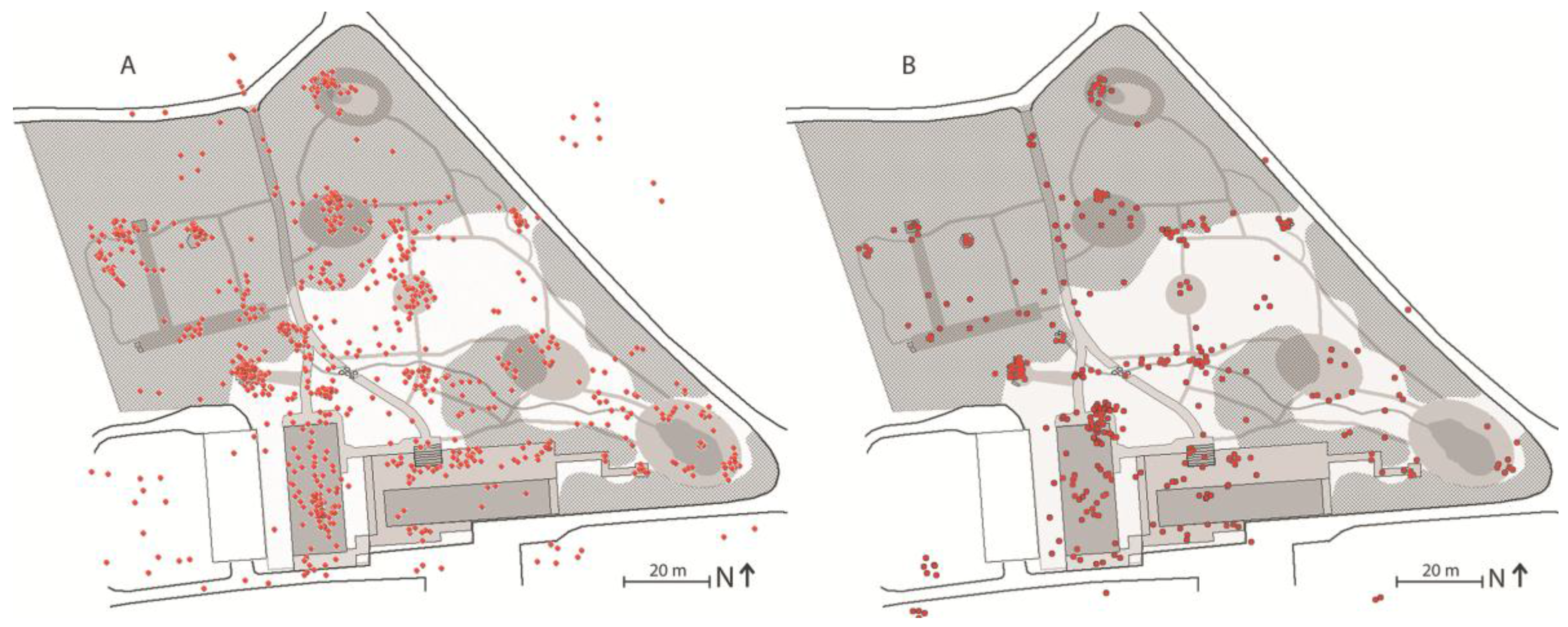
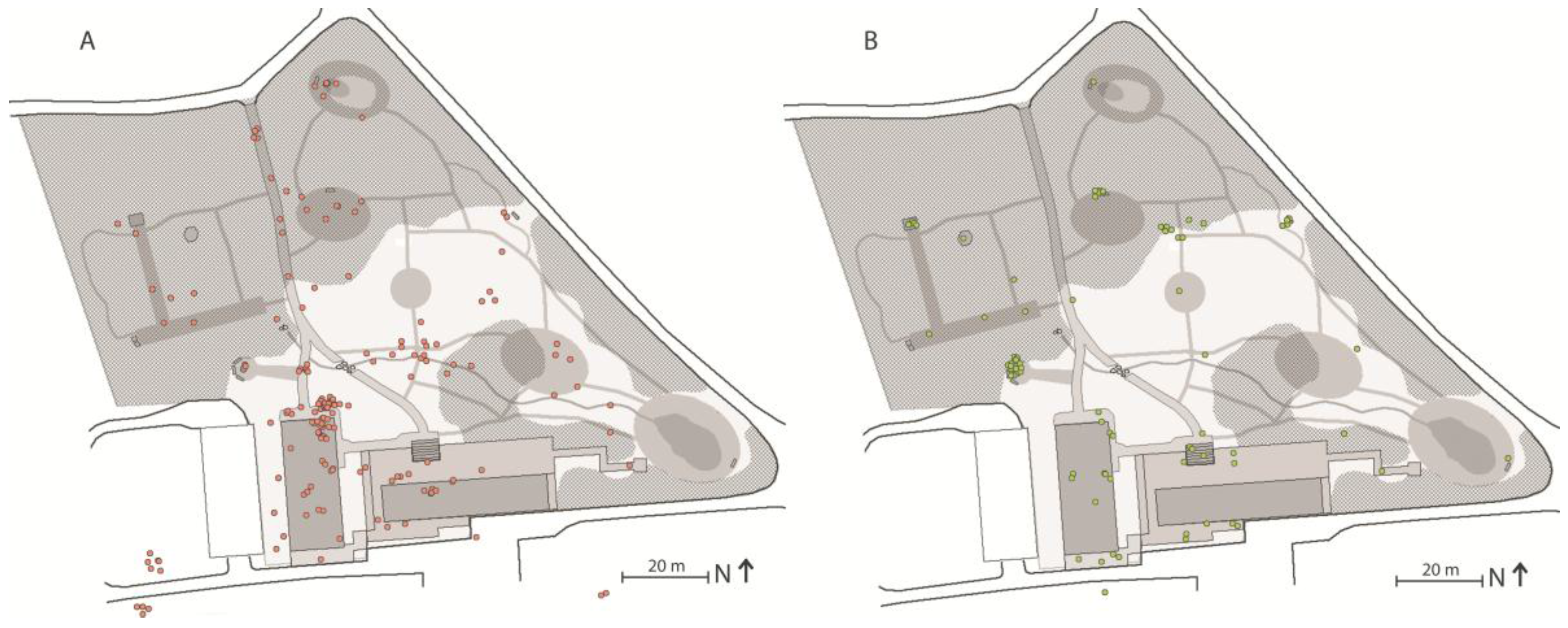
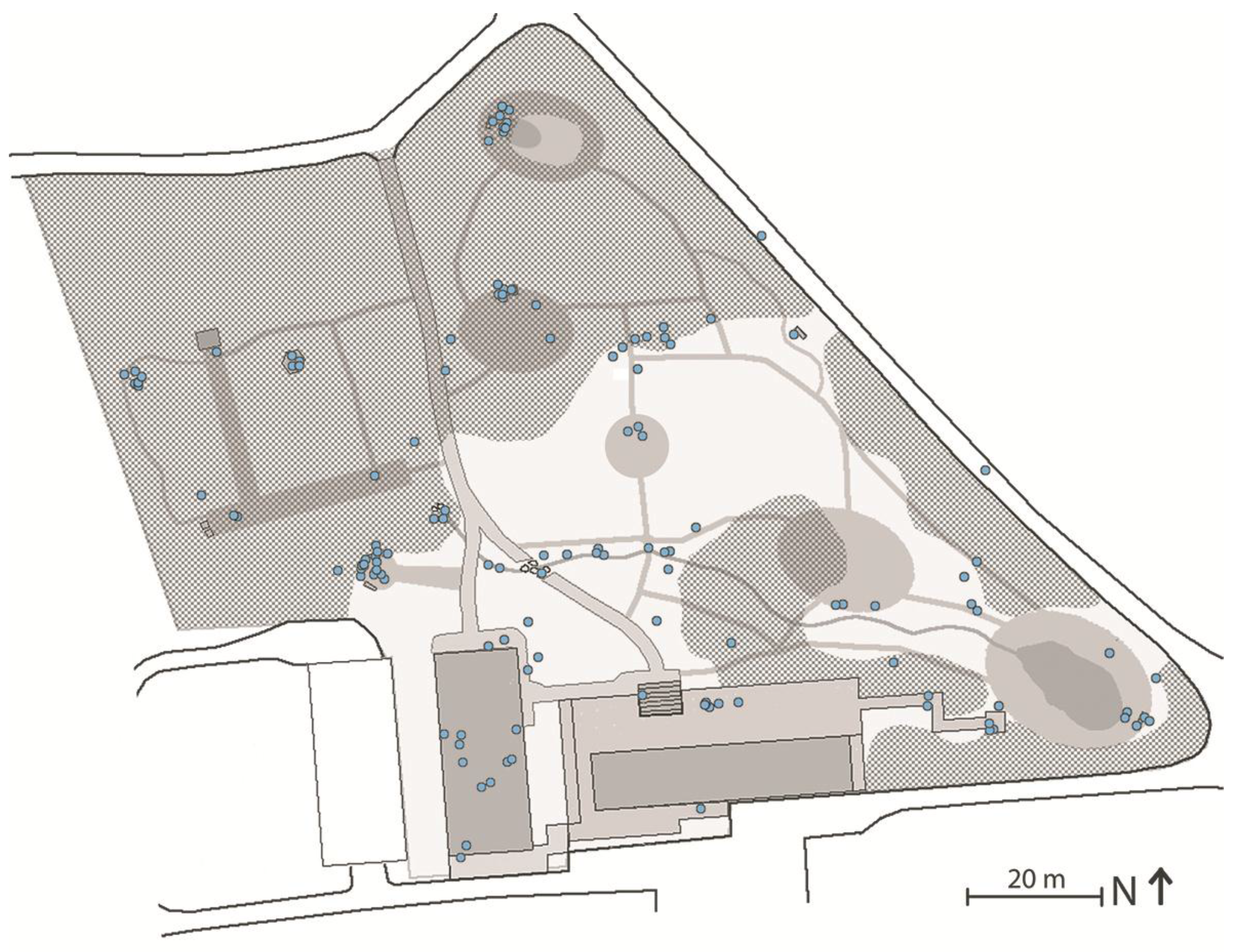
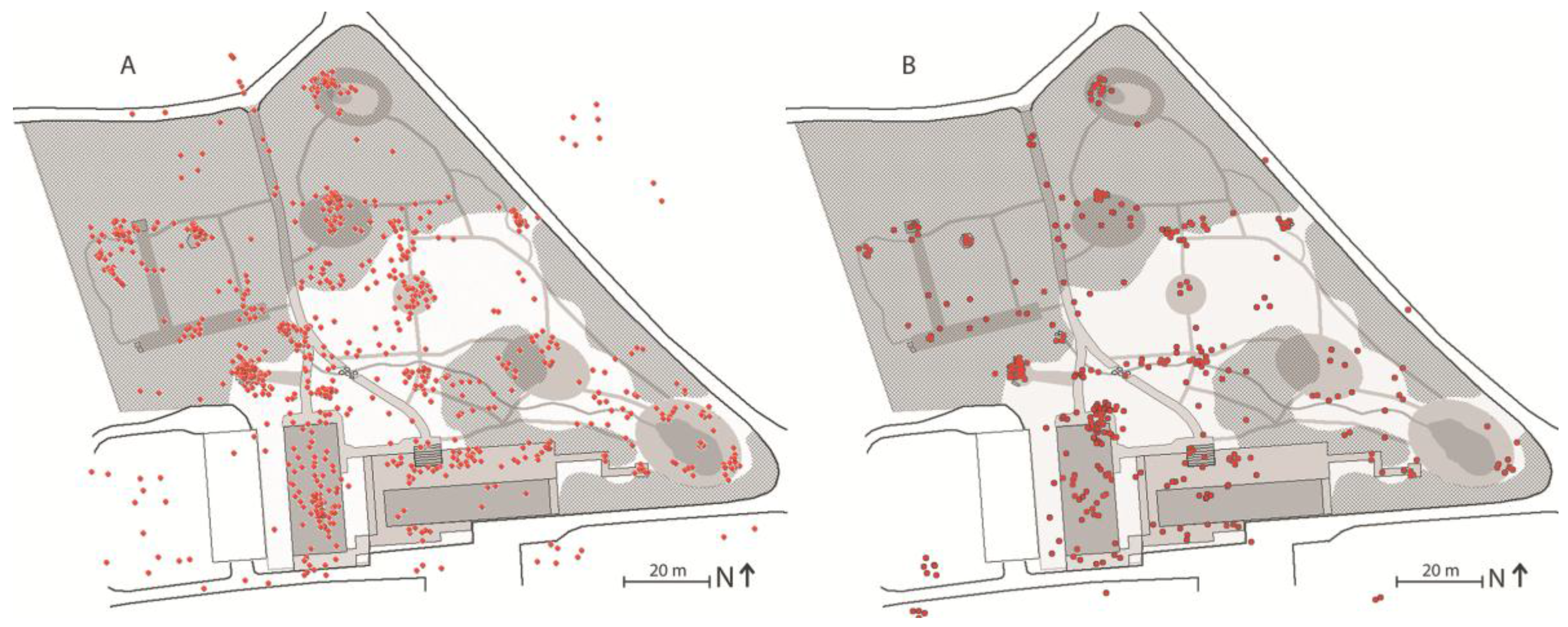
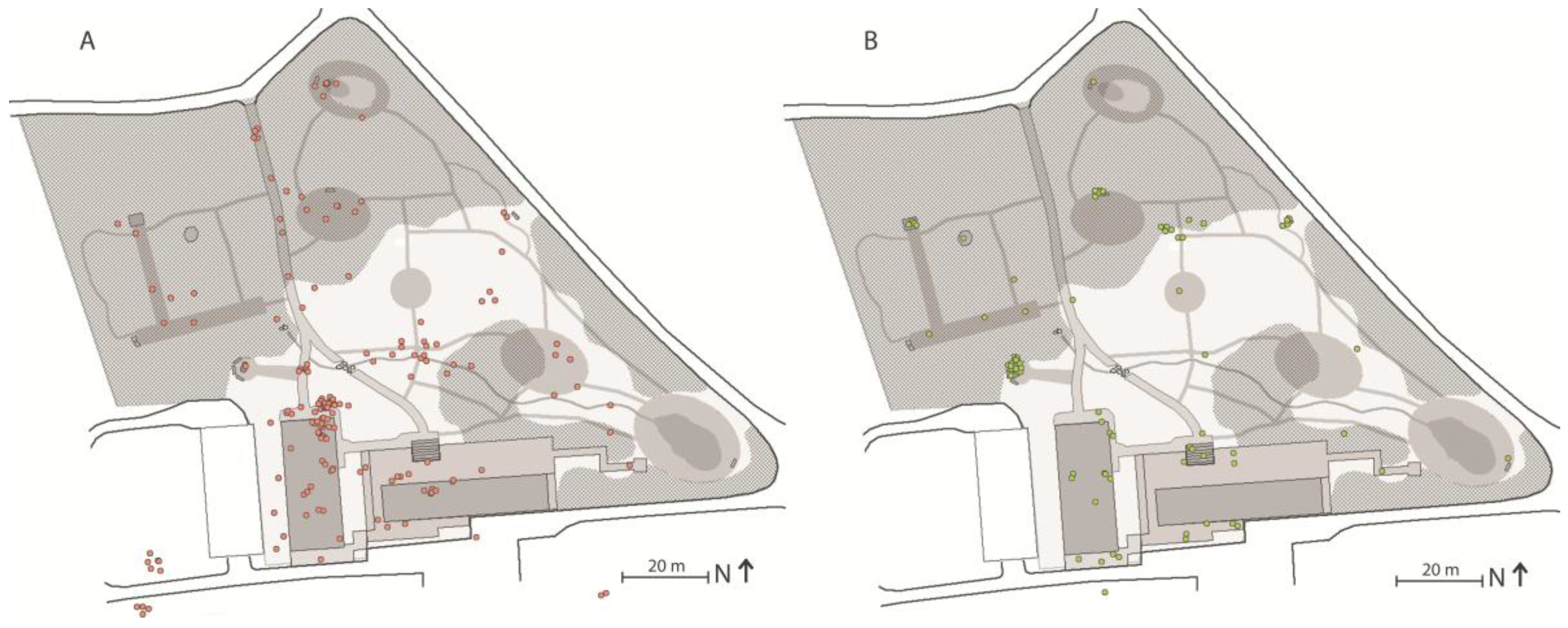
45] for DPOEs and in health science studies. The data from the various methods was corroborated during the examination of the core points of examination. Corroborating behaviour mapping, interviews and the spatial landscape analysis provided a comprehensive understanding of the participants’ experiences in the garden. Further, a concrete example illustrated the need to corroborate data from the behaviour mapping in order to gain a fuller understanding of this aspect: During the behaviour mapping, certain spaces were observed to be used less frequently than others. However, based upon the interviews, participants actually significantly preferred these same spaces. Participants recounted that there was a collective understanding on the part of the participants that these spaces were for solitary use, rather than social use. The logbook narratives provided further information in this respect; if these preferred spaces were occupied, the participants would go somewhere else. For this reason, the triangulation of methods was considered to yield more nuanced findings.
In general, the participants’ graphical mappings from the logbooks are too imprecise to be used quantitatively. The map in the logbooks which the participants were provided with in order to map their routes was small and was misunderstood by some. The logbooks were given to the participants to give them the opportunity to document their daily experiences and thoughts on a voluntary basis. The participants were more inclined to use the logbooks during the first half of the NBT period. Thus it was not possible to use the information from the logbooks to describe or quantify any development in their use or experiences of the garden from the start to the conclusion of the programme. The participants used various types of marking on the maps, which made them difficult to interpret. In future therapy garden projects, it is recommended that the logbooks include larger and better quality maps and clearer user instructions so that any markings users employ are more uniform. In order to make using the logbooks simpler, it is also recommended that fewer questions in general, and fewer open questions in particular, are included, together with a fixed set of factors to choose from when describing experiences of the garden and operations. Finally, in order to encourage the participants to use the logbooks throughout the entire NBT programme, time could be allocated in the daily programme for this purpose. This would support the DPOE, and would likely also support the participants given that they stated that they found that writing in the logbooks was beneficial for their recovery process.
4.4. Implications for Practitioners
The DPOE is part of the EBHDL model and is considered to be generic and, as such, applicable to other therapy garden projects. By presenting the DPOE as a stepwise model, the ambition is to make it user-friendly and provide the developer and/or therapy garden manager with a tool with which to identify the successes and failures of the design. By definition, a therapy garden should contribute positively to the participants’ health and wellbeing. Employing a DPOE that systematically examines the design of the therapy garden will provide knowledge of how the environment and the operations which take place there are experienced and what effect they have on the participants’ health. This knowledge is of potential relevance to both landscape architects and therapists.
The current DPOE was developed as part of a research project and is considered to be applicable to other therapy garden projects. In the final textbook of the COST Action E37 Forest, trees and human health [
5], the difficulties of comparing the results of different nature-based therapies were raised. By applying the EBHDL model and the DPOE model, it would be possible to transparently document the process and the results. However, the generic DPOE model would benefit from being applied to, and possibly validated by, other therapy gardens. At present collaborative projects are underway with a number of therapy gardens managed by municipalities in Denmark. An extra dimension here, which lends importance to the DPOE, is that the effectiveness of the garden projects can be examined thoroughly so as to provide evidence that can also be used as a basis for municipal healthcare decisions.
4.5. Limitations and Future Research
The present study aims to identify successes and failures in the design of the Nacadia® therapy garden. In accordance with the original aim and objectives of Nacadia®, successes and failures were identified in relation to the potential impact of the environment and the operations on the intended positive health outcomes.
Based on the DPOE it was established which environments and operations were positively experienced, and based on participants own narratives it was established how they experienced support and benefitted from the environment and the operations. The participants self-assessed general health status was found to have improved significantly during the course of the NBTN. This provides strong indications of positive impacts of the environment and the operations on the participants’ wellbeing. However, based on the present study it is not possible to establish whether it was the environment, the activities and/or the combination of the two that led to these significant improvements to the participants wellbeing, and thus conclusions as to what extent the environment and the operations have an impact on the measured positive health outcomes must be limited to strong assumptions. It should therefore be emphasized that there may be several other plausible explanations which cannot be excluded, given that the specific causalities have not been the focus of the present study. On the contrary, it was found that the participants had different needs and preferences that changed over the course of the NBTN in step with their individually fluctuating physical and mental capacities. The same environment and operation were found to have a different impact on the various participants. A specific operation beneficial for one participant may not be beneficial for other participants. During the NBT programme the participants were encouraged to complete homework assignments to test some of the activities which make up the NBT programme, and where possible to implement some of the tools that they have found to be specifically beneficial for them in their own life situations. This makes it even more difficult, not to say impossible, to exclude other possible causalities from the environment and operations in the NBT setting.
The NBT evaluated in the present study adopts a biopsychosocial and multispectral approach to human health as found in contemporary health science and clinical practice [
13,
45,
46]. The impact of the NBT components (environment and operations) should be considered in the context of the participants’ various and changing life situations, as the components of the NBT may not solely be the direct cause of the positive health outcomes. Since all human beings are different (e.g., biologically, social, personality), we all have different preferences and needs. An NBT operation beneficial for one patient may not be beneficial for others. In causality studies of therapy gardens it may be possible to identify a specific causality for one patient, while it may be more difficult to find common specific causalities. In cases of NBT intended for individuals suffering from severe stress, specific causality measures may not be of great significance, and could potentially even result in a limitation of the range of citizens who otherwise would benefit from the NBT. It is considered important that the environment and operations of NBT settings (and other care settings) are able to accommodate a wide range of people, and the present study demonstrates that a diverse group of people have all benefitted and developed individually from the therapeutic tools they have discovered, explored and developed over the course of the NBTN. This accords with the overall salutogenic approach of the NBTN [
5], which aims to consolidate what is already healthy within the participants [
47] by guiding and supporting them to discover and explore the potential health benefits within themselves, the environment and the activities.
There may be the risk that if a therapeutic setting is based on common specific causalities it will exclude some individuals, because this could potentially limit the spectrum in which the individual clients are allowed to explore and develop. This could be a concern for settings intended for patients suffering from stress-related illnesses, given that the ‘stress diagnosis’ is based on multidimensional stress-related symptoms [
48]. However, for settings intended for patient groups with more distinctive symptoms and pronounced needs, the findings of causality studies would be of great value.
Given that the current study does not provide knowledge of the specific causalities of the measured positive health outcomes, in-depth studies of the possible impact of the various specific NBT components on positive health outcomes is considered a relevant next step in order to provide more certain knowledge of specific causalities. The present study is a part of a major randomized clinical trial, the Nacadia® Effect Study (NEST), which aims to study causality. Over the course of the NEST a vast amount of data has been collected, and as the project continues all elements of the NEST will be utilised in an attempt to provide sound assumptions and knowledge of specific causalities in relation to the environment, activities and positive health outcomes for citizens suffering from stress-related illnesses.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}