A Population-Based Case-Control Study of Drinking-Water Nitrate and Congenital Anomalies Using Geographic Information Systems (GIS) to Develop Individual-Level Exposure Estimates

Abstract
:1. Introduction
2. Experimental Section
2.1. Research Ethics Board Approvals
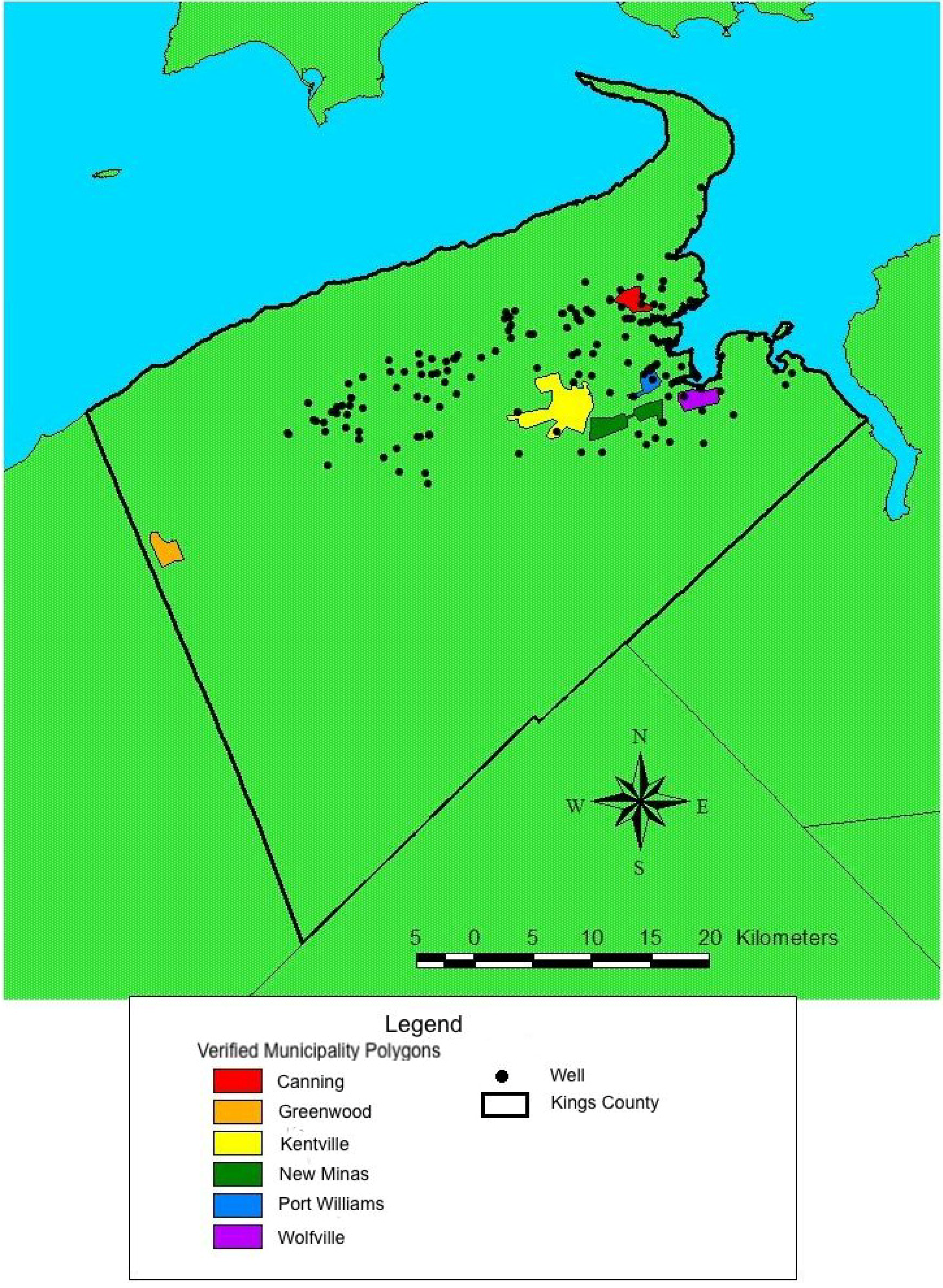
2.2. Study Area

{kind=link}
{kind=link}
| Location | Water Source | # of Sample Locations | Total # of Samples | Min. [Nitrate] | Max. [Nitrate] | Mean [Nitrate] * | Median [Nitrate) | Nitrate Exposure Level |
|---|---|---|---|---|---|---|---|---|
| All rural wells | Groundwater | 140 | 1,113 | 0.0 | 43.0 | 6.44 (5.99–6.89) | 3.8 | n/a |
| All municipalities | Ground and surface water | 20 | 53 | 0.0 | 10.4 | 2.03 (1.58–2.48) | 1.7 | n/a |
| Canning | Groundwater | 2 | 24 | 1.0 | 2.5 | 1.63 (1.47–1.80) | 1.7 | 1.0–5.56 |
| Greenwood | Groundwater | 2 | 5 | 0.0 | 1.0 | 0.63 (0.12–1.14) | 0.9 | <1.0 |
| Kentville | Surfacewater | 1 | 2 | 0.4 | 1.0 | 0.69 (0.00–4.28) | 0.7 | <1.0 |
| New Minas | Groundwater | 9 | 10 | 1.0 | 2.9 | 1.68 (1.92–2.07) | 1.6 | 1.0–5.56 |
| Port Williams | Groundwater | 4 | 6 | 1.4 | 10.4 | 5.08 (1.64–8.52) | 4.6 | 1.0–5.56 |
| Wolfville | Groundwater | 2 | 6 | 2.4 | 3.6 | 2.77 (2.33–3.21) | 2.7 | 1.0–5.56 |
2.3. Data Sources
2.4. Inclusion and Exclusion Criteria
2.5. Demographic and Health Data Collection
2.6. Nitrate Concentration Measurement


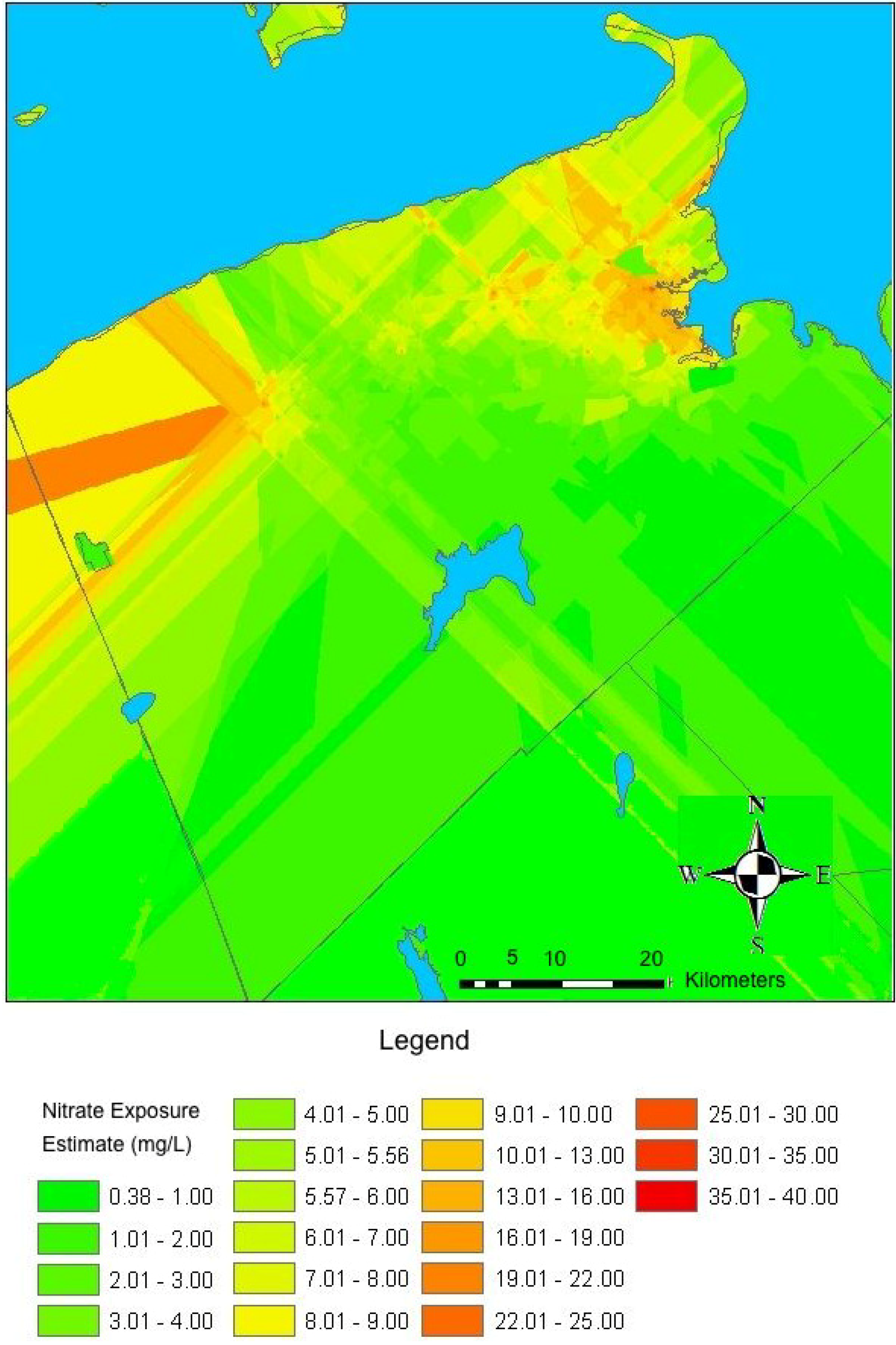
2.7. Exposure Assessment
2.8. Statistical Analyses
3. Results and Discussion
3.1. Results
| Class of Anomaly | Entire Study Period | Before Folate Fortification | After Folate Fortification | |||
|---|---|---|---|---|---|---|
| 1987–2006 | 1987–997 | 1998–2006 | ||||
| Number of cases | Percentage of all congenital anomalies | Number of cases | Percentage of all congenital anomalies for period | Number of cases | Percentage of all congenital anomalies for period | |
| All Anomalies | 606 | 100 | 300 | 100 | 306 | 100 |
| Central Nervous System | 286 | 47 | 98 | 33 | 188 | 61 |
| Musculoskeletal System | 101 | 17 | 58 | 19 | 43 | 14 |
| Genitourinary System | 50 | 8 | 25 | 8 | 25 | 8 |
| Cardiovascular System | 47 | 8 | 26 | 9 | 21 | 7 |
| Inguinal Canal | 37 | 6 | 26 | 9 | 11 | 4 |
| Multiple Anomalies | 33 | 5 | 24 | 8 | 9 | 3 |
| Eye, Ear, Nose, Throat and Mouth | 27 | 4 | 17 | 6 | 10 | 3 |
| Other | 27 | 3 | 16 | 5 | 11 | 4 |
| Missing | 53 | 9 | 53 | 18 | 0 | 0 |
| Variable | Cases (n = 606) | Controls (n = 1,635) | Crude Odds Ratio ** | p-value * | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Sex | 0.91 | |||||
| Female | 268 | 48 | 788 | 48 | 1.0 | |
| Male | 285 | 52 | 847 | 52 | 0.99 (0.82–1.20) | |
| Missing | 53 | 0 | ||||
| Season of conception | 0.96 | |||||
| Winter | 83 | 14 | 244 | 15 | 1.0 | |
| Spring | 139 | 15 | 393 | 24 | 1.04 (0.76–1.43) | 0.63 |
| Summer | 162 | 25 | 484 | 30 | 0.98 (0.73–1.34) | 0.87 |
| Fall | 169 | 29 | 514 | 31 | 0.97 (0.71–1.31) | 0.70 |
| Missing | 53 | 0 | ||||
| Year of Conception | ||||||
| 1987–1991 | 83 | 15 | 245 | 15 | 1.0 | |
| 1992–1996 | 113 | 20 | 342 | 21 | 0.98 (0.70–1.35) | 0.75 |
| 1997–2001 | 282 | 51 | 838 | 51 | 0.99 (0.75–1.32) | 0.87 |
| 2002–2006 | 75 | 14 | 210 | 13 | 1.05 (0.73–1.52) | 0.67 |
| Missing | 53 | 0 | ||||
| Parity | 0.01 | |||||
| 0 | 273 | 49 | 687 | 42 | 1.0 | |
| 1–2 | 252 | 46 | 852 | 52 | 0.74 (0.61–0.91) | 0.29 |
| 3+ | 28 | 5 | 96 | 6 | 0.73 (0.47–1.14) | 0.46 |
| Missing | 53 | 0 | ||||
| Pre-pregnancy weight (kg) | 0.55 | |||||
| <50 | ||||||
| 50–69 | 44 | 9 | 129 | 9 | 1.02 (0.70–1.47) | 0.68 |
| ≥70 | 281 | 59 | 837 | 56 | 1.0 | |
| Missing | 155 | 32 | 520 | 35 | 0.89 (0.71–1.11) | 0.33 |
| 126 | 149 | |||||
| Smoker | ||||||
| No | 358 | 59 | 1140 | 70 | 1.0 | |
| Yes | 248 | 41 | 495 | 30 | 1.60 (1.32–1.94) | <0.001 |
| Thyroid | ||||||
| No | 604 | 1,626 | 99 | 1.0 | ||
| Yes | 2 | 100 | 9 | 1 | 0.60 (0.13–2.78) | 0.51 |
| Folate supplementation | ||||||
| No | 111 | 58 | 317 | 57 | 1.0 | 0.74 |
| Yes | 79 | 42 | 239 | 43 | 0.94 (0.67–1.32) | 0.74 |
| Missing | 416 | 1,079 | ||||
| Folate Fortification | ||||||
| No | 300 | 50 | 740 | 45 | 1.0 | |
| Yes | 306 | 50 | 895 | 55 | 0.84 (0.70–1.02) | 0.07 |
| Water source | ||||||
| Surface | 118 | 19 | 304 | 19 | 1.0 | |
| Ground | 488 | 81 | 1,331 | 81 | 0.95 (0.75–1.20) | 0.64 |
| Municipal water | ||||||
| Yes | 245 | 40 | 609 | 37 | 1.0 | |
| No | 361 | 60 | 1,026 | 63 | 0.88 (0.72–1.06) | 0.17 |
| Nitrate exposure level | ||||||
| <1 mg/L | 127 | 21 | 353 | 22 | 1.0 | |
| 1–5.56 mg/L | 351 | 58 | 931 | 57 | 1.02 (0.81–1.30) | 0.68 |
| >5.56 mg/L | 127 | 21 | 351 | 21 | 0.97 (0.73–1.29) | 0.71 |
| Variable | Basic Model: Matching Variables | Basic Model Plus Maternal Demographic Variables | Basic Model Plus Maternal Demographic and Health Variables | Basic Model Plus Maternal Demographic, Health and Water Source Variables | Final Model: Effect of Nitrate Exposure Level on Congenital Anomalies after Controlling for All Other Variables |
|---|---|---|---|---|---|
| Sex | |||||
| Female | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Male | 0.99 (0.82–1.20) | 0.99 (0.82–1.21) | 0.98 (0.81–1.20) | 0.99 (0.81–1.20) | 0.98 (0.81–1.20) |
| Season of conception | |||||
| Winter | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Spring | 1.04 (0.76–1.43) | 1.05 (0.76–1.44) | 1.05 (0.76–1.44) | 1.05 (0.76–1.44) | 1.05 (0.76–1.44) |
| Summer | 0.97 (0.72–1.34) | 0.99 (0.72–1.34) | 1.00 (0.73–1.37) | 1.00 (0.74–1.37) | 1.00 (0.74–1.37) |
| Fall | 0.97 (0.72–1.32) | 0.96 (0.72–1.27) | 0.97 (0.71–1.32) | 0.97 (0.71–1.32) | 0.98 (0.72–1.33) |
| Year of conception | |||||
| 1987–1991 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 1992–1996 | 0.98 (0.71–1.36) | 0.97 (0.70–1.36) | 0.98 (0.71–1.37) | 0.99 (0.71–1.38) | 0.99 (0.71–1.38) |
| 1997–2001 | 1.00 (0.71–1.36) | 0.96 (0.72–1.27) | 0.97 (0.73–1.29) | 0.98 (0.74–1.31) | 1.00 (0.75–1.34) |
| 2002–2006 | 1.05 (0.73–1.51) | 1.02 (0.70–1.45) | 1.02 (0.71–1.48) | 1.03 (0.72–1.49) | 1.05 (0.72–1.52) |
| Maternal age | |||||
| <20 | 1.01 (0.71–1.44) | 0.94 (0.66–1.35) | 0.94 (0.66–1.35) | 0.95 (0.66–1.36) | |
| 20–34 | 1.0 | 1.0 | 1.0 | 1.0 | |
| ≥35 | 1.38 (1.01–1.88) | 1.40 (1.02–1.91) | 1.39 (1.02–1.91) | 1.40 (1.02–1.91) | |
| Parity | |||||
| 0 | 1.0 | 1.0 | 1.0 | 1.0 | |
| 1–2 | 0.73 (0.60–0.90) | 0.73 (0.59–0.89) | 0.73 (0.59–0.89) | 0.73 (0.60–0.90) | |
| 3+ | 0.68 (0.43–1.07) | 0.67 (0.43–1.06) | 0.68 (0.43–1.07) | 0.70 (0.43–1.06) | |
| Smoker | |||||
| No | 1.0 | 1.0 | 1.0 | ||
| Yes | 1.28 (1.03–1.57) | 1.28 (1.03–1.57) | 1.27 (1.03–1.57) | ||
| Diabetes | |||||
| No | 1.0 | 1.0 | 1.0 | ||
| Gestational | 1.30 (0.70–2.41) | 1.29 (0.70–2.40) | 1.31 (0.71–2.44) | ||
| Other diabetes | 0.97 (0.34–2.73) | 0.97 (0.34–2.73) | 0.96 (0.34–2.70) | ||
| Thyroid disease | |||||
| No | 1.0 | 1.0 | 1.0 | ||
| Yes | 0.64 (0.14–3.00) | 0.65 (0.14–3.05) | 0.64 (0.14–3.01) | ||
| Water source | |||||
| Surface | 1.0 | 1.0 | |||
| Ground | 0.85 (0.66–1.09) | 0.70 (0.35–1.41) | |||
| Municipal water | |||||
| Yes | 1.0 | 1.0 | |||
| No | 1.10 (0.81–1.51) | 0.82 (0.63–1.07) | |||
| Nitrate exposure level | |||||
| <1 mg/L | 1.0 | ||||
| 1–5.56 mg/L | 1.65 (0.83–3.27) | ||||
| >5.56 mg/L | 1.66 (0.81–3.42) |
3.2. Discussion
| Variable | Cases and Controls Conceived from 1987–1997 (n = 987) | Cases and Controls Conceived from 1998–2006 (n = 1,201) |
|---|---|---|
| Sex | ||
| Female | 1.0 | 1.0 |
| Male | 1.0 (0.75–1.34) | 0.96 (0.73–1.24) |
| Season of conception | ||
| Winter | 1.0 | 1.0 |
| Spring | 1.0 (0.61–1.63) | 1.12 (0.73–1.71) |
| Summer | 1.01 (0.62–1.63) | 1.01 (0.67–1.53) |
| Fall | 0.98 (0.62–1.55) | 0.98 (0.64–1.50) |
| Year of conception | ||
| 1987–1991 | 1.0 | – |
| 1992–1996 | 0.96 (0.69–1.35) | – |
| 1997–2001 | 0.94 (0.62–1.42) | 1.0 |
| 2002–2006 | – | 1.02 (0.75–1.39) |
| Maternal age | ||
| <20 | 0.85 (0.50–1.43) | 1.01 (0.61–1.68) |
| 20–34 | 1.0 | 1.0 |
| ≥35 | 1.35 (0.76–2.39) | 1.50 (1.03–2.19) |
| Parity | ||
| 0 | 1.0 | 1.0 |
| 1–2 | 0.77 (0.56–1.05) | 0.68 (0.52–0.90) |
| 3+ | 0.75 (0.39–1.45) | 0.59 (0.31–1.11) |
| Smoker | ||
| No | 1.0 | 1.0 |
| Yes | 1.01 (0.74–1.38) | 1.55 (1.16–2.06) |
| Thyroid disease | ||
| No | 1.0 | 1.0 |
| Yes | 1.55 (0.13–18.10) | 0.36 (0.04–3.01) |
| Diabetes | ||
| No | 1.0 | 1.0 |
| Gestational | 1.63 (0.73–3.64) | 2.27 (0.30–16.71) |
| Other diabetes | 0.49 (0.06–4.15) | – |
| Water source | ||
| Surface | 1.0 | 1.0 |
| Ground | 2.50 (0.62–10.08) | 0.54 (0.23–1.29) |
| Municipal | ||
| Yes | 1.0 | 1.0 |
| No | 0.78 (0.53–1.14) | 0.82 (0.56–1.20) |
| Nitrate Exposure level | ||
| <1 mg/L | 1.0 | 1.0 |
| 1–5.56 mg/L | 0.48 (0.10–1.60) | 2.44 (1.05–5.66) |
| >5.56 mg/L | 0.47 (0.11–1.90) | 2.25 (0.92–5.52) |
3.2.1. Study Strengths
3.2.2. Study Limitations
4. Conclusions
List of Abbreviations
| CNS | Central Nervous System |
| FAD | Fetal Anomaly Database |
| GIS | Geographic Information Systems |
| MAC | Maximum Allowable Concentration |
| NSAPD | Nova Scotia Atlee Perinatal Database |
Supplementary Files
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Congenital Anomalies in Canada; Health Canada: Ottawa, Canada, 2002; pp. 1–87.
- Dodds, L.; Seviour, R. Congenital anomalies and other birth outcomes among infants born to women living near a hazardous waste site in Sydney, Nova Scotia. Can. J. Publ. Health-Rev. Can. San. 2001, 92, 331–334. [Google Scholar]
- World Health Organization. Rolling Revision of the WHO Guidelines for Drinking-water Quality: Nitrates and Nitrates in Drinking-water. 2004. Available online: http://www.who.int/water_sanitation_health/dwq/chemicals/en/nitrateschap1.pdf (accessed on 2 October 2007).
- Health Canada. Nitrate/Nitrite. 1992. Available online: http://www.hc-sc.gc.ca/ewh-semt/pubs/water-eau/doc_sup-appui/nitrate_nitrite/index_e.html#Guideline (accessed on 26 January 2006).
- Fields, S. Global nitrogen: Cycling out of control. Environ. Health Perspect. 2004, 112, 557–563. [Google Scholar]
- Bruning-Fann, C.S.; Kaneene, J.B. The effects of nitrate, nitrite and N-nitroso compounds on human health: A review. Vet. Hum. Toxicol. 1993, 35, 521–538. [Google Scholar]
- Fan, A.M.; Willhite, C.C.; Book, S.A. Evaluation of the nitrate drinking water standard with reference to infant methemoglobinemia and potential reproductive toxicity. Regul. Toxicol. Pharmacol. 1987, 7, 135–148. [Google Scholar] [CrossRef]
- Givelber, H.M.; DiPaolo, J.A. Teratogenic effects of N-Ethyl-N-nitrosourea in the syrian hamster. Cancer Res. 1969, 29, 1151–1155. [Google Scholar]
- Inouye, M.; Murakami, U. Teratogenic effect of N-Methyl-N'-nitrosoguanidine in mice. Teratology 1978, 18, 263–268. [Google Scholar] [CrossRef]
- Koyama, T.; Handa, J.; Handa, H.; Matsumoto, S. Methylnitrosourea-induced malformations of brain in SD-JCL rat. Arch. Neurol. 1970, 22, 342–343. [Google Scholar] [CrossRef]
- Dorsch, M.M.; Scragg, R.K.; McMichael, A.J.; Baghurst, P.A.; Dyer, K.F. Congenital malformations and maternal drinking water supply in rural South Australia: A case-control study. Amer. J. Epidemiol. 1984, 119, 473–486. [Google Scholar]
- Arbuckle, T.E.; Sherman, G.J.; Corey, P.N.; Walters, D.; Lo, B. Water nitrates and CNS birth defects: A population-based case-control study. Arch. Environ. Health 1988, 43, 162–167. [Google Scholar] [CrossRef]
- Croen, L.A.; Todoroff, K.; Shaw, G.M. Maternal exposure to nitrate from drinking water and diet and risk for neural tube defects. Amer. J. Epidemiol. 2001, 153, 325–331. [Google Scholar] [CrossRef]
- Cedergren, M.I.; Selbing, A.J.; Lofman, O.; Kallen, B.J. Chlorination byproducts and nitrate in drinking water and risk for congenital cardiac defects. Environ. Res. 2002, 89, 124–130. [Google Scholar] [CrossRef]
- Manassaram, D.M.; Backer, L.C.; Moll, D.M. A review of nitrates in drinking water: Maternal exposure and adverse reproductive and developmental outcomes. Environ. Health Perspect. 2006, 114, 320–327. [Google Scholar] [CrossRef]
- Trescott, P.C. Groundwater Resources and Hydrogeology of the Annapolis-Cornwallis Valley, Nova Scotia; Halifax: Nova Scotia, AB, Canada, 1968. [Google Scholar]
- Rivard, C.; Deblonde, C.; Boivin, R.; Boldue, A.; Paradis, S.J.; Liao, S.; Gauthier, M-J.; Blackmore, A.; Trepanier, S.; Castonguay, S.; et al. Canadian Groundwater Inventory: Hydrogeological Atlas of the Annapolis Valley, Nova Scotia. Geological Service of Canada: Ottawa, ON, Canada, 2007. [Google Scholar]
- The Municipality of the County of Kings. Water Utility. 2005. Available online: http://www.county.kings.ns.ca/engpw/watutil.htm (accessed on 13 July 2006).
- Wolfville Water Utility. Public Information Brochure. 2002. Available online: http://www.town.wolfville.ns.ca/forms/waterbrochurejan2002.pdf (accessed on 17 April 2006).
- The Town of Kentville. Kentville Water Commission. 2006. Available online: http://www.town.kentville.ns.ca/water.pdf (accessed on 12 July 2006).
- The Town of Port Williams. Nova Scotia Port Williams Industrial Park. 2004. Available online: http://www.targetnovascotia.com/IPPDF/PortWilliams.pdf (accessed on 12 July 2006).
- Province of Nova Scotia. Nova Scotia Civic Address File (NSCAF). 2008. Available online: http://www.gov.ns.ca/snsmr/land/projects/civic/ (accessed on 15 April 2008).
- Benson, V.S.; VanLeeuwen, J.A.; Sanchez, J.; Dohoo, I.R.; Somers, G.H. Spatial analysis of land use impact on ground water nitrate concentrations. J. Environ. Qual. 2006, 35, 421–432. [Google Scholar] [CrossRef]
- Ruckart, P.Z.; Henderson, A.K.; Black, M.L.; Flanders, W.D. Are nitrate levels in groundwater stable over time? J. Expo. Sci. Environ. Epidemiol. 2008, 18, 129–133. [Google Scholar]
- Briggins, D.R.; Moerman, D.E. Pesticides, nitrate-N and bacteria in farm wells of King’s County, Nova Scotia. Water Qual. Res. J. Can. 1995, 30, 429–442. [Google Scholar]
- Aller, L.; Bennett, T.; Lehr, J.H.; Petty, R.J.; Hackett, G. DRASTIC: A Standardized System for Evaluating Ground Water Pollution Potential using Hydrogeologic Settings; EPA: Ada, OK, USA, 1987. [Google Scholar]
- Levallois, P.; Theriault, M.; Rouffignat, J.; Tessier, S.; Landry, R.; Ayotte, P.; Girard, M.; Gauvin, D.; Gingras, S.; Chiasson, C. Groundwater contamination by nitrates associated with intensive potato culture in Quebec. Sci. Total Envir. 1998, 217, 91–101. [Google Scholar] [CrossRef]
- Rudolph, D.L.; Barry, D.A.J.; Goss, M.J. Contamination in Ontario farmstead domestic wells and its association with agriculture: Results from multilevel monitoring well installations. J. Contam. Hydrol. 1998, 32, 295–311. [Google Scholar] [CrossRef]
- Woods, S.E.; Raju, U. Maternal smoking and the risk of congenital birth defects: A cohort study. J. Am. Board Fam. Med. 2001, 14, 330–334. [Google Scholar]
- Morales-Suarez-Varela, M.; Bille, C.; Christensen, K.; Olsen, J. Smoking habits, nicotine use, and congenital malformations. Obstet. Gynecol. 2006, 107, 51–57. [Google Scholar] [CrossRef]
- Malloy, M.H.; Kleinman, J.C.; Bakewell, J.M.; Schramm, W.F.; Land, G.H. Maternal smoking during pregnancy: No association with congenital malformations in Missouri 1980–1983. Amer. J. Public Health 1989, 79, 1243–1246. [Google Scholar] [CrossRef]
- Carmichael, S.L.; Shaw, G.M.; Laurent, C.; Olney, R.S.; Lammer, E.J. Maternal reproductive and demographic characteristics as risk factors for hypospadias. Paediatr. Perinat. Epidemiol. 2007, 21, 210–218. [Google Scholar] [CrossRef]
- Akre, O.; Lipworth, L.; Cnattingius, S.; Sparen, P.; Ekbom, A. Risk factor patterns for cryptorchidism and hypospadias. Epidemiology 1999, 10, 364–369. [Google Scholar] [CrossRef]
- Persad, V.L.; van den Hof, M.C.; Dube, J.M.; Zimmer, P. Incidence of open neural tube defects in Nova Scotia after folic acid fortification. Can. Med. Assn. J. 2002, 167, 241–245. [Google Scholar]
- Ericson, A.; Kallen, B.; Lofkvist, E. Environmental factors in the etiology of neural tube defects: A negative study. Environ. Res. 1988, 45, 38–47. [Google Scholar] [CrossRef]
- Mattix, K.D.; Winchester, P.D.; Scherer, L.R. Incidence of abdominal wall defects is related to surface water atrazine and nitrate levels. J. Pediat. Surg. 2007, 42, 947–949. [Google Scholar] [CrossRef]
- Brender, J.D.; Olive, J.M.; Felkner, M.; Suarez, L.; Marckwardt, W.; Hendricks, K.A. Dietary nitrites and nitrates, nitrosatable drugs, and neural tube defects. Epidemiology 2004, 15, 330–336. [Google Scholar] [CrossRef]
- Moerman, D.; Briggins, D. Nova Scotia Farm Well Water Quality Assurance Study Final Report; Province of Nova Scotia: Halifax, NS, Canada, 1994.
- Blair, K. Temporal and Spatial Profiles of Groundwater Nitrate Concentration in Kings County, Nova Scotia. Master Thesis, Dalhousie University, Halifax, NS, Canada, 2001. [Google Scholar]
- Nuckols, J.R.; Ward, M.H.; Jarup, L. Using geographic information systems for exposure assessment in environmental epidemiology studies. Environ. Health Perspect. 2004, 112, 1007–1015. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Holtby, C.E.; Guernsey, J.R.; Allen, A.C.; VanLeeuwen, J.A.; Allen, V.M.; Gordon, R.J. A Population-Based Case-Control Study of Drinking-Water Nitrate and Congenital Anomalies Using Geographic Information Systems (GIS) to Develop Individual-Level Exposure Estimates. Int. J. Environ. Res. Public Health 2014, 11, 1803-1823. https://doi.org/10.3390/ijerph110201803
Holtby CE, Guernsey JR, Allen AC, VanLeeuwen JA, Allen VM, Gordon RJ. A Population-Based Case-Control Study of Drinking-Water Nitrate and Congenital Anomalies Using Geographic Information Systems (GIS) to Develop Individual-Level Exposure Estimates. International Journal of Environmental Research and Public Health. 2014; 11(2):1803-1823. https://doi.org/10.3390/ijerph110201803
Chicago/Turabian StyleHoltby, Caitlin E., Judith R. Guernsey, Alexander C. Allen, John A. VanLeeuwen, Victoria M. Allen, and Robert J. Gordon. 2014. "A Population-Based Case-Control Study of Drinking-Water Nitrate and Congenital Anomalies Using Geographic Information Systems (GIS) to Develop Individual-Level Exposure Estimates" International Journal of Environmental Research and Public Health 11, no. 2: 1803-1823. https://doi.org/10.3390/ijerph110201803