
The Prevalence of Dry Eye Syndrome’s and the Likelihood to Develop Sjögren’s Syndrome in Taiwan: A Population-Based Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Patients and Variables
2.2. Statistical Analysis
3. Results
Demographic Data

{kind=link}
| Variable | DES Patients (n = 48,704) | Comparison Group (n = 128,542) | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age, median ( IQR a) | 49.8 (10) | 48.7 (15) | |||
| Gender | <0.01 * | ||||
| Male | 14,543 | 29.9 | 43,624 | 33.9 | |
| Female | 34,161 | 70.1 | 84,918 | 66.1 | |
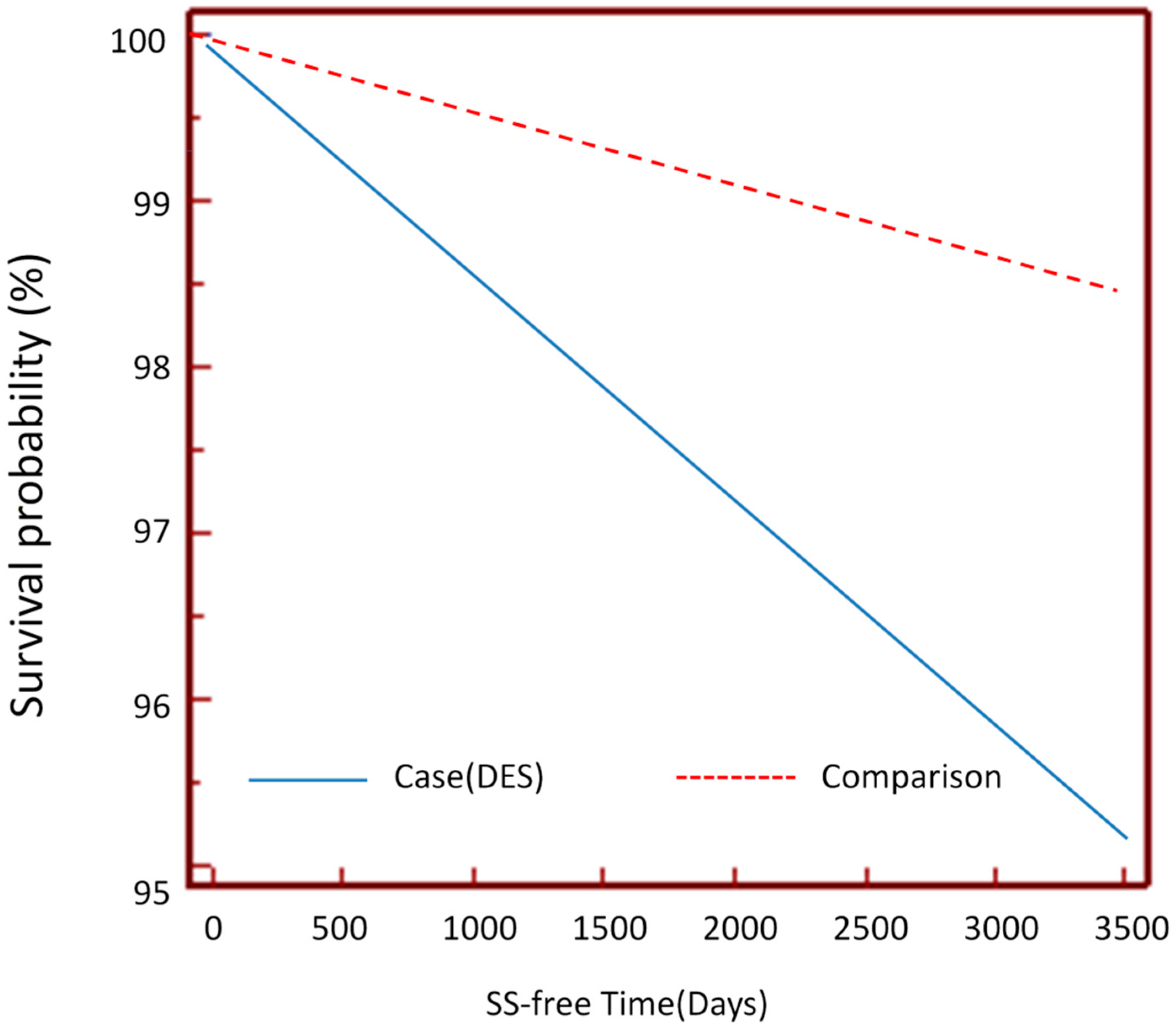
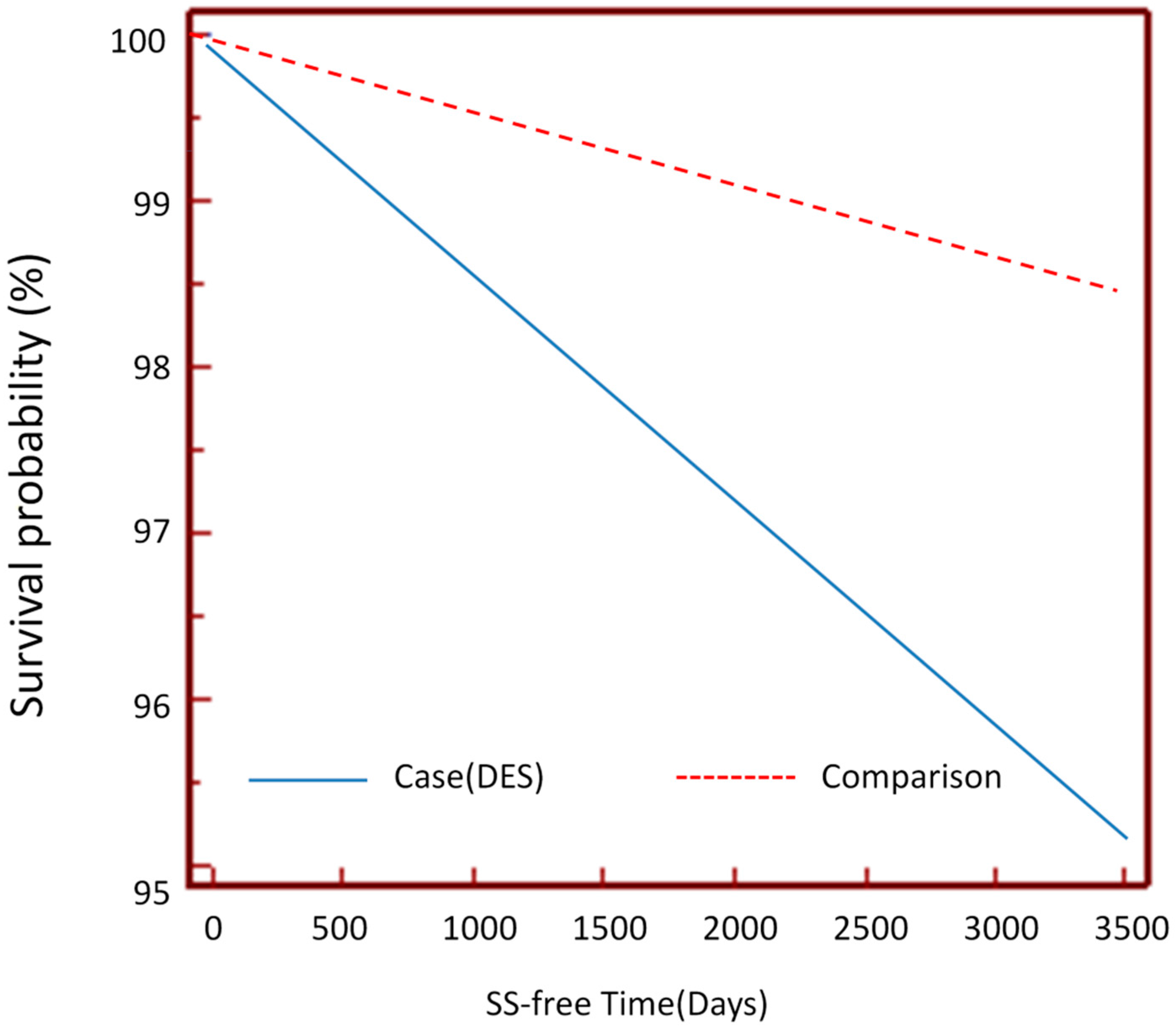
| SS | 2329 | 4.8 | 1927 | 1.5 | <0.0001 ** |
| Observation duration (days, median, IQR a) | 1418 | 781–2316 | 1641 | 971–2512 | <0.001 ** |
| Development of SS | Total | DES | Comparison Group | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| Yes | 4256 | 2.4 | 2329 | 4.8 | 1927 | 1.5 |
| No | 172,990 | 97.6 | 46,375 | 95.2 | 126,615 | 98.5 |
| Crude HR (95% CI) | – | 3.30 (3.10–3.50) | 1.00 | |||
| Adjusted a HR (95% CI) | – | 3.64 (3.43–3.87) | 1.00 | |||
4. Discussion
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Moss, S.E.; Klein, R.; Klein, B.E. Prevalence of and risk factors for dry eye syndrome. JAMA Ophthalmol. 2000, 118, 1264–1268. [Google Scholar] [CrossRef]
- Schein, O.D.; Munoz, B.; Tielsch, J.M.; Bandeen-Roche, K.; West, S. Prevalence of dry eye among the elderly. Am. J. Ophthalmol. 1997, 124, 723–728. [Google Scholar] [CrossRef]
- Uchino, M.; Nishwaki, Y.; Michikawa, T.; Shirakawa, K.; Kuwahara, E.; Yamada, M.; Dogru, M.; Schaumberg, D.A.; Kawakita, T.; Takebayashi, T.; et al. Prevalence and risk factors of dry eye disease in Japan: Koumi study. Ophthalmology 2011, 118, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Blch, K.J.; Buchanan, W.W.; Wohl, M.J.; Bunim, J.J. Sjogren’s Syndrome: A Clinical, Pathological, and Serological Study of Sixty-Two Cases. Medicine 1965, 44, 187–231. [Google Scholar]
- Morgn, W.S.; Castleman, B. A clinicopathologic study of Mikulics’s disease. Am. J. Pathol. 1953, 29, 471–503. [Google Scholar]
- Anderson, L.A.; Gadalla, S.; Morton, L.M.; Landgren, O.; Pfeiffer, R.; Warren, J.L.; Berndt, S.I.; Ricker, W.; Parsons, R.; Engels, E.A. Population-based study of autoimmune conditions and the risk of specific lymphoid malignancies. Int. J. Cancer. 2009, 125, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.H.; Jan, R.L.; Wong, S.F.; Wang, J.J.; Chioc, C.C.; Wei, F.T.; Chu, C.C. Retinal artery occlusion and the 3-year risk of stroke in Taiwan: A Nationwide Population-Based Study. Am. J. Ophthalmol. 2012, 154, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Van der Vaart, R.; Weaver, M.A.; Lefebvre, C.; Davis, R.M. The association between dry eye disease and depression and anxiety in a large population-based study. Am. J. Ophthalmol. 2015, 159, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.A.; Galor, A.; Arheart, K.L.; Musselman, D.L.; Venincasa, V.D.; Florez, H.J.; Lee, D.J. Dry eye syndrome, posttraumatic stress disorder, and depression in an older male veteran population. Invest. Ophthalmol. Vis. Sci. 2013, 54, 3666–3672. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Sullivan, D.A.; Buring, J.E.; Dana, M.R. Prevalence of dry eye syndrome among US women. Am. J. Ophthalmol. 2003, 136, 318–326. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Dana, R.; Buring, J.E.; Sullivan, D.A. Prevalence of dry eye disease among US men: Estimates from the Physicians’ Health Studies. Arch. Ophthalmol. 2009, 127, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Lee, J.; Saw, S.M.; Gazzard, G.; Koh, D.; Widjaja, D.; Tan, D.T. Prevalence and risk factors associated with dry eye symptoms: A population based study in Indonesia. Br. J. Ophthalmol. 2002, 86, 1347–1351. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Tsai, S.Y.; Cheng, C.Y.; Liu, J.H.; Chou, P.; Hsu, W.M. Prevalence of dry eye among an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology 2003, 110, 1096–1101. [Google Scholar] [CrossRef]
- Kang, J.H.; Lin, H.C. Comorbidities in patients with primary Sjogren’s syndrome: A registry-based case-control study. J. Rheumatol. 2010, 37, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Wang, I.J.; Hu, C.C.; Lin, H.C. Comorbidities of dry eye disease: A nationwide population-based study. Acta Ophthalmol. 2012, 90, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Akpek, E.K.; Mathews, P.; Hahn, S.; Hessen, M.; Kim, J.; Grader-Beck, T.; Birnbaum, J.; Baer, A.N. Ocular and systemic morbidity in a longitudinal cohort of Sjogren’s syndrome. Ophthalmology 2015, 122, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Shan, S.J.; Wu, E.I.; Akpek, E.K. Sterile corneal melt after Descemet stripping endothelial keratoplasty in patients with previously undiagnosed Sjogren syndrome. Arch. Ophthalmol. 2009, 127, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.I.; Manche, E.E. Corneal perforation after conductive keratoplasty in a patient with previously undiagnosed Sjogren syndrome. Arch. Ophthalmol. 2007, 125, 1131–1132. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.T.; Bennett, R.M. Chronic anterior and posterior uveitis and primary Sjogren’s syndrome. Am. J. Ophthalmol. 1987, 104, 346–352. [Google Scholar] [CrossRef]
- Bridges, A.J.; Burns, R.P. Acute iritis associated with primary Sjogren’s syndrome and high-titer anti-SS-A/Ro and anti-SSB/La antibodies. Treatment with combination immunosuppressive therapy. Arthritis Rheum 1992, 35, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi-Simab, K.; Lamprecht, P.; Nolle, B.; Ai, M.; Gross, W.L. Successful treatment of refractory anterior scleritis in primary Sjogren’s syndrome with rituximab. Ann. Rheum Dis. 2005, 64, 1087–1088. [Google Scholar] [CrossRef] [PubMed]
- Liew, M.S.; Zhang, M.; Kim, E.; Akpek, E.K. Prevalence and predictors of Sjogren’s syndrome in a prospective cohort of patients with aqueous-deficient dry eye. Br. J. Ophthalmol. 2012, 96, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, J.-C.; Hsu, C.-A.; Li, Y.-C.; Hsu, M.-H. The Prevalence of Dry Eye Syndrome’s and the Likelihood to Develop Sjögren’s Syndrome in Taiwan: A Population-Based Study. Int. J. Environ. Res. Public Health 2015, 12, 7647-7655. https://doi.org/10.3390/ijerph120707647
Yen J-C, Hsu C-A, Li Y-C, Hsu M-H. The Prevalence of Dry Eye Syndrome’s and the Likelihood to Develop Sjögren’s Syndrome in Taiwan: A Population-Based Study. International Journal of Environmental Research and Public Health. 2015; 12(7):7647-7655. https://doi.org/10.3390/ijerph120707647
Chicago/Turabian StyleYen, Ju-Chuan, Chia-An Hsu, Yu-Chuan (Jack) Li, and Min-Huei Hsu. 2015. "The Prevalence of Dry Eye Syndrome’s and the Likelihood to Develop Sjögren’s Syndrome in Taiwan: A Population-Based Study" International Journal of Environmental Research and Public Health 12, no. 7: 7647-7655. https://doi.org/10.3390/ijerph120707647