Effect of Smoking Behavior before and during Pregnancy on Selected Birth Outcomes among Singleton Full-Term Pregnancy: A Murmansk County Birth Registry Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
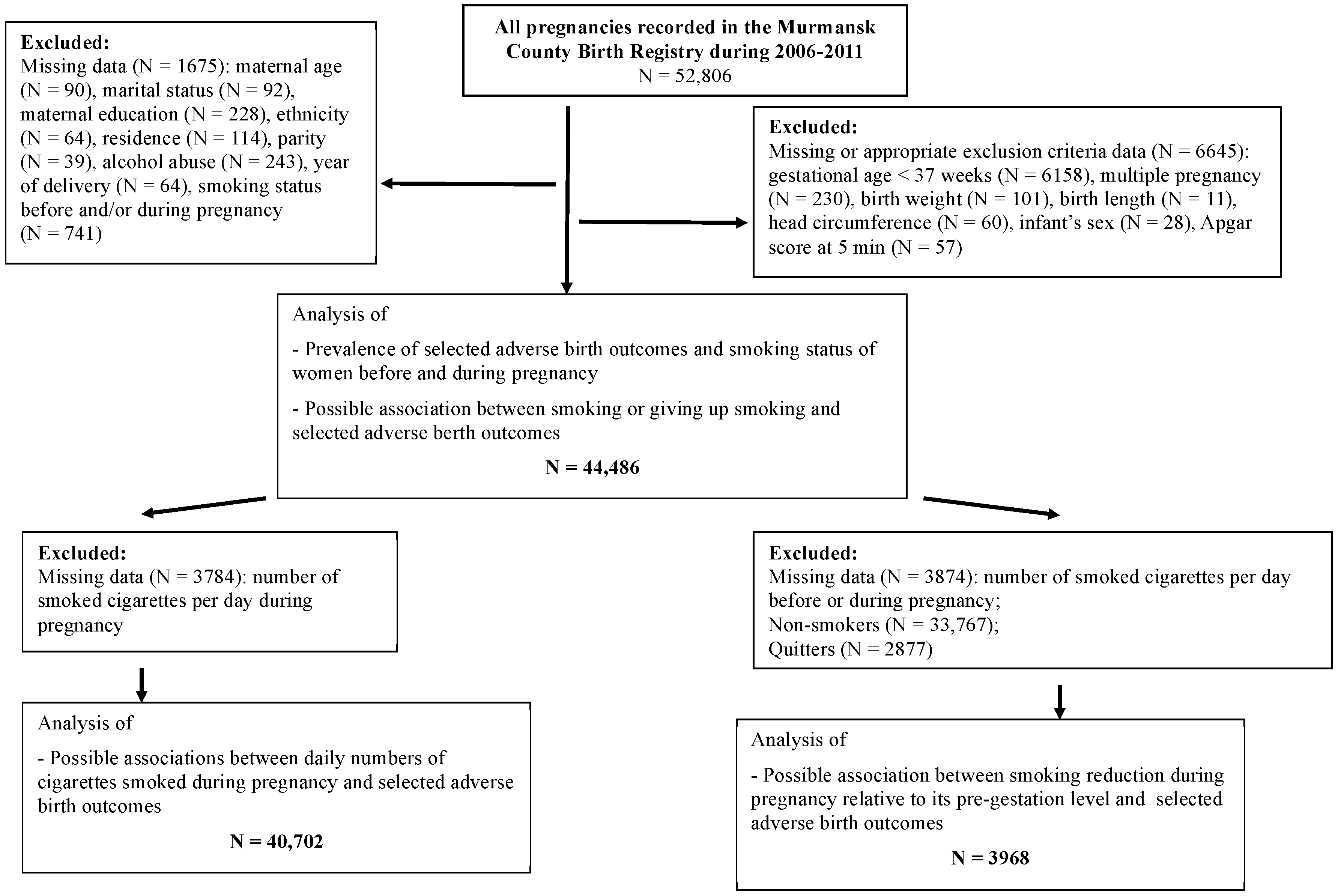
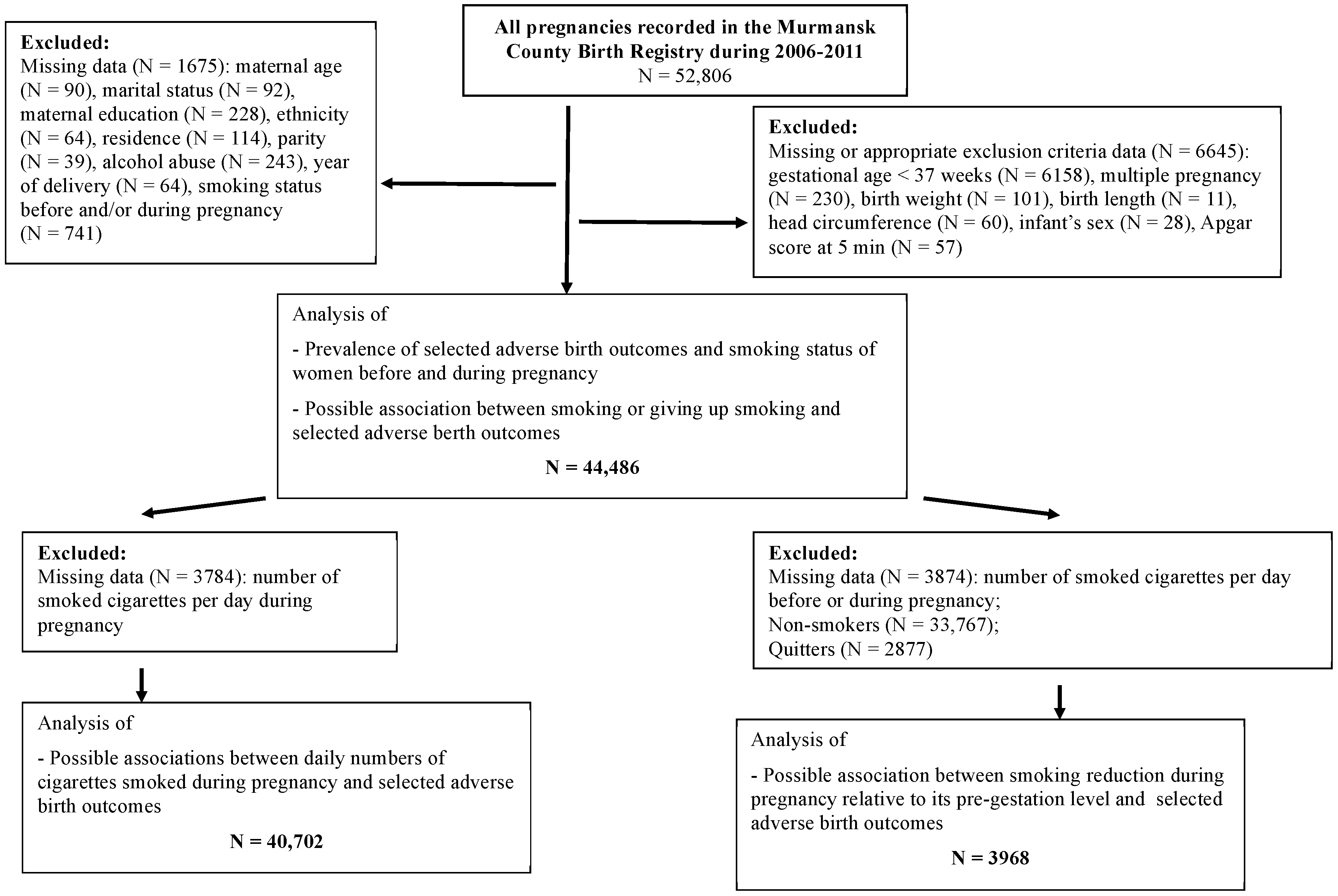
2.1. Study Setting, Design and Sample Size
2.2. Data Collection
2.3. Dependent Variable
2.4. Independent Variables
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Prevalence of Selected Adverse Birth Outcomes and Smoking Behaviour of Women before and during Pregnancy
3.2. Association between Daily Numbers of Smoked Cigarettes during Pregnancy and Selected Adverse Birth Outcomes among Women with Singleton Full-Term Pregnancies
3.3. Association of Selected Adverse birth Outcomes and Smoking, Giving-Up Smoking, or Smoking Reduction
4. Discussion
4.1. Main Findings
4.2. Data Interpretation and Comparisons with Previous Studies
4.2.1. Smoking before and during Pregnancy
4.2.2. Daily Number of Cigarettes Smoked during Pregnancy
4.2.3. Giving up Smoking in the First-Trimester
4.2.4. Smoking Reduction during Pregnancy Compared to Pre-Gestation Level
4.3. Limitations and Strengths
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tobacco USE. Data by Country. WHO. Available online: http://apps.who.int/gho/data/node.main.65 (accessed on 13 June 2017).
- Grjibovski, A.; Bygren, L.O.; Svartbo, B. Socio-demographic determinants of poor infant outcome in north-west Russia. Paediatr. Perinat Epidemiol. 2002, 16, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Kharkova, O.A.; Krettek, A.; Grjibovski, A.M.; Nieboer, E.; Odland, J.O. Prevalence of smoking before and during pregnancy and changes in this habit during pregnancy in Northwest Russia: A Murmansk County Birth Registry study. Reprod. Health 2016, 13, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zdravkovic, T.; Genbacev, O.; McMaster, M.T.; Fisher, S.J. The adverse effects of maternal smoking on the human placenta: A review. Placenta 2005, 26 (Suppl. A), S81–S86. [Google Scholar] [CrossRef] [PubMed]
- Tikkanen, M.; Nuutila, M.; Hiilesmaa, V.; Paavonen, J.; Ylikorkala, O. Prepregnancy risk factors for placental abruption. Acta Obstet. Gynecol. Scand. 2006, 85, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Oyelese, Y.; Smulian, J.C. Placenta Previa, placenta accreta, and vasa Previa. Obstet. Gynecol. 2006, 107, 927–941. [Google Scholar] [CrossRef] [PubMed]
- Saraiya, M.; Berg, C.J.; Kendrick, J.S.; Strauss, L.T.; Atrash, H.K.; Ahn, Y.W. Cigarette smoking as a risk factor for ectopic pregnancy. Am. J. Obstet. Gynecol. 1998, 178, 493–498. [Google Scholar] [CrossRef]
- Mishra, G.D.; Dobson, A.J.; Schofield, M.J. Cigarette smoking, menstrual symptoms and miscarriage among young women. Aust. N. Z. J. Public Health 2000, 24, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Burton, G.J. Morphological and biological effects of maternal exposure to tobacco smoke on the feto-placental unit. Early Hum. Dev. 2007, 83, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Naruse, H.; Yorifuji, T.; Kato, T.; Murakoshi, T.; Doi, H.; Subramanian, S.V. Impact of maternal and paternal smoking on birth outcomes. J. Public Health (Oxf.) 2016. [Google Scholar] [CrossRef] [PubMed]
- Timur Taşhan, S.; Hotun Sahin, N.; Omaç Sönmez, M. Maternal smoking and newborn sex, birth weight and breastfeeding: A population-based study. J. Matern.-Fetal Neonatal Med. 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Tikellis, G.; Sun, C.; Pezic, A.; Wang, L.; Wells, J.C.; Cochrane, J.; Ponsonby, A.L.; Dwyer, T. The effect of maternal prenatal smoking and alcohol consumption on the placenta-to-birth weight ratio. Placenta 2014, 35, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.J.; Tsai, L.Y.; Chu, L.C.; Yeh, S.J.; Leung, C.; Chen, C.Y.; Chou, H.C.; Tsao, P.N.; Chen, P.C.; Hsieh, W.S. Parental smoking during pregnancy and its association with low birth weight, small for gestational age, and preterm birth offspring: A birth cohort study. Pediatr. Neonatol. 2014, 55, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Benjamin-Garner, R.; Stotts, A. Impact of smoking exposure change on infant birth weight among a cohort of women in a prenatal smoking cessation study. Nicotine Tob. Res. 2013, 15, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.; Lewis, S.; Coleman, T. Prevalence of maternal smoking and environmental tobacco smoke exposure during pregnancy and impact on birth weight: Retrospective study using Millennium Cohort. BMC Public Health 2007, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Durmus, B.; Kruithof, C.J.; Gillman, M.H.; Willemsen, S.P.; Hofman, A.; Raat, H.; Eilers, P.H.; Steegers, E.A.; Jaddoe, V.W. Parental smoking during pregnancy, early growth, and risk of obesity in preschool children: The Generation R Study. Am. J. Clin. Nutr. 2011, 94, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Kallen, K. Maternal smoking during pregnancy and infant head circumference at birth. Early Hum. Dev. 2000, 58, 197–204. [Google Scholar] [CrossRef]
- Jaddoe, V.W.; Verburg, B.O.; de Ridder, M.A.; Hofman, A.; Mackenbach, J.P.; Moll, H.A.; Steegers, E.A.; Witteman, J.C. Maternal smoking and fetal growth characteristics in different periods of pregnancy: The generation R study. Am. J. Epidemiol. 2007, 165, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Ingvarsson, R.F.; Bjarnason, A.O.; Dagbjartsson, A.; Hardardottir, H.; Haraldsson, A.; Thorkelsson, T. The effects of smoking in pregnancy on factors influencing fetal growth. Acta Paediatr. 2007, 96, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Grjibovski, A.; Bygren, L.O.; Svartbo, B.; Magnus, P. Housing conditions, perceived stress, smoking, and alcohol: Determinants of fetal growth in Northwest Russia. Acta Obstet. Gynecol. Scand. 2004, 83, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Haste, F.M.; Anderson, H.R.; Brooke, O.G.; Bland, J.M.; Peacock, J.L. The effects of smoking and drinking on the anthropometric measurements of neonates. Paediatr. Perinat. Epidemiol. 1991, 5, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Lindley, A.A.; Gray, R.H.; Herman, A.A.; Becker, S. Maternal cigarette smoking during pregnancy and infant ponderal index at birth in the Swedish Medical Birth Register, 1991–1992. Am. J. Public Health 2000, 90, 420–423. [Google Scholar] [PubMed]
- Apgar, V. A proposal for a new method of evaluation of the newborn infant. Curr. Res. Anesth. Analg. 1953, 32, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, S.; Mackay, D.F.; Smith, G.C.; Pell, J.P.; Nelson, S.M. Apgar score and the risk of cause-specific infant mortality: A population-based cohort study. Lancet 2014, 384, 1749–1755. [Google Scholar] [CrossRef]
- Walfisch, A.; Nikolovski, S.; Talevska, B.; Hallak, M. Fetal growth restriction and maternal smoking in the Macedonian Roma population: A causality dilemma. Arch. Gynecol. Obstet. 2013, 287, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Anda, E.E.; Nieboer, E.; Voitov, A.V.; Kovalenko, A.A.; Lapina, Y.M.; Voitova, E.A.; Kovalenko, L.F.; Odland, J.Ø. Implementation, quality control and selected pregnancy outcomes of the Murmansk County Birth Registry in Russia. Int. J. Circumpolar Health 2008, 67, 318–334. [Google Scholar] [CrossRef] [PubMed]
- WHO. Available online: http://www.who.int/childgrowth/standards/ru/ (accessed on 26 January 2017).
- United Nations Children’s Fund and World Health Organization. Low Birthweight: Country, Regional and Global Estimates; UNICEF: New York, NY, USA, 2004. [Google Scholar]
- Suzuki, K.; Shinohara, R.; Sato, M.; Otawa, S.; Yamagata, Z. Association between Maternal Smoking during Pregnancy and Birth Weight: An Appropriately Adjusted Model From the Japan Environment and Children’s Study. J. Epidemiol. 2016, 26, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Veloso, H.J.; da Silva, A.A.; Bettiol, H.; Goldani, M.Z.; Filho, F.L.; Simoes, V.M.; Batista, R.F.; Barbieri, M.A. Low birth weight in Sao Luis, northeastern Brazil: Trends and associated factors. BMC Pregnancy Childbirth 2014, 14, 155. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Yorifuji, T.; Inoue, S.; Doi, H.; Kawachi, I. Association of birth length and risk of hospitalisation among full-term babies in Japan. Paediatr. Perinat. Epidemiol. 2013, 27, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.R.; Simonsen, U.; Uldbjerg, N.; Aalkjaer, C.; Stender, S. Smoking cessation early in pregnancy and birth weight, length, head circumference, and endothelial nitric oxide synthase activity in umbilical and chorionic vessels: An observational study of healthy singleton pregnancies. Circulation 2009, 119, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Roza, S.J.; Verburg, B.O.; Jaddoe, V.W.; Hofman, A.; Mackenbach, J.P.; Steegers, E.A.; Witteman, J.C.; Verhulst, F.C.; Tiemeier, H. Effects of maternal smoking in pregnancy on prenatal brain development: The Generation R Study. Eur. J. Neurosci. 2007, 25, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Fattal-Valevski, A.; Toledano-Alhadef, H.; Leitner, Y.; Geva, R.; Eshel, R.; Harel, S. Growth patterns in children with intrauterine growth retardation and their correlation to neurocognitive development. J. Child Neurol. 2009, 24, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Howe, L.D.; Matijasevich, A.; Tilling, K.; Brion, M.J.; Leary, S.D.; Smith, G.D.; Lawlor, D.A. Maternal smoking during pregnancy and offspring trajectories of height and adiposity: Comparing maternal and paternal associations. Int. J. Epidemiol. 2012, 41, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Gray, T.R.; Eiden, R.D.; Leonard, K.E.; Connors, G.; Shisler, S.; Huestis, M.A. Nicotine and metabolites in meconium as evidence of maternal cigarette smoking during pregnancy and predictors of neonatal growth deficits. Nicotine Tob. Res. 2010, 12, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Su, S.J.; River, L.P. Comparison of associated high-risk factors and perinatal outcome between symmetric and asymmetric fetal intrauterine growth retardation. Am. J. Obstet. Gynecol. 1991, 164 Pt 1, 1535–1541. [Google Scholar] [CrossRef]
- Garn, S.M.; Johnston, M.; Ridella, S.A.; Petzold, A.S. Effect of maternal cigarette smoking on Apgar scores. Am. J. Dis. Child. 1981, 135, 503–506. [Google Scholar] [PubMed]
- Bosley, A.R.; Newcombe, R.G.; Dauncey, M.E. Maternal smoking and Apgar score. Lancet 1981, 1, 337–338. [Google Scholar] [CrossRef]
- Hingson, R.; Gould, J.B.; Morelock, S.; Kayne, H.; Heeren, T.; Alpert, J.J.; Zuckerman, B.; Day, N. Maternal cigarette smoking, psychoactive substance use, and infant Apgar scores. Am. J. Obstet. Gynecol. 1982, 144, 959–966. [Google Scholar] [CrossRef]
- Nijiati, K.; Satoh, K.; Otani, K.; Kimata, Y.; Ohtaki, M. Regression analysis of maternal smoking effect on birth weight. Hiroshima J. Med. Sci. 2008, 57, 61–67. [Google Scholar] [PubMed]
- Vardavas, C.I.; Chatzi, L.; Patelarou, E.; Plana, E.; Sarri, K.; Kafatos, A.; Koutis, A.D.; Kogevinas, M. Smoking and smoking cessation during early pregnancy and its effect on adverse pregnancy outcomes and fetal growth. Eur. J. Pediatr. 2010, 169, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Secker-Walker, R.H.; Vacek, P.M. Infant birth weight as a measure of harm reduction during smoking cessation trials in pregnancy. Health Educ. Behav. 2002, 29, 557–569. [Google Scholar] [CrossRef] [PubMed]
- England, L.J.; Kendrick, J.S.; Wilson, H.G.; Merritt, R.K.; Gargiullo, P.M.; Zahniser, S.C. Effects of smoking reduction during pregnancy on the birth weight of term infants. Am. J. Epidemiol. 2001, 154, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.L.; Cheadle, A.; Thompson, D.C.; Diehr, P.; Koepsell, T.; Kinne, S. The validity of self-reported smoking: A review and meta-analysis. Am. J. Public Health 1994, 84, 1086–1093. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Smoking Behavior of Pregnant Women | Low Birth Weight | Low Birth Length | Low Head Circumference | Low Ponderal Index | Low Apgar Score at 5 min | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | p | N | % | p | N | % | p | N | % | p | N | % | p | |
| Smoking status during pregnancy (N = 44,486) | <0.001 | <0.001 | <0.001 | 0.002 | 0.065 | ||||||||||
| Non-smoker | 290 | 0.9 | 142 | 0.4 | 673 | 2.0 | 3611 | 10.7 | 305 | 0.9 | |||||
| Quitter | 24 | 0.8 | 13 | 0.5 | 66 | 2.3 | 323 | 11.2 | 26 | 0.9 | |||||
| Smoker | 194 | 2.5 | 98 | 1.2 | 338 | 4.3 | 947 | 12.1 | 93 | 1.2 | |||||
| Number of smoked cigarettes per day during pregnancy (N = 40,702) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||
| 0 | 314 | 0.9 | 155 | 0.4 | 739 | 2.0 | 3933 | 10.7 | 331 | 0.9 | |||||
| 1–5 | 40 | 2.2 | 20 | 1.1 | 69 | 3.8 | 298 | 16.4 | 23 | 1.3 | |||||
| 6–10 | 38 | 2.2 | 26 | 1.5 | 84 | 5.0 | 186 | 11.0 | 29 | 1.7 | |||||
| ≥11 | 17 | 3.1 | 19 | 3.4 | 65 | 11.7 | 35 | 6.3 | 11 | 2.0 | |||||
| Smoking reduction during pregnancy relative to its pre-gestation level (N = 3968) | 0.176 | 0.208 | 0.208 | 0.156 | 0.572 | ||||||||||
| No | 61 | 2.5 | 43 | 1.8 | 140 | 5.7 | 295 | 12.1 | 41 | 1.7 | |||||
| Yes | 28 | 1.8 | 19 | 1.2 | 73 | 4.8 | 207 | 13.6 | 22 | 1.4 | |||||
| Adverse Birth Outcome | Crude OR (95% CI) | Adjusted OR (95% CI) 1 | ||||||
|---|---|---|---|---|---|---|---|---|
| Daily Numbers of Smoked Cigarettes during Pregnancy | Daily Numbers of Smoked Cigarettes during Pregnancy | |||||||
| 0 | 1–5 | 5–10 | ≥11 | 0 | 1–5 | 5–10 | ≥11 | |
| Low birth weight | 1.00 | 2.60 (1.87–3.63) | 2.66 (1.89–3.73) | 3.66 (2.23–6.0) | 1.00 | 2.02 (1.43–2.86) | 1.80 (1.25–2.58) | 2.06 (1.19–3.58) |
| Low birth length | 1.00 | 2.62 (1.64–4.18) | 3.67 (2.42–5.58) | 8.36 (5.15–13.6) | 1.00 | 2.25 (1.38–3.68) | 2.75 (1.76–4.30) | 5.36 (3.08–9.32) |
| Low head circumference | 1.00 | 1.92 (1.49–2.46) | 2.54 (2.01–3.20) | 6.46 (4.93–8.45) | 1.00 | 1.69 (1.31–2.19) | 2.08 (1.63–2.65) | 5.19 (3.89–6.92) |
| Low ponderal index | 1.00 | 1.63 (1.43–1.85) | 1.03 (0.88–1.20) | 0.56 (0.40–0.79) | 1.00 | 1.57 (1.38–1.80) | 0.99 (0.84–1.16) | 0.56 (0.40–0.80) |
| Low Apgar score at 5 min | 1.00 | 1.41 (0.92–2.15) | 1.91 (1.30–2.80) | 2.22 (1.21–4.08) | 1.00 | 1.35 (0.87–2.08) | 1.83 (1.23–2.73) | 2.06 (1.10–3.89) |
| Adverse Birth Outcome | Crude OR (95% CI) | Adjusted OR (95% CI) 1 | ||||
|---|---|---|---|---|---|---|
| Smoking Status during Pregnancy | Smoking Status during Pregnancy | |||||
| Non-Smoker | Quitter | Smoker | Non-Smoker | Quitter | Smoker | |
| Low birth weight | 1.00 | 0.97 (0.64–1.47) | 2.92 (2.44–3.52) | 1.00 | 0.89 (0.58–1.36) | 2.10 (1.72–2.57) |
| Low birth length | 1.00 | 1.07 (0.61–1.90) | 3.00 (2.31–3.88) | 1.00 | 1.09 (0.61–1.93) | 2.36 (1.78–3.14) |
| Low head circumference | 1.00 | 1.15 (0.89–1.49) | 2.21 (1.94–2.53) | 1.00 | 1.04 (0.80–1.34) | 1.77 (1.53–2.04) |
| Low ponderal index | 1.00 | 1.06 (0.94–1.19) | 1.15 (1.06–1.24) | 1.00 | 1.05 (0.93–1.19) | 1.15 (1.06–1.24) |
| Low Apgar score at 5 min | 1.00 | 1.00 (0.67–1.50) | 1.32 (1.04–1.66) | 1.00 | 0.94 (0.62–1.40) | 1.24 (0.97–1.59) |
| Adverse Birth Outcome | Crude OR (95% CI) | Adjusted OR (95% CI) 1 | ||
|---|---|---|---|---|
| Smoking Reduction during Pregnancy | Smoking Reduction during Pregnancy | |||
| No | Yes | No | Yes | |
| Low birth weight | 1.00 | 0.73 (0.47–1.15) | 1.00 | 0.87 (0.54–1.39) |
| Low birth length | 1.00 | 0.71 (0.41–1.22) | 1.00 | 0.83 (0.47–1.46) |
| Low head circumference | 1.00 | 0.83 (0.62–1.11) | 1.00 | 0.83 (0.62–1.12) |
| Low ponderal index | 1.00 | 0.86 (0.51–1.45) | 1.00 | 0.86 (0.50–1.46) |
| Low Apgar score at 5 min | 1.00 | 1.15 (0.95–1.40) | 1.00 | 1.10 (0.91–1.34) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kharkova, O.A.; Grjibovski, A.M.; Krettek, A.; Nieboer, E.; Odland, J.Ø. Effect of Smoking Behavior before and during Pregnancy on Selected Birth Outcomes among Singleton Full-Term Pregnancy: A Murmansk County Birth Registry Study. Int. J. Environ. Res. Public Health 2017, 14, 867. https://doi.org/10.3390/ijerph14080867
Kharkova OA, Grjibovski AM, Krettek A, Nieboer E, Odland JØ. Effect of Smoking Behavior before and during Pregnancy on Selected Birth Outcomes among Singleton Full-Term Pregnancy: A Murmansk County Birth Registry Study. International Journal of Environmental Research and Public Health. 2017; 14(8):867. https://doi.org/10.3390/ijerph14080867
Chicago/Turabian StyleKharkova, Olga A., Andrej M. Grjibovski, Alexandra Krettek, Evert Nieboer, and Jon Ø. Odland. 2017. "Effect of Smoking Behavior before and during Pregnancy on Selected Birth Outcomes among Singleton Full-Term Pregnancy: A Murmansk County Birth Registry Study" International Journal of Environmental Research and Public Health 14, no. 8: 867. https://doi.org/10.3390/ijerph14080867