
Indicated Prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of Case Management

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Procedures
2.1. Methods
2.2. Sample and Recruitment
2.3. Case Management Model
2.4. Data Collection and Analysis
3. Results and Discussion
3.1. Descriptive Statistics for the Sample

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Risk Variable | All Enrolled Women (N = 67) Mean (SD) | Women Who Completed CM (n = 51) Mean (SD) | Women Who Dropped out (n = 16) Mean (SD) | t | p ^ |
|---|---|---|---|---|---|
| Age (years) | 24.9 (5.4) | 24.8 (5.7) | 25.1 (5.2) | −0.174 | 0.862 |
| Gravidity | 2.6 (1.4) | 2.6 (1.4) | 2.4 (1.3) | 0.377 | 0.707 |
| Parity | 1.3 (1.1) | 1.3 (1.1) | 1.2 (1.0) | 0.276 | 0.783 |
| Height (cm) | 155.2 (6.9) | 155.8 (7.2) | 153.0 (5.7) | 1.427 | 0.158 |
| Weight (kg) | 57.7 (12.6) | 58.5 (13.5) | 55.1 (9.1) | 0.938 | 0.352 |
| Head circumference (cm) | 54.5 (2.3) | 54.8 (2.3) | 53.6 (2.2) | 1.847 | 0.069 |
| BMI | 23.7 (3.9) | 23.8 (4.1) | 23.5 (3.2) | 0.259 | 0.797 |
| Age of first drinking | 16.0 (2.2) | 16.1 (2.1) | 15.9 (2.7) | 0.285 | 0.776 |
| Number of years drinking regularly | 7.7 (4.6) | 7.6 (4.8) | 8.1 (4.0) | −0.424 | 0.673 |
| AUDIT score (baseline) | 18.9 (8.0) | 18.7 (8.1) | 19.6 (8.0) | −0.387 | 0.700 |
| All Enrolled Women (N = 67) % | Women Who Completed CM (n = 51) % | Women Who Dropped out (n = 16) % | χ2 | p ^ | |
|---|---|---|---|---|---|
| Paid work | 38.8 | 37.3 | 43.8 | 0.216 | 0.642 |
| Occupation | 52.2 | 45.1 | 75.0 | 5.288 | 0.259 |
| Farm worker | 10.4 | 13.7 | 0.0 | ||
| Factory worker | 10.4 | 11.8 | 6.3 | ||
| Housewife | 11.9 | 13.7 | 6.3 | ||
| Other occupation | 14.9 | 15.7 | 12.5 | ||
| Usually does not work | 52.2 | 45.1 | 75.0 | ||
| Usual employment status | |||||
| Full-time | 28.8 | 28.0 | 31.3 | 2.725 | 0.436 |
| Part-time | 6.1 | 8.0 | 0.0 | ||
| Seasonal | 10.6 | 8.0 | 18.8 | ||
| Unemployed | 54.5 | 56.0 | 50.0 | ||
| How stressful is life? | |||||
| Very or extremely | 49.3 | 47.1 | 56.3 | 1.868 | 0.393 |
| Somewhat or medium | 25.4 | 23.5 | 31.3 | ||
| Not at all | 25.4 | 29.4 | 12.5 | ||
| How many current friends drink alcohol? | |||||
| Most or all | 55.2 | 56.9 | 50.0 | 0.502 | 0.918 |
| Some or half | 28.4 | 27.5 | 31.3 | ||
| None | 7.5 | 7.8 | 6.3 | ||
| Has no friends | 9.0 | 7.8 | 12.5 | ||
| Frequency of church attendance | |||||
| Never or not very often | 59.4 | 60.4 | 56.3 | 0.086 | 0.769 |
| Often or very often | 40.6 | 39.6 | 43.8 |
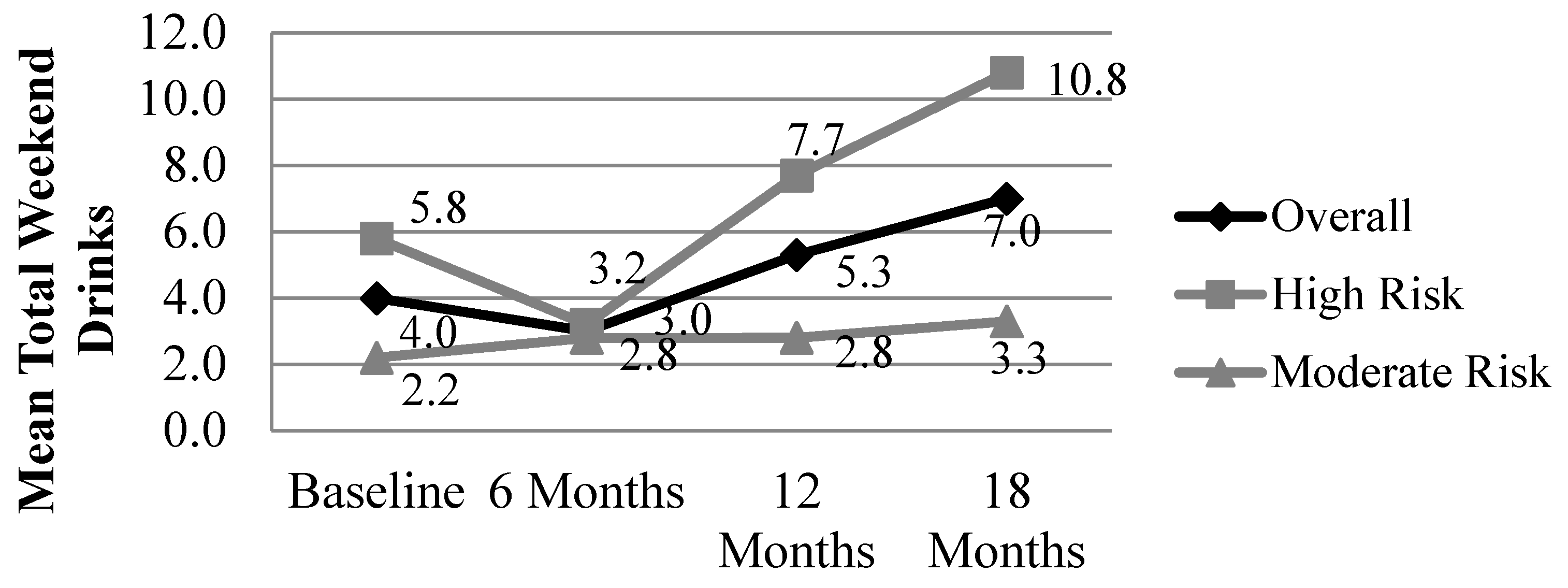
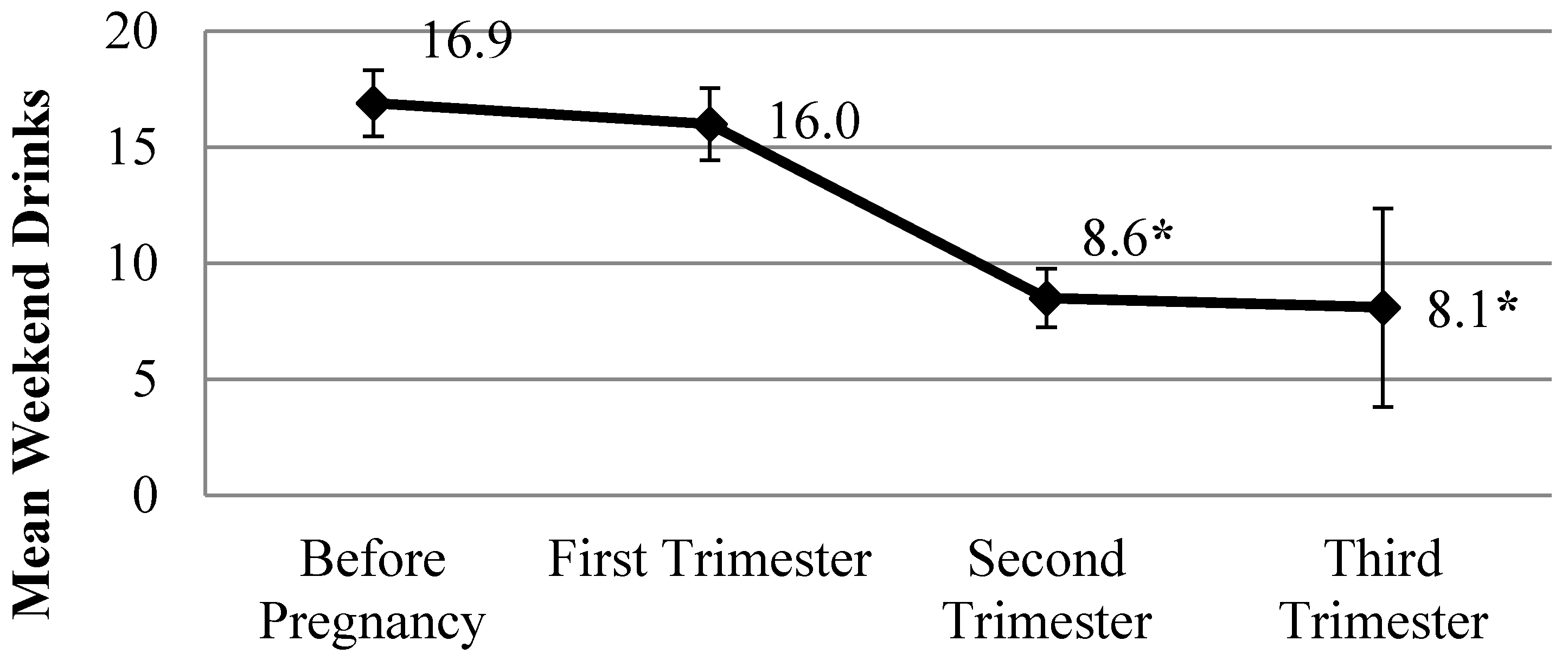
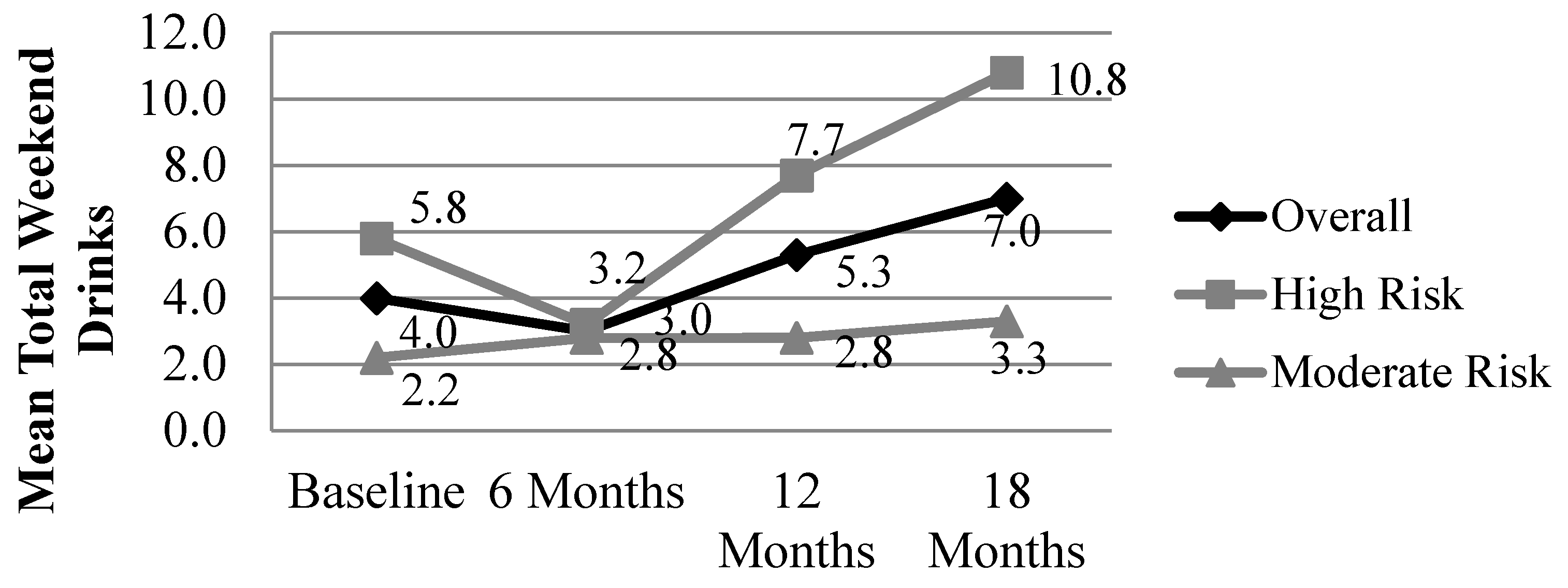
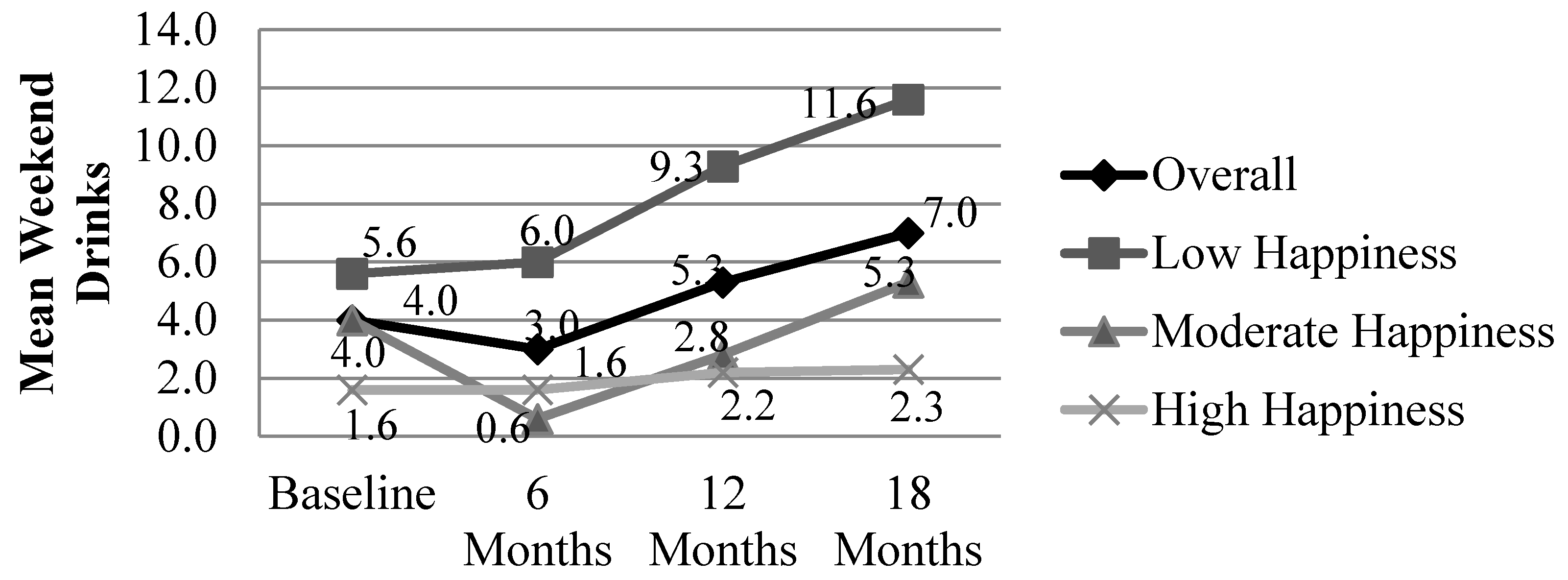
3.2. Drinking Outcomes


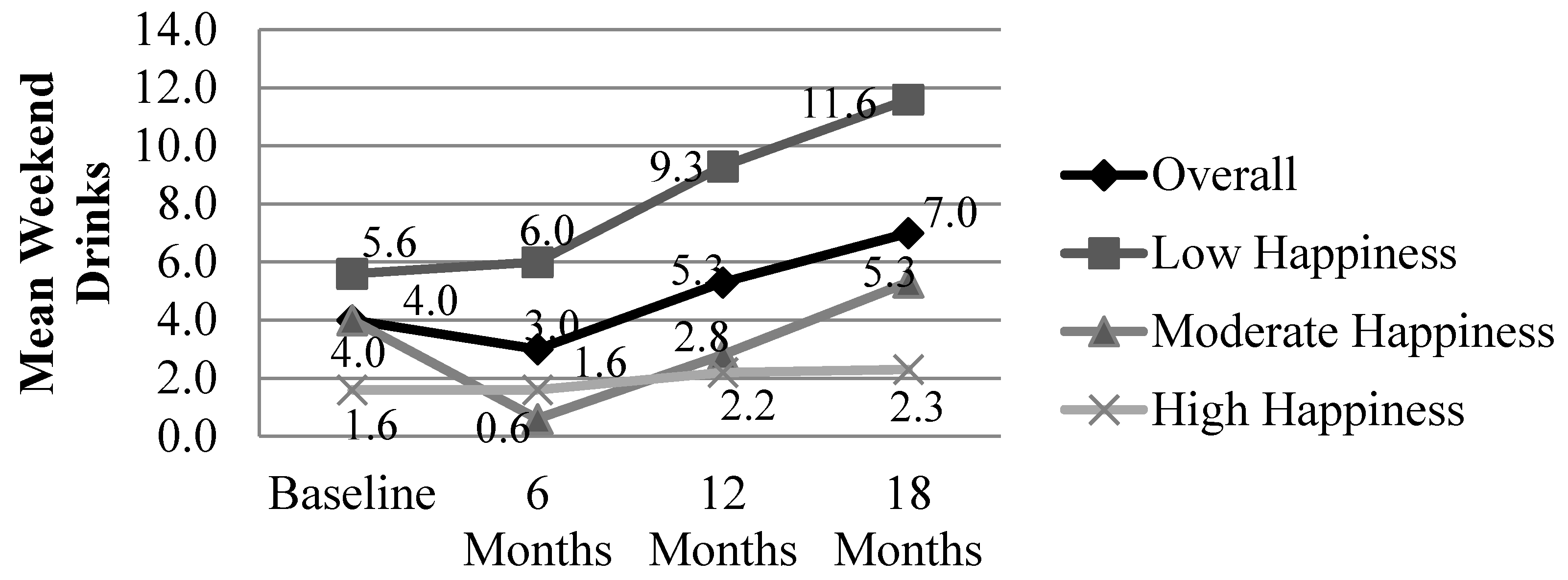
3.3. Happiness Outcomes

| Time Point | Friday Drinks R (p) | Saturday Drinks R (p) | Sunday Drinks R (p) |
|---|---|---|---|
| Baseline: Total happiness score | −0.242 (0.049) * | −0.369 (0.002) * | −0.154 (0.213) |
| 6 Month: Total happiness score | −0.335 (0.008) * | −0.446 (0.000) * | −0.130 (0.319) |
| 12 Month: Total happiness score | −0.477 (0.000) * | −0.453 (0.001) * | −0.336 (0.012) * |
| 18 Month: Total happiness score | −0.454 (0.001) * | −0.474 (0.001) * | −0.503 (0.000) * |
4. Discussion
4.1. Summary of Main Findings
4.2. Strengths and Limitations
4.3. Implications for Practice
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hoyme, H.E.; May, P.A.; Kalberg, W.O.; Kodituwakku, P.; Gossage, J.P.; Trujillo, P.M.; Buckley, D.; Miller, J.H.; Aragon, A.S.; Khaole, N.; et al. A practical clinical approach to diagnosis of fetal alcohol spectrum disorders: Clarification of the 1996 Institute of Medicine critera. Pediatrics 2005, 115, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Stratton, K.; Howe, C.; Battaglia, F.C. Fetal Alcohol Syndrome: Diagnosis, Epidemiology, Prevention, and Treatment; National Academy Press: Washington, DC, USA, 1996. [Google Scholar]
- May, P.A.; Tabachnick, B.G.; Gossage, J.P.; Kalberg, W.O.; Marais, A.S.; Robinson, L.K.; Manning, M.; Buckley, D.; Hoyme, H.E. Maternal risk factors predicting child physical characteristics and dysmorphology in fetal alcohol syndrome and partial fetal alcohol syndrome. Drug Alcohol Depend. 2011, 119, 18–27. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Hamrick, K.J.; Corbin, K.D.; Hasken, J.; Marais, A.S.; Brooke, L.E.; Blankenship, J.; Hoyme, H.E.; Gossage, J.P. Dietary intake, nutrition, and fetal alcohol spectrum disorders in the Western Cape Province of South Africa. Reprod. Toxicol. 2014, 46, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Surgeon Generalʼs advisory on alcohol and pregnancy. FDA Drug Bull. 1981, 11, 9–10. [Google Scholar]
- U.S. Surgeon General. Advisory on Alcohol Use in Pregnancy. Available online: http://www.cdc.gov/ncbddd/fasd/documents/surgeongenbookmark.pdf (accessed on 21 October 2015).
- May, P.A.; Blankenship, J.; Marais, A.S.; Gossage, J.P.; Kalberg, W.O.; Barnard, R.; de Vries, M.; Robinson, L.K.; Adnams, C.M.; Buckley, D.; et al. Approaching the prevalence of the full spectrum of fetal alcohol spectrum disorders in a South African population-based study. Alcohol. Clin. Exp. Res. 2013, 37, 818–830. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Blankenship, J.; Marais, A.S.; Gossage, J.P.; Kalberg, W.O.; Joubert, B.; Cloete, M.; Barnard, R.; de Vries, M.; Hasken, J.; et al. Maternal alcohol consumption producing fetal alcohol spectrum disorders (FASD): Quantity, frequency, and timing of drinking. Drug Alcohol Depend. 2013, 133, 502–512. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Gossage, J.P.; Brooke, L.E.; Snell, C.L.; Marais, A.S.; Hendricks, L.S.; Croxford, J.A.; Viljoen, D.L. Maternal risk factors for fetal alcohol syndrome in the Western Cape Province of South Africa: A population-based study. Am. J. Public Health 2005, 95, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Gossage, J.P.; Marais, A.S.; Hendricks, L.S.; Snell, C.; Tabachnick, B.G.; Stellavato, C.; Buckley, D.; Brooke, L.E.; Viljoen, D.L. Maternal risk factors for fetal alcohol syndrome and partial fetal alcohol syndrome in South Africa: A third study. Alcohol. Clin. Exp. Res. 2008, 32, 738–753. [Google Scholar] [CrossRef] [PubMed]
- Viljoen, D.L.; Croxford, J.; Gossage, J.P.; May, P.A. Characteristics of mothers of children with fetal alcohol syndrome in the Western Cape Province of South Africa: A case-control study. J. Stud. Alcohol 2002, 63, 6–17. [Google Scholar] [PubMed]
- May, P.A.; Marais, A.S.; Gossage, J.P.; Barnard, R.; Joubert, B.; Cloete, M.; Hendricks, N.; Roux, S.; Blom, A.; Steenekamp, J.; et al. Case management reduces drinking during pregnancy among high-risk women. Int. J. Alcohol Drug Res. 2013, 2, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Bull, L.B.; Kvigne, V.L.; Leonardson, G.R.; Lacina, L.; Welty, T.K. Validation of a self-administered questionnaire to screen for prenatal alcohol use in Northern Plains Indian women. Am. J. Prev. Med. 1999, 16, 240–243. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Rapp, R.C.; van den Noortgate, W.; Wanderplasschen, W. The efficacy of case management with persons who have substance abuse problems: A three-level meta-analysis of outcomes. J. Consult. Clin. Psychol. 2014, 82, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Uten, L.M.; Jones, H.E.; Schaeffer, C.M.; Stiter, M.L. The role of case management in substance abuse treatment. In Reinforcment-Based Treatment for Substance Use Disorders: A Comprehensive Behavioral Approach; American Psychological Association: Washington, DC, USA, 2012; pp. 121–144. [Google Scholar]
- Vanderplasschen, W.; Wolf, J.; Rapp, R.C.; Broekaert, E. Effectiveness of different models of case management for substance abusing popuations. J. Psychoact. Drugs 2007, 39, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Motivational Interviewing, 2nd ed.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Miller, W.R.; Rollnick, S. Motivational Interviewing; Guilford Press: New York, NY, USA, 1991. [Google Scholar]
- Meyers, R.J.; Roozen, H.G.; Smith, J.E. The community reinforcement approach: An update of the evidence. Alcohol Res. Health 2011, 33, 380–388. [Google Scholar] [PubMed]
- Meyers, R.J.; Smith, J.E. Clinical Guide to Alcohol Treatment: The Community Reinforcement Approach; Guilford Press: New York, NY, USA, 1995. [Google Scholar]
- Hartman, A. Diagrammatic assessment of family relationships. Fam. Soc. 1995, 76, 111–122. [Google Scholar]
- IBM Corp: IBM SPSS Statistics for Windows, 22.0 ed.; IBM Corp: Armonk, NY, USA, 2013.
- Choi, K.W.; Watt, M.H.; MacFarlane, J.C.; Sikkema, K.J.; Skinner, D.; Peterse, D.; Kalichman, S.C. Drinking in the context of life stressors: A multidimensional coping strategy among South African women. Subst. Use Misuse 2014, 49, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Watt, M.H.; Eaton, L.A.; Choi, K.W.; Velloza, J.; Kalichman, S.C.; Skinner, D.; Sikkema, K.J. “Itʼs better for me to drink, at least the stress is going away”: Perspectives on alcohol use during pregnancy among South African women attending drinking establishments. Soc. Sci. Med. 2014, 116, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Thanh, N.X.; Jonsson, E.; Moffatt, J.; Dennett, L.; Chuck, A.W.; Birchard, S. An economic evaluation of the parent-child assistance program for preventing fetal alcohol spectrum disorder in Alberta, Canada. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 10–18. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vries, M.M.; Joubert, B.; Cloete, M.; Roux, S.; Baca, B.A.; Hasken, J.M.; Barnard, R.; Buckley, D.; Kalberg, W.O.; Snell, C.L.; et al. Indicated Prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of Case Management. Int. J. Environ. Res. Public Health 2016, 13, 76. https://doi.org/10.3390/ijerph13010076
De Vries MM, Joubert B, Cloete M, Roux S, Baca BA, Hasken JM, Barnard R, Buckley D, Kalberg WO, Snell CL, et al. Indicated Prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of Case Management. International Journal of Environmental Research and Public Health. 2016; 13(1):76. https://doi.org/10.3390/ijerph13010076
Chicago/Turabian StyleDe Vries, Marlene M., Belinda Joubert, Marise Cloete, Sumien Roux, Beth A. Baca, Julie M. Hasken, Ronel Barnard, David Buckley, Wendy O. Kalberg, Cudore L. Snell, and et al. 2016. "Indicated Prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of Case Management" International Journal of Environmental Research and Public Health 13, no. 1: 76. https://doi.org/10.3390/ijerph13010076
APA StyleDe Vries, M. M., Joubert, B., Cloete, M., Roux, S., Baca, B. A., Hasken, J. M., Barnard, R., Buckley, D., Kalberg, W. O., Snell, C. L., Marais, A.-S., Seedat, S., Parry, C. D. H., & May, P. A. (2016). Indicated Prevention of Fetal Alcohol Spectrum Disorders in South Africa: Effectiveness of Case Management. International Journal of Environmental Research and Public Health, 13(1), 76. https://doi.org/10.3390/ijerph13010076