A Prospective Cohort Study of Alcohol Exposure in Early and Late Pregnancy within an Urban Population in Ireland

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Sample and Recruitment
2.2. Data Collection
2.3. Antenatal Care
2.4. Perinatal Outcomes
2.5. Analysis
3. Results
3.1. Descriptive Statistics

{kind=link}
| Characteristic | Study Population at Recruitment i n = 1,300 (%) | Study Population at Third Trimester ii n = 907 (%) | Study Population at Delivery iii n = 1,216 (%) | General Hospital Population iv n = 6,720 (%) |
|---|---|---|---|---|
| Maternal age at booking | ||||
| <20 years | 34 (2.6) | 19 (2.1) | 31 (2.5) | 200 (3.0) |
| 20–24 years | 161 (12.4) | 102 (11.2) | 152 (12.5) | 776 (11.6) |
| 25–29 years | 362 (27.8) | 235 (25.9) | 336 (27.6) | 1,527 (22.7) |
| 30–34 years | 453 (34.8) | 334 (36.8) | 427 (35.1) | 2,322 (34.6) |
| 35–39 years | 247 (19.0) | 188 (20.7) | 232 (19.1) | 1,592 (23.7) |
| >40 years | 43 (3.3) | 29 (3.2) | 38 (3.1) | 301 (4.5) |
| Marital status | ||||
| Married | 679 (52.2) | 505 (55.7) | 635 (52.2) | 3,952 (58.5) |
| Single | 621 (47.8) | 402 (44.3) | 581 (47.8) | 2,685 (40.0) |
| Socioeconomic group | ||||
| Professional | 341 (26.2) | 258 (28.4) | 317 (26.1) | 2,077 (30.9) |
| Home duties | 222 (17.1) | 135 (14.9) | 206 (16.9) | 961 (14.3) |
| Non-manual | 491 (37.8) | 369 (40.7) | 481 (39.6) | 2,622 (39.0) |
| Manual | 65 (5.0) | 44 (4.9) | 46 (3.8) | 267 (4.0) |
| Unemployed | 117 (9.0) | 50 (5.5) | 103 (8.5) | 501 (7.5) |
| Non-classifiable | 64 (4.9) | 51 (5.6) | 63 (5.2) | 289 (4.3) |
| Nationality | ||||
| Irish | 888 (68.3) | 618 (68.1) | 839 (69.0) | 5,510 (82.0) |
| Non-Irish | 412 (31.7) | 289 (31.9) | 377 (31.0) | 1,189 (17.7) |
| Gestation at booking * | ||||
| <12 weeks | 528 (40.8) | 369 (40.7) | 493 (40.5) | 2,666 (39.8) |
| 12–20 weeks | 729 (56.3) | 523 (57.7) | 687 (56.5) | 3,683 (55.0) |
| >20 weeks | 37 (2.9) | 15 (1.7) | 36 (3.0) | 349 (5.2) |
| Private Health Care | ||||
| Yes | 145 (11.2) | 122 (13.5) | 142 (11.7) | 1,219 (18.1) |
| No | 1,155 (88.8) | 785 (86.5) | 1,074 (88.3) | 5,499 (81.9) |
| Total n = 731 i | Ex-Drinker All Pregnancy n = 441 (%) | Third Trimester Drinker Only n = 185 (%) | First and Third Trimester Drinker n = 105 (%) |
|---|---|---|---|
| Aware of units of alcohol in drinks(moderate or good knowledge) | 46 (10.4) | 21 (11.3) | 20 (19.1) p = 0.03 |
| Aware of recommended alcohol units women should not exceed | 35 (7.9) | 16 (8.6) | 16 (15.2) p = 0.02 |
| Units consumed pre-pregnancy <1–5 (per week) 6–14 15–20 >20 Any binge drinking episode | 279 (63.3) 127 (28.8) 24 (5.4) 33 (7.5) 174 (39.5) | 73 (39.5) 72 (38.9) 23 (12.4) 17 (9.2) 86 (46.5) | 44 (41.9) 37 (35.3) 9 (8.6) 15 (14.3) p = 0.01 56 (53.3) p = 0.03 |
| Alcohol source ii Alcopop Beer Wine Cider Spirits | 30 (6.8) 102 (23.1) 154 (34.9) 21 (4.8) 51 (11.6) | 7 (3.7) 58 (31.4) 90 (48.7) 13 (7.0) 19 (10.3) | 6 (5.8) 33 (31.4) 50 (47.6) 8 (7.6) 17 (16.2) |
| Units consumed first trimester <1–5 (per week) 6–14 15–20 >20 Any binge drinking episode | __ __ __ __ __ | __ __ __ __ __ | 97 (92.4) 7 (6.7) ∫ 1 (1.0) 0 (0.0) 1 (1.0) |
| Units consumed third trimester <1–5 (per week) 6–14 15–20 >20 Any binge drinking episode | __ __ __ __ __ | 135 (73.0) 30 (16.3) 3 (1.6) 0 (0.0) 5 (2.7) | 79 (75.2) 21 (20.0) ∫ 1 (1.0) 2 (2.0) 7 (6.7) |
| Total n = 907 | Non-Drinker n = 617 (%) | Third trimester only n = 185 (%) | First and Third Trimester n = 105 (%) | Odds ratio i 95% Confidence Intervals | Odds ratio ii 95% Confidence Intervals |
|---|---|---|---|---|---|
| Maternal age < 20 years 20–29 years ∫ 30–39 years >40 years | 16 (2.6) 256 (41.5) 326 (52.8) 19 (3.1) | 2 (1.1) 55 (29.7) 122 (66.0) 6 (3.2) | 1 (1.0)26 (24.7)74 (70.5)4 (3.8) | 0.58 (0.13–2.60) 1.00 1.74 (1.22–2.49) * 1.47 (0.56–3.85) | 0.62 (0.08–4.83) 1.00 2.24 (1.39–3.60) *2.07 (0.66–6.55) |
| Single Marital status | 260 (42.1) | 90 (48.6) | 52 (49.5) | 1.30 (0.94–1.81) | 1.35 (0.89–2.04) |
| Socioeconomic group Professional Home duties ∫ Non-manual Manual Unemployed Non-classifiable | 159 (25.8) 99 (16.0) 262 (42.5) 31 (5.0) 31 (5.0) 35 (5.7) | 64 (34.6) 23 (12.4) 73 (39.5) 7 (3.8) 12 (6.5) 6 (3.2) | 35 (33.3) 13 (12.4) 34 (32.4) 6 (5.7) 7 (6.7) 10 (9.5) | 1.73 (1.01–2.97) *1.00 1.20 (0.71–2.02) 0.97 (0.38–2.48) 1.67 (0.74–3.73) 0.74 (0.28–1.96) | 1.68 (0.85–3.32)1.00 0.99 (0.50–1.95) 1.47 (0.52–4.20) 1.72 (0.63–4.69) 2.18 (0.88-5.41) |
| Irish Nationality | 383 (62.1) | 148 (80.0) | 87 (82.9) | 2.44 (1.65–3.63) * | 2.95 (1.73–5.03) * |
| Private Health Care | 68 (11.0) | 33 (17.8) | 21 (20.0) | 1.75 (1.11–2.76) * | 2.02 (1.18–3.47) * |
| Nulliparous | 290 (47.0) | 91 (49.2) | 38 (36.2) | 1.09 (0.79–1.52) | 0.64 (0.42–0.98) |
| Unplanned pregnancy | 202 (32.7) | 52 (28.1) | 34 (32.4) | 0.80 (0.56–1.15) | 0.98 (0.63–1.53) |
| Gestation at booking <12 weeks ∫ 12–20 weeks >20 weeks | 255 (41.3) 351 (56.9) 11 (1.8) | 78 (42.2) 105 (56.8) 2 (1.1) | 36 (34.3) 67 (63.8) 2 (1.9) | 1.00 0.98 (0.70–1.37) 0.59 (0.13–2.74) | 1.00 1.35 (0.87–2.09) 1.29 (0.27–6.05) |
| Current smoker | 56 (9.1) | 25 (13.5) | 29 (27.6) | 1.57 (0.95–2.59) | 3.82 (2.30–6.36) * |
| Illicit drug use (ever) | 57 (9.2) | 34 (18.4) | 24 (22.9) | 2.21 (1.39–3.51) * | 2.91 (1.71–4.95) * |
| Social worker referral | 16 (2.6) | 5 (2.7) | 1 (1.0) | 1.04 (0.38–2.75) | 0.36 (0.05–2.75) |
3.2. Perinatal Outcomes
| Alcohol Intake | Non-Drinker n = 617 | Third Trimester Only Alcohol n = 185 | First and Third Trimester Alcohol n = 105 | Third Trimester Only vs. Non-Drinker Odds Ratio (95% CI) Adjusted i OR (95% CI) | First and Third Trimester vs. Non-Drinker Odds Ratio (95% CI) Adjusted i OR (95% CI) |
|---|---|---|---|---|---|
| Gestational age (weeks) Mean (SD) Range Mean difference (95% CI) | 39.6 (1.5) 29–42 | 40.0 (1.5) 32–42 | 39.7 (1.5) 32–42 | 0.4 (0.2–0.6)* | 0.1 (−0.2–0.4) |
| Birth weight (g) Mean (SD) Range Mean difference (95% CI) | 3,460 (498) 1,145–5,160 | 3,494 (500) 1,970–5,030 | 3,527 (571) 1,530–4,700 | 34 (−48–116) | 67 (−39–173) |
| Preterm birth <37 weeks (%) | 33 (5.3) | 6 (3.2) | 3 (2.9) | 0.77 (0.50–1.20) 0.78 (0.50–1.37) | 0.52 (0.16–1.73) 0.50 (0.15–1.74) |
| Low birth weight <2,500 g (%) | 23 (3.7) | 5 (2.7) | 3 (2.9) | 0.72 (0.27–1.91) 0.83 (0.50–1.37) | 0.76 (0.22–2.58) 0.67 (0.19–2.39) |
| Intrauterine growth restriction i, ii (%) | 80 (13.0) | 32 (17.3) | 13 (12.4) | 1.40 (0.90–2.20) 1.22 (0.97–1.55) | 0.95 (0.51–1.77) 0.90 (0.46–1.77) |
| Apgar score <7 at 5 min (%) | 5 (0.9) | 1 (0.5) | 1 (1.0) | 0.67 (0.08–5.73) 1.00 (0.34–3.04) | 1.18 (0.14–10.2) 1.30 (0.13–12.68) |
| Admitted to neonatal unit (%) | 108 (17.5) | 29 (15.7) | 11 (10.5) | 0.88 (0.56–1.37) 0.91 (0.71–1.16) | 0.55 (0.29–1.07) 0.46 (0.22–1.01) |
4. Discussion
4.1. Summary of Main Findings
4.2. Strengths and Limitations of the Study
4.3. Comparison with Existing Literature
4.4. Implications for Practice
5. Conclusions
Acknowledgments
Authors Contributions
Conflicts of Interest
References
- O’Leary, C.M.; Nassar, N.; Kurinczuk, J.J.; Bower, C. The effect of maternal alcohol consumption on fetal growth and preterm birth. BJOG 2009, 116, 390–400. [Google Scholar] [CrossRef]
- Crozier, S.R.; Robinson, S.M.; Borland, S.E.; Godfrey, K.M.; Cooper, C.; Inskip, H.M.; the SWS Study Group. Do women change their health behaviours in pregnancy? Findings from the southampton women’s survey. Paediatr. Perinat. Epidemiol. 2009, 23, 446–453. [Google Scholar] [CrossRef]
- Mullally, A.; Cleary, B.J.; Barry, J.; Fahey, T.P.; Murphy, D.J. Prevalence, predictors and perinatal outcomes of peri-conceptional alcohol exposure—Retrospective cohort study in an urban obstetric population in Ireland. BMC Pregnancy Childbirth 2011, 11. [Google Scholar] [CrossRef]
- Borges, G.; Lopez-Cervantes, M.; Medina-Mora, M.E.; Tapia-Conyer, R.; Garrido, F. Alcohol consumption, low birth weight, and preterm delivery in the National Addiction Survey (Mexico). Int. J. Addict. 1993, 28, 355–368. [Google Scholar]
- Lundsberg, L.S.; Bracken, M.B.; Saftlas, A.F. Low-to-moderate gestational alcohol use and intrauterine growth retardation, low birthweight and preterm delivery. Ann. Epidemiol. 1997, 7, 498–508. [Google Scholar] [CrossRef]
- Patra, J.; Bakker, R.; Irving, H.; Jaddoe, V.W.; Malini, S.; Rehm, J. Dose-response relationship between alcohol consumption before and during pregnancy and the risks of low birthweight, preterm birth and small for gestational age (SGA)—A systematic review and meta-analysis. BJOG 2011, 118, 1411–1421. [Google Scholar] [CrossRef]
- Henderson, J.; Gray, R.; Brocklehurst, P. Systematic review of effects of low-moderate prenatal alcohol exposure on pregnancy outcome. BJOG 2007, 114, 243–252. [Google Scholar] [CrossRef]
- Pfinder, M.; Kunst, A.E.; Feldmann, R.; van Eijsden, M.; Vrijkotte, T.G. Preterm birth and small for gestational age in relation to alcohol consumption during pregnancy: Stronger associations among vulnerable women? Results from two large Western-European studies. BMC Pregnancy Childbirth 2013, 13. [Google Scholar] [CrossRef]
- Henderson, J.; Kesmodel, U.; Gray, R. Systematic review of the fetal effects of prenatal binge-drinking. J. Epidemiol. Community Health 2007, 61, 1069–1073. [Google Scholar] [CrossRef]
- Kesmodel, U. Binge-drinking in pregnancy—Frequency and methodology. Am. J. Epidemiol. 2001, 154, 777–782. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. Antenatal Care: Routine Care For the Healthy Pregnant Woman; National Institute for Health and Clinical Excellence: London, UK, 2008. [Google Scholar]
- Murphy, D.J.; Mullally, A.; Cleary, B.J.; Fahey, T.P.; Barry, J. Behavioural change in relation to alcohol exposure in early pregnancy and impact on perinatal outcomes—A prospective cohort study. BMC Pregnancy Childbirth 2013, 13. [Google Scholar] [CrossRef]
- Murphy, D.J.; Dunney, C.; Mullally, A.; Adnan, N.; Deane, R. Population-based study of smoking behaviour throughout pregnancy and adverse perinatal outcomes. Int. J. Res. Public Health 2013, 10, 3855–3867. [Google Scholar] [CrossRef]
- O’Leary, C.; Halliday, J.; Bartu, A.; D’Antoine, H.; Bower, C. Alcohol-use disorders during and within one year of pregnancy: A population-based cohort study 1985–2006. BJOG 2013, 120, 744–753. [Google Scholar] [CrossRef]
- McCarthy, F.P.; O’Keeffe, L.M.; Khashan, A.S.; North, R.A.; Poston, L.; McCowan, L.M.E.; Baker, P.N.; Dekker, G.A.; Roberts, C.T.; WalKer, J.J.; et al. Association between maternal alcohol consumption in early pregnancy and pregnancy outcomes. Obstet. Gynecol. 2013, 122, 830–837. [Google Scholar] [CrossRef]
- Comasco, E.; Hallberg, G.; Helander, A.; Oreland, L.; Sundelin-Wahlsten, V. Alcohol consumption among pregnant women in a Swedish sample and its effects on the newborn outcomes. Alcohol. Clin. Exp. Res. 2012, 36, 1779–1786. [Google Scholar] [CrossRef]
- Bakker, R.; Pluimgraaff, L.E.; Steegers, E.A.; Raat, H.; Tiemeier, H.; Hofman, A.; Jaddoe, V.W.V. Associations of light and moderate maternal alcohol consumption with fetal growth characteristics in different periods of pregnancy: The Generation R Study. Int. J. Epidemiol. 2010, 39, 777–789. [Google Scholar] [CrossRef]
- Guidelines and Audit Committee of the Royal College of Obstetricians and Gynaecologists. Statement on Alcohol Consumption and the Outcomes of Pregnancy; Royal College of Obstetricians and Gynaecologists: London, UK, 2006. [Google Scholar]
Appendix
| Item | Item No | Recommendation |
|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract Included—title and abstract |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found Included, page 2 | ||
| Introduction | ||
| Background/Rationale | 2 | Explain the scientific background and rationale for the investigation being reported Included, page 4–5 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses Included, page 5 |
| Methods | ||
| Study design | 4 | Present key elements of study design early in the paper Included, page 5–7 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection Included, Page 5 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up Included, page 5–6 |
| (b)For matched studies, give matching criteria and number of exposed and unexposed Not applicable | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable Included, page 5–7 |
| Data sources/Measurement | 8 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group Included, page 5–7 |
| Bias | 9 | Describe any efforts to address potential sources of bias Not applicable, complete cohort |
| Study size | 10 | Explain how the study size was arrived at Time limited cohort |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why Described statistics section |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding |
| (b) Describe any methods used to examine subgroups and interactions | ||
| (c) Explain how missing data were addressed | ||
| (d) If applicable, explain how loss to follow-up was addressed | ||
| (e) Describe any sensitivity analyses Described, statistics section | ||
| Results | ||
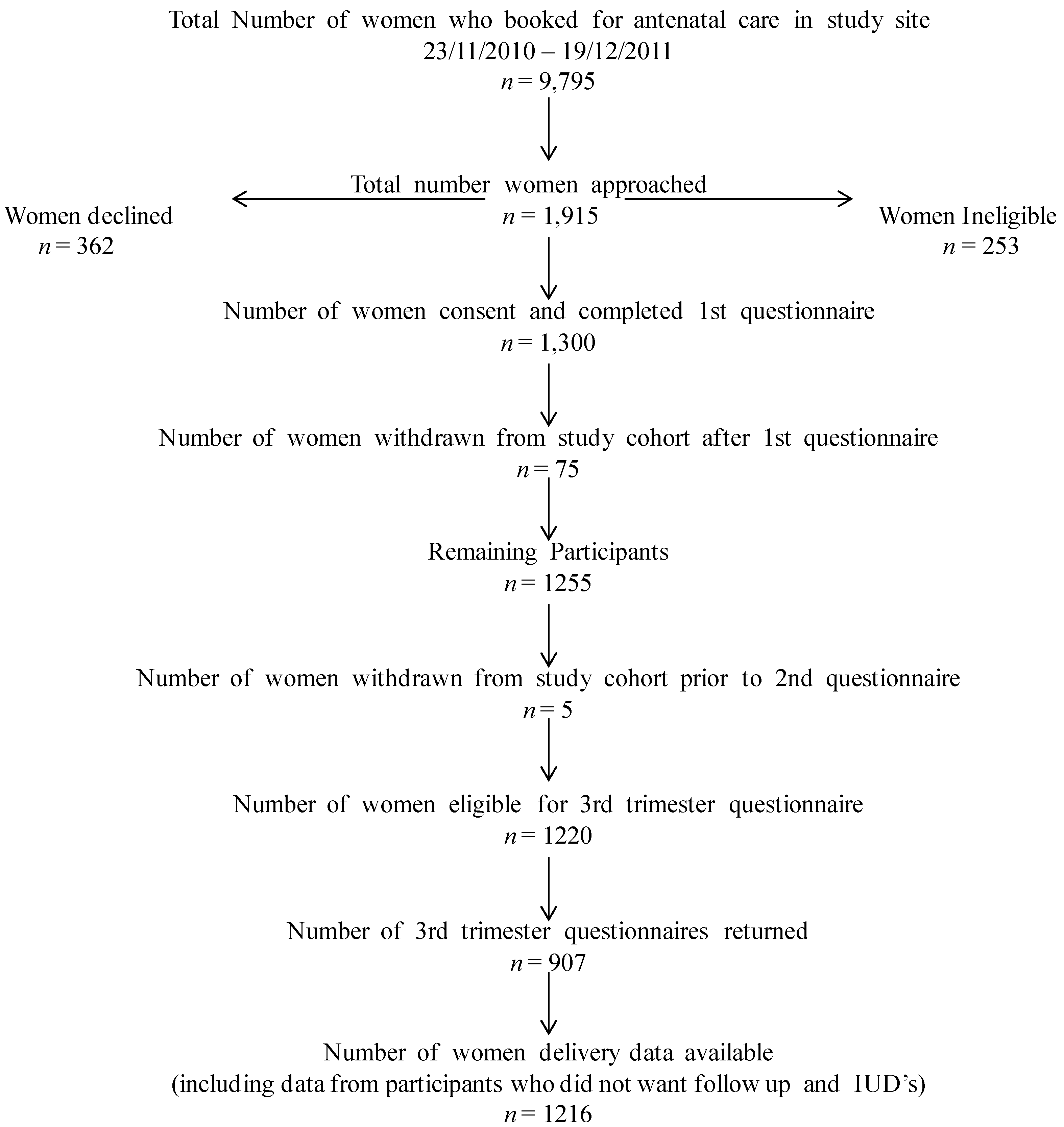
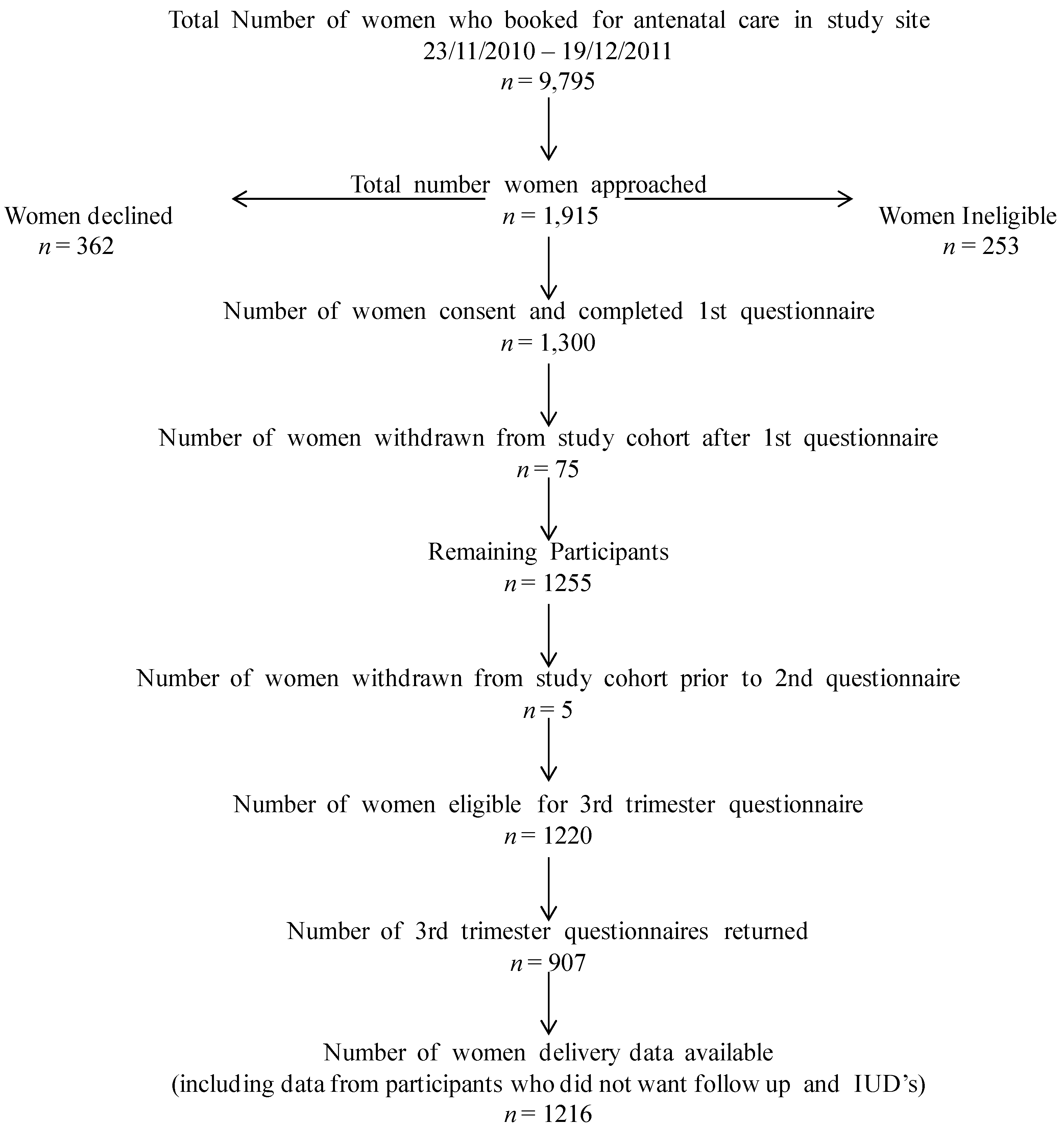
| Participants | 13 * | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed See footnote Table 1and methods section |
| (b) Give reasons for non-participation at each stage | ||
| (c) Consider use of a flow diagram | ||
| Descriptive data | 14 * | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders |
| (b) Indicate number of participants with missing data for each variable of interest | ||
| (c) Summarise follow-up time (e.g., average and total amount) Descriptive data presented - results and Tables | ||
| Outcome data | 15 * | Report numbers of outcome events or summary measures over time Outcome data presented - results and Tables |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included |
| (b) Report category boundaries when continuous variables were categorized | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period Appropriate estimates adjusted—unadjusted presented | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses |
| Discussion | ||
| Key results | 18 | Summarise key results with reference to study objectives |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results Discussion follows recommended format |
| Other information | ||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based Included, page 14 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Murphy, D.J.; Dunney, C.; Mullally, A.; Adnan, N.; Fahey, T.; Barry, J. A Prospective Cohort Study of Alcohol Exposure in Early and Late Pregnancy within an Urban Population in Ireland. Int. J. Environ. Res. Public Health 2014, 11, 2049-2063. https://doi.org/10.3390/ijerph110202049
Murphy DJ, Dunney C, Mullally A, Adnan N, Fahey T, Barry J. A Prospective Cohort Study of Alcohol Exposure in Early and Late Pregnancy within an Urban Population in Ireland. International Journal of Environmental Research and Public Health. 2014; 11(2):2049-2063. https://doi.org/10.3390/ijerph110202049
Chicago/Turabian StyleMurphy, Deirdre J., Clare Dunney, Aoife Mullally, Nita Adnan, Tom Fahey, and Joe Barry. 2014. "A Prospective Cohort Study of Alcohol Exposure in Early and Late Pregnancy within an Urban Population in Ireland" International Journal of Environmental Research and Public Health 11, no. 2: 2049-2063. https://doi.org/10.3390/ijerph110202049