Heat Exposure and Maternal Health in the Face of Climate Change


Abstract
1. Introduction
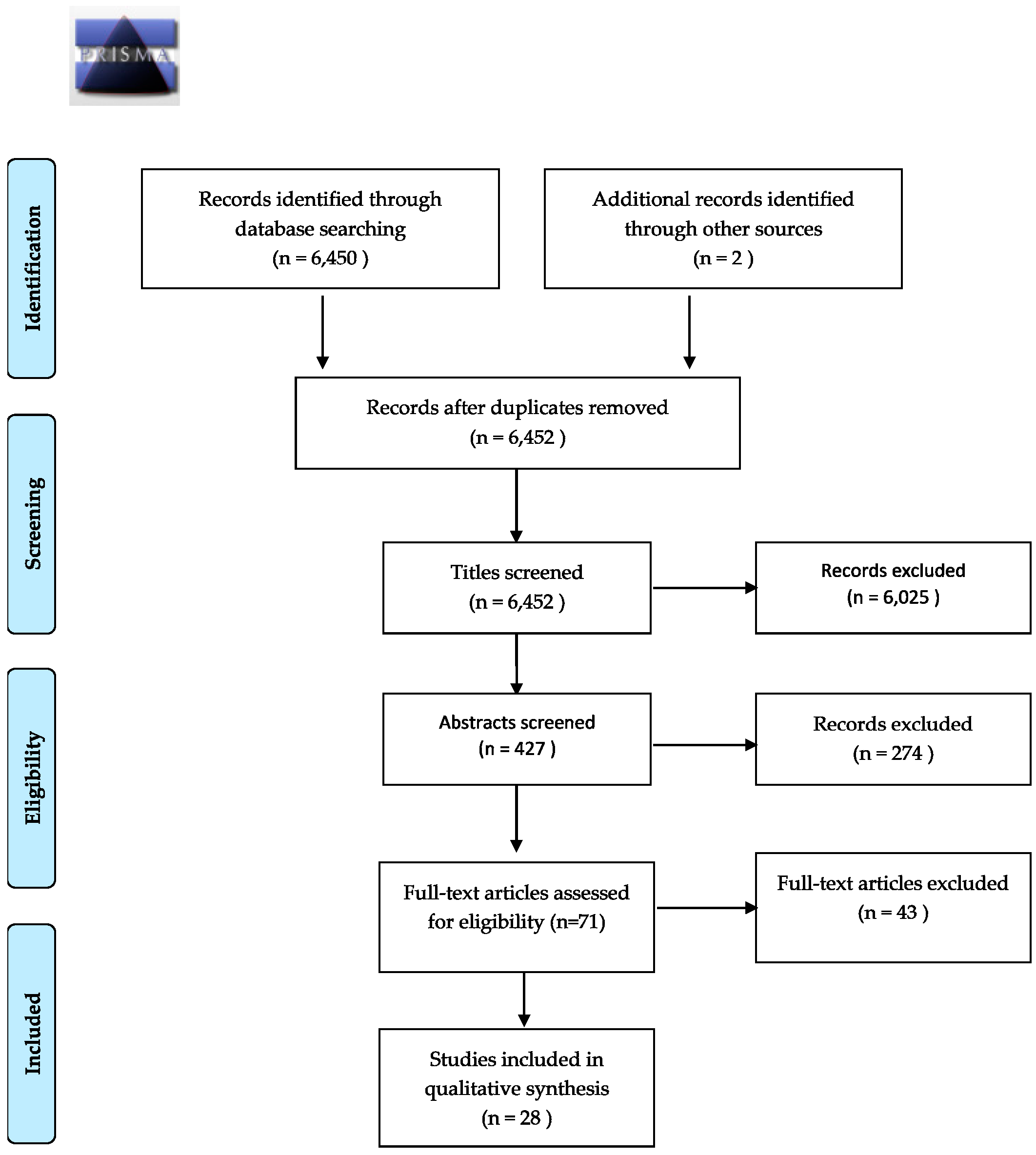
2. Materials and Methods
3. Results
3.1. Birth Outcomes
3.1.1. Measuring Exposure
3.1.2. Exposure/Outcome Relationship
3.2. Critical Exposure Window
3.3. Duration versus Threshold
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Garcia, C.V.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Crimmins, A.; Balbus, J.; Gamble, J.L.; Beard, C.B.; Bell, J.E.; Dodgen, D.; Eisen, R.J.; Fann, N.; Hawkins, M.; Herring, S.C.; et al. The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; U.S. Global Change Research Program: Washington, DC, USA, 2016.
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Costello, A.; Abbas, M.; Allen, A.; Ball, S.; Bell, S.; Bellamy, R.; Friel, S.; Groce, N.; Johnson, A.; Kett, M.; et al. Managing the health effects of climate change. Lancet 2009, 373, 1693–1733. [Google Scholar] [CrossRef]
- National Oceanic and Atmospheric Administration (NOAA). National Weather Service. Weather Fatality, Injury and Damage Statistics. Available online: http://www.nws.noaa.gov/om/hazstats.shtml (accessed on 10 May 2014).
- Bouchama, A.; Knochel, J.P. Heat stroke. N. Engl. J. Med. 2002, 346, 1978–1988. [Google Scholar] [CrossRef] [PubMed]
- Harlan, S.L.; Brazel, A.J.; Prashad, L.; Stefanov, W.L.; Larsen, L. Neighborhood microclimates and vulnerability to heat stress. Soc. Sci. Med. 2006, 63, 2847–2863. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Zanobetti, A.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Outdoor temperature is associated with serum HDL and LDL. Environ. Res. 2011, 111, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Zhou, W.; Cadenasso, M.L. Is everyone hot in the city? Spatial pattern of land surface temperatures, land cover and neighborhood socioeconomic characteristics in Baltimore, MD. J. Environ. Manag. 2011, 92, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Intergovernmental Panel on Climate Change; Fifth Assessment Report; Cambridge University Press: Cambridge, UK, 2014.
- World Health Organization. Health in 2015: From MDGS to SDGs; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes for child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- Wells, J.C. Thermal environment and human birth weight. J. Theor. Biol. 2002, 214, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Rylander, C.; Odland, J.Ø.; Sandanger, T.M. Climate change and environmental impacts on maternal and newborn health with focus on Arctic populations. Glob. Health. Action 2011, 4. [Google Scholar] [CrossRef] [PubMed]
- Poursafa, P.; Keikha, M.; Kelishadi, R. Systematic review on adverse birth outcomes of climate change. J. Res. Med. Sci. 2015, 20, 397–402. [Google Scholar] [PubMed]
- Carolan-Olah, M.; Frankowska, D. High environmental temperature and preterm birth: A review of the evidence. Midwifery 2013, 30, 50–59. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO: Recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet. Gynecol. Scand. 1977, 56, 247–253. [Google Scholar]
- Auger, N.; Naimi, A.I.; Smargiassi, A.; Lo, E.; Kosatsky, T. Extreme heat and risk of early delivery among preterm and term pregnancies. Epidemiology 2014, 25, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Strand, L.B.; Barnett, A.G.; Tong, S. Maternal exposure to ambient temperature and the risks of preterm birth and stillbirth in Brisbane, Australia. Am. J. Epidemiol. 2012, 175, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Williams, G.; Guo, Y.; Pan, X.; Tong, S. Maternal exposure to heatwave and preterm birth in Brisbane, Australia. BJOG 2013, 120, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Schifano, P.; Asta, F.; Dadvand, P.; Davoli, M.; Basagana, X.; Michelozzi, P. Heat and air pollution exposure as triggers of delivery: A survival analysis of population-based pregnancy cohorts in Rome and Barcelona. Environ. Int. 2016, 88, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Iniguez, C.; Barona, C.; Ballester, F. Exposure to elevated temperatures and risk of preterm birth in Valencia, Spain. Environ. Res. 2014, 134, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Malig, B.; Ostro, B. High ambient temperature and the risk of preterm delivery. Am. J. Epidemiol. 2010, 172, 1108–1117. [Google Scholar] [CrossRef] [PubMed]
- Kent, S.T.; McClure, L.A.; Zaitchik, B.F.; Smith, T.T.; Gohlke, J.M. Heat waves and health outcomes in Alabama (USA): The importance of heat wave definition. Environ. Health Perspect. 2014, 122, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Díaz, J.; Ortiz, C.; Carmona, R.; Sáez, M.; Linares, C. Short term effect of air pollution, noise and heat waves on preterm births in Madrid (Spain). Environ. Res. 2016, 145, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Schifano, P.; Lallo, A.; Asta, F.; De Sario, M.; Davoli, M.; Michelozzi, P. Effect of ambient temperature and air pollutants on the risk of preterm birth, Rome 2001–2010. Environ. Int. 2013, 61, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Olsson, D.; Forsberg, B. Exposure to seasonal temperatures during the last month of gestation and the risk of preterm birth in Stockholm. Int. J. Environ. Res. Public Health 2015, 12, 3962–3978. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.; Vicedo-Cabrera, A.M.; Gasparrini, A.; Roels, H.A.; Martens, E.; Vangronsveld, J.; Forsberg, B.; Nawrot, T.S. Ambient temperature as a trigger of preterm delivery in a temperate climate. J. Epidemiol. Community Health 2016, 70, 1–9. [Google Scholar] [CrossRef] [PubMed]
- He, J.-R.; Liu, Y.; Xia, X.-Y.; Ma, W.-J.; Lin, H.-L.; Kan, H.-D.; Liu, J.-H.; Feng, Q.; Mo, W.-J.; Wang, P.; et al. Ambient temperature and the risk of preterm birth in Guangzhou, China (2001–2011). Environ. Health Perspect. 2016, 124, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Lin, Y.; Ma, Y.; Zhang, L.; Zhang, X.; Li, L.; Zhang, S.; Cheng, Y.; Zhou, X.; Lin, H.; et al. The association between ambient temperature and preterm birth in Shenzhen, China: A distributed lag non-linear time series analysis. Environ. Health 2016, 15, 84. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, T.A.; Modin, B.; Vågerö, D. Cold ambient temperature in utero and birth outcomes in Uppsala, Sweden, 1915–1929. Ann. Epidemiol. 2014, 24, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Mathew, S.; Mathur, D.; Chang, A.B.; McDonald, E.; Singh, G.R.; Nur, D.; Gerristen, R. Examining the effects of ambient temperature on pre-term birth in Central Australia. Int. J. Environ. Res. Public Health 2017, 14, 147. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Armstrong, B. The association of season and temperature with adverse pregnancy outcome in two German states, a time-series analysis. PLoS ONE 2012, 7, e40228. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Melly, S.J.; Coull, B.A.; Nordio, F.; Schwartz, J.D. Using satellite-based spatiotemporal resolved air temperature exposure to study the association between ambient air temperature and birth outcomes in massachusetts. Environ. Health Perspect. 2015, 123, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Ngo, N.S.; Horton, R.M. Climate change and fetal health: The impacts of exposure to extreme temperatures in New York City. Environ. Res. 2016, 144, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Basagaña, X.; Sartini, C.; Figueras, F.; Vrijheid, M.; de Nazelle, A.; Sunyer, J.; Nieuwenhuijsen, M.J. Climate extremes and the length of gestation. Environ. Health Perspect. 2011, 119, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Ostro, B.; Figueras, F.; Foraster, M.; Basagaña, X.; Valentín, A.; Martinez, D.; Beelen, R.; Cirach, M.; Hoek, G. Residential proximity to major roads and term low birth weight: The roles of air pollution, heat, noise, and road-adjacent trees. Epidemiology 2014, 25, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Molina, O.; Saldarriaga, V. The perils of climate change: In utero exposure to temperature variability and birth outcomes in the Andean region. Econ. Hum. Biol. 2016, 24, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.; Arroyo, V.; Ortiz, C.; Carmona, R.; Linares, C. Effect of environmental factors on low weight in non-premature births: A time series analysis. PLoS ONE 2016, 11, e0164741. [Google Scholar] [CrossRef] [PubMed]
- Poeran, J.; Birnie, E.; Steegers, E.A.; Bonsel, G.J. The Impact of Extremes in Outdoor Temperature and Sunshine Exposure on Birth Weight. J. Environ. Health 2016, 78, 92–100. [Google Scholar] [PubMed]
- Jensen, P.M.; Sørensen, M. Differences in human birth weight and corollary attributes as a result of temperature regime. Ann. Hum. Biol. 2013, 40, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Cole, T.J. Birth weight and environmental heat load: A between-population analysis. Am. J. Phys. Anthropol. 2002, 119, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Fukuda, K.; Shimizu, T.; Nobunaga, M.; Mamsen, L.S.; Andersen, C.Y. Climate change is associated with male: Female ratios of fetal deaths and newborn infants in Japan. Fertil. Steril. 2014, 102, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Kakkad, K.; Barzaga, M.L.; Wallenstein, S.; Azhar, G.S.; Sheffield, P.E. Neonates in Ahmedabad, India, during the 2010 heat wave: A climate change adaptation study. J. Environ. Public Health 2014, 2014, 946875. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Pearson, D.; Sie, L.; Broadwin, R. A case-crossover study of temperature and infant mortality in California. Paediatr. Perinat. Epidemiol. 2015, 29, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Strand, L.B.; Barnett, A.G.; Tong, S. Methodological challenges when estimating the effects of season and seasonal exposures on birth outcomes. BMC Med. Res. Methodol. 2011, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; FitzGerald, G.; Guo, Y.; Jalaludin, B.; Tong, S. Impact of heatwave on mortality under different heatwave definitions: A systematic review and meta-analysis. Environ. Int. 2016, 89–90, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Wang, X.Y.; Barnett, A.G. Assessment of heat-related health impacts in Brisbane, Australia: Comparison of different heatwave definitions. PLoS ONE 2010, 5, e12155. [Google Scholar] [CrossRef] [PubMed]
- Montero, J.C.; Miron, I.J.; Criado, J.J.; Linares, C.; Díaz, J. Difficulties of defining the term, ”heat wave“, in public health. Int. J. Environ. Health Res 2013, 23, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Montero, J.C.; Mirón, I.J.; Criado, J.J.; Linares, C.; Díaz, J. Comparison between two methods of defining heat waves: a retrospective study in Castile-La Mancha (Spain). Sci. Total Environ. 2010, 408, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.S.; Carter, R.; Kish, J.K.; Gronlund, C.J.; White-Newsome, J.L.; Manarolla, X.; Zanobetti, X.; Zanobetti, A.; Schwartz, J.D. Preventing heat-related morbidity and mortality: New approaches in a changing climate. Maturitas 2009, 64, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.J.; Berry, P. Health co-benefits and risks of public health adaptation strategies to climate change: A review of current literature. Int. J. Public Health 2013, 58, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 282, 785–795. [Google Scholar] [CrossRef]
- Fleischer, N.L.; Merialdi, M.; van Donkelaar, A.; Vadillo-Ortega, F.; Martin, R.V.; Bertran, A.P.; Souza, J.P.; O’Neill, M.S. Outdoor air pollution, preterm birth, and low birth weight: Analysis of the world health organization global survey on maternal and perinatal health. Envion. Health Perspect. 2014, 122, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; Stayner, L.; Slama, R.; Sørensen, M.; Figueras, F.; Nieuwenhuijsen, M.J.; Raaschou-Nielsen, O.; Dadvand, P. Ambient air pollution and pregnancy-induced hypertensive disorders: A systematic review and meta-analysis. Hypertension 2014, 65, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; de Nazelle, A.; Triguero-Mas, M.; Schembari, A.; Cirach, M.; Amoly, E.; Figueras, F.; Basagaña, X.; Ostro, B.; Nieuwenhuijsen, M. Surrounding greenness and exposure to air pollution during pregnancy: An analysis of personal monitoring data. Envion. Health Perspect. 2012, 120, 1286–1290. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.R.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Strand, L.B.; Barnett, A.G.; Tong, S. The influence of season and ambient temperature on birth outcomes: A review of the epidemiological literature. Envion. Res. 2011, 111, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Balbus, J.M.; Malina, C. Identifying vulnerable subpopulations for climate change health effects in the United States. J. Occup. Envion. Med. 2009, 51, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Martiello, M.A.; Giacchi, M.V. High temperatures and health outcomes: A review of the literature. Scand. J. Public Health 2010, 38, 826–837. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Location | Sample Size | Early Birth | Preterm Birth | Low Birth Weight | Reduced Birth Weight | Stillbirth | Postnatal Outcomes | Exposure Window |
|---|---|---|---|---|---|---|---|---|---|
| Auger et al. 2014 [18] | Montreal, Canada | 206,929 | Yes | No | - | - | - | - | 1 week prior to delivery |
| Strand et al. 2012 [19] | Brisbane, Australia | 101,870 | Yes | Yes | - | - | Yes | - | 4 weeks prior to delivery |
| Wang et al. 2013 [20] | Brisbane, Australia | 50,848 | - | Yes | - | - | - | - | Up to 3 months prior to delivery |
| Schifano et al. 2016 [21] | Rome, Italy and Barcelona, Spain | 78,633 (Rome), 27,255 (Barcelona) | Yes | Yes | - | - | - | - | Full gestation |
| Vicedo-Cabrera et al. 2014 [22] | Valencia, Spain | 20,148 | - | Yes | - | - | - | - | 3 weeks prior to delivery |
| Basu et al. 2010 [23] | California, USA | 60,000 | - | Yes | - | - | - | - | 1 week prior to delivery |
| Kent et al. 2014 [24] | Alabama, USA | 60,466 | - | Yes | - | - | - | - | 1 week pior to delivery |
| Arroyo et al. 2016 [25] | Madrid, Spain | 298,705 | - | Yes | - | - | - | - | Full gestation |
| Schifano et al. 2013 [26] | Rome, Italy and Barcelona, Spain | 132,691 | - | Yes | - | - | - | - | Full gestation |
| Vicedo-Cabrera et al. 2015 [27] | Stockholm, Sweden | 95,069 | - | Yes | - | - | - | - | 4 weeks prior to delivery |
| Cox et al. 2016 [28] | Flanders, Belgium | 807,835 | Yes | Yes | - | - | - | - | Full gestation |
| He et al. 2016 [29] | Guangzhou, China | 838,146 | - | Yes | - | - | - | Full gestation | |
| Liang et al. 2016 [30] | Shenzhen, China | 1,040,638 | - | Yes | - | - | - | - | Full gestation |
| Bruckner et al. 2014 [31] | Uppsala, Sweden | 13,657 | - | Yes | - | No | No | - | Full gestation |
| Mathew et al. 2017 [32] | Alice Springs, Australia | 16,870 | - | Yes | - | - | - | - | 3 weeks prior to delivery |
| Wolf and Armstrong 2012 [33] | Brandenburg and Saxony, Germany | 291,517 | - | No | No | - | - | - | Full gestation |
| Kloog et al. 2015 [34] | Massachusetts, USA | 450,407 | - | Yes | Yes | Yes | - | - | Full gestation |
| Ngo and Horton 2016 [35] | New York, USA | 514,104 | No | - | - | Yes | - | - | Full gestation |
| Dadvand et al. 2011 [36] | Barcelona, Spain | 7585 | Yes | - | - | - | - | - | 1 week prior to delivery |
| Dadvand et al. 2014 [37] | Barcelona, Spain | 6438 | - | - | Yes | - | - | - | Full gestation |
| Molina and Saldarriaga 2017 [38] | Bolivia, Colombia, and Peru | 86,000 | - | - | Yes | Yes | - | - | Full gestation |
| Díaz et al. 2016 [39] | Madrid, Spain | 298,705 | - | - | No | - | - | - | Full gestation |
| Poeran et al. 2016 [40] | Netherlands | 1,460,401 | - | - | - | Yes | - | - | Full gestation |
| Jensen and Sørensen 2013 [41] | Global Data: 125 populations | Not Reported | - | - | - | Yes | - | Full gestation | |
| Wells and Cole 2002 [42] | Global Data: 140 populations | Average: 97,237 | - | - | - | Yes | - | - | Full gestation |
| Fukuda et al. 2014 [43] | Japan | Not Reported | - | - | - | - | Yes | - | Full gestation |
| Kakkad et al. 2014 [44] | Ahmedabad, India | 2025 | - | - | - | - | - | Yes | After delivery |
| Basu et al. 2015 [45] | California, USA | 12,356 | - | - | - | - | - | Yes | After delivery |
| Heat Wave Definitions Tested in Reviewed Articles | ||
| Kakkad et al. 2014 [44] | 1. When normal temperature is <40 °C: | Heat wave if 5–6 °C increase |
| Severe heat wave if 7 °C+ increase | ||
| 2. When normal temperature is ≥40 °C: | Heat wave if 4–5 °C increase | |
| Severe heat wave if 6 °C+ increase | ||
| 3. If temperatures exceed 45 °C: | Severe heat wave | |
| Wang et al. 2013 [20] | 1. Exceed 90th temperature percentile (30.38 °C) over a 2, 3, or 4 day minimum duration | |
| 2. Exceed 95th temperature percentile (31.32 °C) over a 2, 3, or 4 day minimum duration | ||
| 3. Exceed 99th temperature percentile (32.52 °C) over a 2, 3, or 4 day minimum duration | ||
| Mathew et al. 2017 [32] | Temperature >40 °C for 3 consecutive days | |
| Extreme Heat Definitions Measured in Reviewed Articles: | ||
| Auger et al. 2014 [18] | 1. ≥32 °C for 3 consecutive days | |
| 2. ≥32 °C for 1, 2, 3, and 4 to 7 days | ||
| Dadvand et al. 2011 [36] | Heat-humidity index >90th, >95th, or >99th percentile for 1 day | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuehn, L.; McCormick, S. Heat Exposure and Maternal Health in the Face of Climate Change. Int. J. Environ. Res. Public Health 2017, 14, 853. https://doi.org/10.3390/ijerph14080853
Kuehn L, McCormick S. Heat Exposure and Maternal Health in the Face of Climate Change. International Journal of Environmental Research and Public Health. 2017; 14(8):853. https://doi.org/10.3390/ijerph14080853
Chicago/Turabian StyleKuehn, Leeann, and Sabrina McCormick. 2017. "Heat Exposure and Maternal Health in the Face of Climate Change" International Journal of Environmental Research and Public Health 14, no. 8: 853. https://doi.org/10.3390/ijerph14080853
APA StyleKuehn, L., & McCormick, S. (2017). Heat Exposure and Maternal Health in the Face of Climate Change. International Journal of Environmental Research and Public Health, 14(8), 853. https://doi.org/10.3390/ijerph14080853