Joint Effects of Smoking and Sedentary Lifestyle on Lung Function in African Americans: The Jackson Heart Study Cohort



 ,
,
Abstract
:1. Introduction
1.1. Smoking and Lung Function
1.2. Sedentary Lifestyle and Lung Function
1.3. Significance
- Are there differences in the lung function of smokers and non-smokers who are physically active versus smokers and non-smokers who are not physically active?
- Does sedentary lifestyle mediate the relationship between smoking and lung function in AAs in the JHS?
2. Design/Methods
2.1. Study Population
2.2. Outcome Measures
2.3. Independent Variables
2.4. Covariates
2.5. Statistical Analysis
3. Results

{kind=link}
| Characteristics | NSK_NSL | NSK_SL | SK_NSL | SK_SL | p |
|---|---|---|---|---|---|
| Women (n = 2,065) | (n = 1,425) | (n = 440) | (n = 152) | (n = 48) | |
| Age, years † | 52 ± 12 | 62 ± 12 | 51 ± 11 | 56 ± 9 | **** |
| Body Mass index | 32.6 ± 7.5 | 33.2 ± 7.7 | 31.4 ± 7.3 | 31.1 ± 7.4 | * |
| Marital status, Married (%) | 46.5 | 47.1 | 42.1 | 35.4 | NS |
| Family income, Affluent (%) | 31.2 | 18.6 | 18.4 | 12.5 | **** |
| Education, ≥College Associate (%) | 51.0 | 30.7 | 29.6 | 27.1 | **** |
| Alcohol Use (%) | 43.6 | 23.1 | 65.1 | 54.2 | **** |
| Hypertension (%) | 56.5 | 73.7 | 49.3 | 78.7 | **** |
| Anti-hypertensive therapy (%) | 49.1 | 67.4 | 38.9 | 65.2 | **** |
| Type 2 Diabetes Mellitus (%) | 14.8 | 24.9 | 11.5 | 28.3 | **** |
| Anti-diabetic medication (%) | 12.9 | 23.3 | 8.2 | 27.3 | **** |
| Total dietary fiber, grams | 15.0 ± 6.8 | 13.8 ± 5.8 | 16.6 ± 7.4 | 14.9 ± 6.8 | *** |
| FEV1 † | 2.21 ± 0.48 | 1.90 ± 0.46 | 2.14 ± 0.50 | 1.89 ± 0.44 | **** |
| FVC † | 2.70 ± 0.57 | 2.38 ± 0.58 | 2.64 ± 0.58 | 2.45 ± 0.53 | **** |
| FEV1/FVC † | 82.1 ± 8.5 | 80.2 ± 8.8 | 81.3 ± 9.1 | 77.4 ± 9.2 | **** |
| FEV1% Predicted † | 95.4 ± 16.7 | 93.8 ± 19.6 | 89.0 ± 15.5 | 85.2 ± 16.1 | **** |
| FVC% Predicted † | 93.7 ± 17.0 | 92.4 ± 20.8 | 88.6 ± 15.5 | 87.8 ± 15.1 | ** |
| Airway Obstruction (%) | 8.1 | 10.7 | 10.1 | 18.8 | * |
| Men (n = 1,191) | (n = 826) | (n = 167) | (n = 155) | (n = 43) | |
| Age, years † | 52 ± 12 | 63 ± 12 | 49 ± 11 | 61 ± 11 | **** |
| Body Mass index † | 29.9 ± 5.9 | 30.2 ± 6.0 | 28.0 ± 6.3 | 28.1 ± 8.4 | *** |
| Marital status, Married (%) | 75.7 | 75.3 | 58.7 | 46.5 | **** |
| Family income, Affluent (%) | 45.2 | 28.1 | 28.4 | 23.3 | **** |
| Education, ≥College Associate (%) | 48.1 | 25.8 | 27.1 | 16.3 | **** |
| Alcohol Use (%) | 60.1 | 45.5 | 87.1 | 67.4 | **** |
| Hypertension (%) | 53.2 | 74.7 | 48.7 | 62.8 | **** |
| Anti-hypertensive therapy (%) | 41.5 | 57.4 | 22.8 | 47.5 | **** |
| Type 2 Diabetes Mellitus (%) | 12.3 | 22.4 | 9.2 | 23.8 | *** |
| Anti-diabetic medication (%) | 10.8 | 20.7 | 6.8 | 17.1 | **** |
| Total dietary fiber, grams | 17.8 ± 8.3 | 16.4 ± 6.7 | 21.0 ± 10.0 | 21.4 ± 16.7 | **** |
| FEV1† | 3.07 ± 0.66 | 2.59 ± 0.63 | 2.97 ± 0.66 | 2.30 ± 0.69 | **** |
| FVC †` | 3.80 ± 0.78 | 3.32 ± 0.92 | 3.84 ± 0.74 | 3.09 ± 0.77 | **** |
| FEV1/FVC † | 81.1 ± 8.1 | 78.8 ± 10.4 | 77.5 ± 10.0 | 74.5 ± 12.0 | **** |
| FEV1% Predicted † | 92.6 ± 15.8 | 88.7 ± 17.2 | 87.9 ± 15.3 | 76.4 ± 17.8 | **** |
| FVC% Predicted | 91.1 ± 15.9 | 88.3 ± 27.4 | 90.8 ± 14.1 | 79.8 ± 17.3 | *** |
| Airway Obstruction (%) | 11.5 | 18.1 | 18.7 | 41.9 | *** |
| Characteristics | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| NSK-SL | SK-NSL | p | NSK-SL | SK-NSL | p | |
| Women | ||||||
| Forced expiratory volume in 1 second (FEV1) | 2.08 ± 0.02 | 2.07 ± 0.03 | 0.7342 | 2.11 ± 0.02 | 2.05 ± 0.04 | 0.1932 |
| Forced Vital Capacity (FVC) | 2.56 ± 0.03 | 2.57 ± 0.04 | 0.8300 | 2.59 ± 0.03 | 2.51 ± 0.05 | 0.1355 |
| FEV1/FVC Ratio | 81.6 ± 0.42 | 80.7 ± 0.68 | 0.2670 | 81.5 ± 0.46 | 81.6 ± 0.76 | 0.9269 |
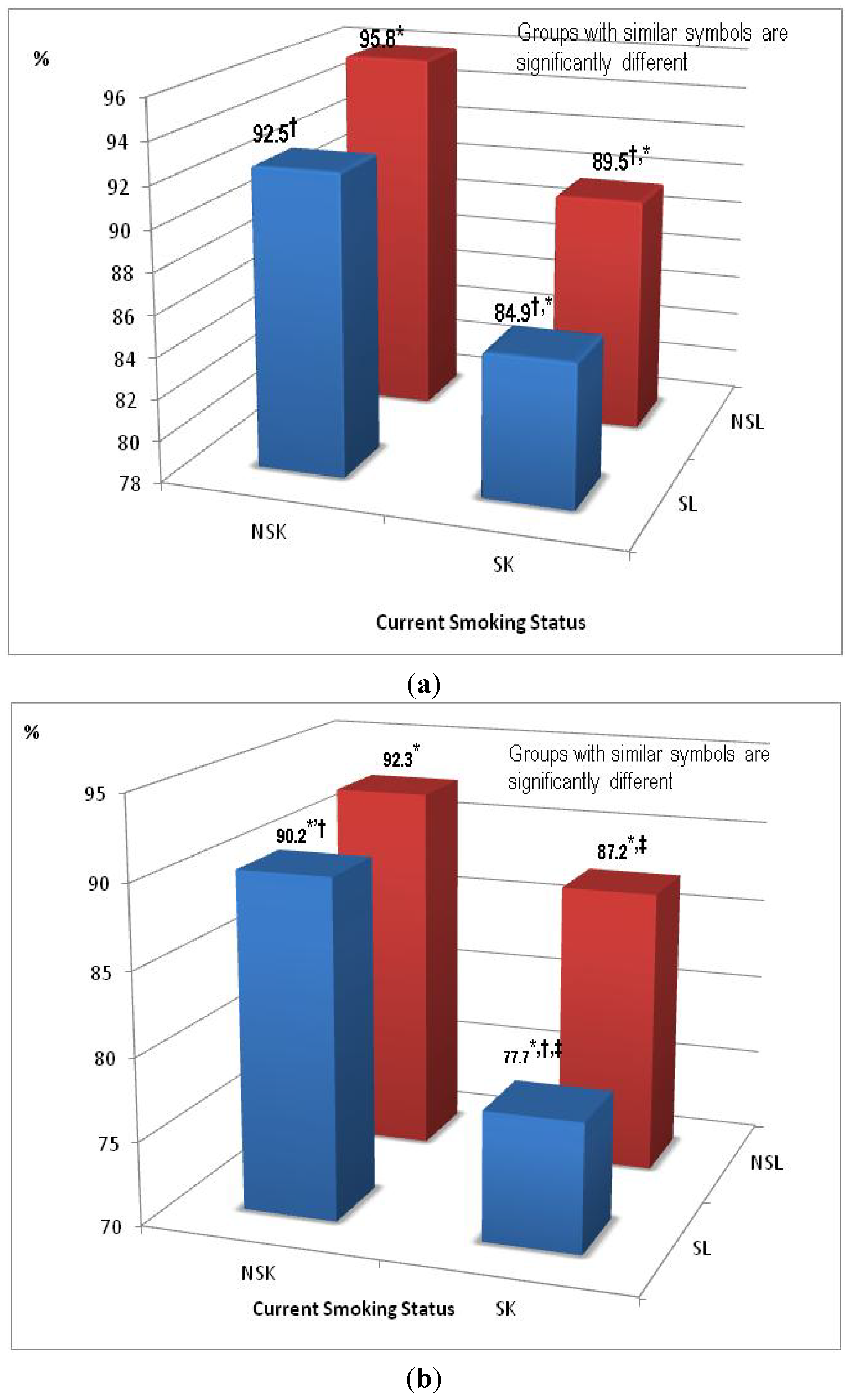
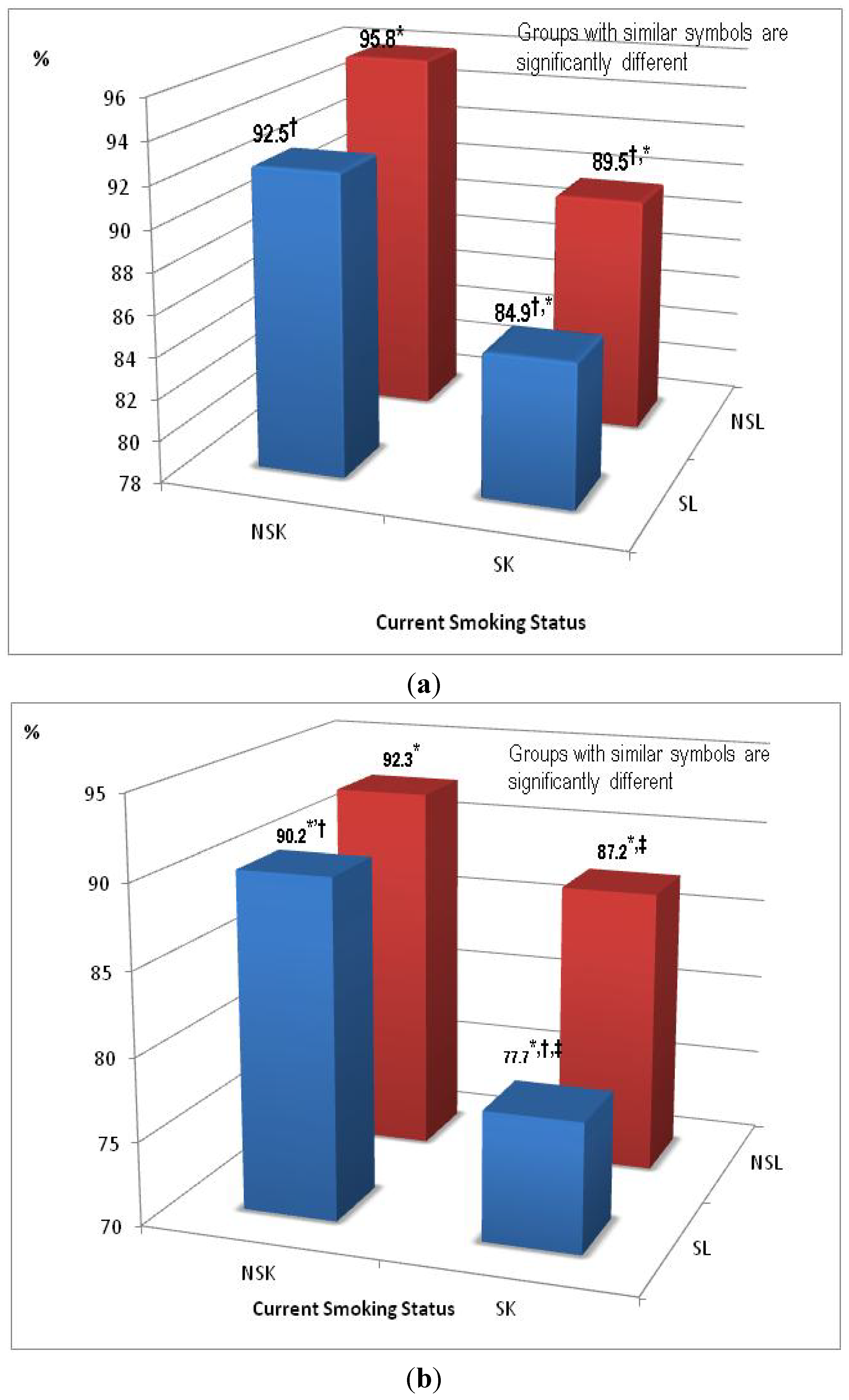
| FEV1% Predicted | 92.5 ± 0.86 | 89.5 ± 1.40 | 0.0689 | 93.3 ± 0.92 | 88.6 ± 1.53 | 0.0102 |
| FVC % Predicted | 91.2 ± 0.89 | 89.1 ± 1.44 | 0.2028 | 92.1 ± 0.95 | 86.9 ± 1.58 | 0.0055 |
| Airways Obstruction | 1.00 | 0.59 (0.30,1.15) | 0.1200 | 1.00 | 0.68 (0.32,1.48) | 0.3328 |
| Men | ||||||
| FEV1 | 2.85 ± 0.04 | 2.86 ± 0.05 | 0.9037 | 2.91 ± 0.05 | 2.89 ± 0.05 | 0.7679 |
| FVC | 3.56 ± 0.06 | 3.74 ± 0.06 | 0.0333 | 3.59 ± 0.06 | 3.71 ± 0.06 | 0.1543 |
| FEV1/FVC | 80.8 ± 0.68 | 76.6 ± 0.69 | <0.0001 | 80.9 ± 0.71 | 78.1 ± 0.69 | 0.0048 |
| FEV1% Predicted | 90.2 ± 1.28 | 87.2 ± 1.29 | 0.1042 | 91.2 ± 1.37 | 87.5 ± 1.34 | 0.0641 |
| FVC % Predicted | 89.6 ± 1.43 | 90.2 ± 1.43 | 0.7942 | 89.2 ± 1.32 | 89.0 ± 1.29 | 0.9312 |
| Airways Obstruction | 1.00 | 1.21 (0.62, 2.34) | 0.5744 | 1.00 | 1.46 (0.66, 3.24) | 0.3471 |
| Lung Functioning Measures | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| 1. Bivariate and Multivariable Analysis: FEV1 | ||||
| Smoking status: | ||||
| Never | 2.13 | 2.11 | 2.12 | 2.11 |
| Former | 2.18 | 2.15 | 2.22 | 2.20 |
| Current | 2.03 | 2.01 | 2.06 | 2.05 |
| p-value | 0.0002 | 0.0005 | 0.0005 | 0.0011 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 2.13 | -- | 2.15 |
| Sedentary Lifestyles | -- | 2.05 | -- | 2.09 |
| p-value | -- | 0.0002 | -- | 0.0215 |
| FVC | ||||
| Smoking status: | ||||
| Never | 2.61 | 2.59 | 2.63 | 2.62 |
| Former | 2.71 | 2.68 | 2.66 | 2.64 |
| Current | 2.55 | 2.53 | 2.46 | 2.45 |
| p-value | 0.0015 | 0.0039 | 0.0004 | 0.0007 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 2.64 | -- | 2.59 |
| Sedentary Lifestyles | -- | 2.56 | -- | 2.55 |
| p-value | -- | 0.0031 | -- | 0.1246 |
| FEV1/FVC | ||||
| Smoking status: | ||||
| Never | 81.7 | 81.6 | 80.8 | 80.7 |
| Former | 81.2 | 81.1 | 83.9 | 83.7 |
| Current | 80.0 | 79.9 | 83.6 | 83.5 |
| P-value | 0.0161 | 0.0156 | 0.1493 | 0.1616 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 81.1 | -- | 82.8 |
| Sedentary Lifestyles | -- | 80.7 | -- | 82.4 |
| P-value | -- | 0.3752 | -- | 0.3687 |
| Percent Predicted FEV1 | ||||
| Smoking status: | ||||
| Never | 94.9 | 94.1 | 94.2 | 93.6 |
| Former | 95.4 | 94.2 | 97.7 | 96.8 |
| Current | 88.3 | 87.6 | 90.2 | 89.6 |
| P-value | <0.0001 | <0.0001 | <0.0001 | 0.0002 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 93.6 | -- | 94.5 |
| Sedentary Lifestyles | -- | 90.3 | -- | 92.2 |
| P-value | -- | 0.0005 | -- | 0.0216 |
| Percent predicted FVC | ||||
| Smoking status: | ||||
| Never | 93.1 | 92.5 | 93.6 | 93.3 |
| Former | 94.4 | 93.5 | 93.4 | 92.8 |
| Current | 88.6 | 88.0 | 85.8 | 85.4 |
| P-value | 0.0008 | 0.0013 | <0.0001 | 0.0001 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 92.6 | -- | 91.3 |
| Sedentary Lifestyles | -- | 90.1 | -- | 89.7 |
| P-value | -- | 0.0096 | -- | 0.1312 |
| Percent Predicted FEV1/FVC | ||||
| Smoking status: | ||||
| Never | 98.9 | 99.2 | 100.1 | 100.6 |
| Former | 99.9 | 100.3 | 96.9 | 97.6 |
| Current | 101.1 | 101.4 | 96.6 | 97.0 |
| P-value | 0.6568 | 0.6468 | 0.8819 | 0.08862 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 99.7 | -- | 97.5 |
| Sedentary Lifestyles | -- | 101.0 | -- | 99.3 |
| P-value | -- | 0.5081 | -- | 0.3954 |
| 2. Odds Ratio Analysis Obstruction | ||||
| Smoking status:(Ref: Never) | ||||
| Former | 0.80 (0.51,1.33) | 0.88 (0.54,1.42) | 1.18 (0.31,4.39) | 1.33 (0.36,4.96) |
| Current | 1.36 (0.86,2.16) | 1.34 (0.84,2.13) | 1.87 (0.50,6.98) | 1.93 (0.52,7.21) |
| Physical Activity(Ref: Non-Sedentary Lifestyles | ||||
| Sedentary Lifestyles | -- | 1.90 (1.33,2.73) | -- | 1.84 (1.25,2.71) |
| Lung Functioning Measures | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| 1. Bivariate and Multivariable Analysis: FEV1 | ||||
| Smoking status: | ||||
| Never | 2.98 | 2.91 | 2.89 | 2.84 |
| Former | 3.04 | 2.97 | 3.20 | 3.13 |
| Current | 2.79 | 2.73 | 2.97 | 2.91 |
| P-value | <0.0001 | <0.0001 | 0.0002 | 0.0003 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 2.97 | -- | 3.04 |
| Sedentary Lifestyles | -- | 2.77 | -- | 2.88 |
| P-value | -- | <0.0001 | -- | 0.0007 |
| FVC | ||||
| Smoking status: | ||||
| Never | 3.69 | 3.61 | 3.60 | 3.54 |
| Former | 3.82 | 3.73 | 4.01 | 3.93 |
| Current | 3.64 | 3.57 | 3.77 | 3.70 |
| P-value | 0.0220 | 0.0406 | 0.0013 | 0.0019 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 3.76 | -- | 3.82 |
| Sedentary Lifestyles | -- | 3.52 | -- | 3.62 |
| P-value | -- | <0.0001 | -- | 0.0021 |
| FEV1/FVC | ||||
| Smoking status: | ||||
| Never | 81.1 | 81.1 | 79.8 | 79.7 |
| Former | 79.9 | 79.9 | 81.3 | 81.2 |
| Current | 76.6 | 76.6 | 80.1 | 80.0 |
| P-value | <0.0001 | <0.0001 | 0.3023 | 0.3071 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 79.2 | -- | 80.4 |
| Sedentary Lifestyles | -- | 79.1 | -- | 80.2 |
| P-value | -- | 0.9491 | -- | 0.8139 |
| Percent Predicted FEV1 | ||||
| Smoking status: | ||||
| Never | 91.8 | 90.7 | 87.6 | 86.8 |
| Former | 92.3 | 91.1 | 99.2 | 98.0 |
| Current | 85.1 | 84.2 | 92.7 | 91.6 |
| P-value | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Physical Activity | ||||
| Non-Sedentary Lifestyles | -- | 90.4 | -- | 93.6 |
| Sedentary Lifestyles | -- | 86.9 | -- | 90.6 |
| P-value | -- | 0.0066 | -- | 0.0294 |
| Percent predicted FVC | ||||
| Smoking status: | ||||
| Never | 90.1 | 89.2 | 86.5 | 85.8 |
| Former | 92.2 | 91.3 | 99.0 | 98.1 |
| Current | 88.1 | 87.4 | 92.7 | 91.9 |
| P-value | 0.0513 | 0.0704 | 0.0001 | 0.0002 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 90.6 | -- | 93.1 |
| Sedentary Lifestyles | -- | 87.9 | -- | 90.8 |
| P-value | -- | 0.0625 | -- | 0.1379 |
| Percent Predicted FEV1/FVC | ||||
| Smoking status: | ||||
| Never | 99.0 | 99.1 | 100.9 | 101.1 |
| Former | 100.2 | 100.3 | 98.3 | 98.6 |
| Current | 105.4 | 105.5 | 99.4 | 99.7 |
| P-value | <0.0001 | <0.0001 | 0.5993 | 0.6157 |
| Physical Activity: | ||||
| Non-Sedentary Lifestyles | -- | 101.5 | -- | 99.4 |
| Sedentary Lifestyles | -- | 101.9 | -- | 100.2 |
| P-value | -- | 0.7670 | -- | 0.5635 |
| 2. Odds Ratio Analysis Obstruction | ||||
| Smoking status(Ref: Never) | ||||
| Former | 1.18 (0.78,1.79) | 1.21 (0.80, | 0.88 (0.11,1.38) | 0.41 (0.11,1.47) |
| Current | 2.38 (1.60,3.56) | 2.31 (1.54,3.46) | 0.75 (0.21,2.72) | 0.78 (0.21,2.84) |
| Physical Activity: (Ref: Non-Sedentary Lifestyles) | ||||
| Sedentary Lifestyles | -- | 1.71 (1.14,2.57) | -- | 1.62 (1.03,2.55) |
4. Discussion
- Women who are nonsmokers and have a sedentary lifestyle tend to have a significantly higher level of lung function (FEV1 % Predicted) compared to women smokers who are non-sedentary.
- Men who are nonsmokers and have a sedentary lifestyle tend to have a significantly higher level of lung function using the FEV1/FVC ratio as a measure of lung function.
Study Limitations and Strengths
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sobol, B.; Herbert, W.; Emirgil, C. The high incidence of pulmonary functional abnormalities in patients with coronary artery disease. Chest 1974, 65, 148–151. [Google Scholar] [CrossRef]
- Vestbo, J.; Lange, P. Forced expiratory volume in 1 second (FEV1)—A respiratory physiological measurement of considerable prognostic value. Ugeskr. Laeger 1991, 153, 2292–2295. [Google Scholar]
- Keys, A.; Aravanis, C.; Blackburn, H.; Djordjevic, B.S.; Dontas, A.S; Fidanza, F.; Karvonen, M.J.; Menotti, A.; Taylor, H.L. Lung function as a risk factor for coronary heart disease. Am. J. Public Health 1972, 62, 1506–1511. [Google Scholar] [CrossRef]
- Knuiman, M.W.; James, A.L.; Divitini, M.L.; Ryan, G.; Bartholomew, H.C.; Musk, A.W. Lung function, respiratory symptoms, and mortality: Results from the Busselton Health Study. Ann. Epidemiol. 1999, 9, 297–306. [Google Scholar]
- Fulambarker, A.; Copur, A.S.; Javeri, A.; Jere, S.; Cohen, M.E. References values for pulmonary function in Asian Indians living in the United States. Chest 2004, 126, 1225–1223. [Google Scholar] [CrossRef]
- Gordon-Larsen, P.; McMurray, R.G.; Popkin, B.M. Adolescent physical activity and inactivity vary by ethnicity: The National Longitudinal Study of Adolescent Health. J. Pediatr. 1999, 135, 301–306. [Google Scholar] [CrossRef]
- Kaczynski, A.T.; Manske, S.R.; Mannell, R.C.; Grewal, K. Smoking and physical activity: A systematic review. Am. J. Health Behav. 2008, 32, 93–110. [Google Scholar]
- Kam, S.W.; Ping, C.; Hok, C.L.; Xin, S.H.; David, S.C. The impact of heavy passive smoking on arterial endothelial function in modernized Chinese. J. Am. Coll. Cardiol. 2000, 36, 1228–1232. [Google Scholar] [CrossRef]
- Ahmad, A.; Reza, G.; Alireza, N.; Amir, G. Effects of aerobic exercise on lung function in overweight and obese students. Tanaffos 2011, 10, 24–31. [Google Scholar]
- Garcia-Aymerich, J.; Lange, P.; Benet, M.; Schnohr, P.; Anto, J. Regular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 458–463. [Google Scholar] [CrossRef]
- Katz, P.; Chen, H.; Omachi, T.A.; Gregorich, S.E.; Julian, L.; Cisternas, M.; Balmes, J.; Blanc, P.D. The role of physical inactivity in increasing disability among older adults with obstructive airway disease. J. Cardiopulm. Rehabil. Prev. 2011, 31, 193–197. [Google Scholar] [CrossRef]
- Jakes, R.W.; Day, N.E.; Patel, B.; Khaw, K.T.; Oakes, S.; Luben, R.; Welch, A.; Bingham, S.; Wareham, N.J. Physical inactivity is associated with lower forced expiratory volume in 1 second: European Prospective Investigation into Cancer-Norfolk Prospective Population Study. Am. J. Epidemiol. 2002, 56, 139–147. [Google Scholar]
- Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000–2004. Morb. Mortal. Wkly. Rep. 2008, 57, 1226–1228. [Google Scholar]
- Centers for Disease Control and Prevention. Health, United States, 2012: With Special Feature on Emergency Care; National Center for Health Statistics: Hyattsville, MD, USA, 2012. Available online: http://www.cdc.gov/nchs/data/hus/hus12.pdf (accessed on 21 November 2013).
- United States. Public Health Services. Tobacco Use Among U.S. Racial/Ethnic Minority Groups—African Americans, American Indians and Alaska Natives, Asian Americans and Pacific Islanders, and Hispanics. In The Report of the Surgeon General; United States. Public Health Services; Atlanta, GA, USA, 1998. [Google Scholar]
- Okuyemi, K.S.; Richter, K.P.; Ahluwalia, J.S.; Mosier, M.C.; Nazir, N.; Resnicow, K. Smoking reduction practices among African American smokers. Nicotine Tob. Res. 2002, 4, S167–S173. [Google Scholar] [CrossRef]
- Markewitz, B.A.; Owens, M.W.; Payne, D.K. The pathogenesis of chronic obstructive pulmonary disease. Am. J. Med. Sci. 1999, 318, 74–78. [Google Scholar] [CrossRef]
- Thorn, J.; Bjorkelund, S.; Bengtsson, C.; Guo, X.; Lissner, L.; Sundh, V. Low socio-economic status, smoking, mental stress and obesity predict obstructive symptoms in women, but only smoking also predicts subsequent experience of poor health. Int. J. Med. Sci. 2007, 4, 7–12. [Google Scholar]
- Lind, E.; Joens-Matre, R.R.; Ekkekakis, P. What intensity of physical activity do previously sedentary middle-aged women select? Evidence of a coherent pattern from physiological, perceptual, and affective markers. Prev. Med. 2005, 40, 407–419. [Google Scholar] [CrossRef]
- Siddiqi, Z.; Tiro, J.A.; Shuval, K. Understanding impediments and enablers to physical activity among African American adults: A systematic review of qualitative studies. Health Educ. Res. 2011, 26, 1010–1024. [Google Scholar] [CrossRef]
- Kriska, A. Ethnic and cultural issues in assessing physical activity. Res. Q. Exercise Sport 2000, 71, 47–53. [Google Scholar]
- Kim, J.S.; Bramlet, M.H.; Wright, L.K.; Poon, L.W. Racial differences in health status and health behaviors of older adults. Nurs. Res. 1998, 47, 243–250. [Google Scholar] [CrossRef]
- Adams-Campbell, L.L.; Rosenberg, L.; Washburn, R.A.; Rao, R.S.; Kim, K.S.; Palmer., J. Descriptive epidemiology of physical activity in African-American women. Prev. Med. 2000, 30, 43–50. [Google Scholar] [CrossRef]
- Chang, J.E.; Lee, J.H.; Kim, M.K.; Kim, S.J.; Kim, K.H.; Park, J.S.; Kim, T.H.; Kim, Y.I.; Lee, E.W.; Kim, J.O.; et al. Determinants of respiratory symptom development in patients with chronic airflow obstruction. Resp. Med. 2006, 100, 2170–2176. [Google Scholar] [CrossRef]
- Agnarsson, U.; Thorgeirsson, G.; Sigvaldason, H.; Sigfusson, N. Effects of leisure-time physical activity and ventilatory function on risk for stroke in men: The Reykjavik Study. Ann. Intern. Med. 1999, 130, 987–990. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G.; Ebrahim, S. Respiratory function and risk of stroke. Stroke 1995, 26, 2004–2010. [Google Scholar] [CrossRef]
- Burchfiel, C.M.; Enright, P.L.; Sharp, D.S.; Chyou, P.H.; Rodriguez, B.L.; Curb, J.D. Factors associated with variations in lung function among elderly Japanese-American men. Chest 1997, 112, 87–97. [Google Scholar] [CrossRef]
- Twisk, J.W.; Staal, B.J.; Brinkman, M.N.; Kemper, H.C.; van Mechelen, W. Tracking of lung function parameters and the longitudinal relationship with lifestyle. Eur. Respir. J. 1998, 12, 627–634. [Google Scholar] [CrossRef]
- Camoes, M.; Lopes, C. Factors associated with physical activity in the Portuguese population. Rev. Saude Publica. 2008, 42, 208–216. [Google Scholar]
- Fuqua, S.R.; Wyatt, S.B.; Sarpong, D.; Henderson, F.R.; Cunningham, M.F.; Taylor, H.A., Jr. Recruiting African-American research participation in the Jackson Heart Study: Methods, response rates, and sample description. Ethn. Dis. 2005, 15, 18–29. [Google Scholar]
- Taylor, H.A., Jr.; Wilson, J.G.; Jones, D.J.; Sarpong, D.F.; Srinivasan, A.; Garrison, R.J; Nelson, C.; Wyatt, S.B. Toward resolution of cardiovascular health disparities in African Americans: Design and methods of the Jackson Heart Study. Ethn. Dis. 2005, 15, 5–17. [Google Scholar]
- Dubbert, P.M.; Carithers, T.; Ainsworth, B.A.; Taylor, H.A., Jr.; Wilson, G.; Wyatt, S.B. Physical activity assessment methods in the Jackson Heart Study. Ethn. Dis. 2005, 15, 56–61. [Google Scholar]
- Payne, T.J.; Wyatt, S.B.; Mosley, T.H.; Dubbert, P.M.; Guiterrez-Mohammed, M.L.; Calvin, R.L.; Taylor, H.A., Jr.; Williams, D.R. Sociocultural methods in the Jackson Heart Study: Conceptual and descriptive overview. Ethn. Dis. 2005, 15, 38–48. [Google Scholar]
- Carithers, T.; Dubbert, P.M.; Crook, E.; Davy, B.; Wyatt, S.B.; Bogle, M.L.; Taylor, H.A., Jr.; Tucker, K.L. Dietary assessment in African Americans: Methods used in the Jackson Heart Study. Ethn. Dis. 2005, 15, 18–29. [Google Scholar]
- Carithers, T.C.; Talegawker, S.A.; Rowser, M.L.; Henry, O.R.; Dubbert, P.M.; Bogle, M.; Taylor, H.A., Jr.; Tucker, K.L. Validity and calibration of food frequency questionnaires used with African American adults in the Jackson Heart Study. J. Am. Diet. Assoc. 2009, 109, 1184–1193. [Google Scholar] [CrossRef]
- Carpenter, M.; Crow, R.; Steffes, M.; Rock, W.; Heilbraun, J.; Evans, G.; Skelton, T.; Jensen, R.; Sarpong, D. Laboratory, reading center, and coordinating center data management methods in the Jackson Heart Study. Am. J. Med. Sci. 2004, 328, 131–144. [Google Scholar] [CrossRef]
- Wilson, J.G.; Rotimi, C.N.; Ekunwe, L.; Royal, C.D.; Crump, M.E.; Wyatt, S.B.; Steffes, M.W.; Adeyemo, A.; Zhou, J.; Taylor, H.A., Jr.; et al. Study design for genetic analysis in the Jackson Heart Study. Ethn. Dis. 2005, 15, 30–37. [Google Scholar]
- Hankinson, J.; Odencrantz, J.; Fedan, K. Spirometric reference values from a sample of the general U.S. population. Am. J. Resp. Crit. Care Med. 1999, 159, 179–187. [Google Scholar] [CrossRef]
- Smitherman, T.; Dubbert, P.; Grothe, K.; Sung, J.H.; Kendzor, D.E.; Reis, J.P.; Ainsworth, B.E.; Newton, R.J., Jr.; Lesniak, K.T.; Taylor, H.A., Jr. Validation of the Jackson Heart Study Physical Activity Survey in African Americans. J. Phys. Act. Health. 2009, 6, S124–S132. [Google Scholar]
- Jacobs, D.R., Jr.; Nelson, E.; Dontas, A.S.; Keller, J.; Slattery, M.L.; Higgins, M. Are race and sex differences in lung function explained by frame size? The CARDIA Study. Am. J. Respir. Dis. 1992, 146, 644–649. [Google Scholar] [CrossRef]
- Harik-Khan, R.I.; Fleg, J.L.; Muller, D.C.; Wise, R.A. The effect of anthropometric and socioeconomic factors on the racial difference in lung function. Am. J. Respir. Crit. Care Med. 2001, 164, 1647–1654. [Google Scholar] [CrossRef]
- Higgins, M.; Keller, J.B.; Wagenknecht, L.E.; Townsend, M.C.; Sparrow, D.; Jacobs, D.R., Jr.; Hughes, G. Pulmonary function and cardiovascular risk factor relationships in black and in white young men and women. The CARDIA Study. Chest 1991, 99, 315–322. [Google Scholar] [CrossRef]
- Tockman, M.S.; Comstock, G.W. Respiratory risk factors and mortality: Longitudinal studies in Washington County, Maryland. Am. Rev. Respir. Dis. 1989, 140, S56–63. [Google Scholar] [CrossRef]
- Tabak, C.; Spijkerman, A.M.; Verschuren, W.M.; Smit, H.A. Does education level influence lung function decline (Doetinchem Cohort Study)? Eur. Respir. J. 2009, 34, 940–947. [Google Scholar] [CrossRef]
- Huxley, R.R.; Yatsuya, H.; Lutsey, P.L.; Woodward, M.; Alonso, A.; Folsom, A.R. Impact of age at smoking initiation, dosage, and time since quitting on cardiovascular disease in African Americans and whites. Am. J. Epidemiol. 175. [CrossRef]
- Verbanck, S.; Schuermans, D.; Meysman, M.; Paiva, M.; Vincken., W. Noninvasive assessment of airway alterations in Ssokers. Am. J. Respir. Crit. Care Med. 2004, 170, 414–419. [Google Scholar] [CrossRef]
- Ferrucci, L.; Izmirlian, G.; Leveille, S.; Phillips, C.L.; Corti, M.C.; Brock, D.B.; Guralnik, J.M. Smoking, physical activity, and active life expectancy. Am. J. Epidemiol. 1999, 149, 645–653. [Google Scholar] [CrossRef]
- Watkins, L.O. Epidemiology and burden of cardiovascular disease. Clin. Cardiol. 2004, 27, 1112–1116. [Google Scholar] [CrossRef]
- Mensah, G.A.; Mokdad, A.H.; Ford, E.S.; Greenlund, K.J.; Croft, J.B. State of disparities in cardiovascular health in the United States. Circulation 2005, 111, 1233–1241. [Google Scholar] [CrossRef]
- Hozawa, A.; Folsom, A.; Sharrett, A.R.; Chambless, L.E. Absolute and attributable risks of cardiovascular disease incidence in relation to optimal and borderline risk factors: Comparison of African American with white subjects—Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 2007, 167, 573–579. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Campbell Jenkins, B.W.; Sarpong, D.F.; Addison, C.; White, M.S.; Hickson, D.A.; White, W.; Burchfiel, C. Joint Effects of Smoking and Sedentary Lifestyle on Lung Function in African Americans: The Jackson Heart Study Cohort. Int. J. Environ. Res. Public Health 2014, 11, 1500-1519. https://doi.org/10.3390/ijerph110201500
Campbell Jenkins BW, Sarpong DF, Addison C, White MS, Hickson DA, White W, Burchfiel C. Joint Effects of Smoking and Sedentary Lifestyle on Lung Function in African Americans: The Jackson Heart Study Cohort. International Journal of Environmental Research and Public Health. 2014; 11(2):1500-1519. https://doi.org/10.3390/ijerph110201500
Chicago/Turabian StyleCampbell Jenkins, Brenda W., Daniel F. Sarpong, Clifton Addison, Monique S. White, DeMarc A. Hickson, Wendy White, and Cecil Burchfiel. 2014. "Joint Effects of Smoking and Sedentary Lifestyle on Lung Function in African Americans: The Jackson Heart Study Cohort" International Journal of Environmental Research and Public Health 11, no. 2: 1500-1519. https://doi.org/10.3390/ijerph110201500