
Decreasing Health Disparities for People with Disabilities through Improved Communication Strategies and Awareness

Abstract
:1. Introduction
1.1. Who is Disabled?
1.2. Health Disparities and Persons with Disabilities
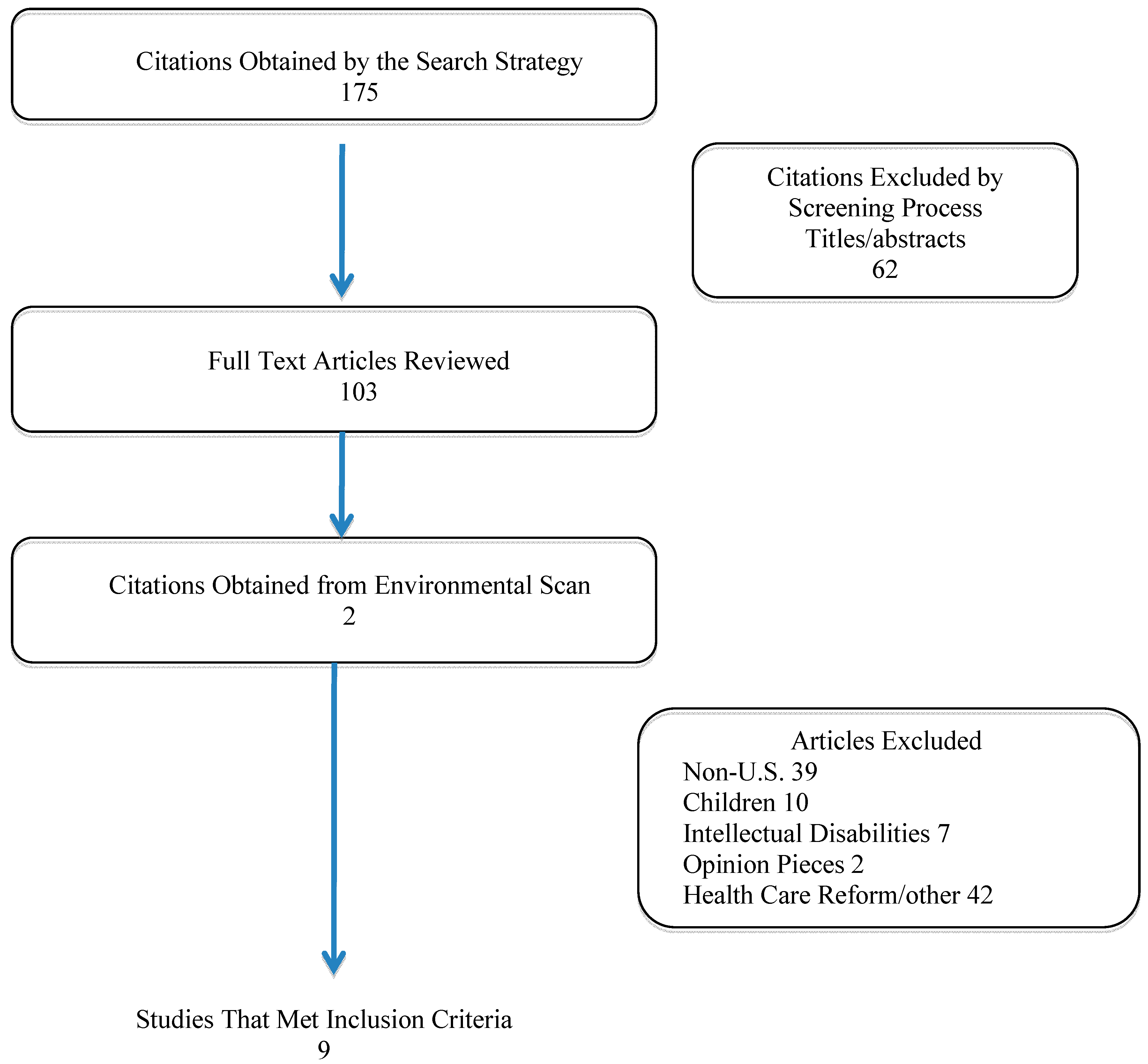
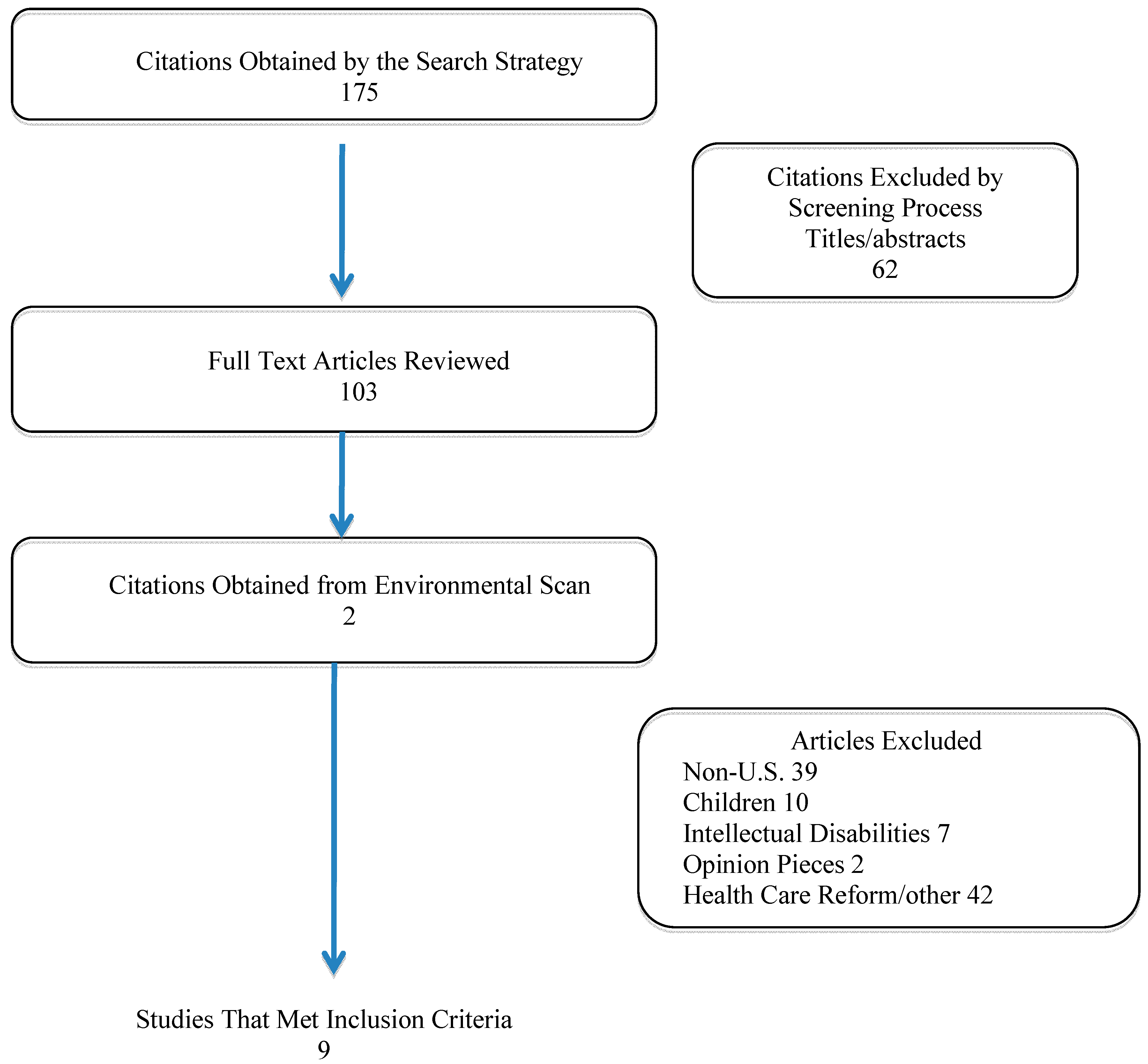
2. Methods
Data Extraction and Analysis
3. Results and Discussion
3.1. Medical Students’ Knowledge and Attitudes

{kind=link}
{kind=link}
| Authors (Year) | Design and Sample | Intervention or Major Aim | Outcomes |
|---|---|---|---|
| Medical Education and Medical Student Perceptions, Attitudes and Comfort Level Working with PWD | |||
| Symons et al, 2014 [21] | Non-randomized controlled study Rx: Medical students enrolled in public medical school with disparities curriculum C: Medical school students from similar institution | Rx: Disabilities curriculum integrated across all four years of study—includes lectures on disability and society, communication with PWD, small group encounters with PWD, precepted clerkship in clinic for PWD, 1/2 workshop on legal and socioeconomic context of caring for PWD, and potential 4-week elective on primary care for PWD | Students in the intervention group reported better attitudes and higher comfort level working with PWD in the following areas: greater comfort working with PWD when someone else is with them (p = 0.008); more positive attitudes towards PWD and perceptions of PWD (p = 0.001). However, male students in the Rx group who encountered PWD in a clinical context had a tendency to agree with more negative statements about PWD |
| Medical Education and Medical Student Perceptions, Attitudes and Comfort Level Working with PWD | |||
| Brown et al, 2010 [19] | Quasi-experimental 146 3rd year medical students engaged in family medicine clerkship | Students engaged in 1 of 3 standardized patient (SP) experiences (1) patient without disability (n = 63); (2) patient with spinal cord injury (SCI) (n = 40); (3) patient with intellectual disability (ID) and his/her caregiver (n = 53) | Students involved in the OSCE with patients with SCI scored lower on history taking, physical exam, ordering of lab tests and interpersonal skills. Ordering of hemoglobin was higher among patients who did not have a disability (OR = 4.16; 95% CI = 1.78–9.17), ordering urinalysis was 3 times higher (OR = 3.08; 95% CI = 1.34–7.08) and oviding lifestyle counseling was 2 times higher (OR = 2.15; 95% CI = 1.04–4.44) |
| Moroz et al, 2010 [20] | Quasi- experimental Rx: 11 PMR residents C: 10 psychiatry residents engaged in standard | Rx: 7-h one day training including didactic lectures, panel presentations covering: disability facts; stories of experiences with medical care from PWD; information and skills on medical evaluation of disability. Following these didactic experiences students were assigned to a play the role of a PWD in a wheelchair or as a caretaker in structured simulations and debriefing sessions. C: Standard medical training | Students demonstrated significant improvements in disability knowledge and more positive attitudes towards PWD. Knowledge in sensitivity training did not persist at 3 months but positive attitudes toward PWD did. |
| Iezzoni et al, 2005 [18] | Focus group study Medical students during final year of study | Focus groups lasted 2 h | Students reported negative views of living with a disability, expressed admiration for PWD who are coping well, most drew their perceptions of PWD from family experiences, students voiced negative attitudes towards a subgroup of PWD, those who are obese and reported morbidly obese patients are responsible for their health status. Students also reported taking short cuts to save time and deal with busy schedules but did not realize this may impact their interactions with PWD. |
| Patient and Provider Perceptions of Health Care and Outcomes | |||
| O’Day et al, 2005 [24] | Focus group 16 patients with psychiatric disabilities in a psychiatric rehabilitation program | Focus group lasted two hours to examine patient perceived barriers to care | PWD reported trouble finding a primary care physician with good communication skills, receiving inadequate information about medication side effects, lack of understanding of their health condition, excess costs due to inadequate health insurance. |
| Patient and Provider Perceptions of Health Care and Outcomes | |||
| Bachman et al , 2006 [23] | Cross-sectional survey 379 health care providers from managed care organizations | No intervention | Providers more likely to provide care to patients with chronic illnesses, mobility, cognitive or psychiatric disabilities than those with communication disorders or visual impairments. Providers reported those with communication disorders are the most difficult to medically manage. The majority perceived PWD do not have easy access to medical care. |
| Morrison et al, 2008 [25] | Focus groups 27 health professionals and 19 adults with disabilities | Focus groups of PWD and providers | Both groups reported primary care providers need more education about PWD, improved education regarding communication and interpersonal skills, improved physical access at clinical sites, more flexible and accessible schedules for medical appointments. |
| Mudrick et al, 2011 [17] | Cross-sectional survey of provider sites conducted by nurses employed by different state health plans | No intervention | Barriers for PWD included physical barriers in bathrooms, examination tables, parking access, and access to buildings. 3.6% had an accessible weight scale and 8.4% had height accessible exam tables. |
| Lagu et al, 2013 [22] | Cross-sectional survey of 256 endocrinology, gynecology, orthopedic surgery, dermatology, urology, ophthalmology, otolaryngology, and psychiatry practices | Researchers posed as a fictional patient who was obese and had hemiparesis, used a wheelchair and could not transfer without assist | 56 (22%) practices reported they could not accommodate the patient, 9 (4%) buildings were inaccessible, 47 (18%) reported they could not transfer the patient to an exam table and 22 (9%) had height adjustable tables or lifts for transfer. Of all practices, gynecology offices were the least accessible |
3.2. Physician and Patient Perceptions
3.3. Access Barriers
3.4. Strategies to Improve Access to Health and Health Outcomes in PWD
| Recommendations for Health Care Providers to Help Decrease Health Disparities for PWD |
|---|
| Make no assumptions about what PWD want. |
| Ask PWD what their preferences are for treatment interventions. |
| Acquire knowledge about conditions that cause disability, functional impacts of these conditions and effective interventions. |
| Develop physical assessment skills to properly examine PWD. |
| Develop sensitivity to the disability experience. |
| Engage in patient-centered care with all health encounters. |
| Be knowledgeable about state and federal statutes that govern accessibility for PWD such as the Americans with Disabilities Act and the Affordable Care Act. |
| Create accessible treatment spaces, including parking and signage. |
| Advocate with third party payers and others to provide adequate time and resources for an effective client encounter. |
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Brault, M. Americans with Disabilities: 2010. Available online: http://www.census.gov/prod/2012pubs/p70-131.pdf (accessed on 16 March 2015).
- Bureau of Labor Statistics, U.S. Department of Labor. Department of Labor. Persons with a Disability: Labor Force Characteristics—2013. Available online: http://www.bls.gov/news.release/pdf/disabl.pdf (accessed on 8 March 2015).
- Yee, S. Health and Health Care Disparities among People with Disabilities. Available online: http://dredf.org/healthcare/Health-and-Health-Care-Disparities-Among-People-with-Disabilities.pdf (accessed on 12 December 2014).
- Anderson, W. The Impact of Disability on Health Care Costs. Available online: http://www.rti.org/files/fellowseminar/fellowseminar_longtermcare_anderson.pdf (accessed 20 December 2014).
- McColl, M.A. Disability studies at the population level: Issues of health service utilization. Amer. J. Occup. Ther. 2005, 59, 516–626. [Google Scholar] [CrossRef]
- Iezzoni, L.I. Eliminating health and health care disparities among the growing population of people with disabilities. Health Affair. 2011, 30, 1947–1956. [Google Scholar] [CrossRef]
- Information and Technical Assistance on the Americans with Disabilities Act. Available online: http://www.ada.gov (accessed on 10 December 2014).
- Roush, S.E.; Sharby, N. Disability reconsidered: The paradox of physical therapy. Phys. Ther. 2011, 91, 1715–1727. [Google Scholar] [CrossRef] [PubMed]
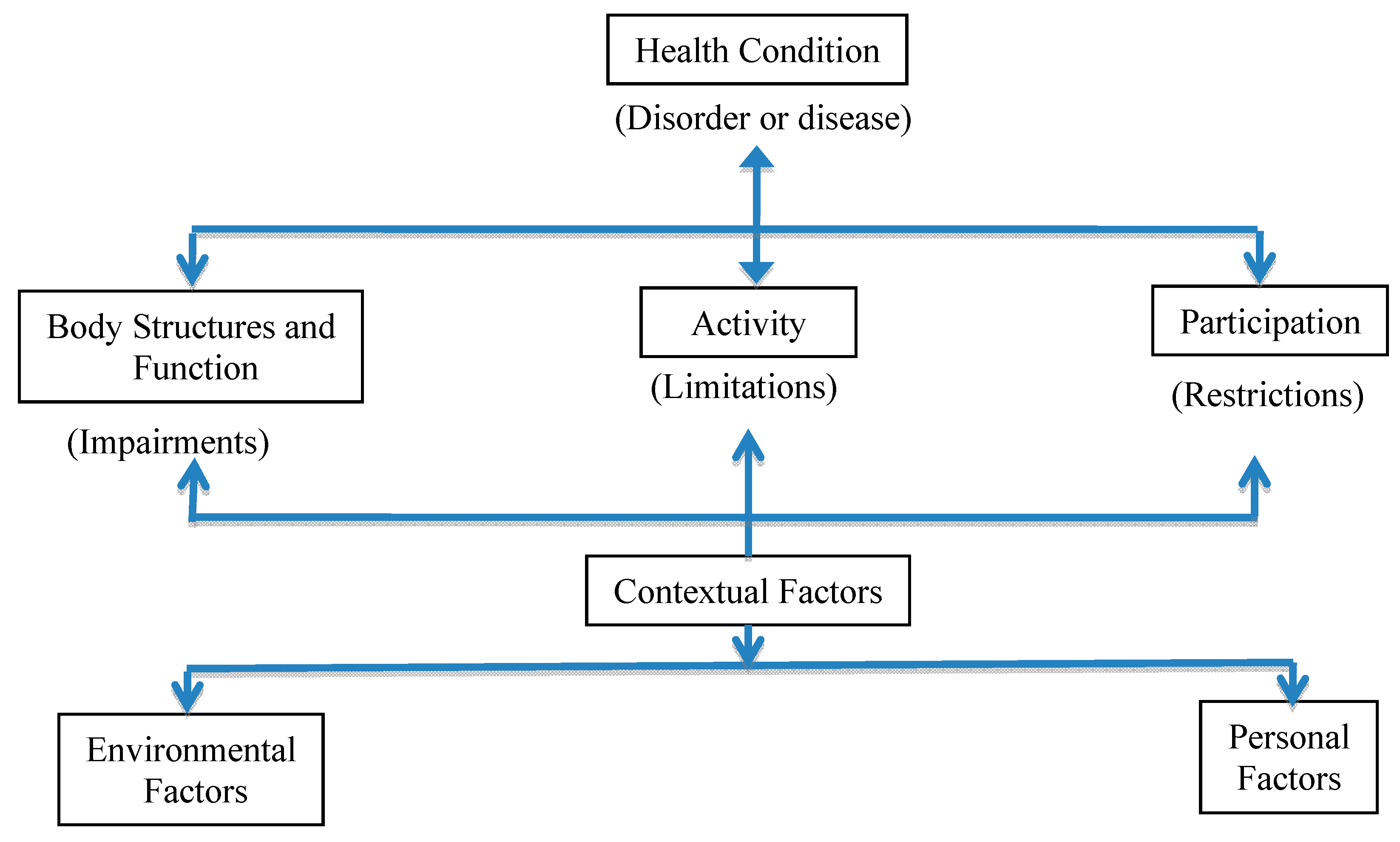
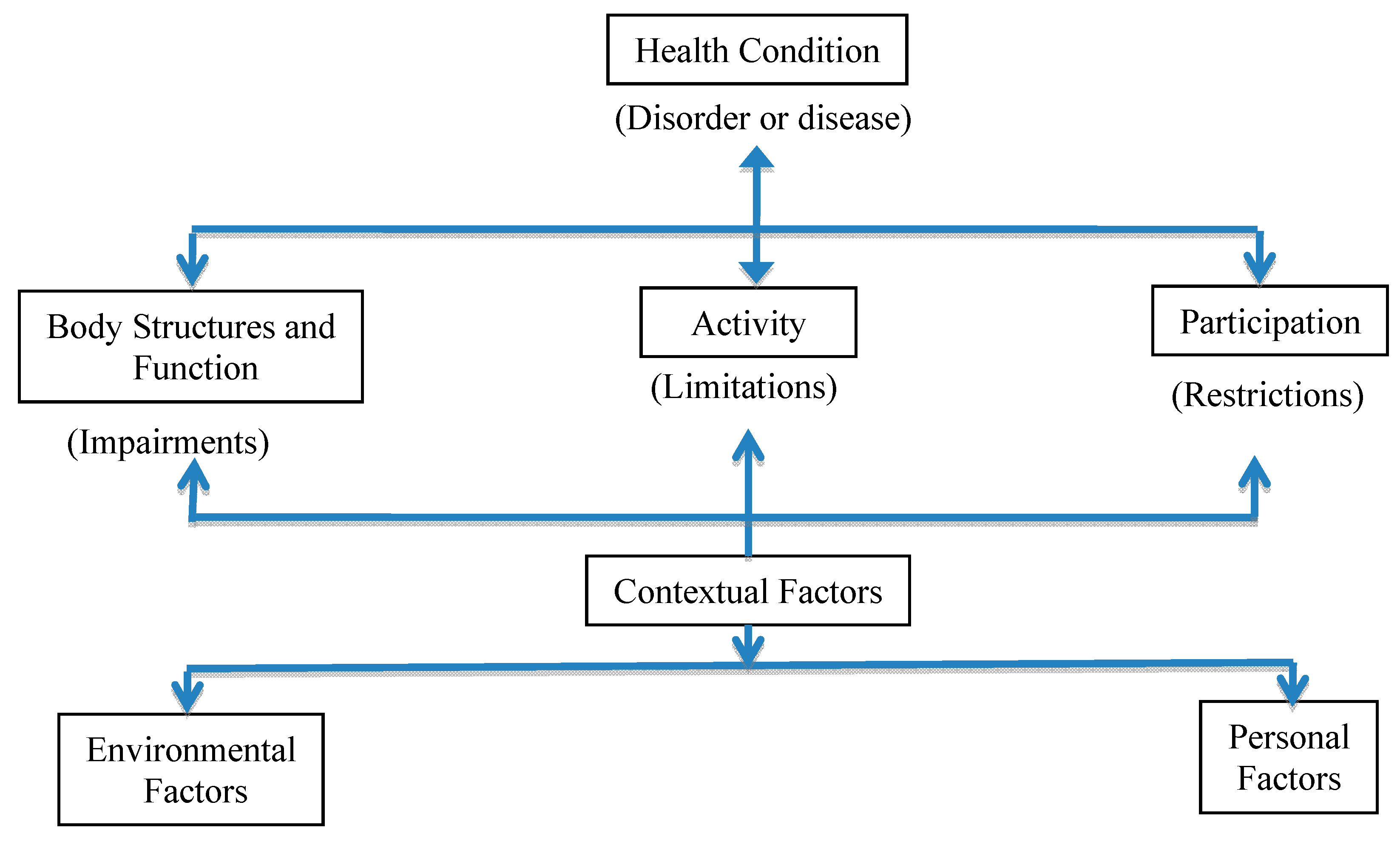
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). Available online: http://www.who.int/classifications/icf/en/ (accessed on 15 December 2014).
- Kielhofner, G. Rethinking disability and what to do about it: Disability studies and its implications for occupational therapy. Amer. J. Occup. Ther. 2005, 59, 487–496. [Google Scholar] [CrossRef]
- Convention on the Rights of People with Disabilities. Available online: http://www.un.org/disabilities/convention/conventionfull.shtml (accessed on 23 December 2014).
- Iezzoni, L.I. Make no assumptions: Communication between persons with disabilities and clinicians. Asst. Technol. 2006, 18, 212–219. [Google Scholar] [CrossRef]
- Goode, T.D.; Carter-Pokras, O.D.; Horner-Johnson, W.; Yee, S. Parallel tracks: Reflections on the need for collaborative health disparities research on race/ethnicity and disability. Med. Care 2014, 52, 3–8. [Google Scholar] [CrossRef]
- Disparities and Disabilities: Another View of a Health Care Issue. Available online: http://www.dpcma.org (accessed on 19 December 2014).
- Jones, G.C.; Sinclair, L.B. Multiple health disparities among minority adults with mobility limitations: An application of the ICF framework and codes. Disabil. Rehabil. 2008, 30, 901–915. [Google Scholar] [CrossRef] [PubMed]
- National Healthcare Disparities Report, 2010. Available online: http://www.ahrq.gov/research/findings/nhqrdr/nhdr10/Chap10a.html (accessed 17 December 2014).
- Mudrick, N.R.; Breslin, M.L.; Liang, M.; Yee, S. Physical accessibility in primary health care settings: Results from California on-site reviews. Disabil. Health J. 2011, 5, 159–167. [Google Scholar] [CrossRef]
- Iezzoni, L.I.; Ramanan, R.A.; Drew, R.E. Teaching Medical Students about Communicating with Patients Who Have Sensory or Physical Disabilities. Available online: http://www.dsq-sds.org/article/view/527/704 (accessed on 12 March 2015).
- Brown, R.S.; Graham, C.L.; Richeson, N.; Wu, J.; McDermott, S. Evaluation of medical student performance on objective structured clinical exams with standardized patients with and without disabilities. Acad. Med. 2010, 85, 1766–1771. [Google Scholar] [CrossRef]
- Moroz, A; Gonzalez-Ramos, G; Festinger, T; Langer, K; Zefferino, S; Kalet, A. Immediate and follow-up effects of a brief disability curriculum on disability knowledge and attitudes of PM&R residents: A comparison group trial. Med. Teach. 2010, 32, 360–364. [Google Scholar]
- Symons, A.B.; Morley, C.P.; McGuigan, D.; Akl, E.A. A curriculum on care for people with disabilities: Effects on medical student self-reported attitudes and comfort level. Disabil. Health J. 2014, 7, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Lagu, T.; Hannon, N.S.; Rothberg, M.B.; Wells, A.S.; Green, K.L.; Windom, M.O.; Dempsey, K.R.; Pekow, P.S.; Avrunin, J.S.; Chen, A.; Lindenauer, P.K. Access to subspecialty care for patients with mobility impairments. Ann. Intern. Med. 2013, 158, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Bachman, S.S.; Vefrani, M.; Drainoni, M.-L.; Tobias, C.; Maisels, L. Provider perceptions of their capacity to offer accessible health care for people with disabilities. J. Disabil. Policy Stud. 2006, 17, 130–136. [Google Scholar] [CrossRef]
- O’Day, B.; Killeen, M.B.; Sutton, J.; Iezzoni, L.I. Primary care experiences of people with psychiatric disabilities: Barriers to care and potential solutions. Psychiat. Rehabil. J. 2005, 28, 339–345. [Google Scholar] [CrossRef]
- Morrison, E.H.; George, V.; Mosqueda, L. Primary care for adults with physical disabilities. Fam. Med. 2008, 40, 645–651. [Google Scholar] [PubMed]
- Serious Mental Illness (SMI) among U.S. Adults. Available online: http://www.nimh.nih.gov/health/statistics/prevalence/serious-mental-illness-smi-among-us-adults.shtml (accessed on 19 December 2014).
- Campbell, F.K. Medical education and disability studies. J. Med. Humanit. 2009, 30, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Courser, G.T. What disability studies has to offer medical education. J. Med. Humanit. 2011, 32, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Byron, M.; Cockshott, Z.; Brownett, H.; Ramkalawan, T. What does “disability” mean for medical students? An exploration of the words medical students associate with the term “disability”. Med. Educ. 2005, 39, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare, T.; Iezzoni, L.I.; Groce, N.E. Disability and the training of health professionals. Lancet 2009, 374, 1815–1816. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, K.L.; Curry, R.H. Educating health professional to care for patients with disabilities. JAMA 2009, 302, 1334–1335. [Google Scholar] [CrossRef] [PubMed]
- Iezzoni, L.I.; Lomng-Bellil, L.M. Training physicians about caring for persons with disabilities: “Nothing about us without us”. Disabil. Health 2012, 5, 136–139. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharby, N.; Martire, K.; Iversen, M.D. Decreasing Health Disparities for People with Disabilities through Improved Communication Strategies and Awareness. Int. J. Environ. Res. Public Health 2015, 12, 3301-3316. https://doi.org/10.3390/ijerph120303301
Sharby N, Martire K, Iversen MD. Decreasing Health Disparities for People with Disabilities through Improved Communication Strategies and Awareness. International Journal of Environmental Research and Public Health. 2015; 12(3):3301-3316. https://doi.org/10.3390/ijerph120303301
Chicago/Turabian StyleSharby, Nancy, Katharine Martire, and Maura D. Iversen. 2015. "Decreasing Health Disparities for People with Disabilities through Improved Communication Strategies and Awareness" International Journal of Environmental Research and Public Health 12, no. 3: 3301-3316. https://doi.org/10.3390/ijerph120303301