Health-Promoting Nature Access for People with Mobility Impairments: A Systematic Review

 ,
,
Abstract
:1. Introduction
- What types of nature interventions and activities for people with mobility impairments are found in research studies?
- What characterizes (diagnosis; mobility impairment; gender and age) the different groups of people participating in the studies.
- What health outcomes are addressed in the studies?
- What is the quality of the studies, based on qualitative, quantitative, and mixed method designs?
- What accessibility issues are perceived by the target group during nature interventions?
2. Methods
2.1. Literature Search Strategies
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
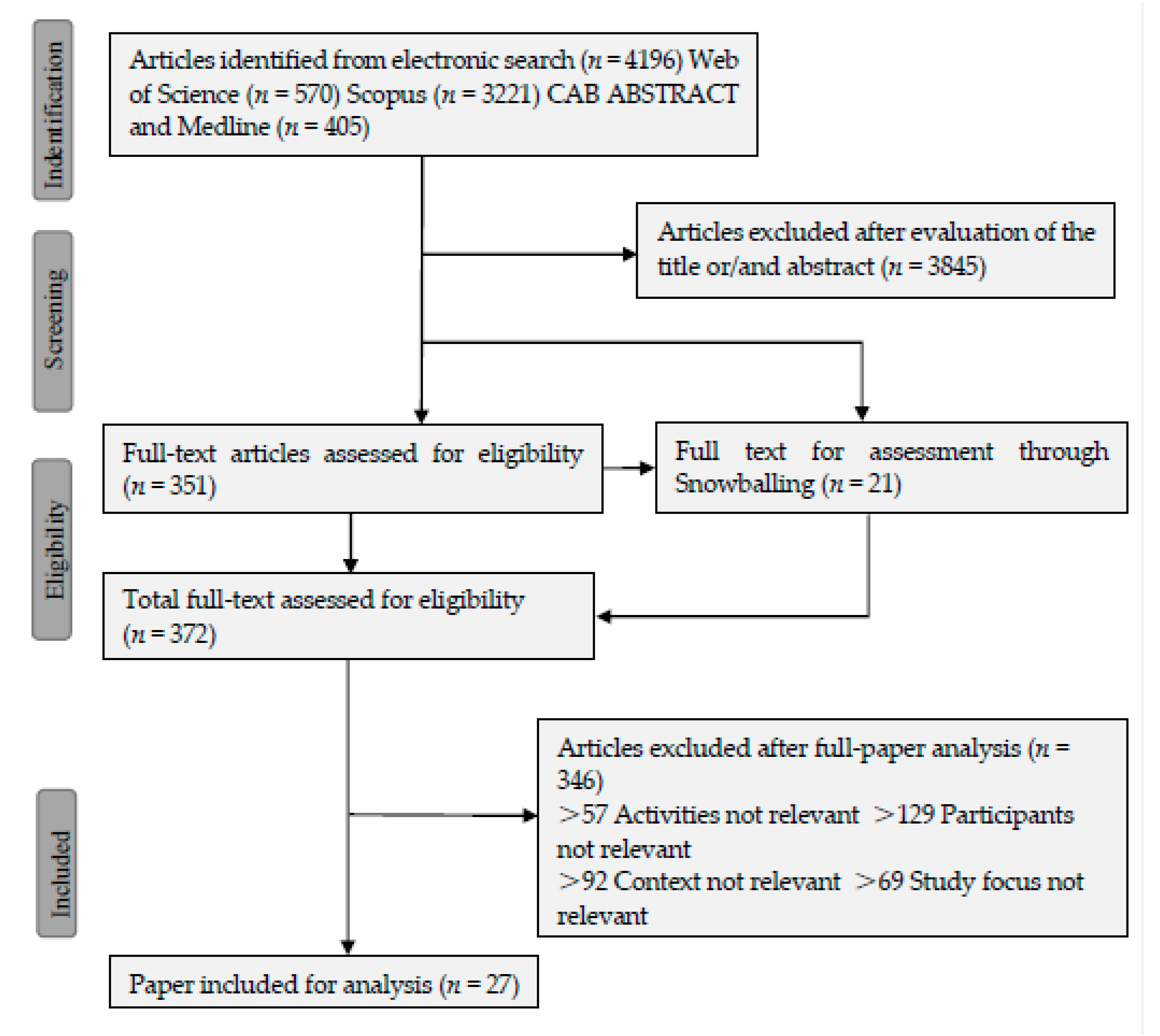
3.1. Study Identificaiton and Selection
3.2. Study Characteristics
3.3. Nature-Related Activities
3.4. Health Impacts from Nature and Nature-Related Activities
3.4.1. Physical Health Benefits
3.4.2. Mental Health Benefits
3.4.3. Social Health Impacts
3.5. Mechanism of the Health Impacts
3.6. Preferences
3.7. Barriers for Nature and Nature-Related Activities
4. Discussion
4.1. Health-Promoting Nature Seen from the Perspective of People with Mobility Impairments
4.2. Implications for Future Practices and Suggestions for Future Research
4.3. Limitations for This Review Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nilsson, K.; Sangster, M.; Gallis, C.; Hartig, T.; De Vries, S.; Seeland, K.; Schipperijn, J. Forests, Trees and Human Health; Springer Science & Business Media: Berlin, Germany, 2010. [Google Scholar]
- Stigsdotter, U.K. Nature, health and design. Alam Cipta 2015, 8, 89–96. [Google Scholar]
- Jiang, B.; Chang, C.-Y.; Sullivan, W.C. A dose of nature: Tree cover, stress reduction, and gender differences. Landscape Urban Plan. 2014, 132, 26–36. [Google Scholar] [CrossRef]
- Sullivan, W. In search of a clear head. In Fostering Reasonableness: Supportive Environments for Bringing out Our Best; University of Michigan Press: Ann Arbor, MI, USA, 2015; pp. 54–69. [Google Scholar]
- Holtan, M.T.; Dieterlen, S.L.; Sullivan, W.C. Social life under cover: Tree canopy and social capital in Baltimore, Maryland. Environ. Behav. 2015, 47, 502–525. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef] [PubMed]
- Hug, S.-M.; Hartig, T.; Hansmann, R.; Seeland, K.; Hornung, R. Restorative qualities of indoor and outdoor exercise settings as predictors of exercise frequency. Health Place 2009, 15, 971–980. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Convention on the Rights of Persons with Disabilities. Available online: https://treaties.un.org/pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-15&chapter=4&clang=_en (accessed on 22 June 2017).
- WHO. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. Disability and Health. Available online: http://www.who.int/mediacentre/factsheets/fs352/en/ (accessed on 6 September 2016).
- Damgaard, M.; Steffensen, T.; Bengtsson, S. Hverdagsliv og Levevilkår for Mennesker med Funktionsnedsættelse: En Analyse af Sammenhængen Mellem Hverdagsliv, Samliv, Udsathed, og Type og Grad af Funktionsnedsættelsean Analysis of the Relationship Between Everyday Life, Living Together, Vulnerability and Type and Degree of Disability; SFI-Det Nationale Forskningscenter for Velfærd: Copenhagen, Denmark, 2013. [Google Scholar]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, chronic diseases, and decrements in health: Results from the world health surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]
- Stigsdotter, U.C.; Ekholm, O. A nationwide Danish survey on the use of green space among individuals with mobility disabilities. Scand. J. Public Health 2017, in press. [Google Scholar]
- Pluye, P.; Gagnon, M.-P.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Botticello, A.L.; Rohrbach, T.; Cobbold, N. Differences in the community built environment influence poor perceived health among persons with spinal cord injury. Arch. Phys. Med. Rehabil. 2015, 96, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Hitzig, S.L.; Alton, C.; Leong, N.; Gatt, K. The evolution and evaluation of a therapeutic recreation cottage program for persons with spinal cord injury. Ther. Recreat. J. 2012, 46, 218. [Google Scholar]
- Taylor, L.P.S.; McGruder, J.E. The meaning of sea kayaking for persons with spinal cord injuries. Am. J. Occup. Ther. 1996, 50, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Ebersbach, G.; Ebersbach, A.; Gandor, F.; Wegner, B.; Wissel, J.; Kupsch, A. Impact of physical exercise on reaction time in patients with Parkinson’s disease—Data from the berlin big study. Arch. Phys. Med. Rehabil. 2014, 95, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Van Eijkeren, F.J.; Reijmers, R.S.; Kleinveld, M.J.; Minten, A.; Bruggen, J.P.; Bloem, B.R. Nordic walking improves mobility in Parkinson’s disease. Mov. Disord. 2008, 23, 2239–2243. [Google Scholar] [CrossRef] [PubMed]
- Ottosson, J.; Lavesson, L.; Pinzke, S.; Grahn, P. The significance of experiences of nature for people with parkinson’s disease, with special focus on freezing of gait—The necessity for a biophilic environment. A multi-method single subject study. Int. J. Environ. Res. Public Health 2015, 12, 7274–7299. [Google Scholar] [CrossRef] [PubMed]
- Reuter, I.; Mehnert, S.; Leone, P.; Kaps, M.; Oechsner, M.; Engelhardt, M. Effects of a flexibility and relaxation programme, walking, and nordic walking on Parkinson’s disease. J. Aging Res. 2011, 2011, 232473. [Google Scholar] [CrossRef] [PubMed]
- Sunvisson, H.; Lökk, J.; Ericson, K.; Winblad, B.; Ekman, S.-L. Changes in motor performance in persons with Parkinson’s disease after exercise in a mountain area. J. Neurosci. Nurs. 1997, 29, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Sunvisson, H.; Ekman, S.L. Environmental influences on the experiences of people with Parkinson’s disease. Nurs. Inq. 2001, 8, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, A.; Carlsson, G. Outdoor environments at three nursing homes: Focus group interviews with staff. J. Hous. Elder. 2006, 19, 49–69. [Google Scholar] [CrossRef]
- Brascamp, W.; Kidd, J. Contribution of Plants to the Well-Being of Retirement Home Residents. In XXVI International Horticultural Congress: Expanding Roles for Horticulture in Improving Human Well-Being and Life Quality 639, Toronto, ON, Canada, 11–17 August 2004; ISHS: Dabhaich, India, 2002; pp. 145–150. [Google Scholar]
- Finlay, J.; Franke, T.; McKay, H.; Sims-Gould, J. Therapeutic landscapes and wellbeing in later life: Impacts of blue and green spaces for older adults. Health Place 2015, 34, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Gallacher, J.; Palmer, S.; Fone, D. Neighbourhood green space, physical function and participation in physical activities among elderly men: The caerphilly prospective study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Rappe, E.; Kivelä, S.-L.; Rita, H. Visiting outdoor green environments positively impacts self-rated health among older people in long-term care. HortTechnology 2006, 16, 55–59. [Google Scholar]
- Rappe, E.; Kivelä, S.-L. Effects of garden visits on long-term care residents as related to depression. HortTechnology 2005, 15, 298–303. [Google Scholar]
- Rodiek, S. Influence of an outdoor garden on mood and stress in older persons. J. Ther Hortic. 2002, 13, 13–21. [Google Scholar]
- Rodiek, S.D.; Fried, J.T. Access to the outdoors: Using photographic comparison to assess preferences of assisted living residents. Landsc. Urban Plan. 2005, 73, 184–199. [Google Scholar] [CrossRef]
- Pasek, P.B.; Schkade, J.K. Effects of a skiing experience on adolescents with limb deficiencies: An occupational adaptation perspective. Am. J. Occup. Ther. 1996, 50, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Terese, L. With nature and the outdoors as a resource: A case of a one-footed elderly man in a wheelchair. Phys. Cult. Sport. Stud. Res. 2015, 65, 24–30. [Google Scholar] [CrossRef]
- Dawson, S.; Liddicoat, K. “Camp gives me hope”: Exploring the therapeutic use of community for adults with cerebral palsy. Ther. Recreat. J. 2009, 43, 9. [Google Scholar]
- Anderson, L.; Schleien, S.J.; McAvoy, L.; Lais, G.; Seligmann, D. Creating positive change through an integrated outdoor adventure program. Ther. Recreat. J. 1997, 31, 214–229. [Google Scholar]
- Brown, T.J.; Kaplan, R.; Quaderer, G. Beyond accessibility: Preference for natural areas. Ther. Recreat. J. 1999, 33, 209. [Google Scholar]
- Freudenberg, P.; Arlinghaus, R. Benefits and constraints of outdoor recreation for people with physical disabilities: Inferences from recreational fishing. Leis. Sci. 2009, 32, 55–71. [Google Scholar] [CrossRef]
- Kearney, A.R.; Winterbottom, D. Nearby nature and long-term care facility residents: Benefits and design recommendations. J. Hous. Elder. 2006, 19, 7–28. [Google Scholar] [CrossRef]
- McAvoy, L.; Holman, T.; Goldenberg, M.; Klenosky, D. Wilderness and persons with disabilities. Int. J. Wilderness 2006, 12, 23–31. [Google Scholar]
- De la Motte, P. Therapeutic Garden Designs in Special Needs Facilities in Victoria, Australia. In XXIX International Horticultural Congress on Horticulture: Sustaining Lives, Livelihoods and Landscapes (IHC2014): XII 1121, Brisbane, Australia, 17 August 2014; ISHS: Dabhaich, India, 2016; pp. 47–50. [Google Scholar]
- Meneghello, F.; Marcassa, G.; Koch, I.; Sgaravatti, P.; Piccolomini, B.; Righetto, C.; Prosdocimi Gianquinto, G.; Orsini, F. Garden therapy in neurorehabilitation: Well-being and skills improvement. In XXIX International Horticultural Congress on Horticulture: Sustaining Lives, Livelihoods and Landscapes (IHC2014): XII 1121, Brisbane, Australia, 17 August 2014; ISHS: Dabhaich, India, 2016; pp. 13–18. [Google Scholar]
- Kelley, M. The therapeutic potential of outdoor adventure: A review, with a focus on adults with mental illness. Ther. Recreat. J. 1993, 27, 110–125. [Google Scholar]
- Maller, C.; Townsend, M.; Pryor, A.; Brown, P.; St Leger, L. Healthy nature healthy people: Contact with nature as an upstream health promotion intervention for populations. Health Promot. Int. 2006, 21, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Schkade, J.K.; Schultz, S. Occupational adaptation: Toward a holistic approach for contemporary practice, part 1. Am. J. Occup. Ther. 1992, 46, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Stoneham, J.; Jones, R. Residential landscapes: Their contribution to the quality of older people’s lives. Act. Adapt. Aging 1997, 22, 17–26. [Google Scholar] [CrossRef]
- Crawford, D.W.; Jackson, E.L.; Godbey, G. A hierarchical model of leisure constraints. Leis. Sci. 1991, 13, 309–320. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category (CAT) | Target Group | Nature | Nature-Related Activities | Health Impacts | Accessibility Issues |
|---|---|---|---|---|---|
| All search words are combined with “OR” within each category |
|
|
|
|
|
| Variables | Number of Included Studies of Certain Mobility Impairments | ||||||
|---|---|---|---|---|---|---|---|
| Type | SCI | PD | MS | Elderly | Limb Deficiency | Cerebral Palsy | Others/Not Specified |
| N1 + N2 | 3 + 1 | 6 + 1 | 0 + 2 | 8 + 2 | 2 + 2 | 1 + 1 | 7 + 1 |
| Author (Year) [Reference] | Country | Research Design | Sample | Mobility Impairments | Nature/Greenspaces | Contact Type | Health Impacts | Other Points | Quality |
|---|---|---|---|---|---|---|---|---|---|
| Botticello (2015) [15] | U.S. | QUAN/Cross-sectional analytic study | 503 | SCI | Community green spaces | - | More mixed land use and small amounts of green spaces—Poor perceived health | Inaccessible and highly developed environment may exacerbate the deleterious effects of stress | ** |
| Hitzig (2012) [16] | CA | QUAN/Non-RCT | 21 (14 EXP; 7 CON) | SCI | Multi-kinds (Land and water) | OET | Self-esteem, affect and self-efficacy ↑ | Participants are satisfied with the programme and willing to participate more | *** |
| Taylor (1996) [17] | U.S. | QUAL/Qualitative description | 3 | SCI | Sea | Active involvement/Kayaking | Relaxation, stress defusion, self-esteem, self-confidence; social interaction; Physical strength, stamina, balance ↑ | Nature atmosphere is appreciated; perceived safety; need awareness and support from surroundings | ** |
| Ebersbach (2014) [18] | DE | QUAN/RCT | 58 | PD | Local parks | Rehabilitative intervention/supervised NW | Immediate and follow-up cognitive aspects of movement preparation ↑ | - | ** |
| Frank (2008) [19] | NL | QUAN/Self-controlled Case series | 19 | PD | City Park | Active interaction/NW | Walking speed, Timed up and go test (TUG) test, timed walking distance and QOL↑ | More active life style in long-term future | *** |
| Ottosson (2015) [20] | SE | MM/Triangulation Design | 5 | PD | Natural environment as compared to built-environment; Site-Alnarp rehabilitation garden | - | Nature induces less freezing of gait than built environment; Better physical performance in nature | The visual environment should try to convey signal of “no danger“ to reduce the FOG. | ** (QUAL **; QUAN **) |
| Reuter (2011) [21] | DE | QUAN/RCT | 90 | PD | Park and forest | Active involvement/Nordic walking and walking | HRQoL, cognitive function, postural instability, mobility, cardio-respiratory capacity ↑ | NW is more preferred than walking and indoor training. More active future life for NW participants. | **** |
| Sunvisson (1997) [22] | SE | QUAN/Self-controlled Case series | 12 | PD | Mountain | OET (1 week walking a year in 3 consecutive years) | Immediate overall motor performance and coordination capacity simultaneous integration ↑ Additional improvement in follow-up | More active outdoor life after participation; a combination of training and social interaction with counterpart contributed to the benefits. | *** |
| Sunvisson (2000) [23] | SE | QUAL/Phenomenology | 11 | PD | Mountain | OET (1 week walking a year for 2 consecutive years) | Feeling of capability, social interaction, self-confidence, self-esteem and positive life attitude ↑ | Social relationships and challenges in the wildness trip make them feel less trapped by daily negative experiences | *** |
| Bengtsson (2013) [24] | SE | QUAL/Phenomenology | 12 patients + 7 next of kin | Elderly residents in nursing homes with limited mobility | Surrounding nature of nursing homes | Passive contact mainly | Sensual pleasure, connection to the past; social involvement ↑ | Fresh air, light and greenery + Different senses like the sound of water and birds and the natural fragrance are appreciated; Accessibility, safety, familiarity and the rights of choice are important. | **** |
| Brascamp (2004) [25] | NZ | MM/Embedded design | 61 | Elderly typically with physical limitations | Green environment near retirement homes | Passive involvement and active interaction (Gardening) | Relaxation, perceived wellbeing and satisfaction ↑ | Passive involvement is perceived to contribute more to wellbeing. Staff encouragement contributes to outdoor enjoyment. | * (QUAL *; QUAN **) |
| Finlay (2015) [26] | U.S. | QUAL/Qualitative description | 141 | Elderly with limited mobility | Blue and green spaces | Passive contact: Nature exposure; Active interaction: walking, gardening and hiking, etc. | Physically active lifestyle, physical strength; spiritual peace and connectedness, rejuvenation; social interaction, social integration, etc. ↑ | Natural sights, sounds and smells are valued; waterscapes are highly preferred; Rest spots and shelters could enhance usage. Distance, Slippery and uneven surfaces (walkability) induce fears. | **** |
| Gong (2014) [27] | U.K. | QUAN/Cross-sectional analytical study | 1010 | Elderly with different level of lower extremity | 400 m radius outdoor environment around home | - | More green space—higher physical activities | Homogeneous vegetation has positive relationship with physical activities | *** |
| Rappe (2006) [28] | FIN | QUAN/Cross-sectional analytic study | 45 | Elderly women with different level of mobility | Outdoor green environments of long-term care | Passive involvement/visit or watching | Pain reduction, tranquility; self-related health ↑ | Restriction of visit: Lack of assistance, bad weather, steep or uneven paths, poor health, door and doorstep; Trees, fragrant flowers and birds are appreciated | *** |
| Rappe (2005) [29] | FIN | QUAN/Cross-sectional analytic study | 26 | Elderly with different level of mobility | Gardens of long-term care | Garden visiting | Mood, feeling of recovery, sleep quality, feeling of balance, concentration, pain relief ↑ | Hindrances: Lack of assistance > bad weather circumstances > steep and uneven paths; Natural elements such as plants, smells, fresh air, activities and animals are main motivations | ** |
| Rodiek (2002) [30] | U.S. | QUAN/RCT | 16 | Elderly with different level of mobility | Outdoor horticulture garden | Passive involvement/Observing | Mood and anxiety level (improved but not significant); Stress level ↓ | - | ** |
| Rodiek (2005) [31] | U.S. | QUAN/Case series | 133 | Assisted living elderly with different level of mobility | Nature surrounding the assisted living facilities | - | - | Places to walk, trees, resting spaces and different views are preferred | ** |
| Pasek (1995) [32] | U.S. | QUAL/Phenomenology | 14 | Limb deficiencies | National sport centre for the disabled in Winter Park, Colorado | Active interaction/Skiing | Activity performance; self-satisfaction, self-esteem, satisfaction with others ↑ | Mastery of skills and social interaction may result in better self-esteem | *** |
| Ramsland (2015) [33] | IT | QUAL/Case-study | 1 | Elderly amputee | Nature around his home in Ålesund | Mainly passive contact | Perceived mental and physical health, mood, positive attitude; social health ↑ stress ↓ | Accessible paths make it possible to go out; Natural elements like the sunshine, air, scents, bird sounds are appreciated. | ** |
| Dawson (2009) [34] | U.S. | QUAL/Phenomenology | 27 | Cerebral palsy | Outdoor centre with universal accessibility | Summer camping including different kinds of nature-related activities | Social involvement and interaction; self-esteem, self-confidence ↑ | The interpersonal relationships and atmosphere are believed to contribute to the benefits | ** |
| Anderson (1997) [35] | U.S. | MM/Triangulation design | 12 with disability + 14 without disability | Different kinds of disabilities | Wilderness | Active interaction/Integrated outdoor adventure program including canoeing as a main part | Social integration, interpersonal relations; relaxation, personal growth, positive attitude toward disabilities, positive lifestyle; Skill development ↑ | Integrated participation with people without disabilities are helpful in different aspects | ** (QUAL *** QUAN **) |
| Brown (1999) [36] | U.S. | QUAN/Descriptive study | 197 (116 with mobility limitation + 81 companions) | People with mobility limitations without classified diagnosis | Scenes of Parks | - | - | Forests are preferred to open fields especially the ones with paths; Feathers that could make them feel confident and comfortable are also important. | *** |
| Freudenberg (2009) [37] | DE | QUAN/Cross-sectional analytic study | 775 (345 with physical disabilities and 428 without) | Varied kinds of physical disabilities and not specifically stated | Fishing sites in wilderness | Active interaction/Recreational fishing | Social interaction benefits, benefits for self-improvement, nature and relaxation-related benefits and challenge-related benefits ↑; Social benefits and benefits for personal growth more significant than people without disabilities | People with disabilities fish more frequently than people without disabilities; Catch-related constraints > access constraints > interpersonal > intrapersonal | *** |
| Kearney (2006) [38] | U.S. | QUAL/Qualitative description | 40 | Residents with limited mobility in long-term care | Nearby nature of long-term care facility | Passive and active | Perceived mental and physical health; invigoration; social interaction; life attitude, etc. ↑ | Passive contact is more popular among the participants; Plants selection is most popular for the place preference. Quietness, accessibility, resting places and materials are also important. Staff assistance and easy access are helpful for barriers. | ** |
| McAVoy (2006) [39] | U.S. | QUAL/Phenomenology | 193 (74 with disabilities and 119 without) | Different kinds of disabilities | Wilderness | Active interaction/Wilderness trips mostly water related | Relaxation, (Self-)awareness, personal growth/challenge, self-confidence; Personal relationship; positive life attitude ↑ | A balance between accessible use and enjoyment of wilderness should be achieved; Information about the level of access is useful | **** |
| Motte (2016) [40] | AUS | QUAL/Case study | - | Special need groups, mainly elderly and people with disabilities | Therapeutic gardens in special needs facilities | - | - | Safe and accessible paths; Avoid space confusion; meditation areas; strong seating; shelters for bad weather; active gardening beds | * |
| Meneghello (2014) [41] | IT | QUAN/Quantitative descriptive studies | 28 | Multi-kinds (SCI, PD, MS, etc.) | Neurorehabilitation Garden | Active involvement/GT | Self-esteem, relaxation, social involvement ↑ | Value being outdoor; GT less fatigue than physiotherapy | ** |
| Items | CAT | Physical Health | Mental Health | Social Health | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CAT | Variables | Strength | Stamina | Pain relief | Balance | Reaction | PHY Independence | Perceived PHY H | Skill Performance | Cardio-respiratory | Awareness | Renewal | Perceived PSY H | Mood | Cognition | Relaxation | Stress Reduction | Self-Satisfaction | Self-esteem | Self-confidence | Life attitude | Relationship | Interaction | Involvement | Willingness | Support |
| Passive | Watch | * | * | |||||||||||||||||||||||
| Stay in | * | * | * | * | * | * | ||||||||||||||||||||
| Active | WT | * | * | * | * | * | ||||||||||||||||||||
| Gardening | * | * | * | * | * | |||||||||||||||||||||
| Skiing | * | * | * | * | * | * | * | |||||||||||||||||||
| Canoeing | * | * | * | * | * | |||||||||||||||||||||
| Walking | * | * | * | * | * | * | ||||||||||||||||||||
| NW | * | * | * | * | * | * | ||||||||||||||||||||
| Fishing | * | * | * | * | * | |||||||||||||||||||||
| Kayaking | * | * | * | * | * | * | * | * | * | |||||||||||||||||
| Rehabilitative | OET | * | * | * | * | * | * | |||||||||||||||||||
| RT | * | * | * | |||||||||||||||||||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, G.; Poulsen, D.V.; Lygum, V.L.; Corazon, S.S.; Gramkow, M.C.; Stigsdotter, U.K. Health-Promoting Nature Access for People with Mobility Impairments: A Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 703. https://doi.org/10.3390/ijerph14070703
Zhang G, Poulsen DV, Lygum VL, Corazon SS, Gramkow MC, Stigsdotter UK. Health-Promoting Nature Access for People with Mobility Impairments: A Systematic Review. International Journal of Environmental Research and Public Health. 2017; 14(7):703. https://doi.org/10.3390/ijerph14070703
Chicago/Turabian StyleZhang, Gaochao, Dorthe V. Poulsen, Victoria L. Lygum, Sus S. Corazon, Marie C. Gramkow, and Ulrika K. Stigsdotter. 2017. "Health-Promoting Nature Access for People with Mobility Impairments: A Systematic Review" International Journal of Environmental Research and Public Health 14, no. 7: 703. https://doi.org/10.3390/ijerph14070703