
Chronic Arsenic Poisoning Probably Caused by Arsenic-Based Pesticides: Findings from an Investigation Study of a Household

Abstract
:1. Introduction
2. Materials and Methods
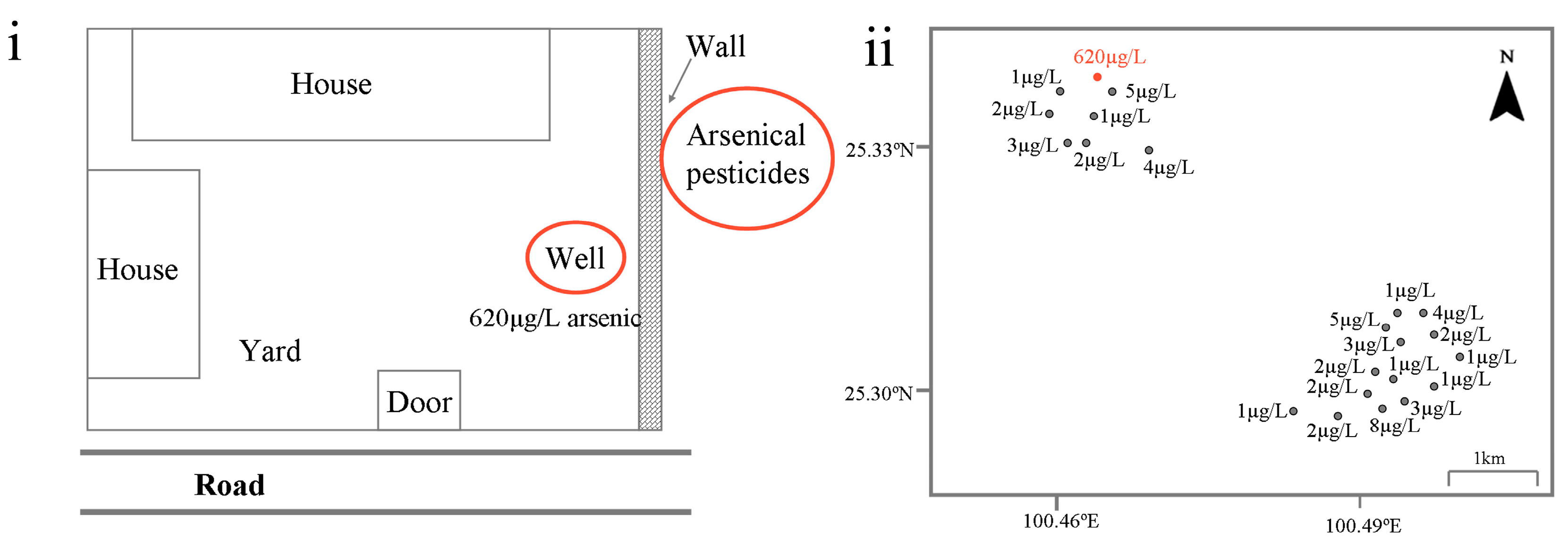
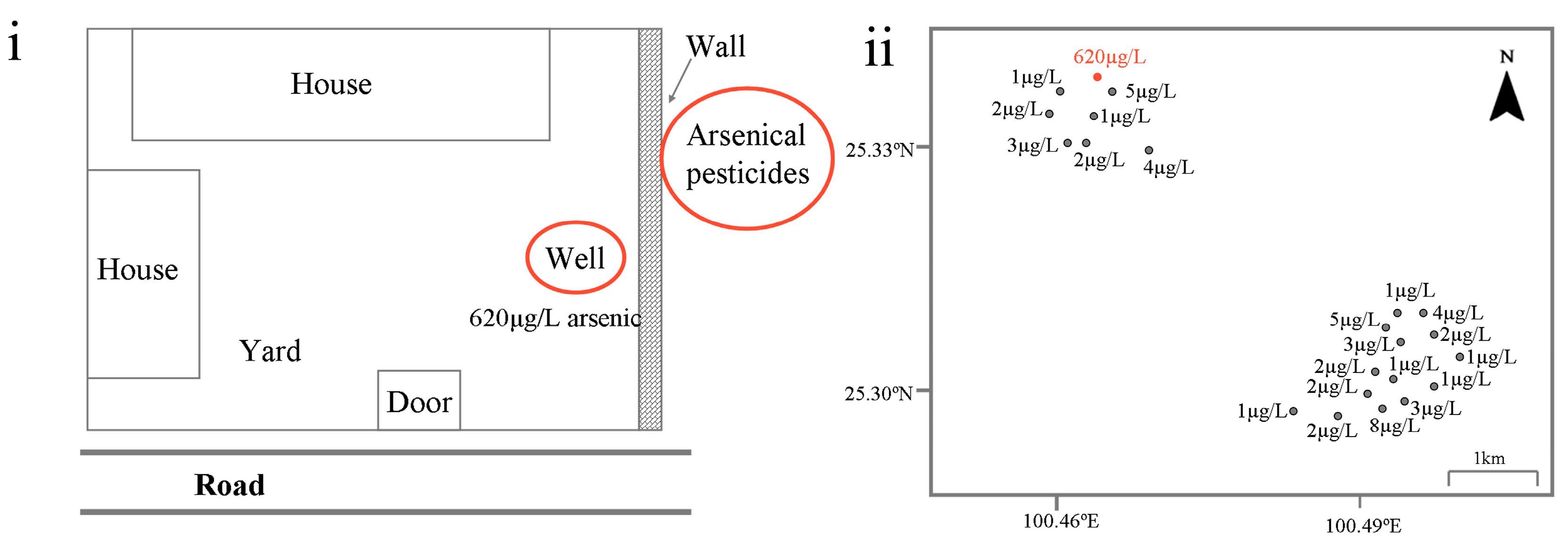
2.1. Background
2.2. Investigation
2.2.1. Urinary Arsenic Speciation Measurement
2.2.2. Biochemical Analysis
2.3. Statistical Analysis
2.4. Ethical Statements
3. Results
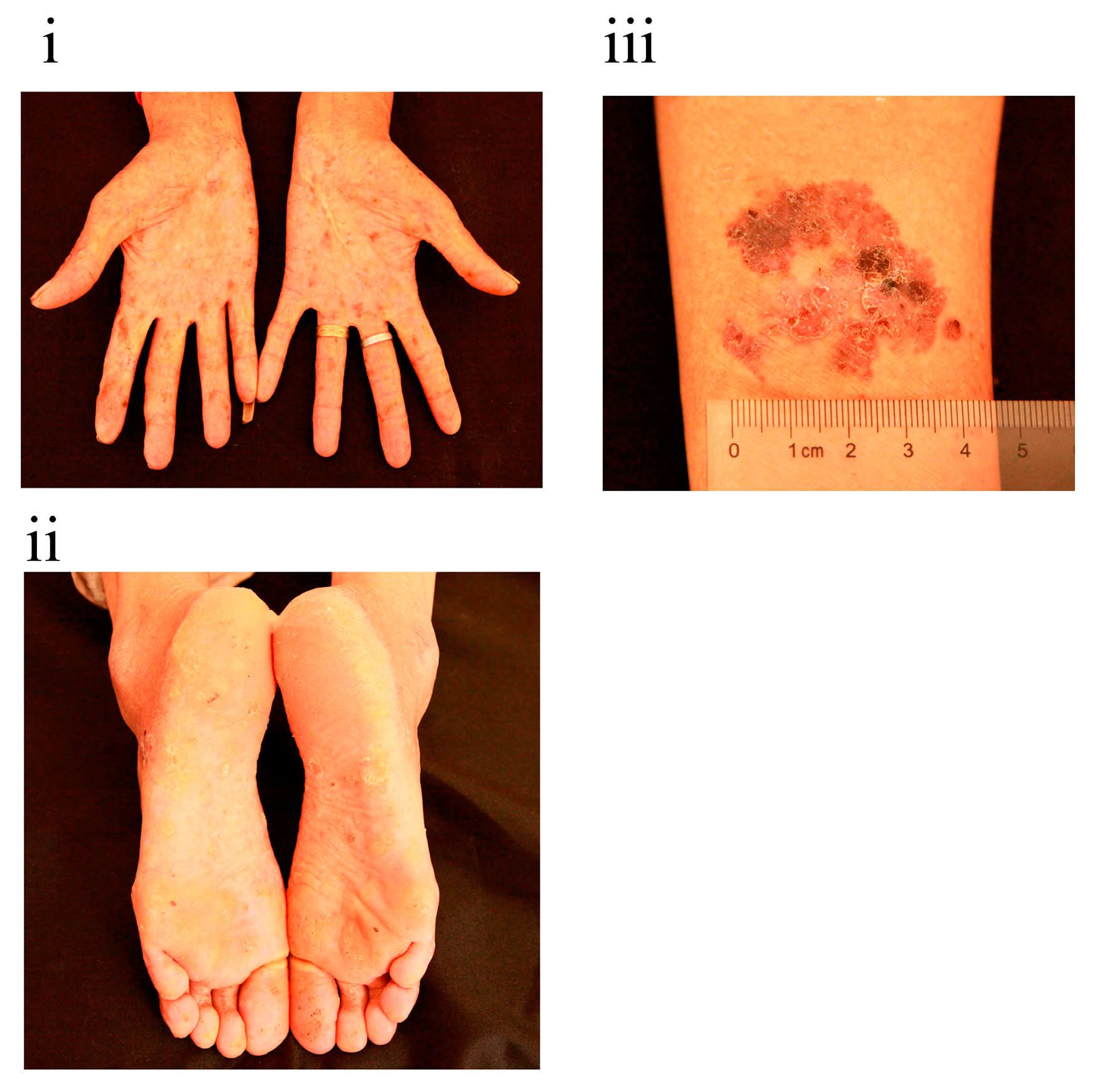
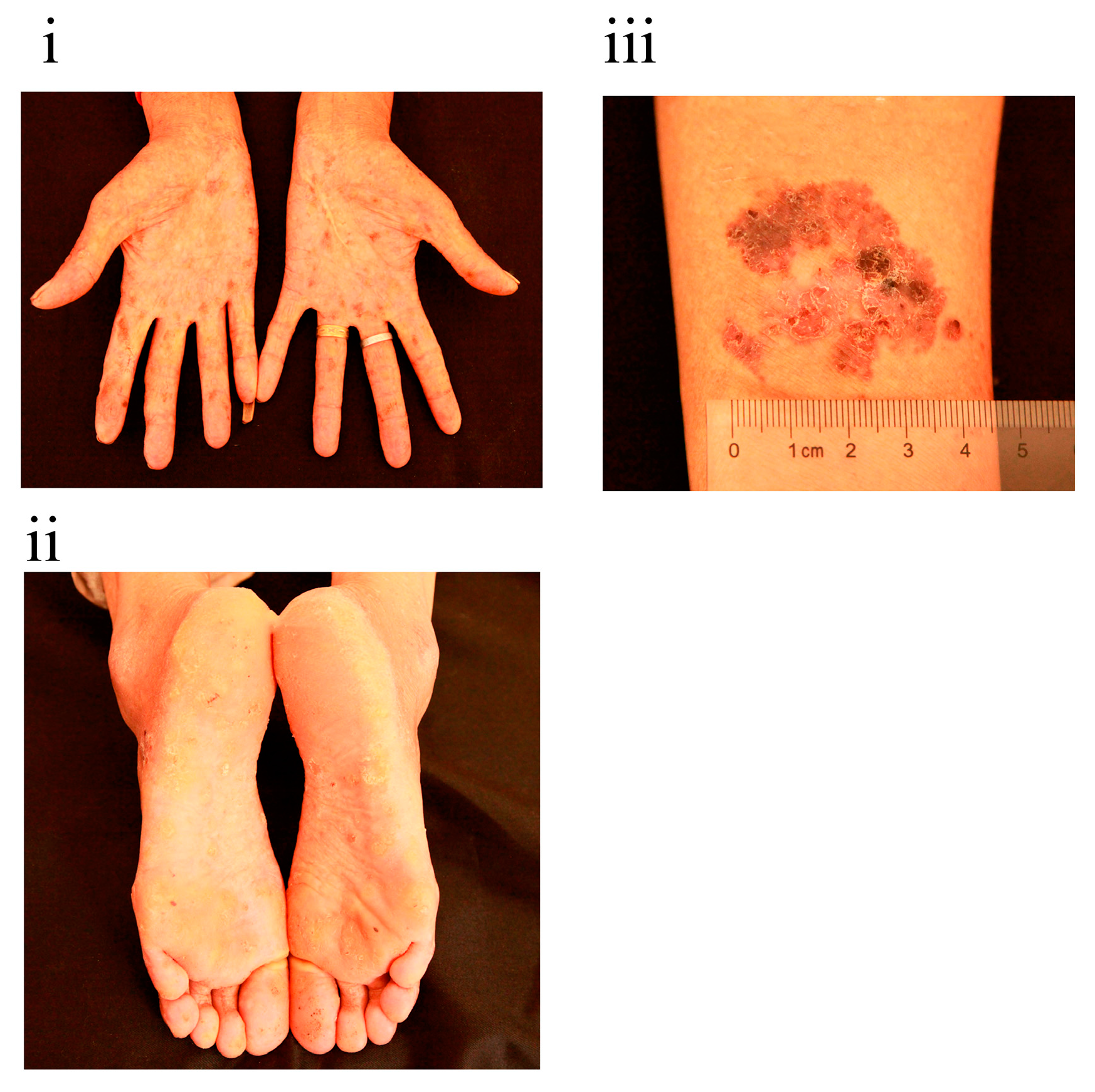
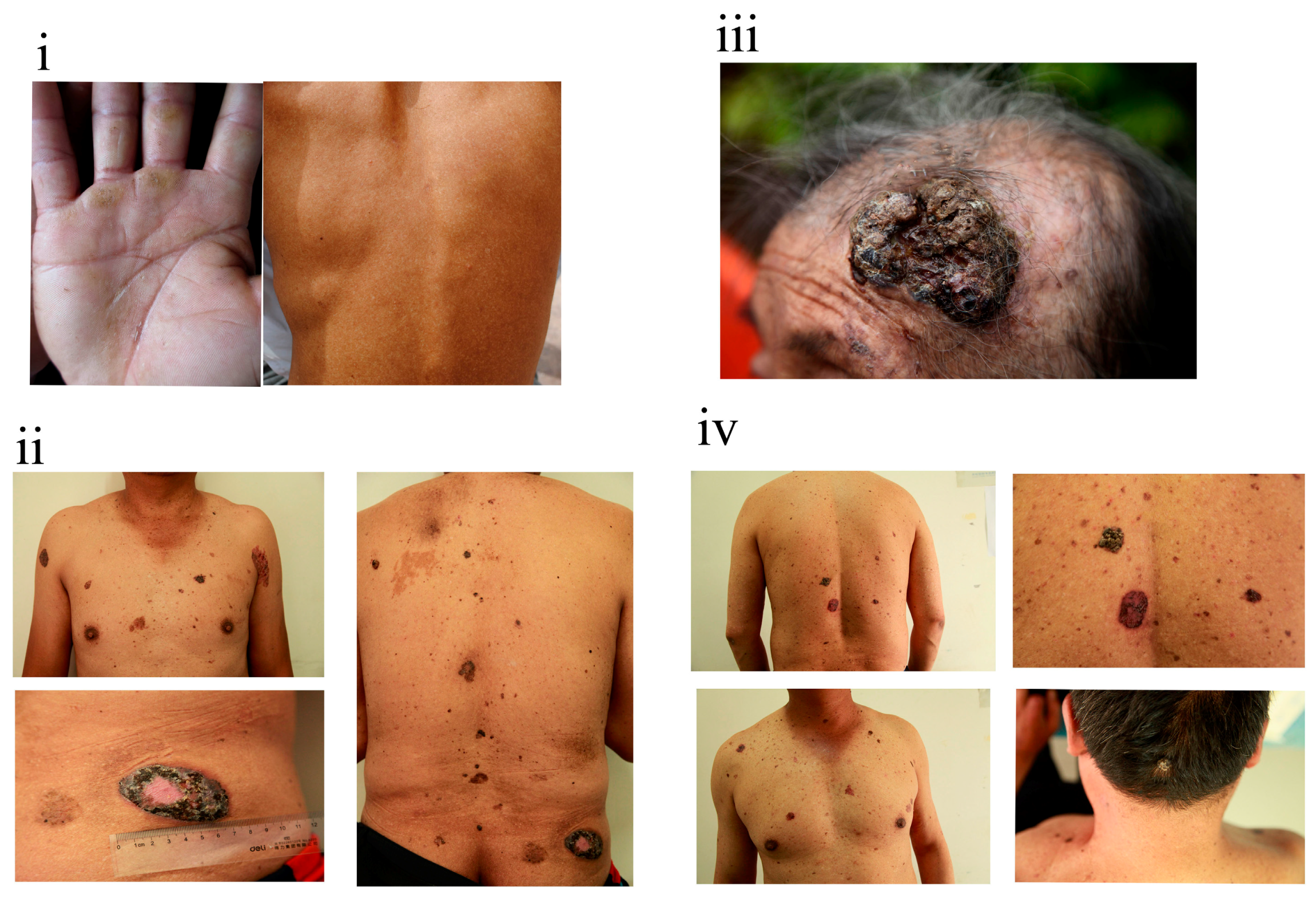
3.1. Chronic Arsenic Poisoning Diagnosed in the Household

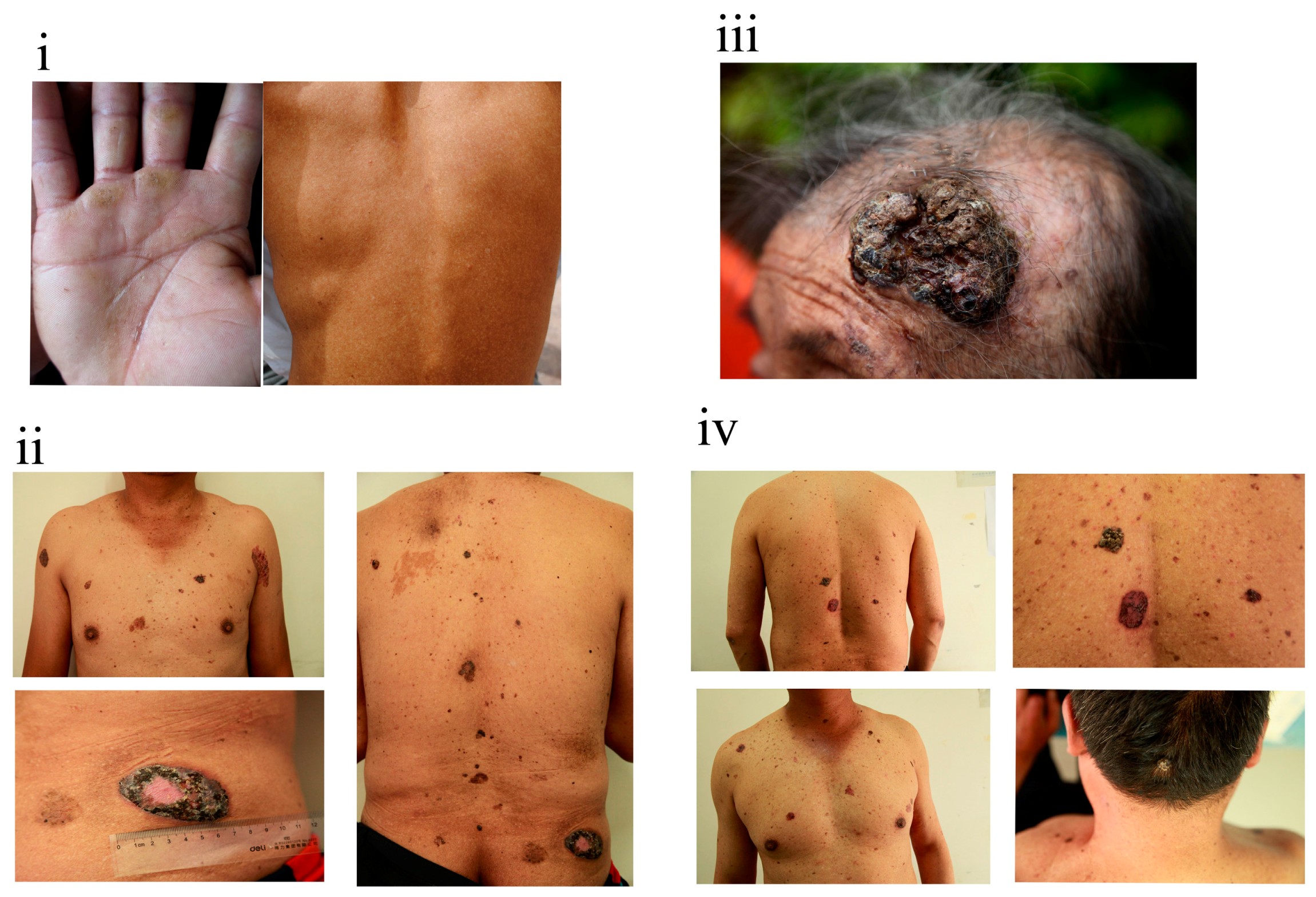
3.2. Persistent Health Influence

{kind=link}
{kind=link}
{kind=link}
{kind=link}
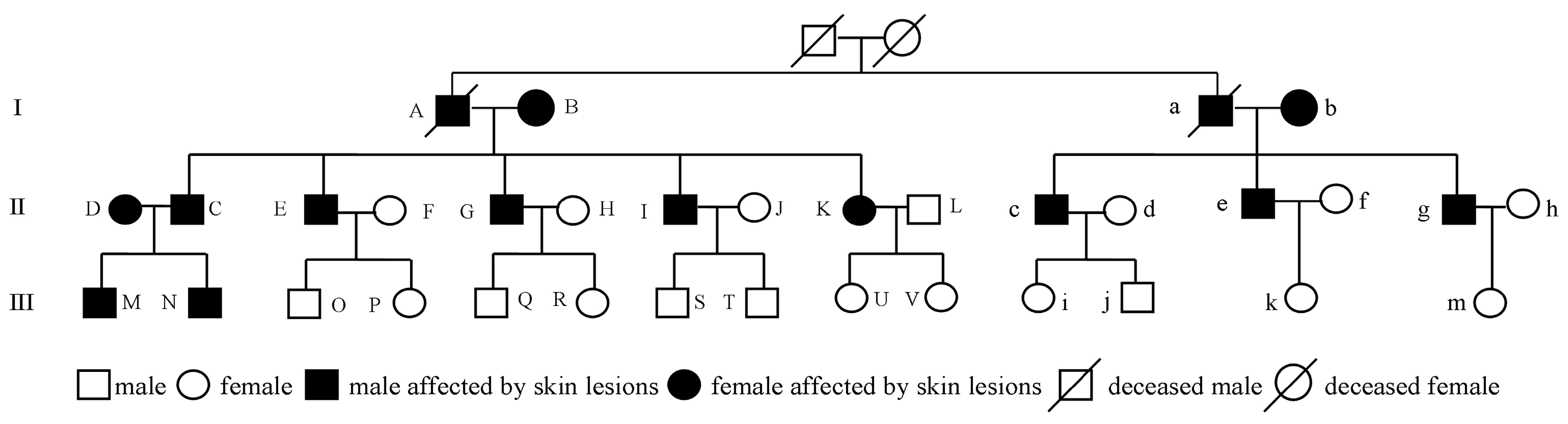
| Variables | Number | Birth Year # | Skin Symptoms | Exposure Duration | Grade † | Pathological Examination |
|---|---|---|---|---|---|---|
| Generation I | A * | 1936 | Yes | 1973–1989 (16) | NA | NA |
| B | 1935 (NA) | Yes | 1973–1989 (16) § | Advanced | Bowen’s disease | |
| a * | 1941 | Yes | 1973–1989 (16) | NA | NA | |
| b | 1945 (1963) | Yes | 1973–1989 (16) | Advanced | Basal cell carcinoma | |
| Generation II | C | 1956 | Yes | 1973–1989 (16) | Advanced | Basal cell carcinoma |
| D | 1958 (1980) | Yes | 1980–1989 (9) | Mild | NA | |
| E | 1963 | Yes | 1973–1989 (16) | Advanced | Basal cell carcinoma | |
| F | 1965 (1990) | No | Non-exposed | |||
| G | 1966 | Yes | 1973–1989 (16) | Advanced | Basal cell carcinoma/Bowen’s disease | |
| H | 1969 (1991) | No | Non-exposed | |||
| I | 1972 | Yes | 1973–1989 (16) | Advanced | Basal cell carcinoma/Bowen’s disease | |
| J | 1976 (1996) | No | Non-exposed | |||
| K | 1970 | Yes | 1973–1989 (16) | Advanced | Bowen’s disease | |
| L $ | NA | No | Non-exposed | |||
| c | 1965 | Yes | 1973–1989 (16) | Advanced | Bowen’s disease | |
| d | 1970 (1989) | No | Non-exposed | |||
| e | 1970 | Yes | 1973–1989 (16) | Advanced | NA | |
| f | 1974 (1997) | No | Non-exposed | |||
| g | 1973 | Yes | 1973–1989 (16) | Advanced | Hyperkeratosis | |
| h | 1976 (2000) | No | Non-exposed | |||
| Generation III | M & | 1981 | Yes | 1981–1989 (8) | NA | NA |
| N | 1983 | Yes | 1983–1989 (6) | Mild | NA | |
| O | 1993 | No | Non-exposed | |||
| P | 1997 | No | Non-exposed | |||
| Q & | NA | No | Non-exposed § | |||
| R & | NA | No | Non-exposed § | |||
| S | 1998 | No | Non-exposed | |||
| T | 2004 | No | Non-exposed | |||
| U | 1996 | No | Non-exposed | |||
| V | 2001 | No | Non-exposed | |||
| i | 1990 | No | Non-exposed | |||
| j & | NA | No | Non-exposed § | |||
| k | 1998 | No | Non-exposed | |||
| m | 2004 | No | Non-exposed |
| Biochemical Variables | Overall (n = 25) | Individuals Exposed to Arsenic (n = 12) | Individuals Unexposed to Arsenic (n = 13) | p-Value |
|---|---|---|---|---|
| ALT (U/L) | 22.0 (16.0, 30.0) | 27.5 (17.0, 30.8) | 18.0 (13.0, 26.0) | 0.185 |
| AST (U/L) | 34.0 (31.0, 38.0) | 37.5 (33.0, 42.5) | 31.0 (29.0, 34.0) | 0.006 |
| γ-GT (U/L) | 14.0 (11.0, 34.0) | 25.5 (13.3, 77.0) | 12.0 (9.0, 19.0) | 0.021 |
| Creatinine (mg/dL) | 102.0 (77.1, 163.1) | 156.5 (108.7, 167.0) | 77.4 (62.9, 127.7) | 0.012 |
| UA (μmol/L) | 286.0 (201.0, 395.0) | 353.5 (249.5, 396.5) | 237.0 (183.0, 286.0) | 0.074 |
| Glu (mmol/L) | 4.1 (3.8, 4.5) | 4.1 (3.8, 4.7) | 4.1 (3.6, 4.4) | 0.518 |
| HbA1c (%) | 5.8 (5.7, 6.1) | 6.1 (5.7, 6.1) | 5.8 (5.5, 6.0) | 0.245 |
| TG (mmol/L) | 1.5 (1.0, 1.6) | 1.4 (1.0, 1.6) | 1.5 (1.0, 1.8) | 0.667 |
| TC (mmol/L) | 4.2 (3.9, 4.8) | 4.2 (3.8, 5.6) | 4.2 (4.0, 4.7) | 0.580 |
| HDL-C (mmol/L) | 1.3 (1.2, 1.5) | 1.4 (1.2, 1.5) | 1.3 (1.2, 1.5) | 0.599 |
| LDL-C (mmol/L) | 1.8 (1.6, 2.4) | 1.7 (1.6, 2.9) | 1.9 (1.6, 2.1) | 0.902 |
| Hcy (μmol/L) | 14.0 (13.4, 16.8) | 15.2 (13.7, 17.7) | 13.7 (12.6, 16.2) | 0.166 |
| Variables | Individuals Exposed to Arsenic (n = 12) | Individuals Unexposed to Arsenic (n = 13) | p-Value |
|---|---|---|---|
| AST (U/L) | 0.039 | ||
| >40 | 4 (33.3) | 0 (0.0) | |
| ≤40 | 8 (66.7) | 13 (100.0) | |
| γ-GT (U/L) | 0.039 | ||
| >50 | 4 (33.3) | 0 (0.0) | |
| ≤50 | 8 (66.7) | 13 (100.0) | |
| UA (μmol/L) | 0.593 | ||
| HUA b | 2 (16.7) | 1 (7.7) | |
| Normal | 10 (83.3) | 12 (92.3) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- IARC. Some drinking water disinfectants and contaminants, including arsenic. In Monographs on the Evaluation of Carcinogenic Risk to Humans; IARC Monographs, IARC: Lyon, France, 2004; Volume 84. [Google Scholar]
- Argos, M.; Kalra, T.; Pierce, B.L.; Chen, Y.; Parvez, F.; Islam, T.; Ahmed, A.; Hasan, R.; Hasan, K.; Sarwar, G.; et al. A prospective study of arsenic exposure from drinking water and incidence of skin lesions in Bangladesh. Am. J. Epidemiol. 2011, 174, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wu, F.; Liu, M.; Parvez, F.; Slavkovich, V.; Eunus, M.; Ahmed, A.; Argos, M.; Islam, T.; Rakibuz-Zaman, M.; et al. A prospective study of arsenic exposure, arsenic methylation capacity, and risk of cardiovascular disease in Bangladesh. Environ. Health Perspect. 2013, 121, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, J.S.; Perez, V.; Garry, M.R.; Alexander, D.D. Association of low-level arsenic exposure in drinking water with cardiovascular disease: A systematic review and risk assessment. Toxicology 2014, 323, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xie, Z.; Lin, Y.; Zhang, D. Association of inorganic arsenic exposure with type 2 diabetes mellitus: A meta-analysis. J. Epidemiol. Community Health 2014, 68, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Rudnai, T.; Sandor, J.; Kadar, M.; Borsanyi, M.; Beres, J.; Metneki, J.; Maraczi, G.; Rudnai, P. Arsenic in drinking water and congenital heart anomalies in Hungary. Int. J. Hyg. Environ. Health 2014, 217, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Quansah, R.; Armah, F.A.; Essumang, D.K.; Luginaah, I.; Clarke, E.; Marfoh, K.; Cobbina, S.J.; Nketiah-Amponsah, E.; Namujju, P.B.; Obiri, S.; et al. Association of arsenic with adverse pregnancy outcomes/infant mortality: A systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Hamadani, J.D.; Tofail, F.; Nermell, B.; Gardner, R.; Shiraji, S.; Bottai, M.; Arifeen, S.E.; Huda, S.N.; Vahter, M. Critical windows of exposure for arsenic-associated impairment of cognitive function in pre-school girls and boys: A population-based cohort study. Int. J. Epidemiol. 2011, 40, 1593–1604. [Google Scholar] [PubMed]
- Camm, G.S.; Glass, H.J.; Bryce, D.W.; Butcher, A.R. Characterisation of a mining-related arsenic-contaminated site, Cornwall, UK. J. Geochem. Explor. 2004, 82, 1–15. [Google Scholar]
- Lagerkvist, B.J.; Zetterlund, B. Assessment of exposure to arsenic among smelter workers: A five-year follow-up. Am. J. Ind. Med. 1994, 25, 477–488. [Google Scholar] [PubMed]
- Park, D.; Yang, H.; Jeong, J.; Ha, K.; Choi, S.; Kim, C.; Yoon, C.; Paek, D. A comprehensive review of arsenic levels in the semiconductor manufacturing industry. Ann. Occup. Hyg. 2010, 54, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Kumaresan, M.; Riyazuddin, P. Overview of speciation chemistry of arsenic. Curr. Sci. India 2001, 80, 837–846. [Google Scholar]
- Murphy, E.A.; Aucott, M. An assessment of the amounts of arsenical pesticide used historically in a geographic area. Sci. Total Environ. 1998, 218, 89–101. [Google Scholar] [CrossRef]
- Datta, R.; Sarkar, D. Consideration of soil properties in assessment of human health risk from exposure to arsenic-enriched soils. Integr. Environ. Assess. Manag. 2005, 1, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Quazi, S.; Sarkar, D.; Datta, R. Human health risk from arsenical pesticide contaminated soils: A long-term greenhouse study. J. Hazard. Mater. 2013, 262, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Feinglass, E.J. Arsenic intoxication from well water in the United States. N. Engl. J. Med. 1973, 288, 828–830. [Google Scholar] [PubMed]
- Armstrong, C.W.; Stroube, R.B.; Rubio, T.; Siudyla, E.A.; Miller, G.B., Jr. Outbreak of fatal arsenic poisoning caused by contaminated drinking water. Arch. Environ. Health 1984, 39, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, D.; Li, X.; Zheng, Q.; Sun, G. A potential synergy between incomplete arsenic methylation capacity and demographic characteristics on the risk of hypertension: Findings from a cross-sectional study in an arsenic-endemic area of inner Mongolia, China. Int. J. Environ. Res. Public Health 2015, 12, 3615–3632. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Xu, Y.; Li, X.; Jin, Y.; Li, B.; Sun, X. Urinary arsenic metabolites in children and adults exposed to arsenic in drinking water in Inner Mongolia, China. Environ. Health Perspect. 2007, 115, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, Y.; Zheng, Q.; Li, X.; Li, B.; Jin, Y.; Sun, X.; Sun, G. Association of oxidative stress with arsenic methylation in chronic arsenic-exposed children and adults. Toxicol. Appl. Pharmacol. 2008, 232, 142–149. [Google Scholar] [CrossRef] [PubMed]
- ATSDR (Agency for Toxic Substances and Disease Registry). ToxGuide™ for Arsenic. Available online: http://www.atsdr.cdc.gov/toxguides/toxguide-2.pdf (accessed on 1 June 2015).
- Smedley, P.L.; Kinniburgh, D.G. A review of the source, behaviour and distribution of arsenic in natural waters. Appl. Geochem. 2002, 17, 517–568. [Google Scholar] [CrossRef]
- Rodrigo, M.A.; Oturan, N.; Oturan, M.A. Electrochemically assisted remediation of pesticides in soils and water: A review. Chem. Rev. 2014, 114, 8720–8745. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q. Arsenic and society. Chem. Teach. Ref. Middle Sch. 1997, 172, 41–43. (In Chinese) [Google Scholar]
- Li, H.; Zhao, M.; Liang, A.; Li, C.; Wang, J.; Xue, B.; Yang, B. Comparative study on contents of As2S2 and As2O3 in realgar and processed products. Chin. J. Exp. Tradit. Med. Formulae 2013, 19, 49–51. (In Chinese) [Google Scholar]
- Jiang, H.; Zhang, Y.; Ding, J.; Shi, S.; Xue, P.; Gao, S.; Gong, H.; Sun, G. Determination of As(III) content in realgar by HPLC-HG-AFS. Chem. Res. 2008, 19, 67–69. (In Chinese) [Google Scholar]
- Sarkar, D.; Datta, R.; Sharma, S. Fate and bioavailability of arsenic in organo-arsenical pesticide-applied soils. Part-I: Incubation study. Chemosphere 2005, 60, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Schrlau, J.E.; Snyder, R.; Snyder, G.H.; Chen, M.; Cisar, J.L.; Cai, Y. Arsenic transport and transformation associated with MSMA application on a golf course green. J. Agric. Food Chem. 2005, 53, 3556–3562. [Google Scholar] [CrossRef] [PubMed]
- Datta, R.; Sarkar, D.; Sharma, S.; Sand, K. Arsenic biogeochemistry and human health risk assessment in organo-arsenical pesticide-applied acidic and alkaline soils: An incubation study. Sci. Total Environ. 2006, 372, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Naujokas, M.F.; Anderson, B.; Ahsan, H.; Aposhian, H.V.; Graziano, J.H.; Thompson, C.; Suk, W.A. The broad scope of health effects from chronic arsenic exposure: Update on a worldwide public health problem. Environ. Health Perspect. 2013, 121, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Das, N.K.; Sengupta, S.R. Arsenicosis: Diagnosis and treatment. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.R.; Das, N.K.; Datta, P.K. Pathogenesis, clinical features and pathology of chronic arsenicosis. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 559–570. [Google Scholar] [PubMed]
- Yu, H.S.; Liao, W.T.; Chai, C.Y. Arsenic carcinogenesis in the skin. J. Biomed. Sci. 2006, 13, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.P. Effects and dose—Response relationships of skin cancer and blackfoot disease with arsenic. Environ. Health Perspect. 1977, 19, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; Mazumder, D.N.; Samanta, S.; Ghosh, N.; Kalman, D.; Smith, M.M.; Mitra, S.; Santra, A.; Lahiri, S.; Das, S.; et al. Arsenic in drinking water and skin lesions: Dose-response data from West Bengal, India. Epidemiology 2003, 14, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Parvez, F.; Gamble, M.; Islam, T.; Ahmed, A.; Argos, M.; Graziano, J.H.; Ahsan, H. Arsenic exposure at low-to-moderate levels and skin lesions, arsenic metabolism, neurological functions, and biomarkers for respiratory and cardiovascular diseases: Review of recent findings from the Health Effects of Arsenic Longitudinal Study (HEALS) in Bangladesh. Toxicol. Appl. Pharmacol. 2009, 239, 184–192. [Google Scholar] [PubMed]
- Smith, A.H.; Arroyo, A.P.; Mazumder, D.N.; Kosnett, M.J.; Hernandez, A.L.; Beeris, M.; Smith, M.M.; Moore, L.E. Arsenic-induced skin lesions among Atacameno people in Northern Chile despite good nutrition and centuries of exposure. Environ. Health Perspect. 2000, 108, 617–620. [Google Scholar] [PubMed]
- Hsueh, Y.M.; Chiou, H.Y.; Huang, Y.L.; Wu, W.L.; Huang, C.C.; Yang, M.H.; Lue, L.C.; Chen, G.S.; Chen, C.J. Serum beta-carotene level, arsenic methylation capability, and incidence of skin cancer. Cancer Epidemiol. Biomark. Prev. 1997, 6, 589–596. [Google Scholar]
- Chen, Y.; Ahsan, H. Cancer burden from arsenic in drinking water in Bangladesh. Am. J. Public Health 2004, 94, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Waalkes, M.P. Liver is a target of arsenic carcinogenesis. Toxicol. Sci. 2008, 105, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Mazumder, D.N. Effect of chronic intake of arsenic-contaminated water on liver. Toxicol. Appl. Pharmacol. 2005, 206, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Santra, A.; Das Gupta, J.; De, B.K.; Roy, B.; Guha Mazumder, D.N. Hepatic manifestations in chronic arsenic toxicity. Indian J. Gastroenterol. 1999, 18, 152–155. [Google Scholar] [PubMed]
- Wang, W.; Cheng, S.; Zhang, D. Association of inorganic arsenic exposure with liver cancer mortality: A meta-analysis. Environ. Res. 2014, 135, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Sohn, W.; Jun, D.W.; Kwak, M.J.; Park, Q.; Lee, K.N.; Lee, H.L.; Lee, O.Y.; Yoon, B.C.; Choi, H.S. Upper limit of normal serum alanine and aspartate aminotransferase levels in Korea. J. Gastroenterol. Hepatol. 2013, 28, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the U.S. population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Chiu, H.F.; Chang, C.C.; Ho, S.C.; Wu, T.N. Bladder cancer mortality reduction after installation of a tap-water supply system in an arsenious-endemic area in southwestern Taiwan. Environ. Res. 2005, 98, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.; Ferreccio, C.; Yuan, Y.; Bates, M.N.; Steinmaus, C.; Selvin, S.; Liaw, J.; Smith, A.H. Fifty-year study of lung and bladder cancer mortality in Chile related to arsenic in drinking water. J. Natl. Cancer Inst. 2007, 99, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Nakadaira, H.; Endoh, K.; Katagiri, M.; Yamamoto, M. Elevated mortality from lung cancer associated with arsenic exposure for a limited duration. J. Occup. Environ. Med. 2002, 44, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.I.; Chen, G.S.; Lee, C.H.; Yang, T.Y.; Chen, Y.H.; Wang, Y.H.; Hsueh, Y.M.; Chiou, H.Y.; Wu, M.M.; Chen, C.J. Use of arsenic-induced palmoplantar hyperkeratosis and skin cancers to predict risk of subsequent internal malignancy. Am. J. Epidemiol. 2013, 177, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; Evans, S.; Gillman, M.; Price Evans, D.A. Medicinal arsenic and internal malignancies. Br. J. Cancer 1982, 45, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; Harris, R.; Mortimer, P.S. Palmar keratoses and cancers of the bladder and lung. Lancet 1984, 1, 530–533. [Google Scholar] [CrossRef]
- Cuzick, J.; Sasieni, P.; Evans, S. Ingested arsenic, keratoses, and bladder cancer. Am. J. Epidemiol. 1992, 136, 417–421. [Google Scholar] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Ye, F.; Wang, A.; Wang, D.; Yang, B.; Zheng, Q.; Sun, G.; Gao, X. Chronic Arsenic Poisoning Probably Caused by Arsenic-Based Pesticides: Findings from an Investigation Study of a Household. Int. J. Environ. Res. Public Health 2016, 13, 133. https://doi.org/10.3390/ijerph13010133
Li Y, Ye F, Wang A, Wang D, Yang B, Zheng Q, Sun G, Gao X. Chronic Arsenic Poisoning Probably Caused by Arsenic-Based Pesticides: Findings from an Investigation Study of a Household. International Journal of Environmental Research and Public Health. 2016; 13(1):133. https://doi.org/10.3390/ijerph13010133
Chicago/Turabian StyleLi, Yongfang, Feng Ye, Anwei Wang, Da Wang, Boyi Yang, Quanmei Zheng, Guifan Sun, and Xinghua Gao. 2016. "Chronic Arsenic Poisoning Probably Caused by Arsenic-Based Pesticides: Findings from an Investigation Study of a Household" International Journal of Environmental Research and Public Health 13, no. 1: 133. https://doi.org/10.3390/ijerph13010133