
Individual Monitoring and Occupational Dose Record Management in China: History, Current Status and Perspectives


Abstract
:1. Introduction
2. History
3. Current Status
3.1. Radiation Units and Radiation Workers and Their Distribution
3.2. Laws and Regulations Governing Individual Monitoring
- (1)
- Having legal representative qualifications or legal-authorized qualification;
- (2)
- Being capable of carrying out corresponding technical service work independently;
- (3)
- Having a permanent office and workplace and working conditions;
- (4)
- Having a reasonable post setting and well-defined responsibility scope;
- (5)
- Having robust quality assurance system.
- (1)
- Being fit for management, technique and quality control required by the programs;
- (2)
- Being familiar with the relevant laws, standards and documents as well as quality management manuals;
- (3)
- Technical director of individual monitoring with junior college diploma or above, or the intermediate technical titles or above and having experiences in related work more than three years;
- (4)
- Being qualified through training and examination;
- (5)
- Total number of operators is not less than three.
- (1)
- Having corresponding instruments and equipment required for carrying out technical service of individual monitoring;
- (2)
- Type, quantity, performance, range and precision of the instruments and equipment are capable of meeting the needs of the work, and the instruments and equipment can run well;
- (3)
- Being regularly subject to metrological verification;
- (4)
- Having a complete set of operating procedures.
3.3. Individual Monitoring Services Providers
3.4. Individual Monitoring Personnel, Equipment and Period
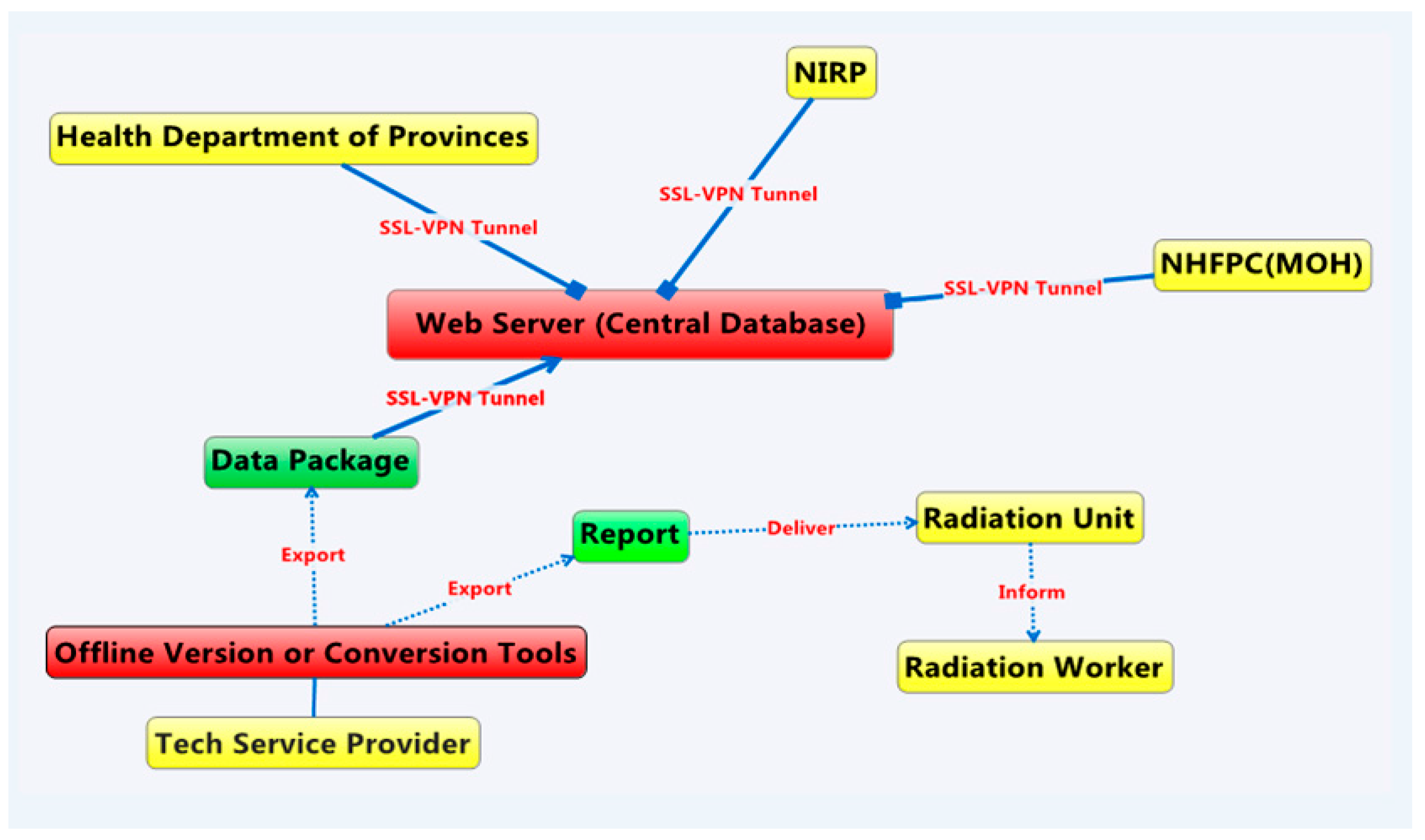
3.5. Dose Record Management and National Dose Register
3.6. Trend of Individual Monitoring Coverage and Annual per Capita Effective Dose
4. Perspectives
4.1. Individual Monitoring in Nuclear Medicine and Interventional Radiology to Be Strengthened
4.2. Regulations and Standards to Be Improved
4.3. Miners and Aircrews to Be Covered
4.4. Safety Awareness of the Radiation Workers to Be Raised
4.5. Supervision and Enforcement to Be Strengthened
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Xiong, L.; Kuang, Y.G. Quality control and management of occupational external dose monitoring for radiation workers. In Proceedings of the Ninth China Nuclear Society Nuclear Technology, Nuclear Applications, Nuclear Economy Forum, Hangzhou, China, 2012. (In Chinese)
- National Occupational Health Standard of China. GBZ 128-2002. In Specifications of Individual Monitoring for Occupational External Exposure; China Standard Press: Beijing, China, 2002. [Google Scholar]
- The Ministry of Health of the People’s Republic of China. Decree of the Ministry of Health of the People’s Republic of China (No. 55). Management Methods for Occupational Health of Radiation Workers; The Ministry of Health of the People’s Republic of China: Beijing, China, 2007.
- Standing Committee of the National People’s Congress. Law of the People’s Republic of China on Prevention and Control of Occupational Disease; Decree of the President of the People’s Republic of China (No. 52); Standing Committee of the National People’s Congress: Beijing, China, 2011. [Google Scholar]
- Sun, Q.F.; Niu, H.W.; Li, X.J. Several problems of occupational health management of radiation workers in China. Chin. J. Radiol. Med. Prot. 2014, 34, 161–163. (In Chinese) [Google Scholar]
- The State Council of the People’s Republic of China. Decree of the State Council of the People’s Republic of China (No. 449). Regulations on Safety and Protection of Radioisotopes and Rays Installations; The State Council of the People’s Republic of China: Beijing, China, 2005.
- The Ministry of Health of China. Red tape of the Ministry of Health of China. Qualification Conditions of Individual Monitoring Services for Radiation Workers; The Ministry of Health of China: Beijing, China, 2008.
- National Occupational Health Standard of China. GBZ 207-2008. In Testing Criteria of Personnel Dosimetry Performance; China Standard Press: Beijing, China, 2008. [Google Scholar]
- Wang, X.T.; Cao, L.; Yang, Y.Y. Improvement to existing individual dose monitoring in China. Radiat. Prot. Bull. 2012, 32, 29–31. (In Chinese) [Google Scholar]
- Yu, H.T.; Niu, H.W.; Sun, Q.F.; Fu, Y.H.; Fan, Y.H.; Yue, B.R. The profile of ESOREX project of European Union and the analysis of individual monitoring present situation in Europe. Chin. J. Radiol. Health 2010, 19, 37–39. (In Chinese) [Google Scholar]
- Yu, H.T.; Niu, H.W.; Sun, Q.F.; Hu, A.Y.; Cao, L.; Yuan, L.; Yue, B.R. The analysis of situation of individual monitoring services in China. Chin. J. Radiol. Med. Prot. 2010, 30, 466–468. (In Chinese) [Google Scholar]
- Yu, C.; Yu, H.T.; Sun, Q.F.; Fu, Y.H.; Niu, H.W.; Cheng, X.Q. The analysis of basic situation of the national radiological health institutions. Chin. J. Radiol. Health 2014, 23, 125–129. (In Chinese) [Google Scholar]
- Fu, Y.H.; Sun, Q.F.; Du, W.X.; Yue, B.R. Radiological health statistics report in China. Chin. J. Radiol. Med. Prot. 2009, 29, 101–103. (In Chinese) [Google Scholar]
- Li, D.P. Some comments on the computer management of individual dose. Radiat. Prot. 1997, 17, 318–320. (In Chinese) [Google Scholar]
- Xu, G.Q.; Tu, Y. Problems and countermeasures about the data management software of occupational external exposure dose. Chin. J. Radiol. Health 2005, 14, 24–25. (In Chinese) [Google Scholar]
- Yu, H.T.; Niu, H.W.; Sun, Q.F.; Fu, Y.H.; Fan, Y.H.; Yue, B.R. Development of the national register of radiation workers: Subsystem for individual monitoring of external exposure. Chin. J. Radiol. Med. Prot. 2010, 30, 66–72. (In Chinese) [Google Scholar]
- Chinese Society of Nuclear Medicine. Briefing of current situation survey of national nuclear medicine of China in 2014. Chin. J. Nucl. Med. Mol. Imaging 2014, 34, 389. (In Chinese) [Google Scholar]
- Lei, S.J.; Sun, Q.F. Exposed dose and protection of interventional radiology staff. Chin. Prev. Med. 2006, 7, 558–559. (In Chinese) [Google Scholar]
- Shao, Y.P.; Xu, X.C.; Sun, Q.F.; Liu, J.X.; Wang, Y.; Zhao, F.L.; Su, X. Analysis of lens opacity among 730 radiation workers. Chin. J. Radiol. Med. Prot. 2014, 34, 136–139. (In Chinese) [Google Scholar]
- Fan, S.M.; Qiu, Y.H.; Zhuang, L. Analysis of exposed dose and health of interventional radiology workers. Chin. J. Radiol. Health 2002, 11, 110. (In Chinese) [Google Scholar]
- China Standard Press. National Standard of People’s Republic of China. GB 18871-2002. Basic Standards for Protection against Ionizing Radiation and for the Safety of Radiation Sources; China Standard Press: Beijing, China, 2002. [Google Scholar]
- International Atomic Energy Agency. Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards; IAEA: Vienna, Austria, 2014. [Google Scholar]
- Li, X.Y.; Sun, Q.F.; Su, X. Investigation and control of radioactive occupational hazards in non-uranium mines in China. Chin. J. Radiol. Med. Prot. 2008, 28, 557–558. (In Chinese) [Google Scholar]
- Yang, Y.H.; Feng, Y.J.; Chen, W.R.; Luo, L.Y.; Zhang, T.; Peng, X.T.; Zhang, J.; Zhao, W.J. Estimation of cosmic radiation level of flight personnel in a certain airline in 2007. J. Environ. Health 2008, 25, 1101–1102. (In Chinese) [Google Scholar]
- International Atomic Energy Agency. Assessment of Occupational Exposure due to External Sources of Radiation; IAEA Safety Guide No.RS-G-1.3; IAEA: Vienna, Austria, 1999. [Google Scholar]

{kind=link}
| Laws and Regulations | Articles | Specific Contents |
|---|---|---|
| Law of the People’s Republic of China on Prevention and Control of Occupational Disease [4] | Article 26 | Radioactive workplace and/or radioisotope storage and transport device shall be equipped, by its operator, with necessary protection equipment and alarm devices, ensuring that workers involving radiation exposure must wear personal dosimeters. |
| Regulations on Safety and Protection of Radioisotopes and Rays Installations [6] | Article 29 | A producer, distributor and/or user of radioisotope and radiation generator shall, in compliance with the relevant national regulations on individual monitoring and health management, perform individual monitoring and occupational health examination of radiation workers for production, distribution and use of radioisotope and radiation generator and establish individual dose files and occupational health surveillance files. |
| Management Methods for Occupational Health of Radiation Workers [3] | Articles 11 to 17 | The detailed requirements of the individual monitoring period, individual monitoring file, wearing of dosimeters, qualification review of individual monitoring services, delivery of the reports, and report procedure of individual monitoring results. |
| Qualification Conditions of Individual Monitoring Services for Radiation Workers [7] | Articles 1 to 3 | Requirements for service providers, personnel, instruments and equipment. |
| Period | Workers Should be Monitored/Thousand | Workers Actually Monitored/Thousand | Individual Monitoring Coverage/% | Collective Effective Dose/(Man·Sv) | Annual per Capita Effective Dose/mSv |
|---|---|---|---|---|---|
| 1986–1990 | 107.4 | 19.8 | 18.4 | 231 | 2.15 |
| 1994–1995 | 89.1 | 34.7 | 38.9 | 131 | 1.47 |
| 1996–2000 | 114.7 | 59.7 | 52.0 | 164 | 1.43 |
| 2002–2005 | 150.0 | 50.3 | 33.5 | 171.0 | 1.14 |
| 2009–2013 | 189.2 | 159.4 | 84.2 | 100.6 | 0.53 |
| Occupation Category | Period | Workers Should be Monitored | Workers Actually Monitored | Individual Monitoring Coverage/% | Collective Effective Dose/(Man·Sv) | Annual per Capita Effective Dose/mSv |
|---|---|---|---|---|---|---|
| Industrial Detecting | 1986–1990 | 4270 | 14.1 | 1.64 | ||
| 1994–1995 | 7470 | 22.4 | 1.42 | |||
| 1996–2000 | 10200 | 22.2 | 1.18 | |||
| Industrial irradiation | 1997 | 1327 | 752 | 56.7 | 0.668 | 0.89 |
| 1998 | 1370 | 796 | 58.1 | 0.811 | 1.02 | |
| 1999 | 1113 | 654 | 58.8 | 0.643 | 0.98 | |
| 2000 | 1396 | 827 | 59.2 | 0.519 | 0.63 | |
| operation of the accelerator | 1997 | 989 | 739 | 74.7 | 0.473 | 0.64 |
| 1998 | 1187 | 722 | 60.8 | 0.413 | 0.57 | |
| 1999 | 975 | 553 | 56.7 | 0.224 | 0.41 | |
| 2000 | 790 | 437 | 55.3 | 0.15 | 0.34 | |
| Others | 1994 | 16032 | 7528 | 47 | 9.65 | 1.28 |
| 1995 | 15378 | 7408 | 48.2 | 11.6 | 1.57 | |
| 1996 | 18051 | 9641 | 53.4 | 12.3 | 1.28 | |
| 1997 | 23638 | 12108 | 51.2 | 14.6 | 1.2 | |
| 1998 | 23999 | 12713 | 53 | 15.2 | 1.2 | |
| 1999 | 22862 | 12227 | 53.5 | 16.5 | 1.35 | |
| 2000 | 19999 | 12696 | 63.5 | 13.8 | 1.09 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-B.; Yu, H.-T.; Sun, Q.-F. Individual Monitoring and Occupational Dose Record Management in China: History, Current Status and Perspectives. Int. J. Environ. Res. Public Health 2016, 13, 558. https://doi.org/10.3390/ijerph13060558
Wang H-B, Yu H-T, Sun Q-F. Individual Monitoring and Occupational Dose Record Management in China: History, Current Status and Perspectives. International Journal of Environmental Research and Public Health. 2016; 13(6):558. https://doi.org/10.3390/ijerph13060558
Chicago/Turabian StyleWang, Hong-Bo, Hai-Tao Yu, and Quan-Fu Sun. 2016. "Individual Monitoring and Occupational Dose Record Management in China: History, Current Status and Perspectives" International Journal of Environmental Research and Public Health 13, no. 6: 558. https://doi.org/10.3390/ijerph13060558