1. Introduction
The concentration of bacterial indicators in recreational water, such as
Escherichia coli (
E. coli), has been linked to cases of waterborne disease [
1,
2,
3]. Health risks associated with exposure to contaminated recreational water include skin, eye, ear, and upper respiratory irritations and infections, as well as gastrointestinal illness (GI) [
4]. Populations that may be at greater risk for contracting GI from contaminated recreational water include children, the elderly, and individuals with compromised immune systems [
5].
The 1986 United States Environmental Protection Agency (EPA) recreational water quality criteria for freshwater beaches include a daily
E. coli concentration of less than 235 colony forming units (CFUs) per 100 milliliters of water [
2,
3,
4,
5,
6]. Bacteria concentrations exceeding these criteria trigger swimming advisories and/or beach closures to prevent exposure to waterborne pathogens.
Recreational water can be contaminated from both point and nonpoint sources [
7,
8]. Additionally, recreational water quality is influenced by precipitation and other hydrometeorological parameters [
9,
10]. Precipitation is positively correlated with
E. coli concentrations in recreational water [
11,
12,
13]. High concentrations of fecal indicator-bacteria have been linked to GI-related health risks [
14], specifically
E. coli concentrations in freshwater [
15].
Heavy precipitation and subsequent stormwater runoff can flush pathogens and other microorganisms directly into nearby surface water, resulting in increased concentrations of bacteria, and increased risk of waterborne disease [
16,
17,
18]. Curriero
et al. [
16] observed that between 1948 and 1994, 51 percent of waterborne outbreaks occurring in the U.S. were preceded by precipitation above the 90th percentile. Additionally, Rose
et al. [
19] observed that between 1971 and 2004, 20 to 40 percent of outbreaks occurring in the U.S. were associated with precipitation above the 90th percentile.
Previous studies have also reported a delayed onset of diarrheal disease following heavy rainfall events [
16,
20,
21,
22]. One explanation for the observed lag could be that the incubation period of waterborne pathogens ranges from one day, for pathogens such as
Shigella, Salmonella, and
Rotavirus, to two weeks for pathogens such as
Cryptosporidium and
E. coli [
23,
24]. In general, cases of GI peak within seven days of exposure to contaminated water [
25,
26].
Under predicted climatic changes, more extreme rain events are expected to occur, particularly in the Great Lakes region, which may increase the risk of poor recreational water quality [
17]. Few epidemiological studies have looked at the effects of precipitation on beach closures and subsequent human health outcomes using time series analysis. This study investigates the association between beach closures and GI-related hospital admissions, comparing multiple smoothing approaches to control for long-term time trends.
While swimmers may be directly impacted by poor recreational water quality, elderly non-swimmers may be exposed to pathogens via drinking water as a result of increased turbidity following extreme events [
22]. Our goal was to characterize the link between extreme precipitation and human health, by first evaluating the association between extreme precipitation and beach closures, and subsequently evaluating the risk of GI-related hospital admissions among the elderly as a function of both extreme precipitation and the occurrence of beach closures. Because recreational water quality data were only available during summer months, we introduce an innovative method to control for long-term time trends in the discontinuous data and evaluate the potential bias of using a discontinuous time-series.
3. Results and Discussion
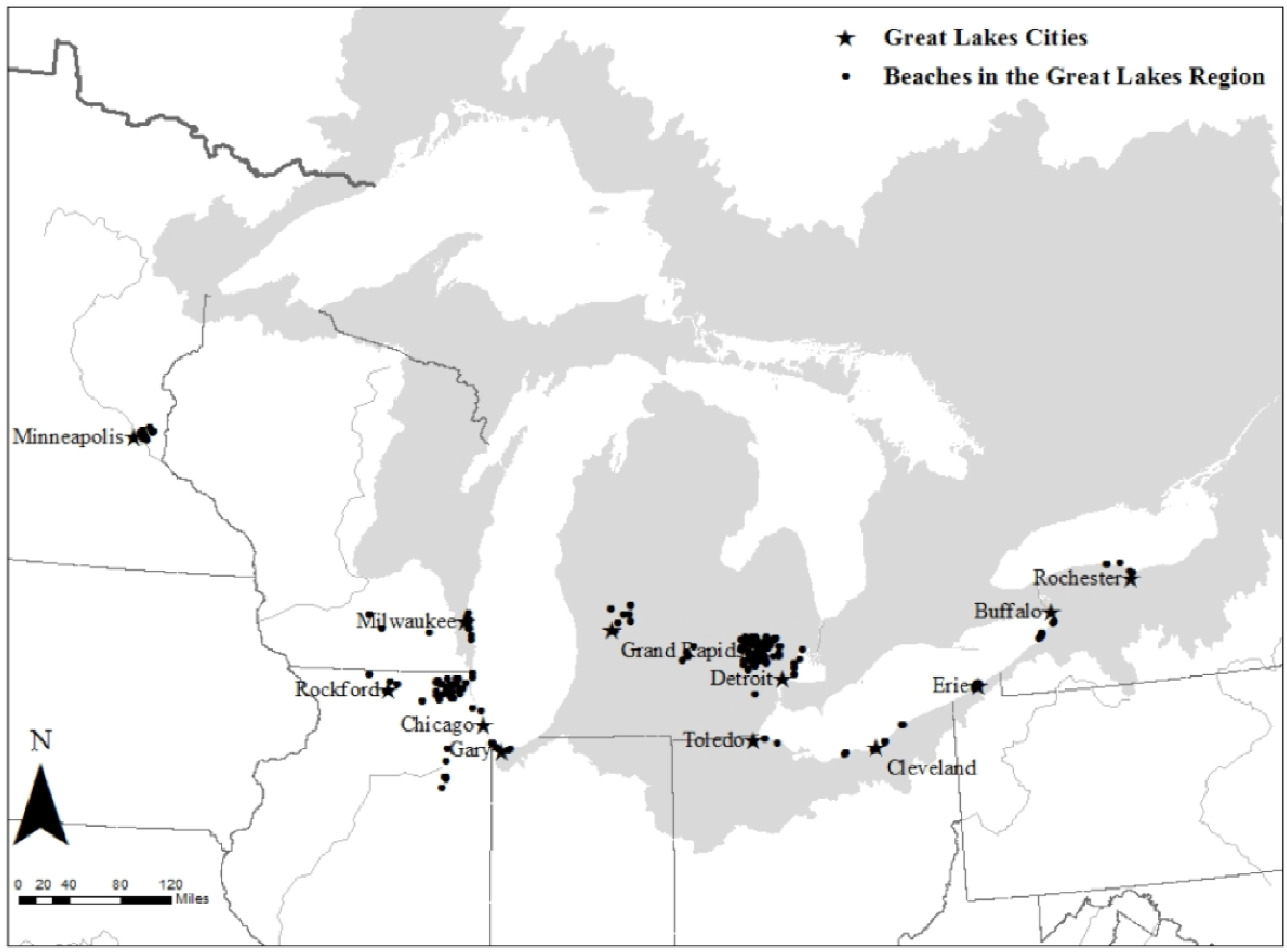
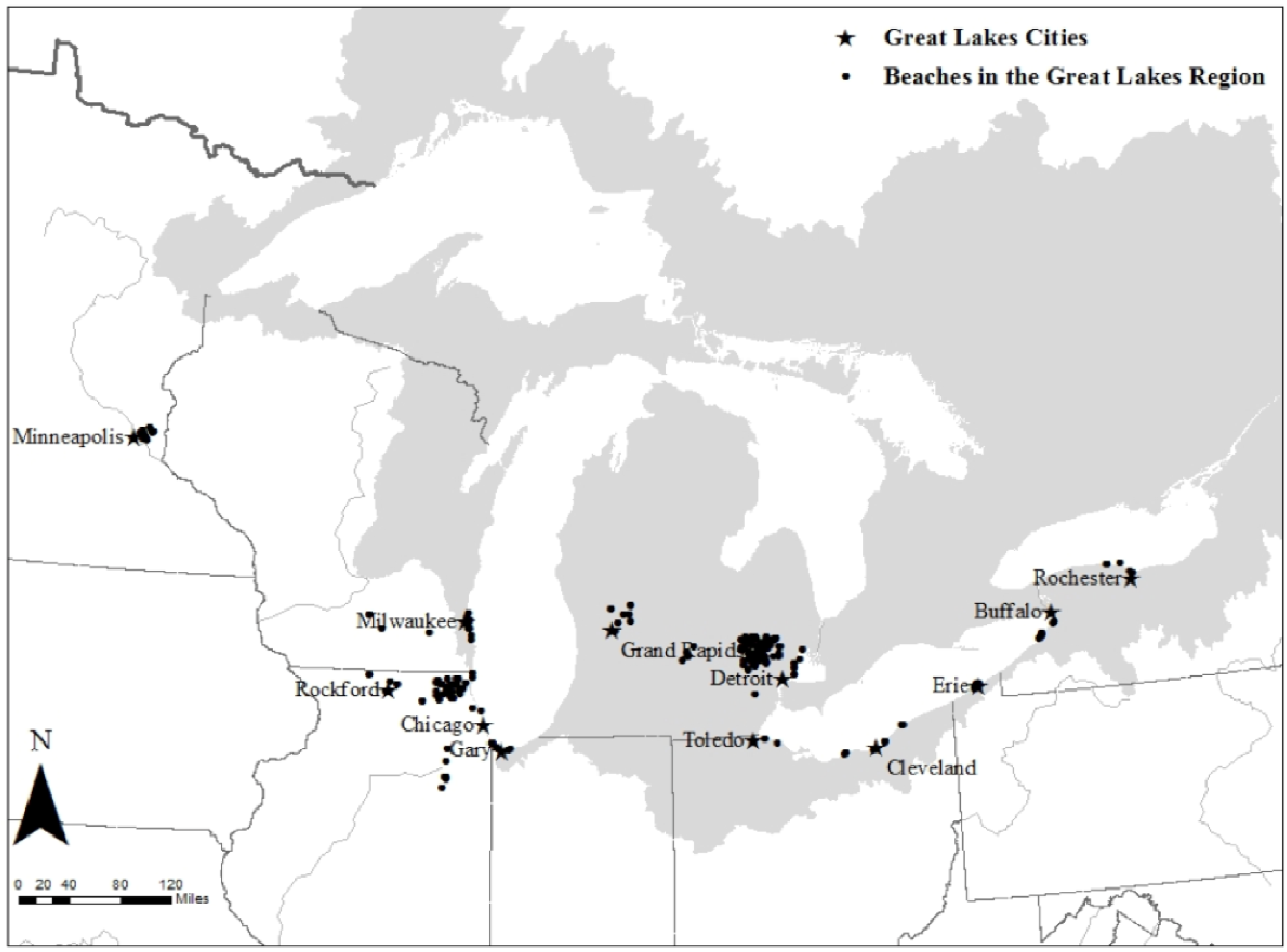
Over the 7-year study period, approximately 40,000 GI-related hospital admissions were recorded among individuals over the age of 65 across 12 cities in the Great Lakes region (
Table 3). The average number of daily GI-related hospital admissions ranged from 0.42 in Erie, PA to 14.47 in Chicago, IL, with an overall daily average of 2.66. From 2000 to 2006, over 100 beach closure days were recorded during the swimming season, defined as May 1st to September 30th. On average, beaches were closed 10% of the time. However, in Chicago, IL; Cleveland, OH; and Milwaukee, WI, beaches were closed over 20% of the time. Daily precipitation during the swimming season in the Great Lakes region ranged from 0 to 4.45 inches (113 mm), with an overall mean daily total of 0.12 inches (3.05 mm). For all 12 cities, precipitation had a skewed distribution, with zero precipitation recorded on nearly 65% of days during the swimming season. Mean daily apparent temperature, for the region, was 19 °C (67 °F). Precipitation and apparent temperature followed consistent seasonal trends throughout the study period across all cities.
Extreme precipitation above the 90th percentile, occurring on the previous day (lag 1), was a significant predictor (
p < 0.05) of beach closures in 8 of the 12 cities (Buffalo, NY; Cleveland, OH; Detroit, MI; Erie, PA; Gary, IN; Milwaukee, WI; Rochester, NY; and Toledo, OH) (
Table 4). However, no consistent trends were observed for the risk of GI-related hospital admissions following a beach closure (
Table 5). In Erie, PA; Minneapolis, MN; Rochester, NY; and Toledo, OH beach closures were positively associated with GI-related hospital admissions among the elderly in at least one of the 7 different lag models. In Buffalo, NY; Chicago, IL; Cleveland, OH; and Detroit, MI, however, the association between beach closures and GI-related hospital admissions indicated a statistically significant inverse relationship in at least one of the seven different lag models. In the four remaining cities Gary, IN; Grand Rapids, MI; Milwaukee, WI; and Rockford, IL no significant associations were found.
In the instances where beach closures were positively associated with GI-related hospital admissions, lags 1, 2, 3, and 7 were significant. Risk ratios ranged from 1.30 (95% confidence interval (CI): 1.00, 1.68) in Rochester at lag 3 to 1.76 (95% CI: 1.13, 2.75) in Minneapolis at lag 1. As a sensitivity analysis, models were re-run with an indicator of cumulative exposure to extreme precipitation (7-day moving average); results were consistent. When the results were pooled across the 12 cities, the overall effect estimate was not significant (
Table 5). The main effect of extreme precipitation on hospital admissions was only significant in two cities: in Chicago at lag 1 with a RR of 1.12 (1.00, 1.24) and in Detroit at lag 6 with a RR of 1.29 (1.06, 1.58) (
Appendix Table A1). The lack of statistical significance may be due to low power related to too few extreme events or too few GI-related hospital admissions.
Table 3.
Summary statistics for 12 Great Lakes cities during the swimming season (1 May–30 September) from 2000 to 2006.
Table 3.
Summary statistics for 12 Great Lakes cities during the swimming season (1 May–30 September) from 2000 to 2006.
| City | Population Over 65a (% of Population) | Mean Daily GI-Related Admissions (per 100,000) | Mean Daily Beach Closures (Total) | Median daily Total Precipitation (mm) (90th Percentile) | Mean daily Apparent Temperature °C (°F) |
|---|
| Buffalo, NY | 151,258 (16) | 1.48 (0.98) | 0.93 (292) | 0.00 (9.40) | 18.99 (66.19) |
| Chicago, IL | 747,777 (11) | 14.47 (1.94) | 0.61 (506) | 0.00 (9.63) | 20.39 (68.71) |
| Cleveland, OH | 284,788 (15) | 4.89 (1.72) | 1.47 (535) | 0.00 (9.63) | 20.22 (68.39) |
| Detroit, MI | 491,592 (12) | 7.35 (1.50) | 0.71 (342) | 0.00 (9.40) | 20.44 (68.80) |
| Erie, PA | 40,256 (14) | 0.42 (1.04) | 0.40 (103) | 0.00 (10.67) | 19.38 (66.89) |
| Gary, IN | 63,234 (13) | 0.95 (1.50) | 0.90 (293) | 0.00 (10.67) | 20.27 (68.49) |
| Grand Rapids, MI | 59,625 (10) | 0.69 (1.16) | 0.43 (15) | 0.00 (11.43) | 19.14 (66.46) |
| Milwaukee, WI | 121,685 (13) | 2.38 (1.96) | 0.90 (376) | 0.00 (9.40) | 19.06 (66.31) |
| Minneapolis, MN | 59,502 (12) | 1.95 (3.28) | 0.23 (17) | 0.00 (10.67) | 19.33 (67.79) |
| Rochester, NY | 95,779 (13) | 0.80 (0.84) | 0.40 (145) | 0.00 (9.65) | 19.29 (66.22) |
| Rockford, IL | 35,450 (13) | 0.51 (1.44) | 0.10 (75) | 0.00 (9.65) | 20.14 (68.26) |
| Toledo, OH | 59,441 (13) | 0.57 (0.96) | 0.44 (115) | 0.00 (9.65) | 20.44 (68.8) |
Table 4.
City-specific odds ratios (OR) with p-values evaluating the association between daily categorical precipitation a at lag 1 (1-day previous) and beach closures in 12 Great Lakes cities from 2000 to 2006.
Table 4.
City-specific odds ratios (OR) with p-values evaluating the association between daily categorical precipitation a at lag 1 (1-day previous) and beach closures in 12 Great Lakes cities from 2000 to 2006.
| Precipitation Category | City-specific OR | City-specific OR | City-specific OR | City-specific OR |
|---|
| | (p-value) | (p-value) | (p-value) | (p-value) |
| | Buffalo, NY | Chicago, IL | Cleveland, OH | Detroit, MI |
| 0 < prcp < 0.01 | 2.42 (0.14) | 1.69 (0.23) | 1.77 (0.30) | 1.28 (0.68) |
| 0.01 ≤ prcp < 90th percentile | 2.94 (<0.001) | 1.34 (0.14) | 1.65 (0.07) | 1.42 (0.13) |
| prcp ≥ 90th percentile | 16.93 (<0.001) | 1.20 (0.41) | 7.39 (0.00) | 4.02 (<0.001) |
| | Erie, PA | Gary, IN | Grand Rapids, MI | Milwaukee, WI |
| 0 < prcp < 0.01 | 0.00 (0.98) | 1.48 (0.70) | - | 0.93 (0.89) |
| 0.01 ≤ prcp < 90th percentile | 2.31 (0.09) | 1.53 (0.15) | 1.71 (0.54) | 1.41 (0.22) |
| prcp ≥ 90th percentile | 10.21 (<0.001) | 2.01 (0.05) | 0.57 (0.64) | 2.01 (0.04) |
| | Minneapolis, MN | Rochester, NY | Rockford, IL | Toledo, OH |
| 0 < prcp < 0.01 | 2.00 (0.59) | 2.67 (0.03) | 0.00 (0.09) | 2.02 (0.29) |
| 0.01 ≤ prcp < 90th percentile | 1.33 (0.75) | 1.91 (0.03) | 0.51 (0.17) | 1.24 (0.55) |
| prcp ≥ 90th percentile | 1.60 (0.50) | 5.67 (<0.001) | 0.66 (0.40) | 9.07 (<0.001) |
Table 5.
City-specific risk ratios a (95% confidence intervals) corresponding to the risk of GI-related hospital admissions among the elderly following beach closures over a 1-week lag using a two-stage spline structure in 12 Great Lakes cities 2000–2006.
Table 5.
City-specific risk ratios a (95% confidence intervals) corresponding to the risk of GI-related hospital admissions among the elderly following beach closures over a 1-week lag using a two-stage spline structure in 12 Great Lakes cities 2000–2006.
| | Buffalo, NY | Chicago, IL | Cleveland, OH | Detroit, MI | Erie, PA |
| lag 1 | 0.96 (0.79, 1.16) | 0.96 (0.91, 1.00) | 0.99 (0.90, 1.09) | 1.01 (0.94, 1.08) | 1.49 (0.90, 2.46) |
| lag 2 | 0.97 (0.79, 1.19) | 1.02 (0.97, 1.07) | 1.05 (0.95, 1.17) | 1.00 (0.93, 1.08) | 1.67 (1.02, 2.76) |
| lag 3 | 1.04 (0.85, 1.28) | 1.00 (0.95, 1.05) | 0.88 (0.80, 0.98) | 0.97 (0.90, 1.05) | 1.15 (0.69, 1.93) |
| lag 4 | 0.98 (0.81, 1.20) | 1.01 (0.96, 1.06) | 0.96 (0.86, 1.06) | 0.99 (0.92, 1.07) | 1.23 (0.70, 2.18) |
| lag 5 | 0.78 (0.63, 0.96) | 1.02 (0.97, 1.07) | 1.02 (0.92, 1.14) | 0.92 (0.86, 0.99) | 0.49 (0.22, 1.06) |
| lag 6 | 0.92 (0.75, 1.12) | 1.02 (0.98, 1.08) | 1.03 (0.93, 1.15) | 0.95 (0.88, 1.02) | 1.54 (0.89, 2.65) |
| lag 7 | 0.92 (0.75, 1.12) | 1.00 (0.96, 1.05) | 0.96 (0.87, 1.06) | 0.97 (0.90, 1.04) | 0.94 (0.52, 1.68) |
| | Gary, IN | Grand Rapids, MI | Milwaukee, WI | Minneapolis, MN | Rochester, NY |
| lag 1 | 0.90 (0.71, 1.15) | 0.70 (0.22, 2.13) | 1.05 (0.89, 1.24) | 1.76 (1.13, 2.75) | 0.84 (0.64, 1.10) |
| lag 2 | 1.08 (0.85, 1.38) | 1.74 (0.74, 4.09) | 1.02 (0.87, 1.20) | 1.13 (0.72, 1.75) | 0.86 (0.65, 1.12) |
| lag 3 | 1.01 (0.80, 1.28) | 1.13 (0.51, 2.51) | 0.99 (0.84, 1.17) | 1.08 (0.68, 1.69) | 1.30 (1.00, 1.68) |
| lag 4 | 1.03 (0.81, 1.31) | 1.26 (0.50, 3.17) | 1.03 (0.88, 1.21) | 0.70 (0.40, 1.22) | 0.96 (0.73, 1.26) |
| lag 5 | 0.99 (0.78, 1.25) | 0.66 (0.17, 2.57) | 1.08 (0.92, 1.27) | 1.14 (0.69, 1.86) | 0.97 (0.74, 1.28) |
| lag 6 | 1.11 (0.87, 1.41) | 1.49 (0.49, 4.50) | 0.99 (0.84, 1.16) | 1.10 (0.73, 1.67) | 1.03 (0.79, 1.35) |
| lag 7 | 0.87 (0.69, 1.11) | 2.41 (0.75, 7.77) | 1.07 (0.91, 1.26) | 0.75 (0.51, 1.10) | 1.19 (0.92, 1.53) |
| | Rockford, IL | Toledo, OH | Pooled-Estimate | | |
| lag 1 | 1.11 (0.67, 1.82) | 0.97 (0.68, 1.38) | 0.98 (0.95, 1.01) | | |
| lag 2 | 0.78 (0.42, 1.43) | 0.70 (0.47, 1.02) | 1.01 (0.98, 1.05) | | |
| lag 3 | 0.83 (0.46, 1.50) | 1.13 (0.77, 1.65) | 0.98 (0.95, 1.02) | | |
| lag 4 | 1.04 (0.62, 1.74) | 0.64 (0.43, 0.97) | 1.00 (0.96, 1.03) | | |
| lag 5 | 1.35 (0.85, 2.13) | 1.03 (0.71, 1.48) | 0.99 (0.95, 1.02) | | |
| lag 6 | 0.77 (0.42, 1.43) | 1.01 (0.71, 1.45) | 1.01 (0.97, 1.04) | | |
| lag 7 | 1.30 (0.81, 2.10) | 1.67 (1.22, 2.30) | 0.99 (0.96, 1.03) | | |
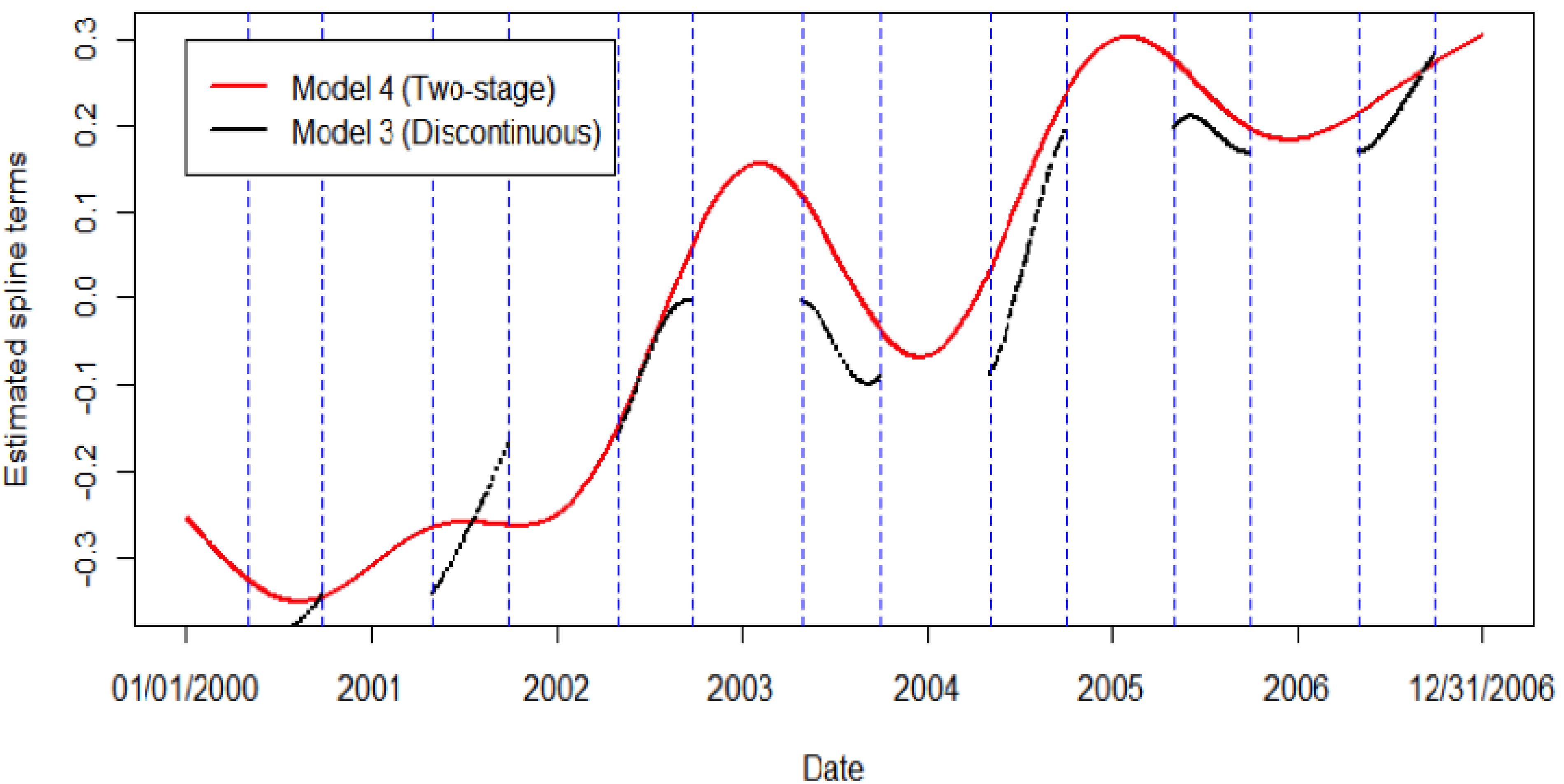
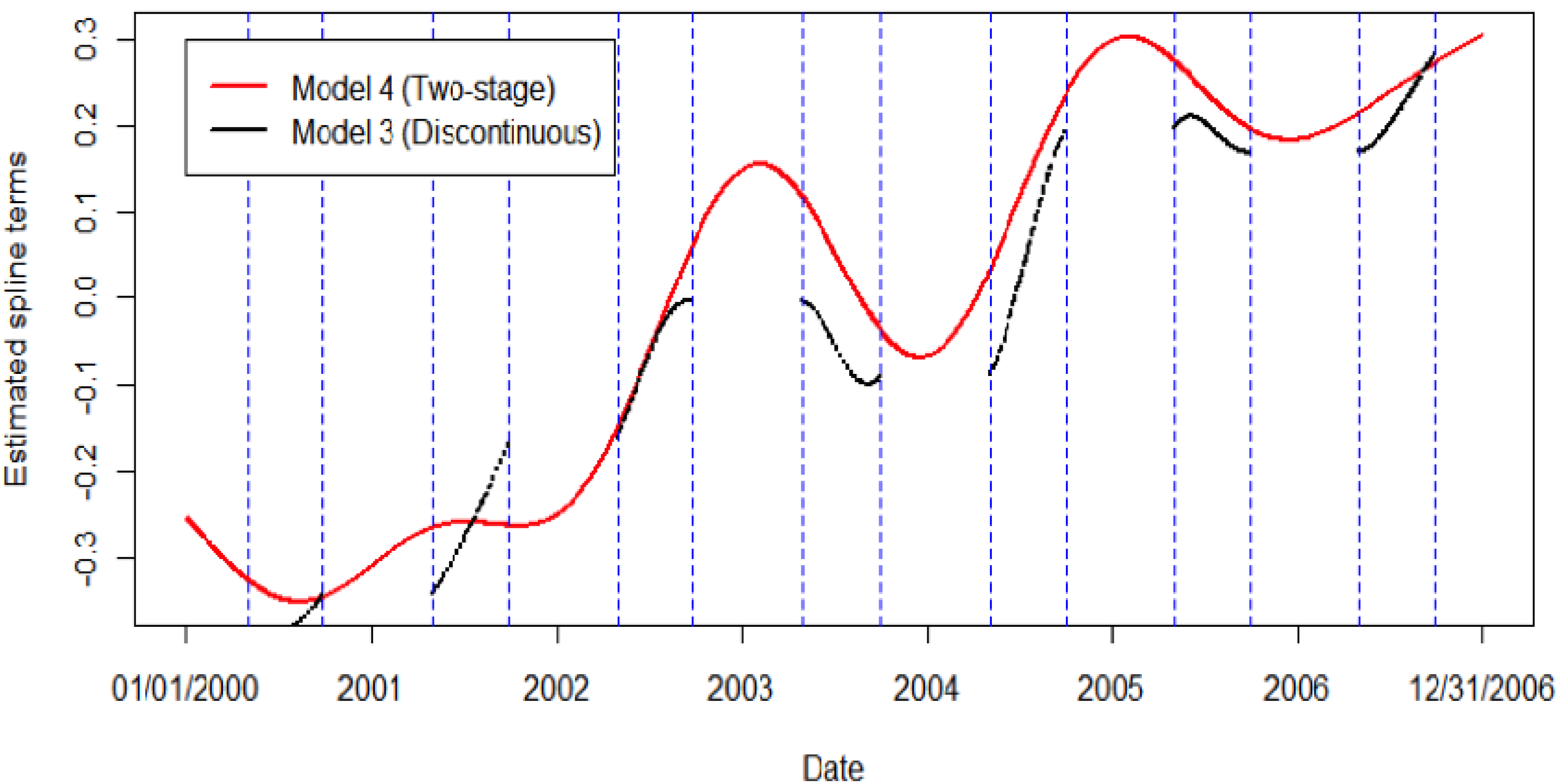
Comparing the different spline structures, no significant differences were observed. In cities where a significant association was observed in at least one of the seven different lag models, that association was consistent across spline structures (
Appendix Table A2). In cities where no association was observed for any lag, that also remained consistent across spline structures. While the different spline structures used to control long-term time trends did not alter the significance or magnitude of the associations reported, there was an observable difference between the two different spline estimates (
Figure 2). Using Detroit as an example, the spline estimated from the discontinuous time-series was unique compared to the spline estimated from the entire time-series in the two-stage analysis. In all instances, the spline estimated from the entire time-series was numerically different from that estimated from the discontinuous time-series.
Figure 2.
The discontinous, summer-only spline compared to the spline estimated using the entire 7-year time-series in the two-stage spline model, using Detroit, MI as an example.
Figure 2.
The discontinous, summer-only spline compared to the spline estimated using the entire 7-year time-series in the two-stage spline model, using Detroit, MI as an example.
In general, extreme precipitation, above the 90th percentile, at lag 1, was a significant predictor of beach closures in 8 of the 12 cities. However, no consistent association between beach closures and GI-related hospital admissions among the elderly was observed. In this study, novel methodology to control for long-term time trends using season-specific data was proposed and results using three different spline structures were compared. While no significant differences in the effect estimates were observed in this analysis, the two-stage Poisson model, which utilizes the full time-series to control for long-term time trends in the outcome variable, is recommended for future work focused on season-specific analyses.
The two-stage spline structure presented in Model 4 can be applied to a variety of studies where only one season is of interest. By comparing results from the two-stage spline model to results from a model with no spline, as well as a model with a spline estimated from the discontinuous, summer-only time-series, we addressed an important methodological question regarding the most appropriate way to conduct time-series analysis when exposure data is only available for a portion of the year. Results, in this case, did not differ markedly across the three different modeling approaches. One explanation may be that GI-related hospital admissions did not display significant variability between summer, the season of interest, and the rest of the year. Differences in effect estimates are more likely to be observed between the discontinuous time-series model and a two-stage time-series model when the health outcome varies across seasons. If hospital admissions had shown more variability across seasons, the two-stage spline structure would have minimized confounding by long-term time trends and reduced potential bias.
Although the results presented here do not reveal a consistent or significant association between beach closures and GI-related hospital admissions, previous research states that poor recreational water quality has the potential to adversely impact human health. Previous research confirms that precipitation is linked to water quality indicators such as
E. coli concentrations and turbidity [
9,
36].
E. coli concentrations in recreational waters are estimated to peak approximately 24 to 72 hours following precipitation events in the Great Lakes region [
11,
13]. Previous research has also reported a delayed onset of diarrheal disease following extreme precipitation and related increases in water quality indicators [
16,
19,
21,
22,
50,
51].
While Sampson
et al. [
52] found no association between rainfall and bacteria at any of their 15 sites along the Wisconsin shores of Lake Superior (water samples were taken following any rain event of at least 0.25 inches (6.35 mm)), our study evaluated extreme precipitation events, above the 90th percentile (0.40 inches (10.16 mm)). These extreme events were found to be a significant predictor of recreational water quality in a majority of cities. Results from a specific location should not necessarily be used to make decisions regarding beach closures at other locations [
52]. For example, Haack
et al. [
36] concluded that rainfall 48 to 72 hours prior was significantly associated with
E. coli concentrations at three Southern beaches in Grand Traverse Bay in Lake Michigan, but only 24 h prior at Western and Eastern beach locations.
Results from our analysis suggest that precipitation should be modeled in a way that accommodates the skewed distribution and the nonlinear associations often observed between precipitation and daily hospital admissions. Modeling precipitation as a categorical variable, as we did, is a suitable approach.
One of the primary limitations of this analysis is related to data specificity; GI-related hospital admissions are dramatically underreported and the etiology is rarely identified [
53,
54]. The symptoms associated with exposure to contaminated recreational water are relatively broad-spectrum symptoms. Therefore, it is challenging to observe direct associations between exposure and outcome. Additionally, the period of interest is quite limited: on average only 35% of summer days had measurable amounts of precipitation. Further, recreational water quality monitoring was not consistent over the study period. Use of a binomial indicator for beach closings may have biased results towards the null. This binary coding also fails to differentiate between when one beach was closed and ten beaches were closed for a particular city, such misclassification may make it more difficult to identify a significant association. The absence of an association between extreme precipitation and GI-related hospitalization could also be due to infrequent use of and limited exposure to surface waters for recreation by Medicare beneficiaries.
Lastly, it is important to note that precipitation can be much localized; use of single city monitoring stations did not allow for spatially explicit analysis. However, a major strength of this analysis was its use of publicly available data across a wide geographic area to explore the impact of extreme precipitation on beach closures and subsequent risk of waterborne disease, which has implications for recreational water management at the local level.
This study was conducted to evaluate whether beach closure and Medicare data, both easily accessible, could be used as a proxy for evaluating risk of GI. The development of such a universal model would help beach managers and public health professionals assess risk across a wide geographic area and prioritize resources accordingly. Because the association between recreational water quality and hospital admissions was only being investigated in select cities in the Great Lakes region, conclusions may not be applicable to marine or estuarine recreational waters or other regions of the country where socio-demographic, meteorological, and hydrodynamic conditions may vary.
Future work in this area should promote the use of a consistent definition of extreme precipitation so that decision-makers can have a shared understanding of the risks associated with heavy precipitation events. Our results linking extreme precipitation to beach closures provide additional support for precipitation-based public health warning systems [
55].


{kind=link}
{kind=link}