Methods for Involving Older People in Health Research—A Review of the Literature

Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
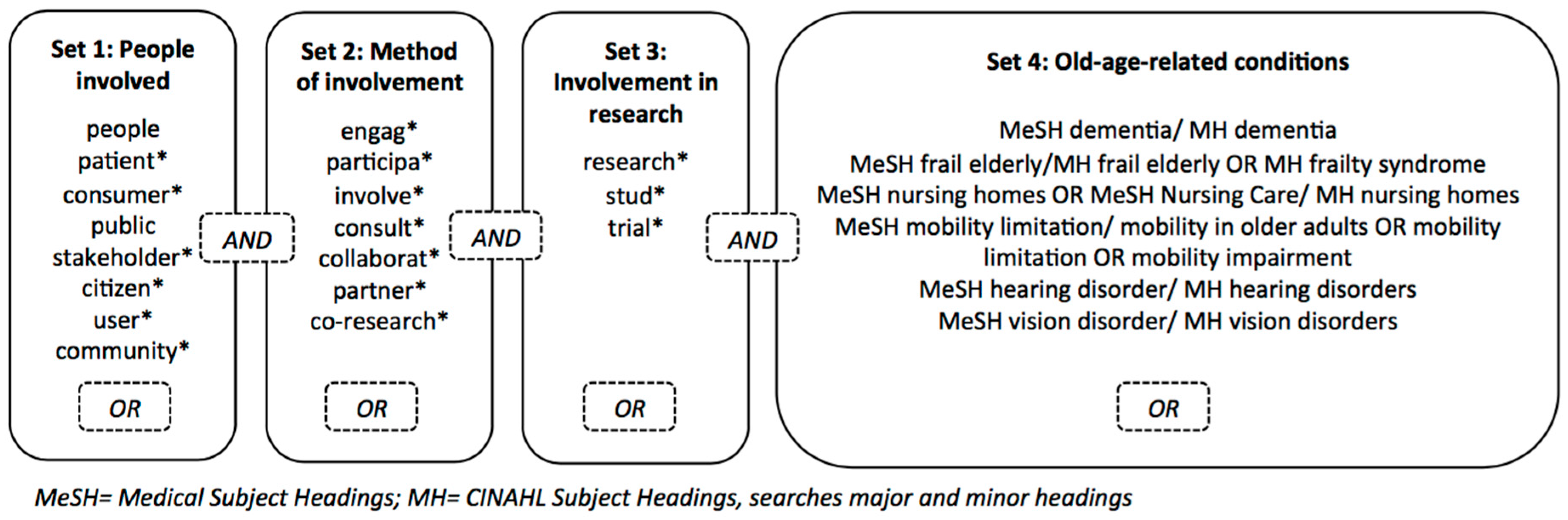
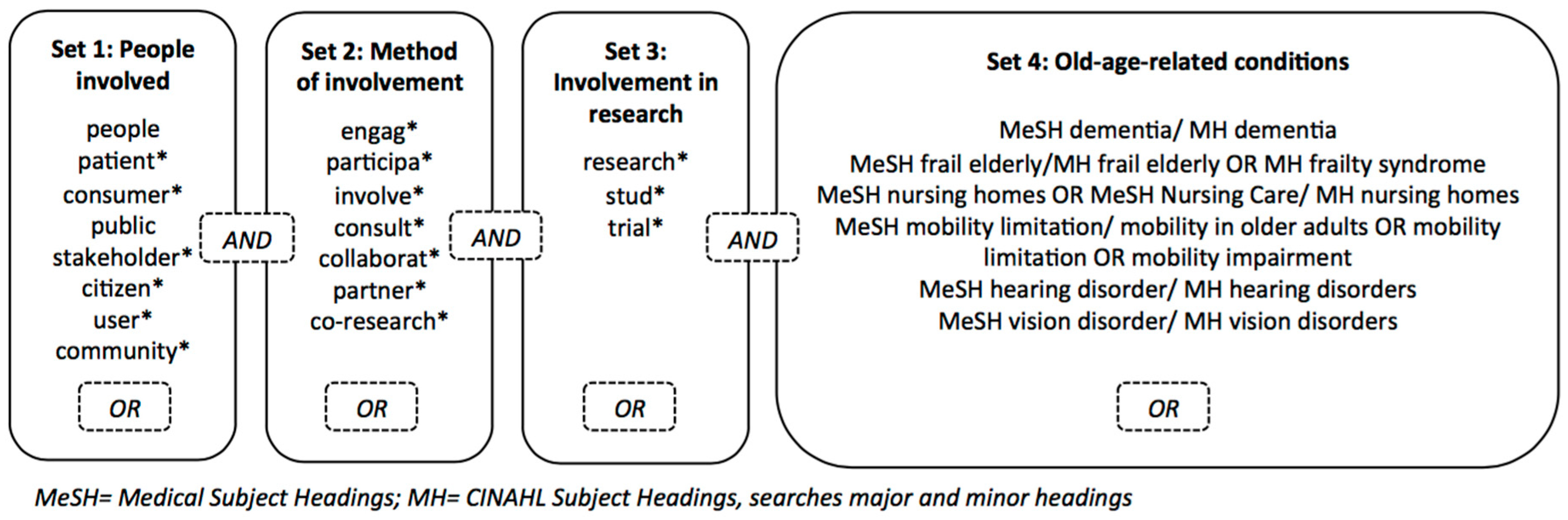
2.2. Search Strategy
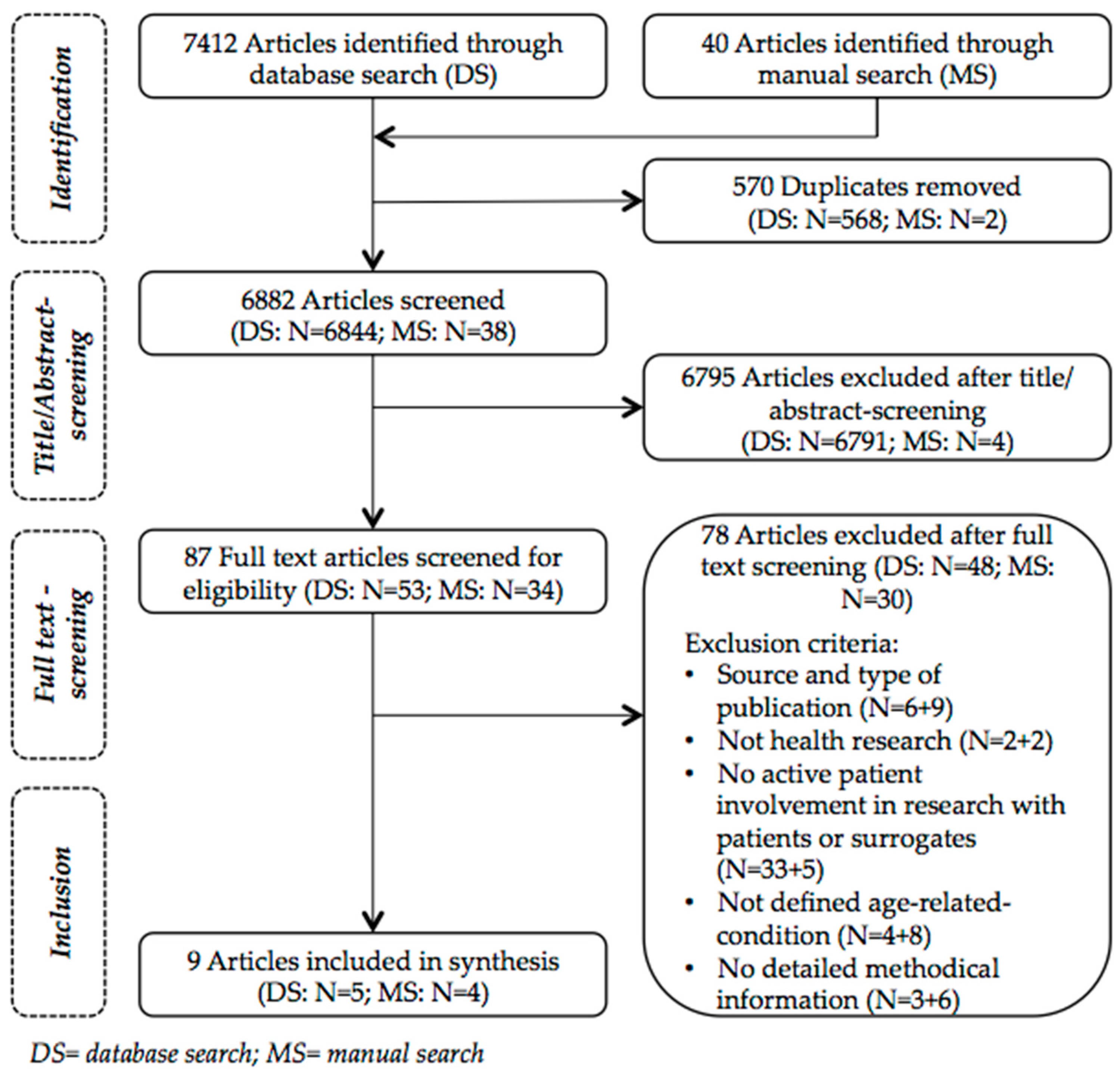
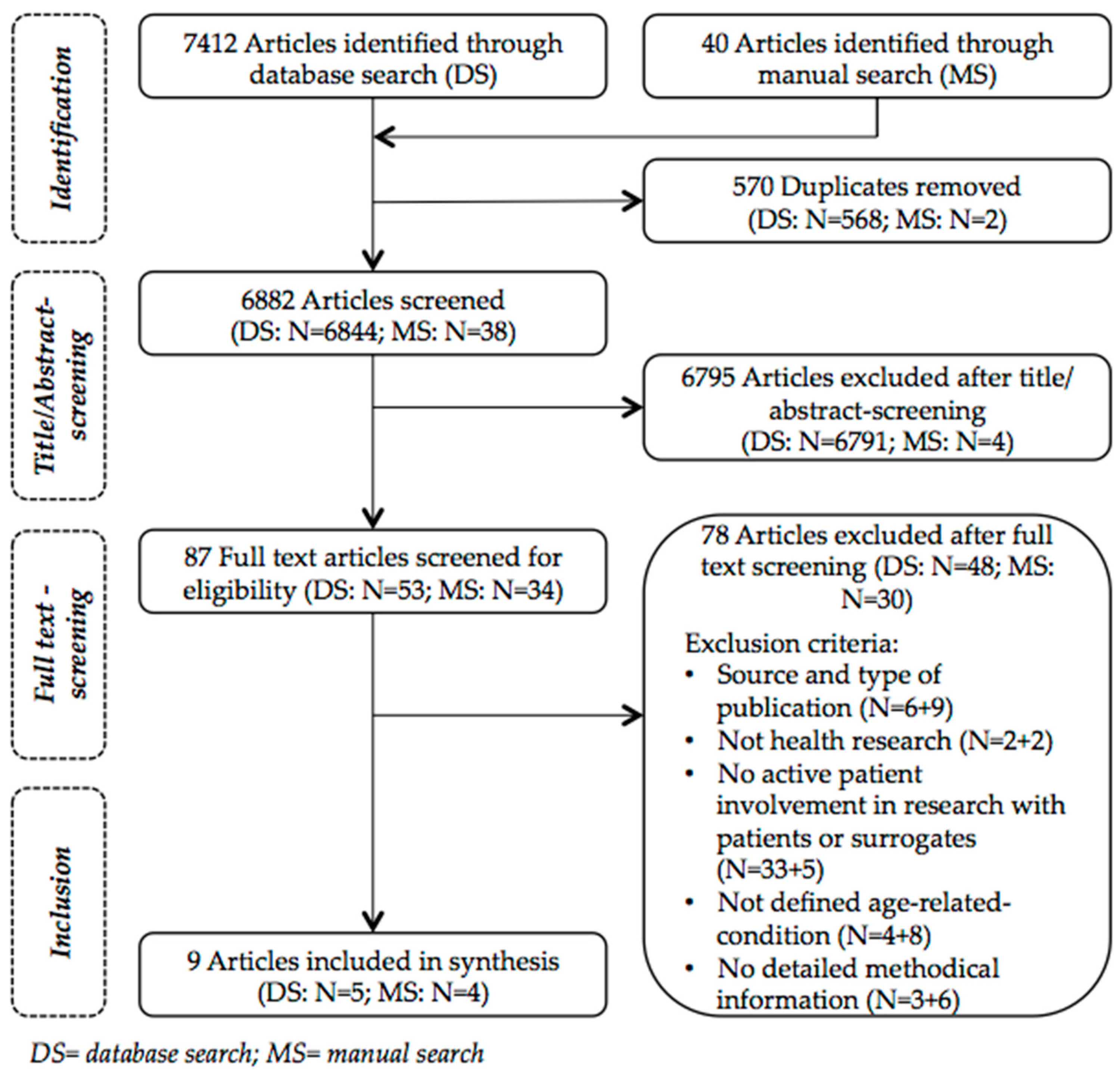
2.3. Article Selection
2.4. Data Extraction and Synthesis
3. Results
3.1. Implementation of PPI
3.1.1. Aim of Involvement
3.1.2. Methods and Stages of Involvement
3.1.3. Participants
3.1.4. Recruitment
3.1.5. Level of Participation and Roles
3.1.6. Setting of Involvement
3.1.7. Ethical Approval
3.2. Practical Challenges and Facilitators for Involvement
3.2.1. Diversity
3.2.2. Communication
3.2.3. Location
3.2.4. Relationship
3.2.5. Timing
3.2.6. Continuity
3.2.7. Support for Participants
4. Discussion
4.1. Issues on PPI that Are Not Related to Specific Methods
4.1.1. Recruitment, Diversity and Equity
4.1.2. Ethics
4.2. Challenges and Facilitators within the Used PPI Methods
4.2.1. Continuity and Flexibility in Long-Term Involvement
4.2.2. Communication, Setting and Relationships in Face-To-Face Methods
4.2.3. Individual Tasks as Alternative to Face-to-Face Methods
4.3. Limitations of This Review
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Domecq, J.; Prutsky, G.; Elraiyah, T.; Wang, Z.; Nabhan, M.; Shippee, N.; Brito, J.; Boehmer, K.; Hasan, R.; Firwana, B.; et al. Patient engagement in research: A systematic review. BMC Health Serv. Res. 2014, 14, 89. [Google Scholar] [CrossRef] [PubMed]
- Esmail, L.; Moore, E.; Rein, A. Evaluating patient and stakeholder engagement in research: Moving from theory to practice. J. Comp. Eff. Res. 2015, 4, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Boote, J.; Baird, W.; Beecroft, C. Public involvement at the design stage of primary health research: A narrative review of case examples. Health Policy 2010, 95, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A. Patient and public involvement: In theory and in practice. J. Laryngol. Otol. 2014, 128, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. A systematic review of the impact of patient and public involvement on service users, researchers and communities. Patient 2012, 7, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, I.; Glasziou, P. Avoidable waste in the production and reporting of research evidence. Lancet 2009, 374, 86–89. [Google Scholar] [CrossRef]
- Canadian Institutes of Health Research (CIHR). Patient Engagement Framework, Strategy for Patient-Oriented Research; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2014. [Google Scholar]
- Sandman, L.; Bond, K.; Hofmann, B. Exploring ethical rationales. In Patient Involvement in Health Technology Assessment; Facey, K., Ploug Hansen, H., Single, A., Eds.; Springer Nature: Singapore, 2017; Volume 1, pp. 17–29. [Google Scholar]
- INVOLVE. Briefing Notes for Researchers: Involving the Public in nhs, Public Health and Social Care Research; INVOLVE: Eastleigh, UK, 2012. [Google Scholar]
- Patient-Centered Outcomes Research Institute (PCORI). What We Mean by Engagement. Available online: https://www.pcori.org/engagement/what-we-mean-engagement (accessed on 10 November 2017).
- Boote, J.; Telford, R.; Cooper, C. Consumer involvement in health research: A review and research agenda. Health Policy 2002, 61, 213–236. [Google Scholar] [CrossRef]
- Brett, J.; Stanizewska, S.; Mockford, C.; Seers, K.; Herron-Marx, S.; Bayliss, H. The PIRICOM Study: A Systematic Review of the Conceptualisation, Measurement, Impact and Outcomes of Patient and Public Involvement in Health and Social Care Research; University of Warwick: Warwick, UK, 2010. [Google Scholar]
- Oliver, S.R.; Rees, R.W.; Clarke-Jones, L.; Milne, R.; Oakley, A.R.; Gabbay, J.; Stein, K.; Buchanan, P.; Gyte, G. A multidimensional conceptual framework for analysing public involvement in health services research. Health Expect. 2008, 11, 72–84. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Research (NIHR). Going the Extra Mile: Improving the Nation’s Health and Wellbeing through Public Involvement in Research; National Institute for Health Research: London, UK, 2015. [Google Scholar]
- Boyle, D.; Slay, J.; Stephens, L. Public Services Inside Out. Putting Co-Production into Practice; NESTA: London, UK, 2010. [Google Scholar]
- Bagley, H.J.; Short, H.; Harman, N.L.; Hickey, H.R.; Gamble, C.L.; Woolfall, K.; Young, B.; Williamson, P.R. A patient and public involvement (PPI) toolkit for meaningful and flexible involvement in clinical trials—A work in progress. Res. Involv. Engagem. 2016, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- INVOLVE. Diversity and Inclusion: What’s It about and Why Is It Important for Public Involvement in Research? INVOLVE: Eastleigh, UK, 2012. [Google Scholar]
- Rivett, E. Research involving people with dementia: A literature review. Work. Older People 2017, 21, 107–114. [Google Scholar] [CrossRef]
- Shura, R.; Siders, R.A.; Dannefer, D. Culture change in long-term care: Participatory action research and the role of the resident. Gerontologist 2011, 51, 212–225. [Google Scholar] [CrossRef] [PubMed]
- Holroyd-Leduc, J.; Resin, J.; Ashley, L.; Barwich, D.; Elliott, J.; Huras, P.; Légaré, F.; Mahoney, M.; Maybee, A.; McNeil, H.; et al. Giving voice to older adults living with frailty and their family caregivers: Engagement of older adults living with frailty in research, health care decision making, and in health policy. Res. Involv. Engagem. 2016, 2, 23. [Google Scholar] [CrossRef] [PubMed]
- Iliffe, S.; McGrath, T.; Mitchell, D. The impact of patient and public involvement in the work of the dementias & neurodegenerative diseases research network (DeNDRoN): Case studies. Health Expect. 2013, 16, 351–361. [Google Scholar] [PubMed]
- Bundesarbeitsgemeinschaft der Klinisch-Geriatrischen Einrichtungen e. V.; Deutsche Gesellschaft für Geriatrie e. V.; Deutsche Gesellschaft für Gerontologie und Geriatrie e. V. Abgrenzungskriterien der Geriatrie. 2004. Available online: http://www.geriatrie-drg.de/public/docs/Abgrenzungskriterien_Geriatrie_V13_16-03-04.pdf (accessed on 10 November 2017).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, R.; Hick, C.; Houston, A.; Gardiner, L.; Wallace, D. Privileging place: Reflections on involving people with dementia in a residency. Dementia (Lond. Engl.) 2015, 14, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Burnell, K.J.; Selwood, A.; Sullivan, T.; Charlesworth, G.M.; Poland, F.; Orrell, M. Involving service users in the development of the support at home: Interventions to enhance life in dementia carer supporter programme for family carers of people with dementia. Health Expect. 2015, 18, 95–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giebel, C.; Roe, B.; Hodgson, A.; Britt, D.; Clarkson, P. Effective public involvement in the HoST-D programme for dementia home care support: From proposal and design to methods of data collection (innovative practice). Dementia 2017. [Google Scholar] [CrossRef] [PubMed]
- Hassan, L.; Swarbrick, C.; Sanders, C.; Parker, A.; Machin, M.; Tully, M.P.; Ainsworth, J. Tea, talk and technology: Patient and public involvement to improve connected health ‘wearables’ research in dementia. Res. Involv. Engagem. 2017, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Heaven, A.; Brown, L.; Foster, M.; Clegg, A. Keeping it credible in cohort multiple randomised controlled trials: The community ageing research 75+ (CARE 75+) study model of patient and public involvement and engagement. Res. Involv. Engagem. 2016, 2, 30. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Lafortune, L.; Hart, N.; Cowan, K.; Fenton, M.; Brayne, C. Dementia priority setting partnership with the James Lind Alliance: using patient and public involvement and the evidence base to inform the research agenda. Age Ageing 2015, 44, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Taylor, B.J. Involving individuals with dementia as co-researchers in analysis of findings from a qualitative study. Dementia 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tanner, D. Co-research with older people with dementia: Experience and reflections. J. Ment. Health 2012, 21, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Fudge, N.; Wolfe, C.D.A.; McKevitt, C. Involving older people in health research. Age Ageing 2007, 36, 492–500. [Google Scholar] [CrossRef] [PubMed]
- National Research Ethics Service (NRES); INVOLVE. Patient and Public Involvement in Research and Research Ethics Committee Review; INVOLVE and NRES: Eastleigh and London, UK, 2009. [Google Scholar]
- Dewing, J. Participatory research: A method for process consent with persons who have dementia. Dementia 2007, 6, 11–25. [Google Scholar] [CrossRef]
- Ives, J.; Damery, S.; Redwod, S. PPI, paradoxes and Plato: Who’s sailing the ship? J. Med. Ethics 2012, 39, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Staley, K. There is no paradox with PPI in research. J. Med. Ethics 2013, 39, 186–187. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| No. | Category | Criteria |
|---|---|---|
| 1 | Date of publication | 1 January 2007–21 July 2017 (up to 8 August 2017 for manual search) |
| 2 | Language | English, German, French, Spanish |
| 3 | Source and type of article | Peer-reviewed journals, empirical articles |
| 4 | Field of research | Health research |
| 5 | Active patient involvement in research | Patients or their surrogates are actively involved in the research process as reported by the authors of the article |
| 6 | Old people | Patients have at least one of the defined old-age-related conditions |
| 7 | Methods of involvement | Methods of involvement in research are described detailed enough to answer at least one of our research questions |
| References | Topic of Article | Aim, Stage and Method of PPI (as Described by Authors) |
|---|---|---|
| Bartlett et al. [24] | Issue of place when involving people with dementia in research | Aim: Engage participants of primary study in dissemination of research findings Stage: Dissemination Method: Co-production in shared domicile |
| Burnell et al. [25] | Involvement of service users in development of intervention study for carers of people with dementia | Aim: Ensure understandability and appropriateness of information sheets for study participants Stage: Development of study information Method: Anonymous postal reader consultation (Additional PPI done with family carers to inform intervention for carers) |
| Giebel et al. [26] | Impact of involvement of people with dementia and informal carers in a study program on home care support | Aim: Opinions of users shall be considered in research process Stages: Proposal; design; data collection (state of PPI at the time of publication) Method: Local reference group (Additional PPI done with informal carers in virtual group) |
| Hassan et al. [27] | Improve research with health devices in dementia through PPI | Aim: Enhance acceptability and feasibility of future research on health devices in dementia Stages: Development of research platform and guide; identification of research questions Method: Workshop (Further PPI done with different groups, e.g., researchers, people with mild cognitive impairment, dementia <65 years, no known memory problems) |
| Heaven et al. [28] | Methods for PPI in a cohort multiple RCT on frailty in primary care | Aim: Include diverse perspectives in original study and whole program, connect program to target population Stages: Proposal; design; data collection; analysis; dissemination Methods: (a) Core reference group; (b) Ad hoc groups and individuals |
| Iliffe et al. [21] | Impact of centrally organized PPI body in three case studies in clinical research (thereof two studies with regard to dementia) Article reports on two studies | Aims: (a) Explore low recruitment rates in on-going study on dementia treatment option; (b) Widening discussion about appropriate ways of introducing topic of dementia with people with Parkinson’s disease Stages: Recruitment; Development of study information Methods: Centrally organized PPI body offers PPI support to individual studies. Resulting in: (a) PPI focus groups; (b) Individually written feedback |
| Kelly et al. [29] | Identification and prioritization of unanswered research questions relating to dementia | Aim: Improve use of resources by integrating stakeholders in priority setting Stage: Identification and prioritization of research questions Methods: (a) Survey; (b) Prioritization within organizations; (c) Prioritization workshop |
| Stevenson et al. [30] | Involving co-researchers with dementia in analyzing research findings on risk communication in care | Aim: Enhance validity in analysis through applying multiple perspectives Stage: Analysis Method: Co-research (Further PPI done but not elaborated) |
| Tanner [31] | Involving co-researchers with dementia in investigating experiences with transitions between services | Aim: Facilitate deeper exchange, good interview experience, richer data Stages: Preparation; data collection; analysis Method: Co-research |
| References | Implementation of PPI | Practical Challenges and Facilitators |
|---|---|---|
| Bartlett et al. [24] | Co-production in shared domicile Aim(s)/Tasks: Plan dissemination Participants: 7 people with dementia Recruitment: All 16 participants from primary study were invited to participate Setting: Large domicile rented for involvement with both space to be alone and to work together Roles: People with dementia as collaborators in research Structure: Two three days meetings, each in shared domicile, one at beginning and one at end of the dissemination project
| Challenges:
|
| Burnell et al. [25] | Anonymous postal reader consultation Aim(s)/Tasks: Give feedback on understandability and appropriateness of documents via feedback forms Participants: 11 people with dementia and 6 family carers returned feedback (12 in each group were asked to participate) Recruitment: Via two disease- and carer-specific networks Setting: Individual task not bound to location Roles: Service users as anonymous advisors Structure: One-time postal consensus method, anonymous
| Challenges:
|
| Giebel et al. [26] | Local reference group Aim(s)/Tasks: Advice on different aspects of study program Participants: 11–15 participants: people with dementia (who have experience with lay involvement), informal carers, members of research team Recruitment: Via group meetings of disease-specific support organization Setting: Meetings take place at one location, reimbursement of travel expenses Roles: People with dementia and carers as advisors and collaborators, shared control with research team members Structure: Biannually face-to-face meetings, cyclic process of involvement
| Challenges:
|
| Hassan et al. [27] | Workshop Aim (s)/Tasks: Discuss (and test) health devices, share experiences, make recommendations for research Participants: 5 people with dementia and 4 carers (age: all but one > 65 years), researchers experienced with PPI and in working with people with dementia Recruitment: Via local dementia resource center and network Setting: Local dementia resource center Roles: People with dementia and carers as advisers Structure: Workshop with two sessions over 1–2 weeks, one week of voluntary device testing in-between:
| Challenges:
Workshop design:
|
| Heaven et al. [28] | Core reference group Aim(s)/Tasks: Monitoring and consultation for original study; overview of whole program; linkage between original and sub-studies; connection to local networks Participants: Organizational representatives from target population (e.g., people over 75 years with frailty), members of research team Recruitment: Via local or research groups Setting: Local meetings (no further information given) Roles: Members of reference group engaged in consultation, collaboration and co-production as appropriate Structure: Quarterly meetings plus interim activity (e.g., facilitation of events, networking)
Aim(s)/Tasks: Flexible consultation activity on request, maintain diversity Participants: Groups and individuals from target population (e.g., people over 75 years with frailty) Recruitment: Via networks of core group Setting: Not available (n.a.) Roles: Participants as one-off advisors Structure: Groups and individuals flexibly engaged when needed | Challenges:
|
| Iliffe et al. [21] | Article reports on two studies with different PPI methods: (a) Focus groups Aim(s)/Tasks: Diagnose aspects interfering with recruitment Participants: 27 patients with mild dementia, carers, 2 people without dementia experience Recruitment: Via 2 local specialized research networks Setting: Local (no further information given) Roles: Patients and carers as discussants Structure: One-time involvement, 2 separate focus groups (no further information given) (b) Individual written feedback Aim(s)/Tasks: Review patient and carer information sheet for study Participants: 15 external PPI panel members responded to request (consisting of people with experience with dementia as patient or carer, patients with Parkinson’s disease) Recruitment: Via local specialized research networks Setting: Individual, not bound to location Roles: Panel members as individual reviewers Structure: External PPI one-time individual request to external panel members
| Challenges: (a) n.a. (b) Authors state that group discussions would be more favorable for task, individual feedback chosen because of:
|
| Kelly et al. [29] | Survey Aim(s)/Tasks: Identify unanswered research questions Participants: 1563 individual stakeholders (4% people with dementia, 76% relatives, 15% professionals, others) Recruitment: Via various ways e.g., websites and material of (partner) organisations, social media, local offices; special efforts to recruit underrepresented groups (e.g., people with dementia) (no further information given) Setting: Not bound to location Roles: Stakeholders as individual respondents Structure: One-off survey
Aim(s)/Tasks: Rank questions for prioritization Participants: 61 organizations representing patients, carers, professionals Recruitment: Via networks Setting: Within organizations Roles: Representing perspective of organization Structure: One-off task
| Challenges: n.a. Facilitators: n.a. |
| Kelly et al. [29] | Prioritization workshop Aim(s)/Tasks: Reach consensus in prioritization Participants: 18 organizational representatives (among them 2 people with dementia, 5 relatives); Recruitment: Via networks Setting: Capital city Roles: n.a. Structure: One-time workshop
| Challenges: n.a. Facilitators: n.a. |
| Stevenson et al. [30] | Co-research Aim(s)/Tasks: Identify themes in analysis Participants: 4 people with dementia (age: 2 participants < 65 years, 2 participants 70–79 years), researchers Recruitment: Existing service user research panel from Alzheimer’s Society asked to participate and agreed Setting: Regular venue of Alzheimer’s Society Service User Review Panel Roles: People with dementia as co-researchers, referred to as members of research team in analysis session Structure: Two hours analysis session
| Challenges:
|
| Tanner [31] | Co-research Aim(s)/Tasks: Preparation of interviews, development of framework, conduction of interviews, first analysis of content and process Participants: Researcher plus 3 people with mild to moderate dementia (age: 60–78 years; gender: 2 males, 1 female; all living at home with their partners) Recruitment: Local dementia service partner published information via various ways (e.g., newsletter, memory café) Setting: Own home and group room for preparation, space of interviews not stated Roles: People with dementia as co-researchers, collaboration Structure: conduction of interviews plus three preparation sessions and two post-interview sessions
| Challenges: Individual challenges in people with dementia
|
|
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schilling, I.; Gerhardus, A. Methods for Involving Older People in Health Research—A Review of the Literature. Int. J. Environ. Res. Public Health 2017, 14, 1476. https://doi.org/10.3390/ijerph14121476
Schilling I, Gerhardus A. Methods for Involving Older People in Health Research—A Review of the Literature. International Journal of Environmental Research and Public Health. 2017; 14(12):1476. https://doi.org/10.3390/ijerph14121476
Chicago/Turabian StyleSchilling, Imke, and Ansgar Gerhardus. 2017. "Methods for Involving Older People in Health Research—A Review of the Literature" International Journal of Environmental Research and Public Health 14, no. 12: 1476. https://doi.org/10.3390/ijerph14121476