
Global Evidence on the Association between POS Advertising Bans and Youth Smoking Participation



Abstract
:1. Introduction
2. Methods
2.1. Data and Measures
MPOWER
2.2. Global Youth Tobacco Survey (GYTS)
2.3. Methodology
3. Results
4. Discussions
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- State of Evidence Review. Institute for Global Tobacco Control. Point of Sale Promotion of Tobacco Products January 2013. Available online: http://globaltobaccocontrol.org/sites/default/files/2013POS_soe.pdf (accessed on 8 March 2016).
- Pollay, R.W. More than meets the eye: On the importance of retail cigarette merchandising. Tob. Control 2007, 16, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Lavack, A.M.; Toth, G. Tobacco point-of-purchase promotion: Examining tobacco industry documents. Tob. Control 2006, 15, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Feighery, E.C.; Ribisl, K.M.; Schleicher, N.C.; Clarket, P.I. Retailer participation in cigarette company incentive programs is related to increased levels of cigarette advertising and cheaper cigarette prices in stores. Prev. Med. 2004, 38, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, M.; Terry-McElrath, Y.; Chaloupka, F.J.; Barker, D.C.; Slater, S.J.; Clark, P.I.; Giovino, G.A. Tobacco industry marketing at point of purchase after the 1998 MSA billboard advertising ban. Am. J. Public Health 2002, 92, 937–940. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, M.; Morley, C.; Horan, J.; Cummings, K.M. The cigarette pack as image: New evidence from tobacco industry documents. Tob. Control 2002, 11, 73–80. [Google Scholar] [CrossRef]
- Bloom, P.N. Role of slotting fees and trade promotions in shaping how tobacco is marketed in retail stores. Tob. Control 2001, 10, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.; Cameron, C.; McGee, R.; Marsh, L.; Hoek, J. Point-of-sale tobacco promotion and youth smoking: A meta-analysis. Tob. Control 2016. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.; McGee, R.; Marsh, L.; Hoek, J. A systematic review on the impact of point-of-sale tobacco promotion on smoking. Nicotine Tob. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Center for Public Health Systems Science. A Tobacco Control Guide—Center for Public Health Systems; Tobacco Control Legal Consortium: St. Louis, MO, USA, 2014. [Google Scholar]
- Spanopoulos, D.; Britton, J.; McNeill, A.; Ratschen, E.; Szatkowski, L. Tobacco display and brand communication at the point of sale: Implications for adolescent smoking behaviour. Tob. Control 2014, 23, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.E.; Loomis, B.R.; Busey, A.H.; Farrelly, M.C.; Willett, L.G.; Juster, H.R. Influence of retail cigarette advertising, price promotions, and retailer compliance on youth smoking-related attitudes and behaviors. J. Public Health Manag. Pract. 2013, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.E.; Nonnemaker, J.M.; Loomis, B.R.; Baig, A.; Hill, E.; Holloway, J.W.; Farrelly, M.C.; Shafer, P.R. Influence of tobacco displays and ads on youth: A virtual store experiment. Pediatrics 2013, 131, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Shadel, W.G.; Martino, S.C.; Setodji, C.; Scharf, D. Exposure to pro-smoking media in college students: Does type of media channel differentially contribute to smoking risk? Ann. Behav. Med. 2013, 45, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.L.; Jason, L.A.; Pokorny, S.; Hunt, Y. Exploration of the link between tobacco retailers in school neighborhoods and student smoking. J. Sch. Health 2013, 83, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.; Sacks, R.; Rane, M.; Kansagra, S.M. Exposure to tobacco retail outlets and smoking initiation among New York City adolescents. J. Urban Health 2013, 90, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, T.R.; Cantrell, J.; Anesetti-Rothermel, A.; Ganz, O.; Vallone, D.M.; Abrams, D.B. Geospatial exposure to point-of-sale tobacco: Real-time craving and smoking-cessation outcomes. Am. J. Prev. Med. 2013, 45, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Dauphinee, A.L.; Doxey, J.R.; Schleicher, N.C.; Fortmann, S.P.; Henriksen, L. Racial differences in cigarette brand recognition and impact on youth smoking. BMC Public Health 2013. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, A.M.; Moodie, C.; Hastings, G. The association between pointof-sale displays and youth smoking susceptibility. Nicotine Tob. Res. 2012, 14, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Loomis, B.R.; Kim, A.E.; Busey, A.H.; Farrellya, M.C.; Willettb, J.G.; Justerb, H.R. The density of tobacco retailers and its association with attitudes toward smoking, exposure to point-of-sale tobacco advertising, cigarette purchasing, and smoking among New York youth. Prev. Med. 2012, 55, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Widome, R.; Brock, B.; Noble, P.; Forster, J.L. The relationship of point-of-sale tobacco advertising and neighborhood characteristics to underage sales of tobacco. Eval. Health Prof. 2012, 35, 331–345. [Google Scholar] [CrossRef] [PubMed]
- West, J.H.; Blumberg, E.J.; Kelley, N.J.; Hill, L.; Sipan, C.L.; Schmitz, K.E.; Ryan, S.; Clapp, J.D.; Hovell, M.F. Does proximity to retailers influence alcohol and tobacco use among Latino adolescents? J. Immigr. Minor. Health 2010, 12, 626–633. [Google Scholar]
- Henriksen, L.; Schleicher, N.C.; Feighery, E.C.; Fortmann, S.P. A longitudinal study of exposure to retail cigarette advertising and smoking initiation. Pediatrics 2010, 126, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Paynter, J.; Edwards, R.; Schluter, P.; McDuff, I. Point of sale tobacco displays and smoking among 14–15 year olds in New Zealand: A cross-sectional study. Tob. Control 2009, 18, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Paynter, J.; Edwards, R. The impact of tobacco promotion at the point of sale: A systematic review. Nicotine Tob. Res. 2009, 11, 25–35. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, W.J.; Mistry, R.; Lu, Y.; Patel, M.; Zheng, H.; Dietsch, B. Density of tobacco retailers near schools: Effects on tobacco use among students. Am. J. Public Health 2009, 99, 2006–2013. [Google Scholar] [CrossRef] [PubMed]
- Dubray, J.M.; Schwartz, R.M.; Garcia, J.M.; Bondy, S.J.; Victor, J.C. Vendor compliance with Ontario’s tobacco point of sale legislation. Can. J. Public Health 2009, 100, 109–112. [Google Scholar]
- Quedley, M.; Ng, B.; Sapre, N.; Blakiston, M.; Crawford, A.; Devadas, R.; McLaren, H.; Anand, S.; Tipu, M.; Dayal, V. In sight, in mind: Retailer compliance with legislation on limiting retail tobacco displays. Nicotine Tob. Res. 2008, 10, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Planinac, L.; Griffin, K.; Robinson, D.J.; O'Connor, S.C.; Lavack, A.; Thompson, F.E.; Di Nardo, J. Tobacco promotions at point-of-sale: The last hurrah. Can. J. Public Health 2008, 99, 166–171. [Google Scholar]
- Henriksen, L.; Feighery, E.C.; Schleicher, N.C.; Cowlingc, D.W.; Klineb, R.S.; Fortmanna, S.P. Is adolescent smoking related to the density and proximity of tobacco outlets and retail cigarette advertising near schools? Prev. Med. 2008, 47, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Slater, S.; Chaloupka, F.; Wakefield, M.; Johnston, L.D.; O’Malley, P.M. The impact of retail cigarette marketing practices on youth smoking uptake. Arch. Pediatr. Adolesc. Med. 2007, 161, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Feighery, E.; Henriksen, L.; Wang, Y.; Schleicher, N.C.; Fortmann, S.P. An evaluation of four measures of adolescents’ exposure to cigarette marketing in stores. Nicotine Tob. Res. 2006, 8, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, L.; Feighery, E.; Wang, Y.; Fortmann, S.P. Association of retail tobacco marketing with adolescent smoking. Am. J. Public Health 2004, 94, 2081–2083. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, L.; Feighery, E.; Schleicher, N.; Haladjian, H.H.; Fortmann, S.P. Reaching youth at the point of sale: Cigarette marketing is more prevalent in stores where adolescents shop frequently. Tob. Control 2004, 13, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Donovan, R.; Jance, J.; Jones, S. Tobacco point of sale advertising increases positive brand user imagery. Tob. Control 2002, 11, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Schooler, C.; Feighery, E.; Flora, J. Seventh graders’ self-reported exposure to cigarette marketing and its relationship to their smoking behavior. Am. J. Public Health 1996, 86, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Lindblom, E.N.; Fleischer, N.; Thrasher, J.; Mohlman, M.K.; Zhang, Y.; Monshouwer, K.; Nagelhout, G.E. Public health effects of restricting retail tobacco product displays and ads. Tob. Regul. Sci. 2015, 1, 61–75. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tobacco Free Initiative (TFI): MPOWER. Available online: http://www.who.int/tobacco/mpower/en/ (accessed on 28 December 2015).
- U.S. Food and Drug Administration. Tobacco Products: Deeming Tobacco Products To Be Subject to the Federal Food, Drug, and Cosmetic Act. Available online: http://www.fda.gov/TobaccoProducts/GuidanceComplianceRegulatoryInformation/ucm394909.htm (accessed on 28 December 2015).
- Scheffels, J.; Lavik, R. Out of sight, out of mind? Removal of point-of-sale tobacco displays in Norway. Tob. Control 2013, 22, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.; Lewis, S.; Edwards, R.; McNeill, A. Economic evaluation of the removal of tobacco promotional displays in Ireland. Tob. Control 2011, 20, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Borland, R.; Fong, G.T.; Thrasher, J.F.; Hammond, D.; Cummings, K.M. Impact of point-of-sale tobacco display bans: Findings from the international tobacco control four country survey. Health Educ. Res. 2013, 28, 898–910. [Google Scholar] [CrossRef] [PubMed]
- McNeill, A.; Lewis, S.; Quinn, C.; Mulcahy, M.; Clancy, L.; Hastings, G.; Edwards, R. Evaluation of the removal of point-of-sale tobacco displays in Ireland. Tob. Control 2011, 20, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Huang, J.; Li, Q.; Chaloupka, F.J. The Association between point-of-sale advertising bans and youth experimental smoking: Findings from the Global Youth Tobacco Survey (GYTS). AIMS Public Health 2015. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Implementation of Article 13 of the WHO Framework Convention on Tobacco Control. Available online: http://www.who.int/fctc/guidelines/article_13.pdf (accessed on 28 December 2015).
- Gravely, S.; Fong, G.T.; Cummings, K.M.; Yan, M.; Quah, A.C.; Borland, R.; Yong, H.H.; Hitchman, S.C.; McNeill, A.; Hammond, D.; et al. Awareness, trial, and current use of electronic cigarettes in 10 countries: Findings from the ITC project. Int. J. Environ. Res. Public Health 2014, 11, 11691–11704. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.E. International Surveys: Motives and methodologies. Available online: http://www.statcan.gc.ca/pub/11-522-x/2008000/article/10937-eng.pdf (accessed on 28 December 2015).
- The Global Youth Tobacco Survey Collaborative Group. Tobacco use among youth: A cross country comparison. Tob. Control 2002, 11, 252–270. [Google Scholar]
- Carter, O.B.; Mills, B.W.; Donovan, R.J. The effect of retail cigarette pack displays on unplanned purchases: Results from immediate post purchase interviews. Tob. Control 2009, 18, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Clattenburg, E.J.; Elf, J.L.; Apelberg, B.J. Unplanned cigarette purchases and tobacco point of sale advertising: A potential barrier to smoking cessation. Tob. Control 2013, 22, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, M.; Germain, D.; Henriksen, L. The effect of retail cigarette pack displays on impulse purchase. Addiction 2008, 103, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Siahpush, M.; Shaikh, R.A.; Cummings, K.M.; Hyland, A.; Dodd, M.; Carlson, L.; Kessler, A.S.; Meza, J.; Wan, N.; Wakefield, M. The association of point-of-sale cigarette marketing with cravings to smoke: Results from a cross-sectional population-based study. Tob. Control 2015. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable Name | Description |
|---|---|
| Individual-level variables | |
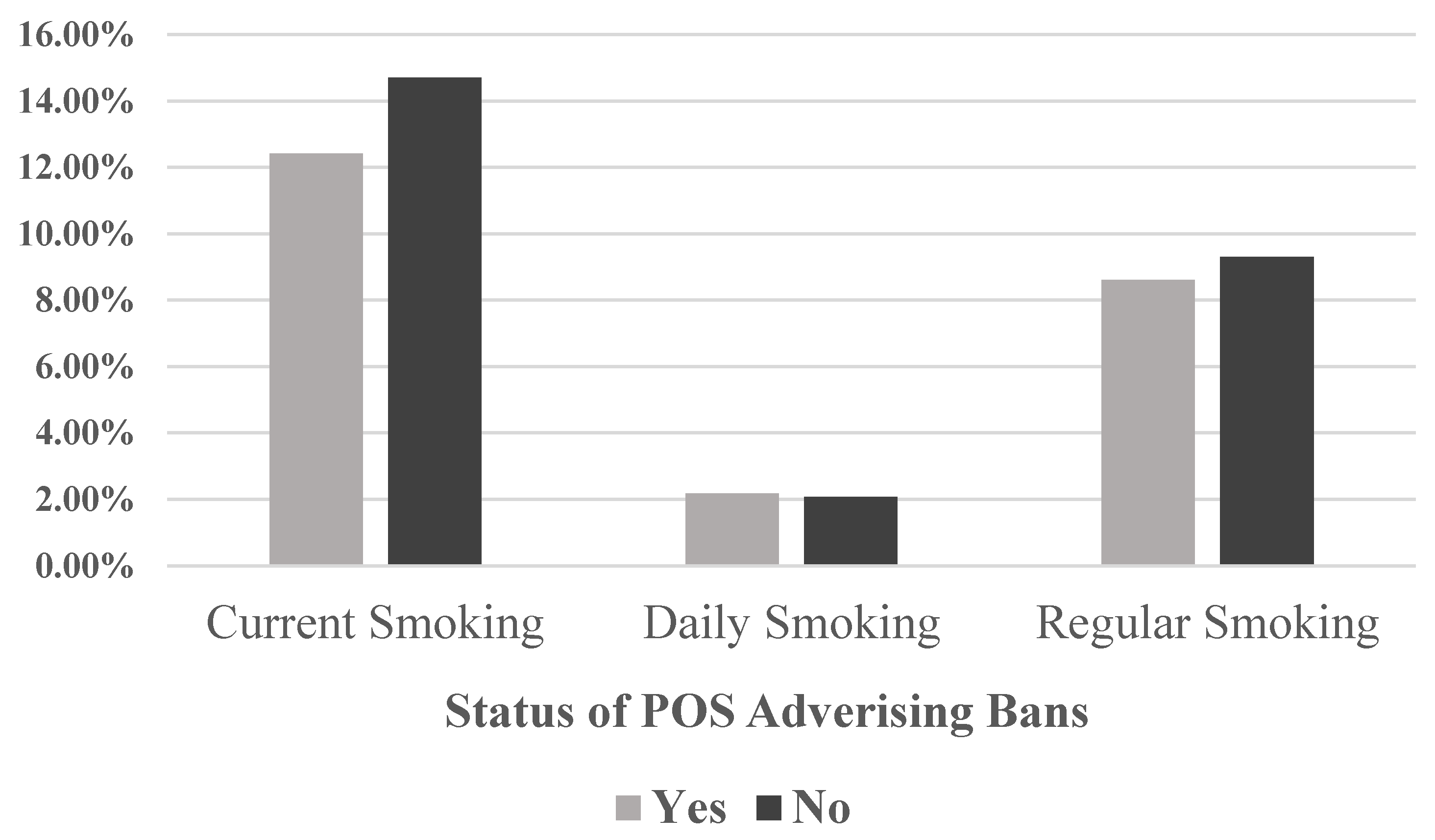
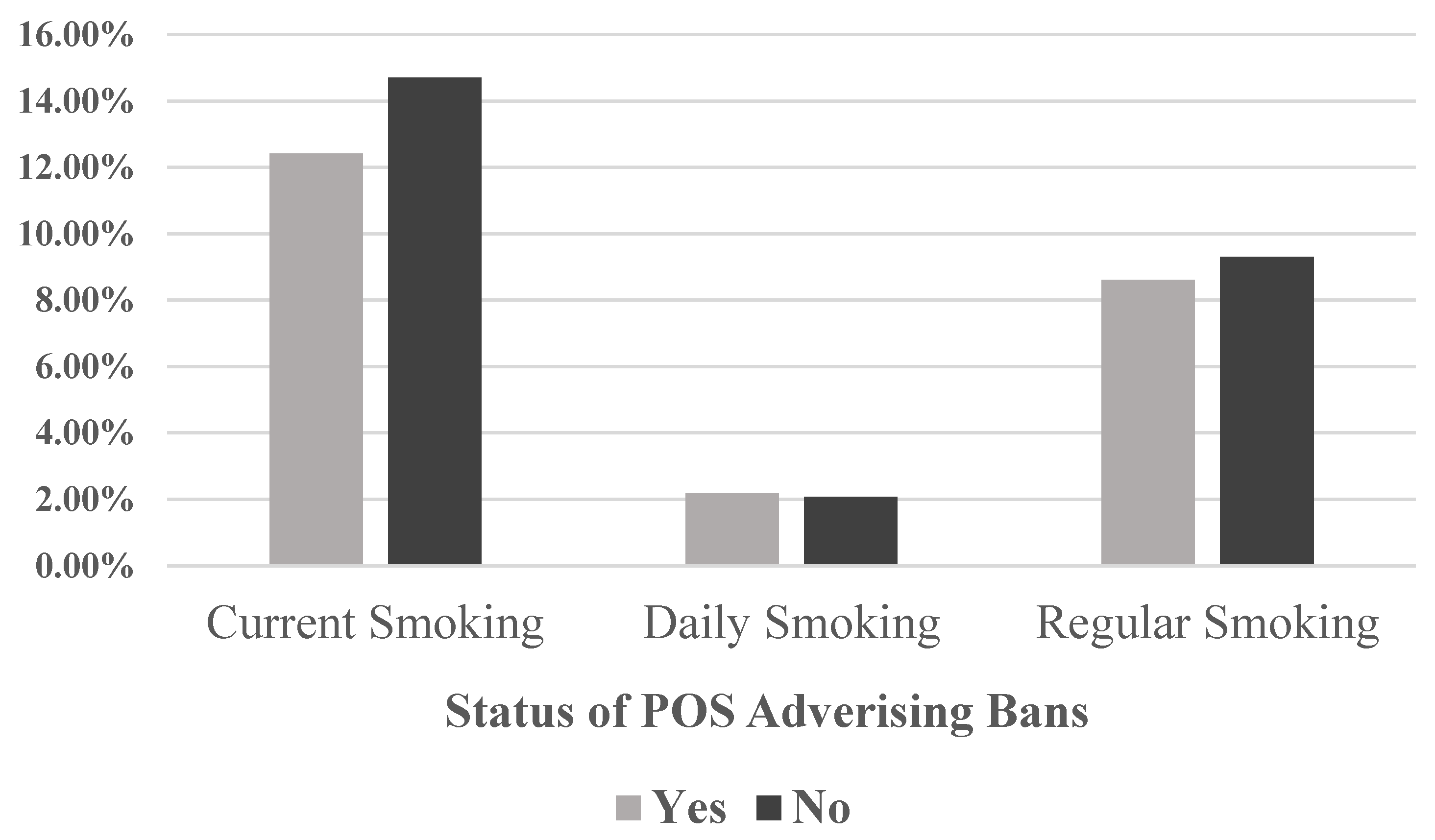
| Current smoking | Binary variable for smoking cigarettes in the past month. |
| Daily smoking | Binary variable for smoking cigarettes daily in the past month. |
| Regular smoking | Binary variable for smoking ≥1 cigarettes on days when they smoked in the past month. |
| Age dummies | Binary indicators for 8 age categories (≤11 years as old-referent) from age 12 to 16, and ≥17 |
| Parents’ smoking status | Binary indicator for 5 categories of parents’ smoking status (neither as referent), both, father only, mother only and missing/don’t know |
| Individual-Level | Mean | (95% C.I.) | Country-level | Mean | (95% C.I.) |
|---|---|---|---|---|---|
| Current Smoking | 0.142 | (0.122, 0.161) | POS ad ban | 0.240 | (0.145, 0.335) |
| Daily Smoking | 0.021 | (0.016, 0.026) | M score | 2.825 | (2.647, 3.002) |
| Regular Smoking | 0.091 | (0.078, 0.105) | M no data | 0.091 | (0.039, 0.143) |
| Age dummies | P score | 2.527 | (2.317, 2.737) | ||
| ≤11 | 0.061 | (0.037, 0.084) | P no data | 0.068 | (0.000,0.149) |
| 12 | 0.089 | (0.074, 0.105) | O score | 3.305 | (3.171, 3.438) |
| 13 | 0.187 | (0.163, 0.210) | W score | 2.674 | (2.424, 2.923) |
| 14 | 0.226 | (0.206, 0.246) | E score | 3.135 | (2.898, 3.372) |
| 15 | 0.204 | (0.185, 0.222) | R score | 3.380 | (3.193, 3.566) |
| 16 | 0.121 | (0.104, 0.138) | R no data | 0.017 | (0.000,0.038) |
| ≥17 | 0.070 | (0.047, 0.093) | GDP per capita | 4.709 | (3.621, 5.797) |
| Missing | 0.043 | (0.000,0.102) | -- | -- | -- |
| Parent smoking status | -- | -- | -- | ||
| Both | 0.070 | (0.056, 0.083) | -- | -- | -- |
| Father only | 0.252 | (0.219, 0.285) | -- | -- | -- |
| Mother only | 0.040 | (0.030, 0.050) | -- | -- | -- |
| Neither | 0.566 | (0.531, 0.601) | -- | -- | -- |
| Don’t know | 0.072 | (0.041, 0.104) | -- | -- | -- |
| Male | 0.494 | (0.487, 0.501) | -- | -- | -- |
| Variables | Current Smoking | Daily Smoking | Regular Smoking | |||
|---|---|---|---|---|---|---|
| AOR | (95% C.I.) | AOR | (95% C.I.) | AOR | (95% C.I.) | |
| POS ad ban | 0.727 * | (0.528, 1.003) | 0.699 * | (0.482, 1.014) | 0.749 ** | (0.562, 0.999) |
| Age Dummies | ||||||
| 12 | 1.160 | (0.559, 2.409) | 1.420 | (0.320, 6.294) | 1.178 | (0.456, 3.043) |
| 13 | 0.852 | (0.519, 1.398) | 0.591 | (0.265, 1.318) | 0.845 | (0.474, 1.505) |
| 14 | 1.104 | (0.693, 1.760) | 0.940 | (0.462, 1.913) | 1.188 | (0.694, 2.034) |
| 15 | 1.533 * | (0.969, 2.426) | 1.785 * | (0.929, 3.430) | 1.759 ** | (1.039, 2.977) |
| 16 | 2.074 *** | (1.318, 3.263) | 3.104 *** | (1.726, 5.580) | 2.471 *** | (1.487, 4.108) |
| 17 | 2.756 *** | (1.760, 4.316) | 5.121 *** | (2.761, 9.498) | 3.391 *** | (2.042, 5.632) |
| Missing | 1.005 | (0.424, 2.381) | 1.341 | (0.664, 2.707) | 1.231 | (0.557, 2.719) |
| Parents’ Smoking | ||||||
| Both | 3.346 *** | (2.882, 3.884) | 4.911 *** | (4.061, 5.939) | 3.497 *** | (3.025, 4.043) |
| Father only | 1.762 *** | (1.600, 1.940) | 1.969 *** | (1.746, 2.222) | 1.857 *** | (1.690, 2.039) |
| Mother only | 2.857 *** | (2.438, 3.347) | 3.814 *** | (3.182, 4.571) | 3.117 *** | (2.675, 3.631) |
| Don’t know | 1.839 *** | (1.405, 2.409) | 2.545 *** | (1.742, 3.719) | 2.054 *** | (1.532, 2.754) |
| Other Controls | ||||||
| Male | 1.683 *** | (1.406, 2.015) | 1.702 *** | (1.408, 2.058) | 1.684 *** | (1.410, 2.011) |
| M score | 0.957 | (0.806, 1.137) | 1.011 | (0.799, 1.278) | 0.961 | (0.814, 1.134) |
| M score missing | 0.709 * | (0.475, 1.058) | 0.555 * | (0.301, 1.025) | 0.605 ** | (0.403, 0.909) |
| P score | 1.058 | (0.923, 1.213) | 1.028 | (0.850, 1.243) | 1.055 | (0.911, 1.221) |
| P score missing | 0.985 | (0.555, 1.750) | 1.290 | (0.539, 3.086) | 1.072 | (0.566, 2.028) |
| O score | 0.992 | (0.762, 1.291) | 1.297 ** | (1.010, 1.665) | 1.137 | (0.932, 1.386) |
| W score | 1.066 | (0.855, 1.328) | 0.931 | (0.778, 1.113) | 0.979 | (0.851, 1.126) |
| E score | 1.019 | (0.885, 1.173) | 1.343 | (1.111, 1.624) | 1.093 | (0.954, 1.251) |
| R score | 1.450 *** | (1.269, 1.657) | 1.528 *** | (1.252, 1.865) | 1.473 *** | (1.284, 1.690) |
| R score missing | 4.366 *** | (1.917, 9.943) | 7.525 *** | (2.321,24.400) | 4.911 *** | (1.833,13.157) |
| GDP per Capita | 1.022 *** | (1.007, 1.037) | 1.037 *** | (1.019, 1.055) | 1.028 *** | (1.013, 1.043) |
| Variables | Current Smoking | Daily Smoking | Regular Smoking | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Prior | Later | Random | Prior | Later | Random | Prior | Later | Random | |
| Marginal Effect | −0.036 * | −0.040 * | −0.038 * | −0.007 * | −0.007 * | −0.007 * | −0.022 ** | −0.024 ** | −0.023 ** |
| (S.E.) | (0.019) | (0.020) | (0.019) | (0.004) | (0.004) | (0.004) | (0.011) | (0.011) | (0.011) |
| Elasticity | −0.273 * | −0.307 * | −0.286 * | −0.350 * | −0.340 * | −0.341 * | −0.262 ** | −0.279 ** | −0.266 ** |
| (S.E.) | (0.139) | (0.151) | (0.143) | (0.184) | (0.186) | (0.182) | (0.132) | (0.131) | (0.129) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shang, C.; Huang, J.; Cheng, K.-W.; Li, Q.; Chaloupka, F.J. Global Evidence on the Association between POS Advertising Bans and Youth Smoking Participation. Int. J. Environ. Res. Public Health 2016, 13, 306. https://doi.org/10.3390/ijerph13030306
Shang C, Huang J, Cheng K-W, Li Q, Chaloupka FJ. Global Evidence on the Association between POS Advertising Bans and Youth Smoking Participation. International Journal of Environmental Research and Public Health. 2016; 13(3):306. https://doi.org/10.3390/ijerph13030306
Chicago/Turabian StyleShang, Ce, Jidong Huang, Kai-Wen Cheng, Qing Li, and Frank J. Chaloupka. 2016. "Global Evidence on the Association between POS Advertising Bans and Youth Smoking Participation" International Journal of Environmental Research and Public Health 13, no. 3: 306. https://doi.org/10.3390/ijerph13030306
APA StyleShang, C., Huang, J., Cheng, K.-W., Li, Q., & Chaloupka, F. J. (2016). Global Evidence on the Association between POS Advertising Bans and Youth Smoking Participation. International Journal of Environmental Research and Public Health, 13(3), 306. https://doi.org/10.3390/ijerph13030306