
Components of Height and Blood Pressure among Ellisras Rural Children: Ellisras Longitudinal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Anthropometry
2.3. Blood Pressure
2.4. Quality Control
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AUC | Area under curve |
| BMI | Body mass index |
| BP | Blood pressure |
| CVD | Cardiovascular diseases |
| DBP | Diastolic blood pressure |
| ELS | Ellisras Longitudinal Study |
| ISAK | International Society for the Advancement of Kinanthropometry |
| LL | Leg length |
| NHANES III | National Health and Nutrition Examination Survey III |
| PP | Pulse pressure |
| SBP | Systolic blood pressure |
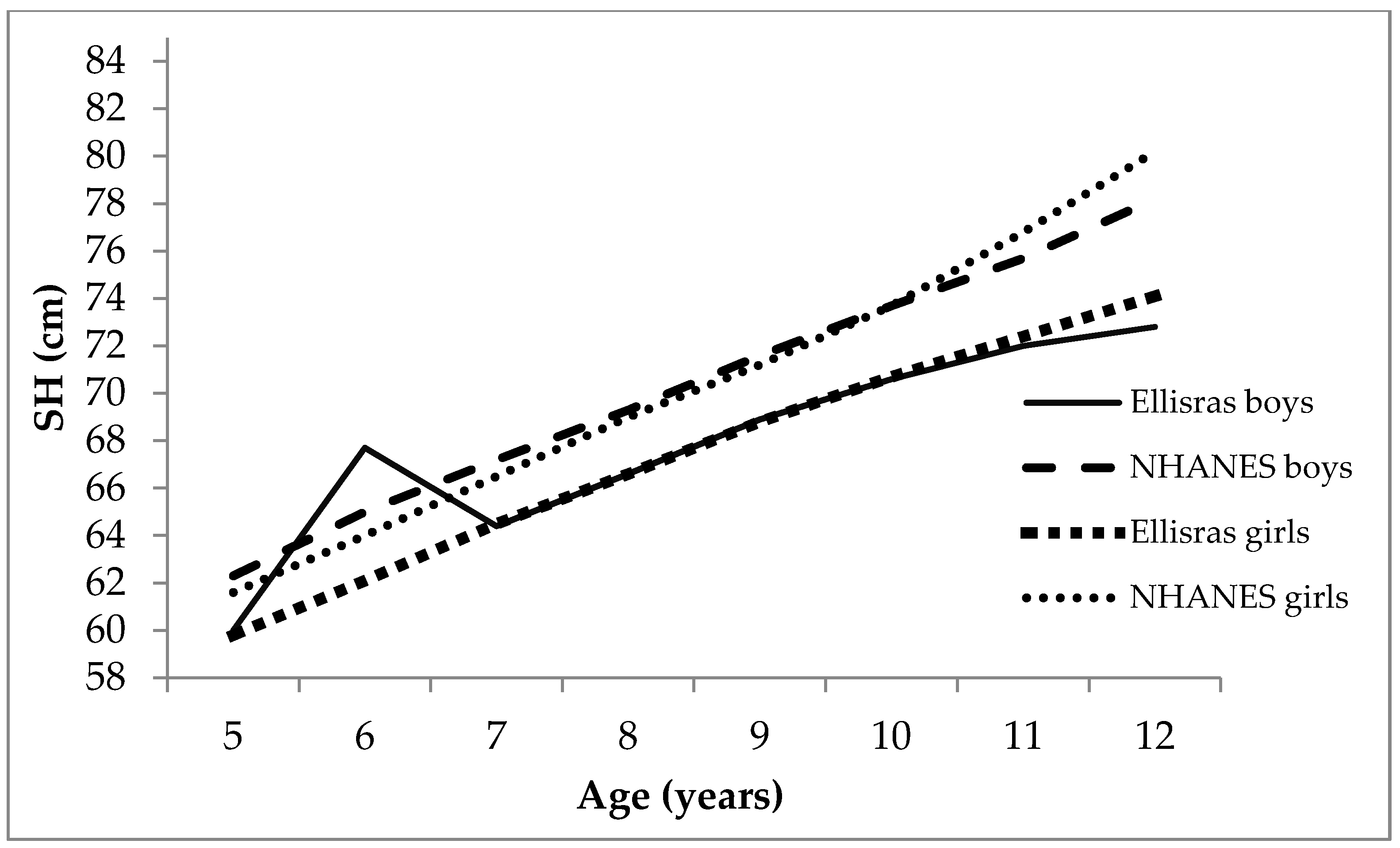
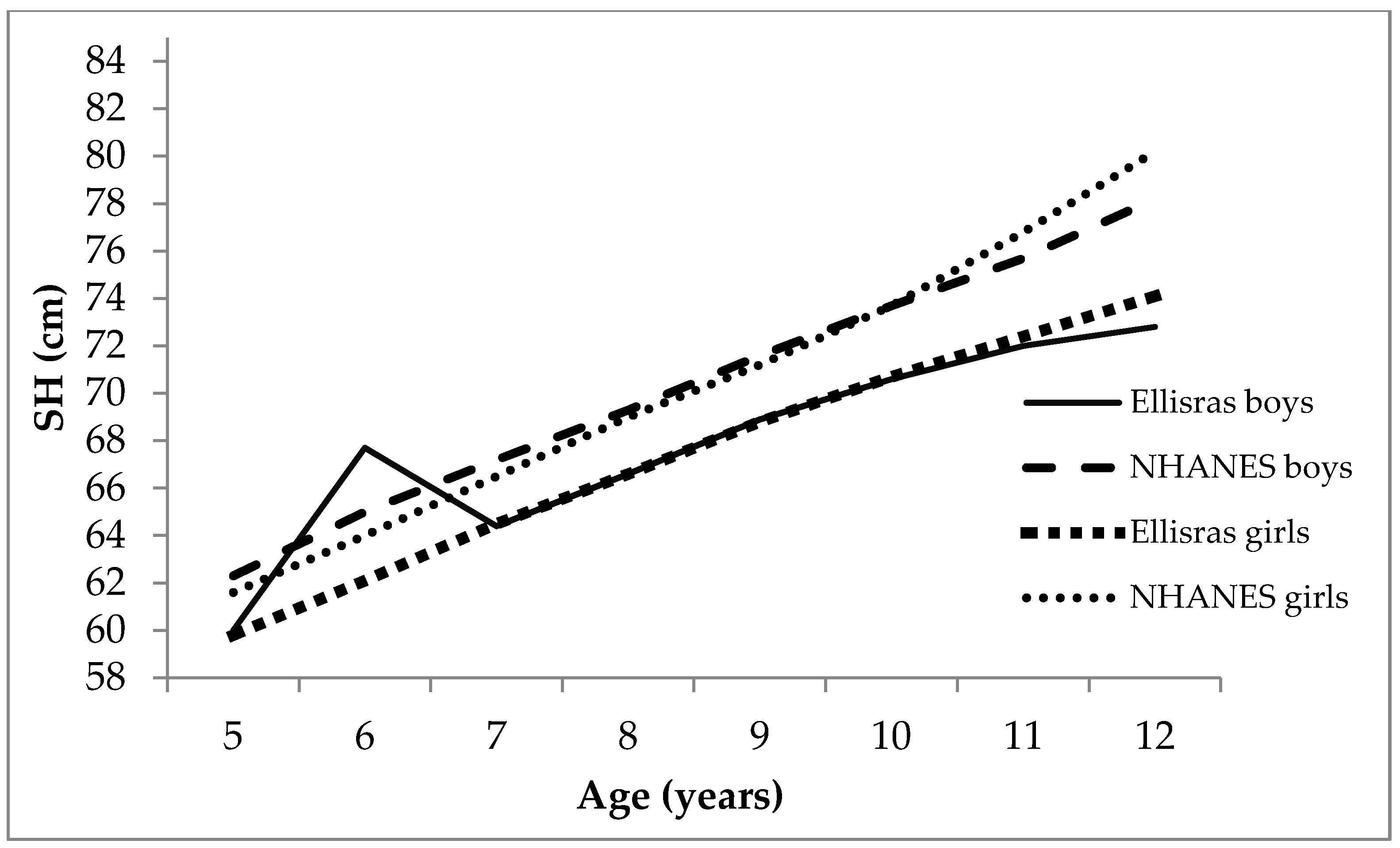
| SH | Sitting height |
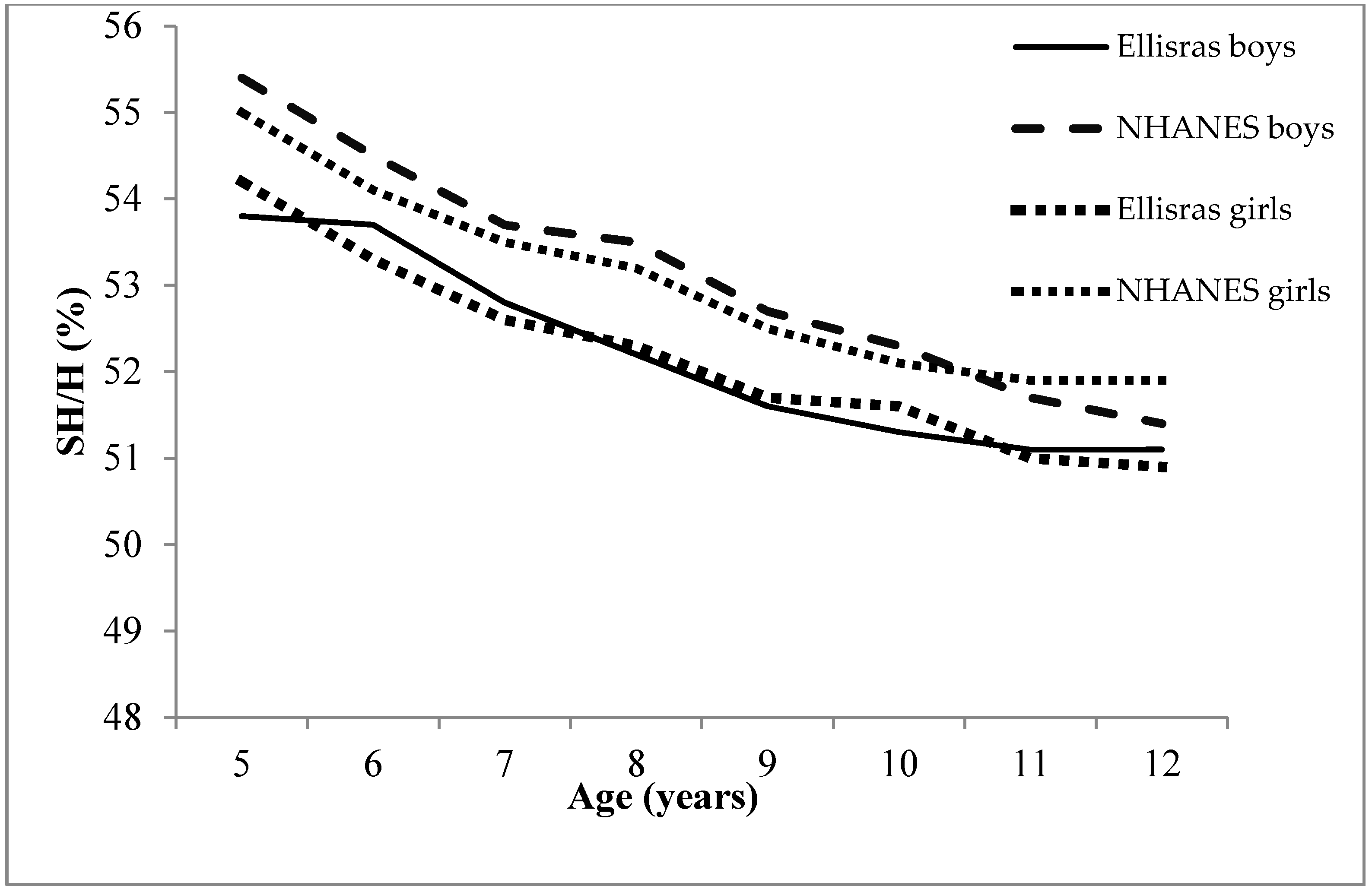
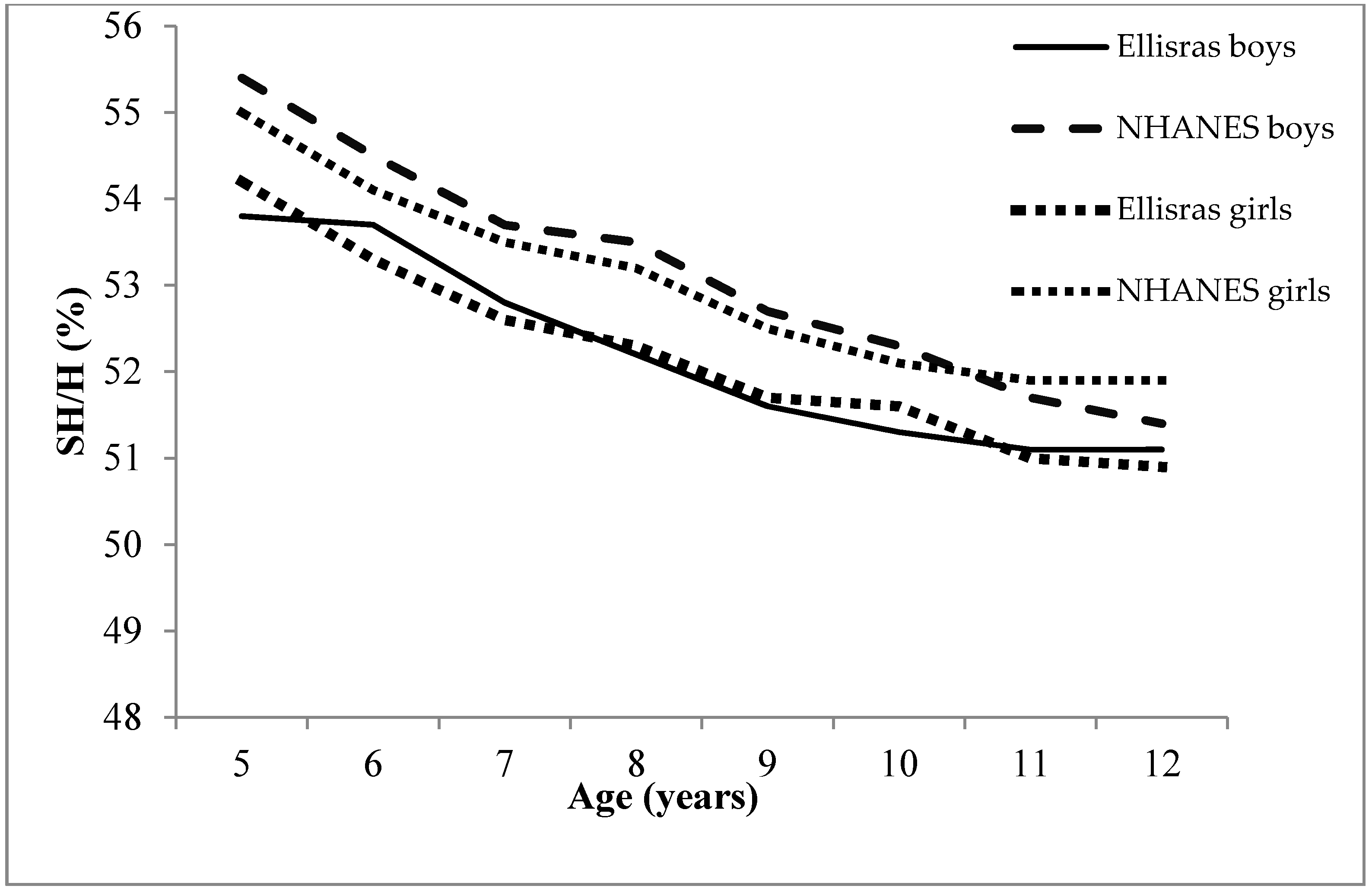
| SH/H | Sitting to height ratio |
| TEM | Technical error of measurements |
| WC | Waist circumference |
References
- Sliwa, K.; Wilkinson, D.; Hansen, C.; Ntyintyane, L.; Tibazarwa, K.; Becker, A.; Stewart, S. Spectrum of heart disease and risk factors in a black urban population in South Africa (the Heart of Soweto Study): A cohort study. Lancet 2008, 371, 915–922. [Google Scholar] [CrossRef]
- Twagirumukiza, M.; De Bacquerb, D.; Kips, J.G.; de Backer, G.; Vander Stichele, R.; Van Bortel, L.M. Current and projected prevalence of arterial hypertension in sub-Saharan Africa by sex, age and habitat: An estimate from population studies. J. Hypertens. 2011, 29, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Libhaber, E.; Carrington, M.; Damasceno, A.; Abbasi, H.; Hansen, C.; Wilkinson, D.; Sliwa, K. The clinical consequences and challenges of hypertension in urban-dwelling black Africans: Insights from the Heart of Soweto Study. Int. J. Cardiol. 2011, 146, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Van Rooyen, J.M.; Kruger, H.S.; Huisman, H.W.; Wissing, M.P.; Margetts, B.M.; Venter, C.S.; Vosrter, H.H. An epidemiological study of hypertension and its determinants in a population in transition: The THUSA study. J. Hum. Hypertens. 2000, 14, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Fredriks, A.M.; van Buuren, S.; van Heel, W.J.M.; Dijkman-Neerincx, R.H.M.; Verloove-Vanhorick, S.P.; Wit, J.M. Nationwide age references for sitting height, leg length, and sitting height/height ratio, and their diagnostic value for disproportionate growth disorders. Arch. Dis. Childhood 2005, 90, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Han, T.S.; Hooper, J.P.; Morrison, C.E.; Lean, M.E. Skeletal proportions and metabolic disorders in adults. Eur. J. Clin. Nutr. 1997, 51, 804–809. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global health Observation; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Lauer, R.M.; Anderson, A.R.; Beaglehole, R.; Burns, T.L. Factors related to tracking of blood pressure in children. U.S. National Center for Health Statistics Health Examination Surveys Cycles II and III. Hypertension 1984, 6, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, J.K.; Mzayek, F.; Liu, L.; Kieltyka, L.; Sherwin, R.; Webber, L.S.; Srinavasan, S.R.; Berenson, G.S. Origins of the “black/white” difference in blood pressure: Roles of birth weight, postnatal growth, early blood pressure, and adolescent body size: The Bogalusa heart study. Circulation 2005, 111, 1932–1937. [Google Scholar] [CrossRef] [PubMed]
- Regnault, N.; Kleinman, K.P.; Rifas-Shiman, S.L.; Lengenberg, C.; Lipshultz, S.E.; Gillman, M.W. Components of height and blood pressure in childhood. Int. J. Epidemol. 2014, 43, 149–159. [Google Scholar] [CrossRef] [PubMed]
- National High Blood Pressure Education Program (NHBPEP) Working Group on Hypertension Control in Children and Adolescents. Update on the 1987 task force report on high blood pressure in children and adolescents: A working group report from the National High Blood Pressure Education Program. Pediatrics 1996, 98, 649–658. [Google Scholar]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar]
- Monyeki, K.D.; Kemper, H.C.G.; Makgae, P.J. The association of fat patterning with blood pressure in rural South African children: The Ellisras Longitudinal Growth and Health Study. Int. J. Epidemiol. 2006, 35, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.; Kemper, H.C.G.; Makgae, P.J. Relationship between fat patterns, physical fitness and blood pressure of rural South African children: Ellisras Longitudinal Growth and Health Study. J. Hum. Hypertens. 2008, 22, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Olds, T. Anthropometrical; University of New South Wales Press: Sydney, Australia, 1996; pp. 396–410. [Google Scholar]
- Mourad, A.; Carney, S.; Gillies, A.; Jones, B.; Nanra, R.; Trevillian, P. Arm position and blood pressure: A risk factor for hypertension? J. Hum. Hypertens. 2003, 17, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Netea, R.T.; Lenders, J.W.; Smits, P.; Thien, T. Both body and arm position significantly influence blood pressure measurement. J. Hum. Hypertens. 2003, 17, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Topouchian, J.; Agnoletti, D.; Blacher, J.; Youssef, A.; Ibanez, I.; Khabouth, J.; Khawaja, S.; Beaino, L.; Asmar, R. Validation of four automatic devices for self-measurement of blood pressure according to the international protocol of the European Society of Hypertension. Vasc. Health Risk Manag. 2011, 7, 709–717. [Google Scholar] [PubMed]
- Monyeki, K.D.; de Ridder, J.H.; Steyn, N.P.; Toriola, A.; Kemper, H.C.G.; Nthangeni, M.E. Stability of somatotypes in 4–10 year-old rural South African girls. Ann. Hum. Biol. 2002, 29, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Olds, T. Antropometrica; Biosystem: Rosario Argentina, 2000. [Google Scholar]
- Frisancho, A.R. Athropometric Standards for the Assessment of Growth and Nutriritinal Status; The University of Michigan Press: Ann Arbor, MI, USA, 1990. [Google Scholar]
- Monyeki, K.D.; Cameron, N.; Getz, B. The growth and nutritional status of rural South African children aged 3–10 years old: The Ellisras Growth Study. Am. J. Biol. 2000, 12, 42–49. [Google Scholar] [CrossRef]
- Feber, M.; van Jaarveld, P.J.; Kunneke, E.; Kruger, H.S.; Schoeman, S.E.; van Stuijvenberg, M.E. Vitamin A and anthropometric status of South African preschool children from four areas with known distinct eating patterns. Nutrition 2015, 31, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Van Den Ende, C.; Twisk, J.W.R.; Monyeki, K.D. The relationship between BMI and dietary intake of primary school children from a rural area of South Africa: The Ellisras Longitudinal Study. Ann. Hum. Biol. 2004, 26, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Marcato, D.G.; Sampaio, J.D.; Alves, E.R.B.; de Jesus, J.S.A.; Fuly, J.T.B.; Giovaninni, N.P.B. Sitting-height measure are related to body mass index and blood pressure in children. Arq Bras Endocrinol. Metab. 2014, 58, 802–806. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhao, J.; Chu, Z.; Wang, L. The association between components of height and blood pressure among children and adolescents in Shandong, China. Int. J. Cardiol. 2015, 182, 18–19. [Google Scholar] [CrossRef] [PubMed]
- Kahn, H.S.; Bain, R.P.; Pullen-Smith, B. Interpretation of children’s blood pressure using a physiologic height correction. J. Chronic. Dis. 1986, 39, 521–531. [Google Scholar] [CrossRef]
- Mitchell, G.; Maloney, S.K.; Mitchell, D.; Keegan, D.J. The origin of mean arterial and jugular venous blood pressures in giraffes. J. Exp. Biol. 2006, 209, 2515–2524. [Google Scholar] [CrossRef] [PubMed]
- Brøndum, E.; Hasenkam, J.M.; Secher, N.H. Jugular venous pooling during lowering of the head affects blood pressure of the anesthetized giraffe. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.P.; Winter, P.D.; Osmond, C.; Margetts, B.; Simmonds, S.J. Weights in infancy and death from ischaemic heart disease. Lancet 1989, 2, 577–580. [Google Scholar] [CrossRef]
- Khan, A.; Haq, F.U.; Pervez, M.B.; Saleheen, D.; Frossard, P.M.; Ishaq, M. Anthropometric correlates of blood pressure in normotensive Pakistani subjects. Int. J. Cardiol. 2008, 124, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, K.D.; Kemper, H.C.G. The risk factors for elevated blood pressure and how to address cardiovascular risk factors: A review in pediatric populations. J. Hum. Hypertens. 2008, 22, 450–459. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Sample Size | Height (cm) | SH (cm) | LL (cm) | SH/H (%) | SBP (mmHg) | DBP (mmHg) | PP (mmHg) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls |
| M | M | M | M | M | M | M | M | M | M | M | M | M | M | |||
| (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | (sd) | |||
| 5 | 53 | 37 | 111.6 | 110.2 | 60.0 | 59.8 | 56.1 | 56.0 | 53.8 | 54.2 | 100.6 | 102.3 | 61.3 | 59.4 | 39.3 | 42.9 |
| (6.1) | (6.7) | (2.7) | (3.6) | (3.9) | (4.8) | (1.8) | (1.4) | (11.7) | (13.3) | (8.3) | (9.5) | (9.8) | (10.6) | |||
| 6 | 64 | 58 | 116.9 | 116.5 | 67.7 | 62.1 | 60.2 | 60.4 | 53.7 | 53.3 | 102.1 | 98.4 | 61.3 | 59.7 | 40.8 | 38.8 |
| (5.1) | (5.8) | (3.2) | (2.0) | (4.2) | (3.8) | (2.1) | (1.2) | (13.8) | (13.8) | (10.9) | (9.2) | (11.0) | (10.9) | |||
| 7 | 97 | 73 | 122.2 | 122.7 | 64.4 | 64.5 | 63.5 | 64.6 | 52.8 | 52.6 | 96.9 | 96.3 | 59.7 | 57.5 | 37.1 | 38.8 |
| (5.6) | (6.4) | (2.7) | (2.9) | (3.7) | (4.5) | (1.3) | (1.8) | (12.2) | (12.8) | (9.3) | (8.4) | (11.5) | (14.1) | |||
| 8 | 117 | 115 | 127.7 | 127.3 | 66.6 | 66.6 | 66.5 | 67.1 | 52.2 | 52.3 | 97.3 | 96.4 | 59.1 | 59.0 | 38.2 | 37.4 |
| (6.5) | (5.3) | (3.4) | (2.6) | (7.0) | (3.6) | (1.5) | (1.1) | (10.2) | (10.0) | (9.1) | (9.7) | (9.9) | (10.3) | |||
| 9 | 184 | 180 | 133.5 | 133.1 | 68.9 | 68.8 | 70.8 | 70.9 | 51.6 | 51.7 | 99.7 | 99.0 | 61.9 | 61.0 | 37.9 | 38.0 |
| (6.2) | (5.3) | (3.2) | (2.7) | (4.1) | (3.8) | (1.1) | (1.3) | (10.7) | (11.3) | (9.9) | (9.8) | (9.9) | (10.3) | |||
| 10 | 231 | 220 | 137.7 | 137.1 | 70.6 | 70.7 | 73.3 | 73.7 | 51.3 | 51.6 | 99.5 | 99.7 | 60.2 | 59.8 | 39.3 | 39.9 |
| (6.1) | (6.1) | (3.1) | (3.2) | (4.2) | (3.8) | (1.4) | (1.6) | (9.7) | (10.2) | (9.4) | (9.2) | (10.4) | (10.8) | |||
| 11 | 187 | 178 | 141.0 | 142.1 | 72.0 | 72.4 | 75.3 * | 76.8 * | 51.1 | 51.0 | 101.6 | 102.0 | 62.0 | 60.9 | 39.6 | 41.1 |
| (7.1) | (6.6) | (3.5) | (3.2) | (4.7) | (4.2) | (1.5) | (1.5) | (10.8) | (11.9) | (9.2) | (9.3) | (9.4) | (11.3) | |||
| 12 | 96 | 71 | 142.6 * | 145.6 * | 72.8 * | 74.1 * | 76.4 * | 78.8 * | 51.1 | 50.9 | 101.9 | 101.8 | 60.8 | 63.1 | 41.1 | 38.7 |
| (6.2) | (7.6) | (3.3) | (3.8) | (4.1) | (4.8) | (1.2) | (1.3) | (9.6) | (10.4) | (8.1) | (8.4) | (10.4) | (9.11) | |||
| Unadjusted | Adjusted for Age, Gender, BMI, and WC | |||||||
|---|---|---|---|---|---|---|---|---|
| β | p-Value | 95% CI | β | p-Value | 95% CI | |||
| SBP | ||||||||
| Height | 0.127 | 0.0001 | 0.082 | 0.172 | 0.058 | 0.2320 | −0.037 | 0.153 |
| SH | 0.134 | 0.0001 | 0.210 | 0.415 | 0148 | 0.1091 | −0.033 | 0.328 |
| LL | 0.187 | 0.0001 | 0.119 | 0.255 | 0.037 | 0.6060 | −0.102 | 0.176 |
| SH/H | −0.023 | 0.3160 | −45.141 | 14.575 | 17.549 | 0.3302 | −17.806 | 52.905 |
| DBP | ||||||||
| Height | 0.080 | 0.0002 | 0.042 | 0.118 | 0.087 | 0.0341 | 0.007 | 0.168 |
| SH | 0.088 | 0.0001 | 0.086 | 0.259 | 0.108 | 0.1680 | −0.045 | 0.261 |
| LL | 0.121 | 0.0001 | 0.064 | 0.179 | 0.123 | 0.0410 | 0.005 | 0.241 |
| SH/H | −0.044 | 0.0540 | −49.629 | 0.407 | −11.900 | 0.436 | 41.856 | 18.057 |
| PP | ||||||||
| Height | 0.047 | 0.0331 | 0.004 | 0.090 | −0.029 | 0.5301 | −0.120 | 0.062 |
| SH | 0.140 | 0.0050 | 0.041 | 0.238 | 0.040 | 0.6502 | −0.135 | 0.213 |
| LL | 0.065 | 0.0481 | 0.001 | 0.130 | −0.086 | 0.2050 | −0.220 | 0.047 |
| SH/H | 9.328 | 0.5182 | −18.993 | 37.649 | 29.449 | 0.0490 | −4.441 | 63.338 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramoshaba, N.; Monyeki, K.; Hay, L. Components of Height and Blood Pressure among Ellisras Rural Children: Ellisras Longitudinal Study. Int. J. Environ. Res. Public Health 2016, 13, 856. https://doi.org/10.3390/ijerph13090856
Ramoshaba N, Monyeki K, Hay L. Components of Height and Blood Pressure among Ellisras Rural Children: Ellisras Longitudinal Study. International Journal of Environmental Research and Public Health. 2016; 13(9):856. https://doi.org/10.3390/ijerph13090856
Chicago/Turabian StyleRamoshaba, Nthai, Kotsedi Monyeki, and Leon Hay. 2016. "Components of Height and Blood Pressure among Ellisras Rural Children: Ellisras Longitudinal Study" International Journal of Environmental Research and Public Health 13, no. 9: 856. https://doi.org/10.3390/ijerph13090856