1. Introduction
Air pollution in both outdoor and indoor environments is a longstanding worldwide issue. Among air pollutants, the most commonly monitored are particulate matter (PM), nitrogen dioxide (NO
2), sulfur dioxide (SO
2), and ozone (O
3). According to the annual report of the World Health Organization (WHO) titled State of Global Air 2017, over 90% of the world’s population live in areas with unhealthy air, which is a leading risk factor for diseases and death [
1]. The WHO has established that premature death by air pollution occurs as the direct results of cardiovascular diseases, respiratory diseases, and lung cancer at rates of 80%, 14%, and 6%, respectively [
2].
One of the most common components of air pollution is PM, which is classified as PM
10, fine PM, and ultrafine particles according to the particles’ aerodynamic diameter [
3]. PM
10 (particles of less than 10 μm diameter) is composed of particles from dust, industrial emissions, and traffic emissions; such inhalation of PM
10 is directly related to various respiratory diseases [
4,
5,
6]. A smaller PM diameter with less than 2.5 μm is defined as fine PM (PM
2.5); PM
2.5 is primarily comprised of organic carbon compounds, nitrates, and sulfates [
4]. Recently, ambient PM
2.5 has become increasingly present in the surrounding air and significantly involved in human health, particularly in regard to respiratory tract diseases, as it can reach the bronchial tubes and deep regions of the lung [
7]. Reference cohort studies in which participants are monitored for decades have discovered that smaller particles such as PM
2.5 have more adverse effects on human health than larger particles [
4,
8,
9,
10]. Additionally, epidemiological investigations into contamination, especially ambient air pollution, indicated that the PM is not only correlative with the exacerbation of cardiovascular diseases and respiratory systemic inflammation impacts but also the progression of inflammatory skin diseases [
11] such as atopic dermatitis (AD) [
12,
13,
14], acne, psoriasis, and allergic reactions [
9,
15,
16,
17].
Nowadays, more evidence is available on the effects of PM of various sizes (PM
10 and PM
2.5) on skin diseases (e.g., AD and eczema in children, cellulitis and skin aging in adult) [
10,
16,
17,
18]. The present study entailed a systematic review and meta-analysis by summarizing the statistically significant effects of PM on human skin and its association with multiple skin diseases and their symptoms.
2. Materials and Methods
2.1. Literature Search and Data Extraction
The literature search on the adverse skin effects of PM10 and PM2.5 air pollution on the adverse skin effects of PM10 and PM2.5 air pollution was performed in the English-language databases PubMed (National Library of Medicine, Bethesda, MD, USA), Elsevier (Information and Analytics, Amsterdam, The Netherlands), and Web of Science (Institute of Scientific Information and Clarivate Analytics, United States) and considered articles published between 1990 and 2017. Combinations of the following keywords were used: PM, PM10, PM2.5, human skin diseases, AD, skin aging, and eczema disease. Reference lists of identified papers were also searched.
Bibliographic reference lists were manually selected for meta-analysis based on identifying associations between PM10, PM2.5, and human skin diseases, articles that presented no data (e.g., review articles and editorials) as well as articles written in languages other than English were excluded. The inclusion criteria for quantitative meta-analysis were estimates of diseases reporting data that could be used to calculate an estimate of the effect.
From each of the selected studies, the title, author, location, publication year, study design, number of events, and specific risk estimates were extracted and entered into a Microsoft Excel database.
2.2. Meta-Analysis
The effect estimates from the selected studies were summarized using the inverse variance method, by which the overall effect estimate was the average of the individual study effect estimates that was weighted by the inverse of the study variance [
19]. In our meta-analysis, first, each study’s heterogeneity was examined using the standard coefficient heterogeneity (I
2) test. The existence of heterogeneity was considered at the 95% level of significance and I
2; according to that result, either fixed-effects or random-effects models were used to assess the pooled estimates.
All analyses were performed using Meta-Disc software (version 1.4, Unit of Clinical Biostatistics, Marid, Spain).
3. Results
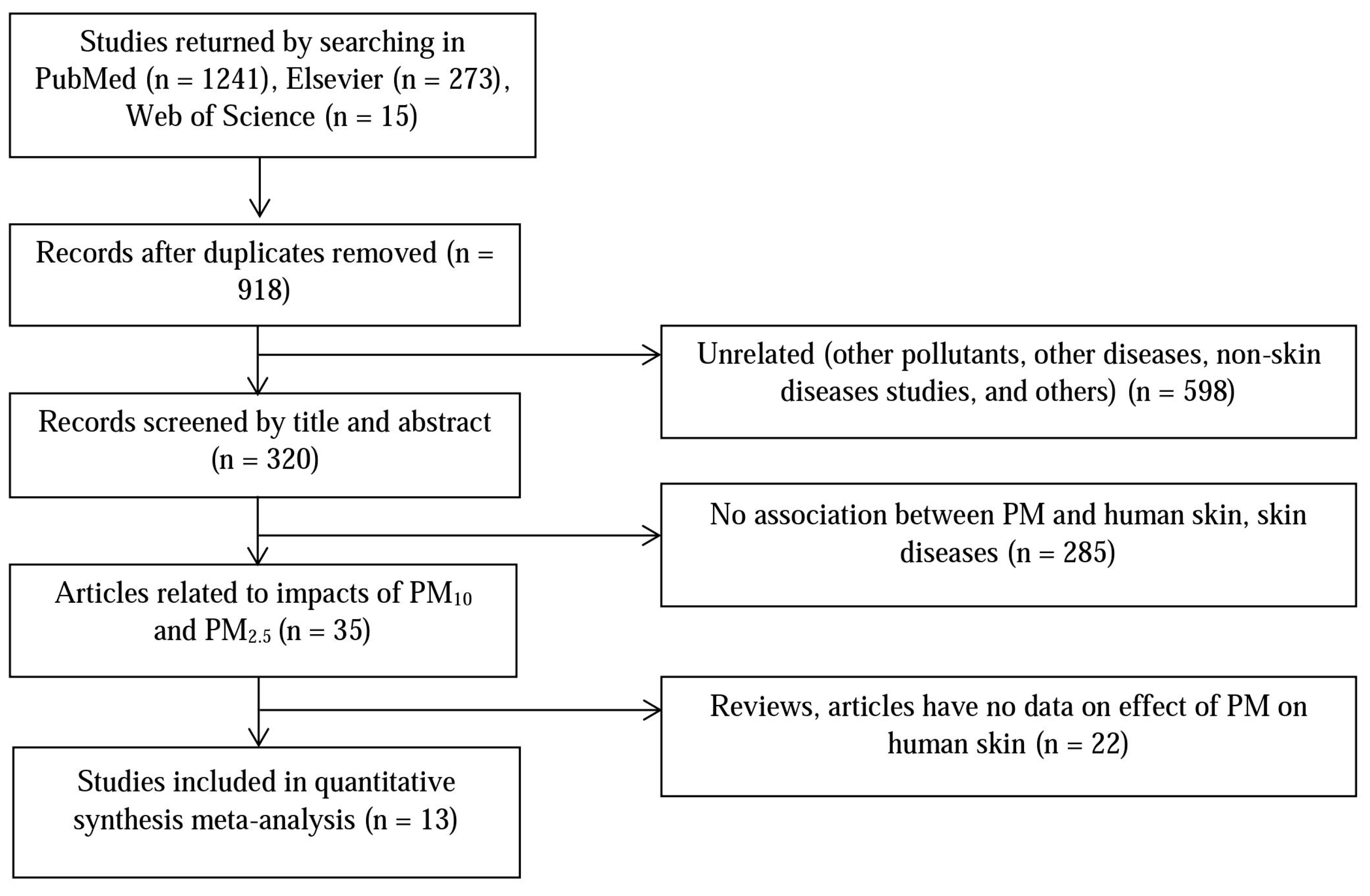
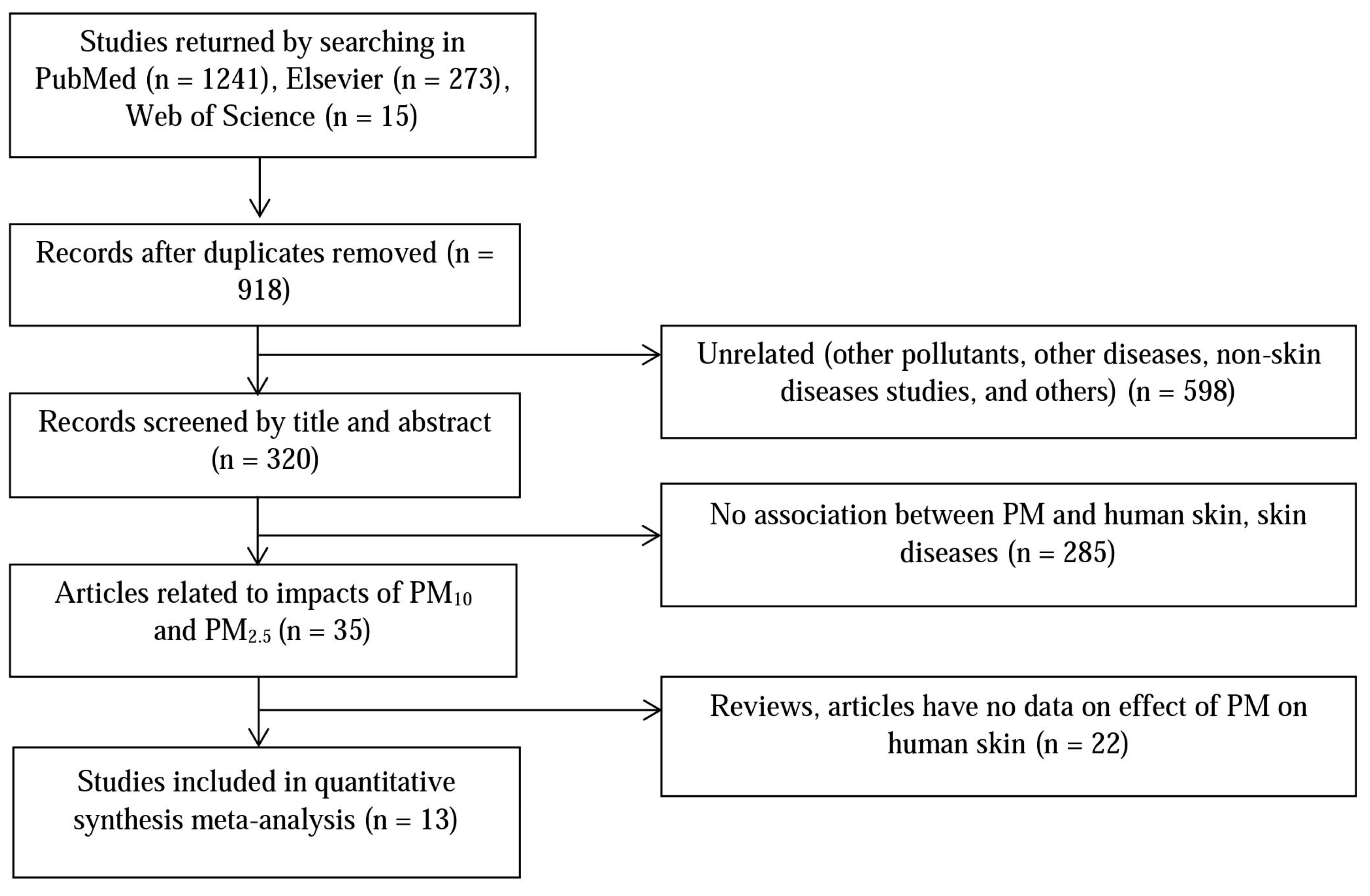
Figure 1 shows the study’s article selection process. The database searches yielded a total of 320 unique publications whose titles and abstracts were screened. After exclusion of articles not relevant to the human skin impacts of PM
10 and PM
2.5, or containing no pertinent data, 13 studies were included in the quantitative meta-analysis. Among them, there was a report of three skin diseases associated with PM [
20]: pigment spots, wrinkles, and skin aging; one study described the effect of PM on two symptoms [
16]: eczema and itchy rash; and the influences of both PM
10 and PM
2.5 on human skin were considered by three studies [
21,
22,
23]. The 13 studies included 72,000 total participants, with school children and women representing almost all of the participants (see
Table 1 for the study’s summary characteristic), and all of the studies provided raw data on the effect estimates.
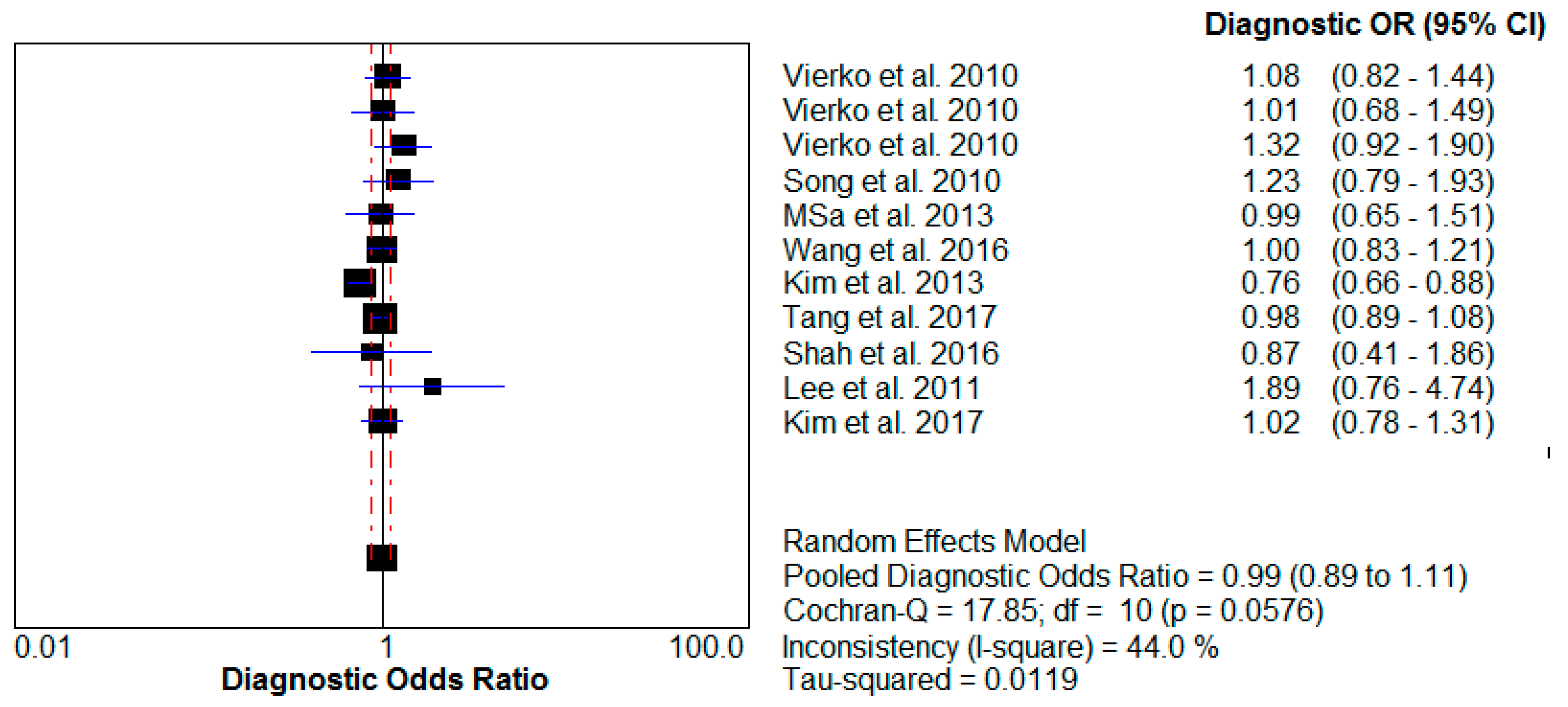
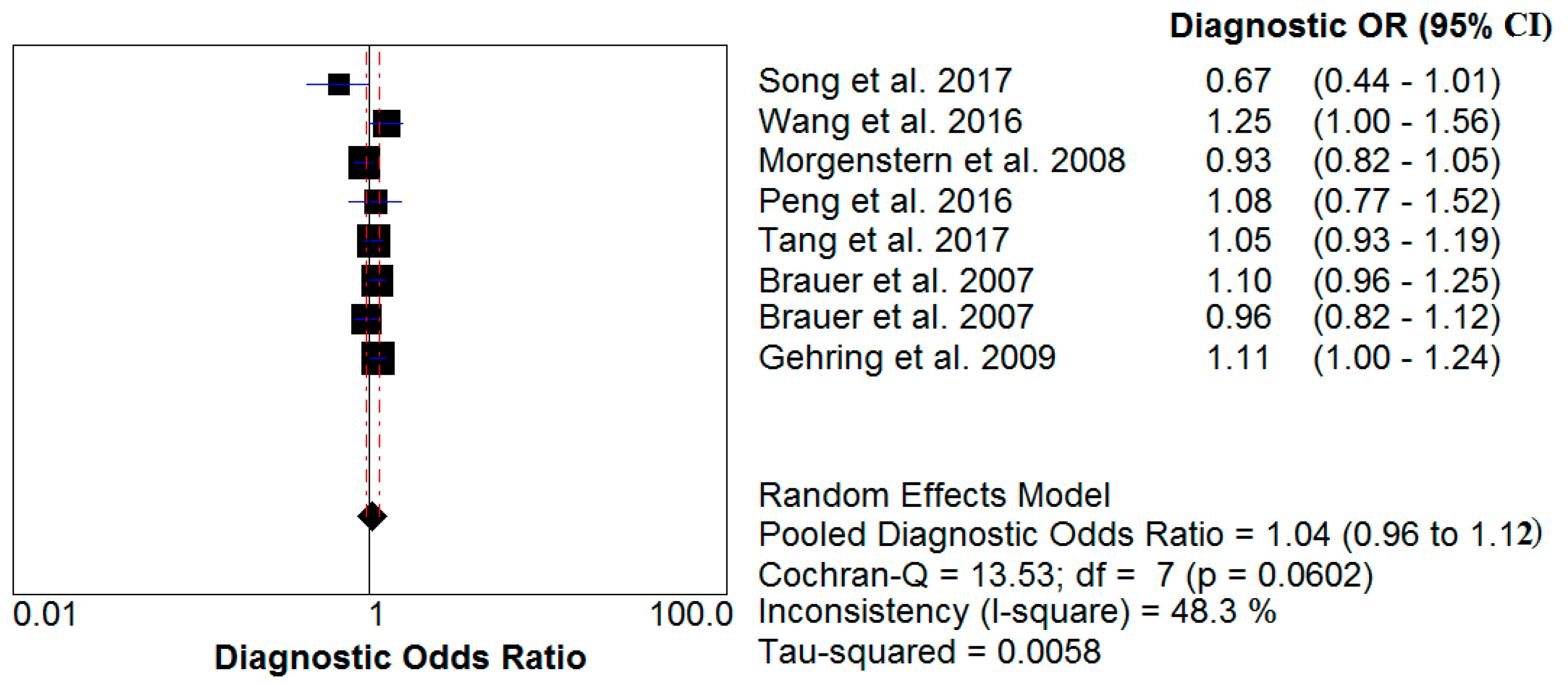
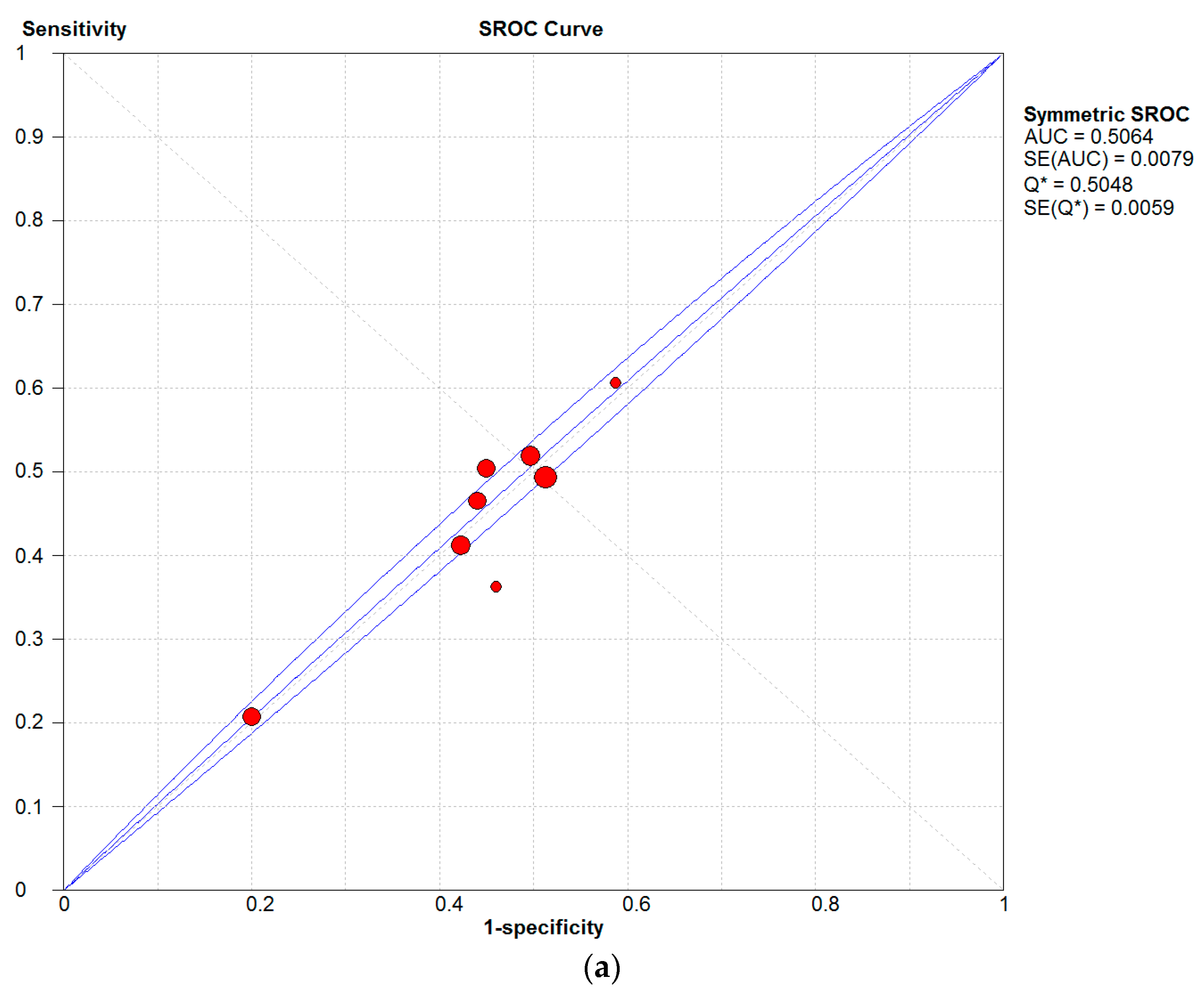
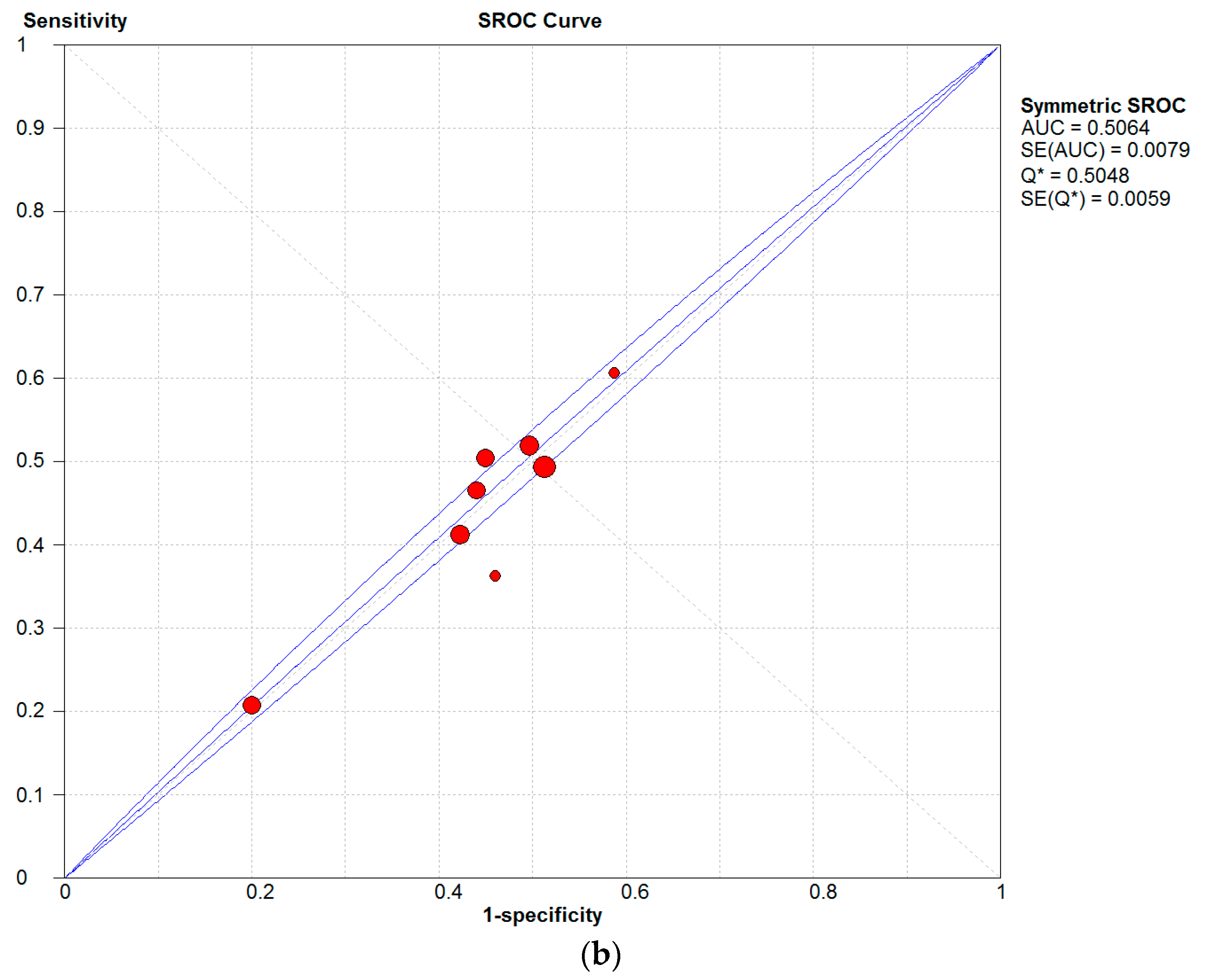
A meta-analysis of these studies yielded summary relative risks (odds ratio) of 0.99 (95% confidence interval (CI) 0.89–1.11) for PM
10 impact and 1.04 (95% CI 0.96–1.12) for PM
2.5 influence. The test for heterogeneity was not significant for either PM
10 (I
2 = 44% < 50%) or PM
2.5 (I
2 = 48.3% < 50%). The results of this analysis are provided (
Table 2,
Figure 2 and
Figure 3).
Furthermore, to assess the impact of PM on the skin in those of a young age, particularly for AD disease, a sub-analysis of studies was performed that included the influence estimates for different sized PM. The results indicated that PM
2.5 is directly related to AD in young people (
Table 3), showing an odds ratio of 1.05 (95% CI 0.95–1.16) and coefficient heterogeneity (I
2) of 46%; in contrast, the heterogeneity was significant for the PM
10 effect, showing an odds ratio of 0.96 (95% CI 0.83–1.11) and I
2 of 62.7% > 50%.
Estimates of the effects of short-term exposure to PM
10 and PM
2.5 were analyzed on the basis of increase incidence of skin diseases per 10 μg/m
3 increase in PM
10 and PM
2.5. For each increase in PM
10 and PM
2.5 concentration, the risk of human skin diseases due to PM was determined to be 1.01% (0.08–2.05) and 1.60% (0.45–2.82), respectively. The results are presented in
Table 4.
The relationship between concentrations of PM and human skin diseases over long-term exposure is presented in
Table 5. The outcomes showed that when concentrations reach upwards of 47.09 μg/m
3 for PM
10 and 26.04 μg/m
3 for PM
2.5 human skin could be adversely affected.
4. Discussion
In this systematic review and meta-analysis of more than 46,100 cases of PM impact on human skin from 13 studies, this study confirmed that both PM
10 and PM
2.5 have a statistically significant impact on skin diseases. Moreover, referencing estimates of the WHO and studies related to the impacts of PM to health [
32,
33,
34], PM not only causes usual skin diseases but may also lead to skin cancer (basal cell carcinoma and squamous cell carcinoma) [
35] and other health issues (e.g., cardiovascular disease, respiratory system, and asthma [
4,
16]).
In this study, it was found that PM is closely associated with AD, eczema, and skin allergies. In
Figure 4, a high sensitivity can be observed for the influences of both PM types on human, which is compelling evidence of an association between air pollution and human skin diseases.
Furthermore, the results demonstrated that with each 10 μg/m
3 increase, PM
10 and PM
2.5 increased disease incidences by 1.01% (0.08–2.05) and 1.60% (0.45–2.82), respectively (
Table 4). The outcomes suggest that an increase in PM
2.5 exposure concentration could slightly elevate the incidence of skin disease compared to PM
10. PMs differ not only according to their varying physical and chemical characteristic but also their concentrations by location (e.g., components, sources, structure, surface, and diameter, etc.) [
36,
37]. In general, PM
10 and PM
2.5 include inhalable particles that are small enough to penetrate deep into skin and regions of the respiratory system, especially as a consequence of long-term exposure. Humans are at risk of a greater incidence of diseases due to lower PM
2.5 concentrations (26.04 μg/m
3) than PM
10 concentrations (47.09 μg/m
3); the results of this study indicated that PM
2.5 was significantly more harmful to human health than PM
10 [
36].
Additionally, according to the results (
Table 6), these estimates demonstrated a larger impact of PM to skin allergies, which demonstrated 54% sensitivity. Even though the estimates showed lower sensitivities for AD and eczema disease (26% and 47% sensitivity, respectively), there were more cases of these skin conditions than skin allergies, particularly among children and infants [
16,
29,
31].
Most of the subjects in all of the studies were young (2–30 years old), including newborns, children, and adolescents. Indeed, the skin of individuals in these age groups is sensitive, resulting in a higher likelihood of effects due to exposure to air pollution. Long-term exposure to air-pollution sources (e.g., smoking, PM, NO
2, SO
2, etc.) in the home, outdoors, and at school contributes to many health problems such as wheezing and asthma as well as cardiovascular and skin diseases (e.g., cellulitis, skin itching, itchy aging, AD, etc.) [
17,
26,
31,
38].
The coefficient heterogeneity (I
2 = 46%) from the results of the meta-analysis demonstrated the presence of high concentrations of PM
2.5 in the air, which was one of the direct causes of AD in the younger age groups, particularly newborns and children. Furthermore, heterogeneity existed for the influence of PM
10 (I
2 = 62.7% > 50%), but it is not easy to include or exclude the causal effect of PM
10 on AD diseases, as more research is needed in order to obtain better statistical evidence and an enhanced understanding of that possible association. In particular, higher contents of cadmium, copper, lead, nickel, vanadium, and zinc in PM
2.5 were associated with increased eczema prevalence and AD [
38], and the ratio of heavy metals in PM was more abundant in PM
2.5 than in PM
10 [
39], thus contributing towards making PM
2.5 potentially more harmful to humans than PM
10, specifically via oxidative stress. Therefore, the next standard will have to focus on smaller particles that are more likely to be responsible for adverse health effects.
5. Conclusions
Observationally, PM is one of the most common components of air pollution. There is evidence that metals in PM cause DNA, skin-cell, and protein damage as well as apoptosis through the mitochondria-regulated death pathway [
39]. PM
10 and PM
2.5 in high concentrations can promote the development and exacerbation of various skin diseases. Based on these meta-analysis results, it can be added that there are associations between PM
10, PM
2.5, and skin diseases, and furthermore, that there is an increased probability of PM-associated diseases at young ages.
The major differences between the two particulate fractions are in the number, concentration, and composition of the smallest particles [
40]. PM
2.5, with its smaller size and a larger number of component metals, can easily penetrate deep into skin cells, and, as such, can pose a higher risk of AD disease than PM
10; PM
2.5 thus has a major role in adverse impacts of air pollution on human health [
41]. Therefore, PM
2.5 might be more closely associated with PM-induced skin diseases.
Even though PM has general diameter and mass concentration standards associated with skin diseases in humans, PM has varying physical and chemical characteristics, hence monitoring of PM
10 and PM
2.5 needs to be improved in many countries to asses population exposure and to assist local authorities in establishing plans for improving air quality (limits for emissions from various sources, reducing energy consumption, and changing modes of transport, etc.) [
36] so that we can control not only human skin diseases but also many serious diseases (e.g., lung cancer, cardiovascular diseases, and respiratory diseases, etc.) due to PM exposure.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}