Embedded Fragments from U.S. Military Personnel—Chemical Analysis and Potential Health Implications

Abstract
:1. Introduction
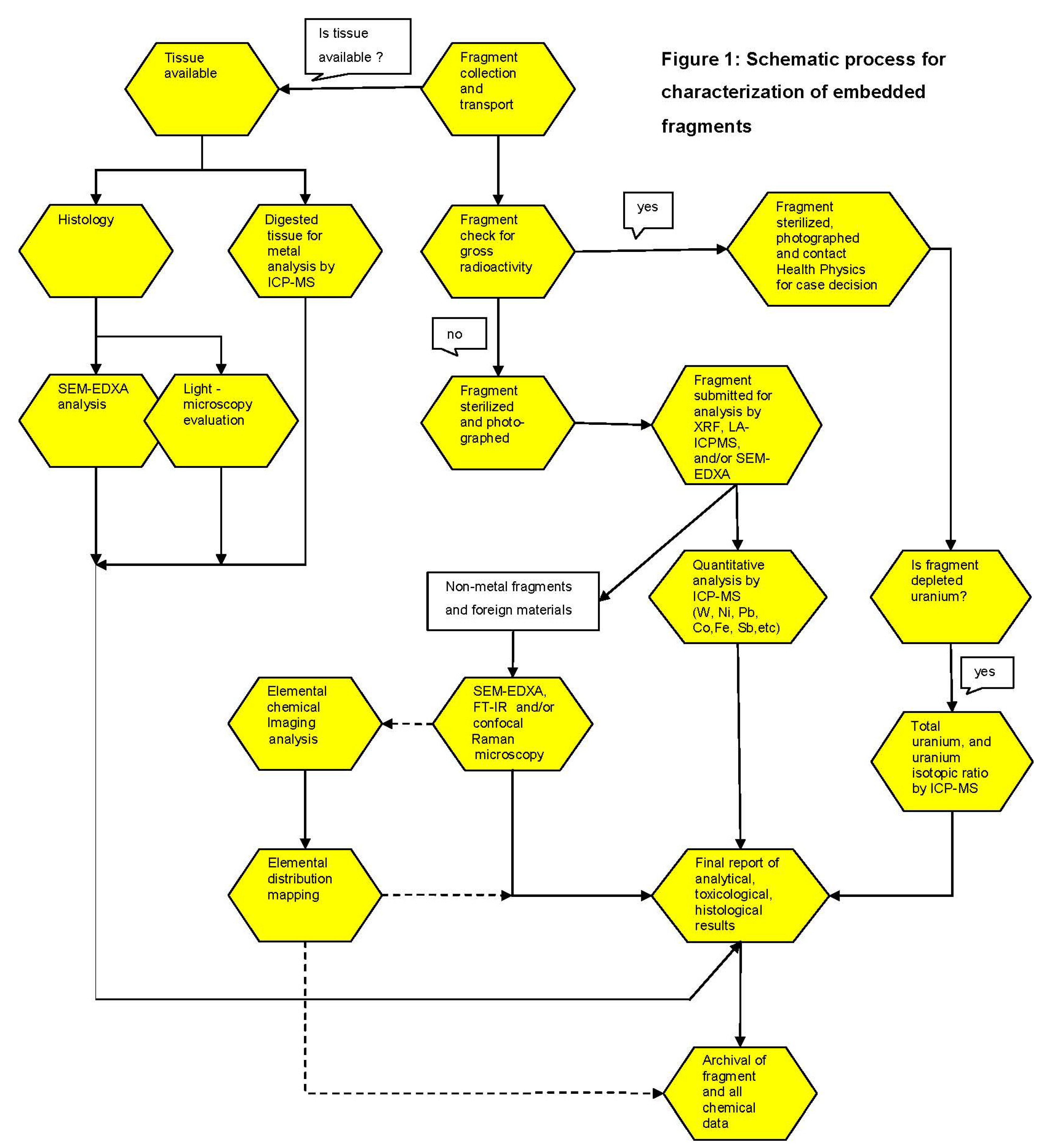
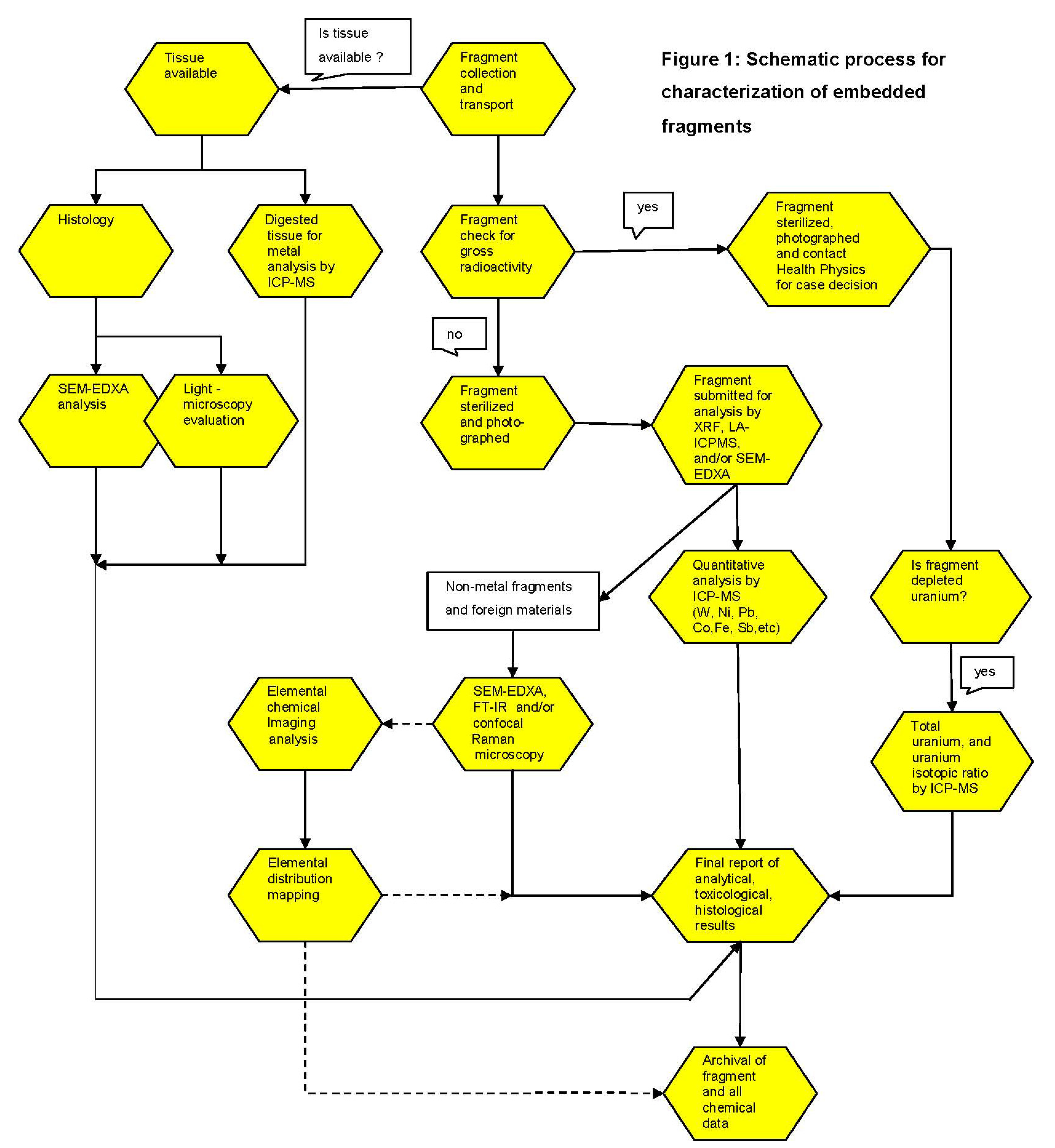
2. Methods
Chemical Analysis of Removed Fragments
3. Results
3.1. Embedded Metal Fragment Registry
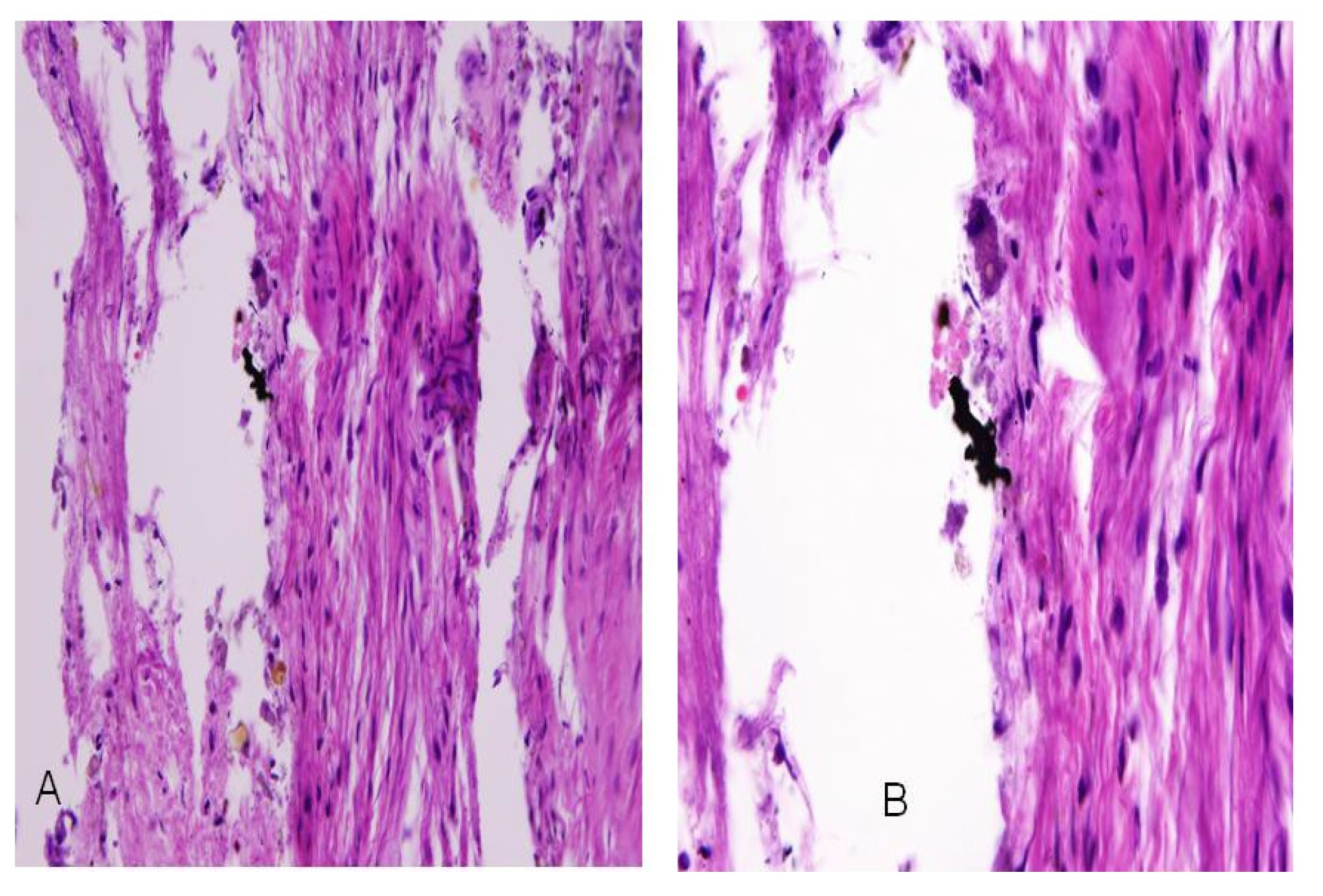
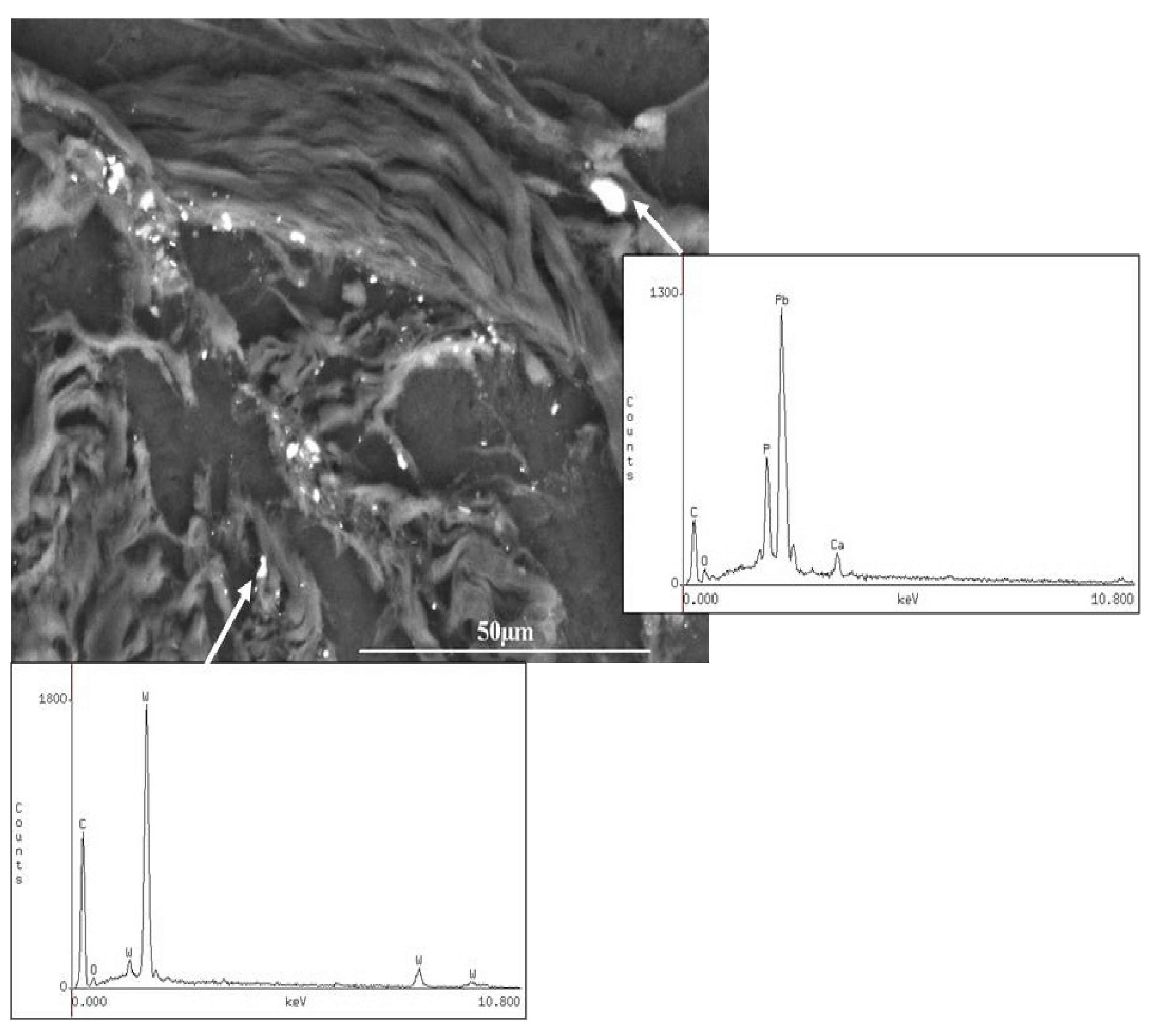
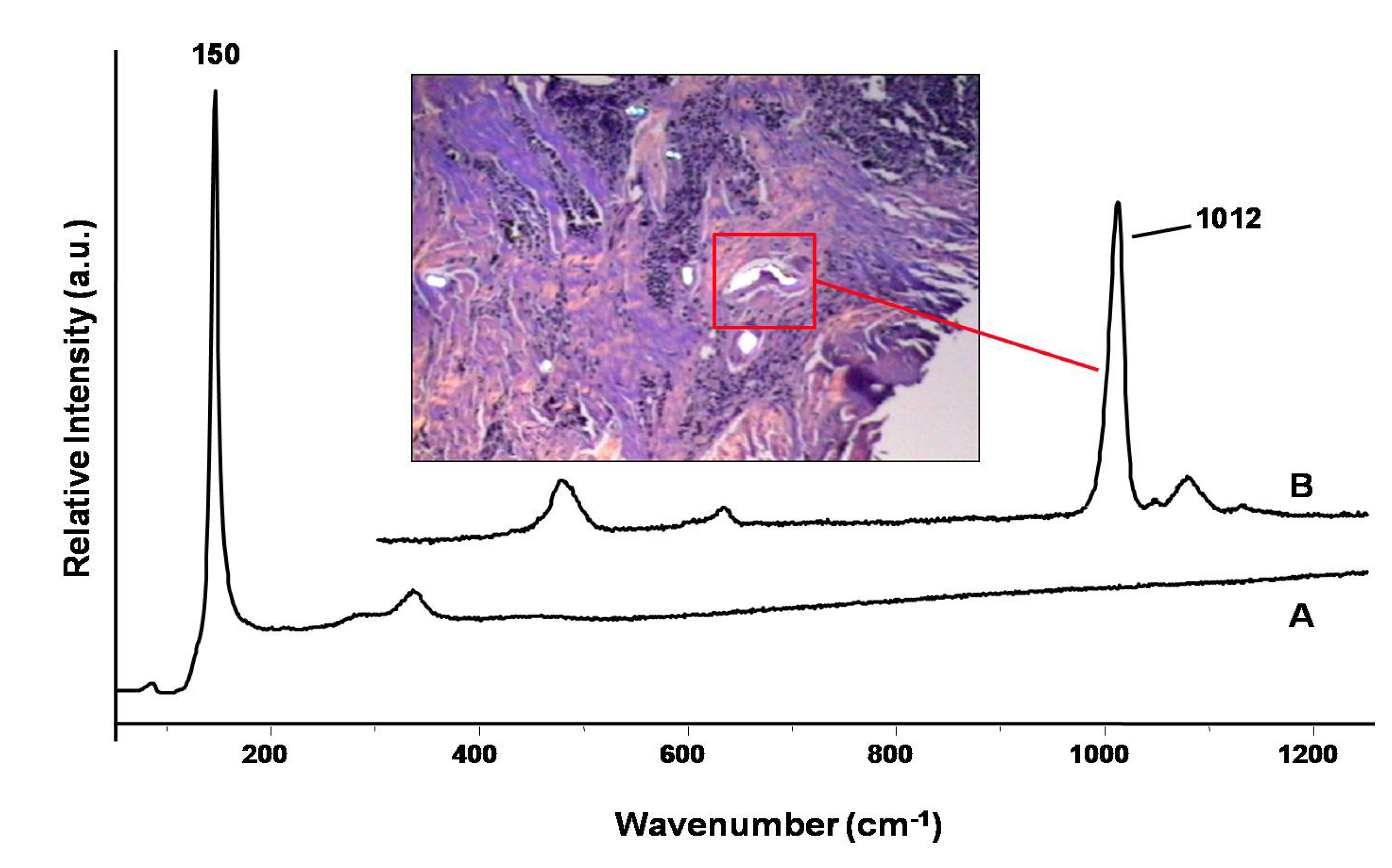
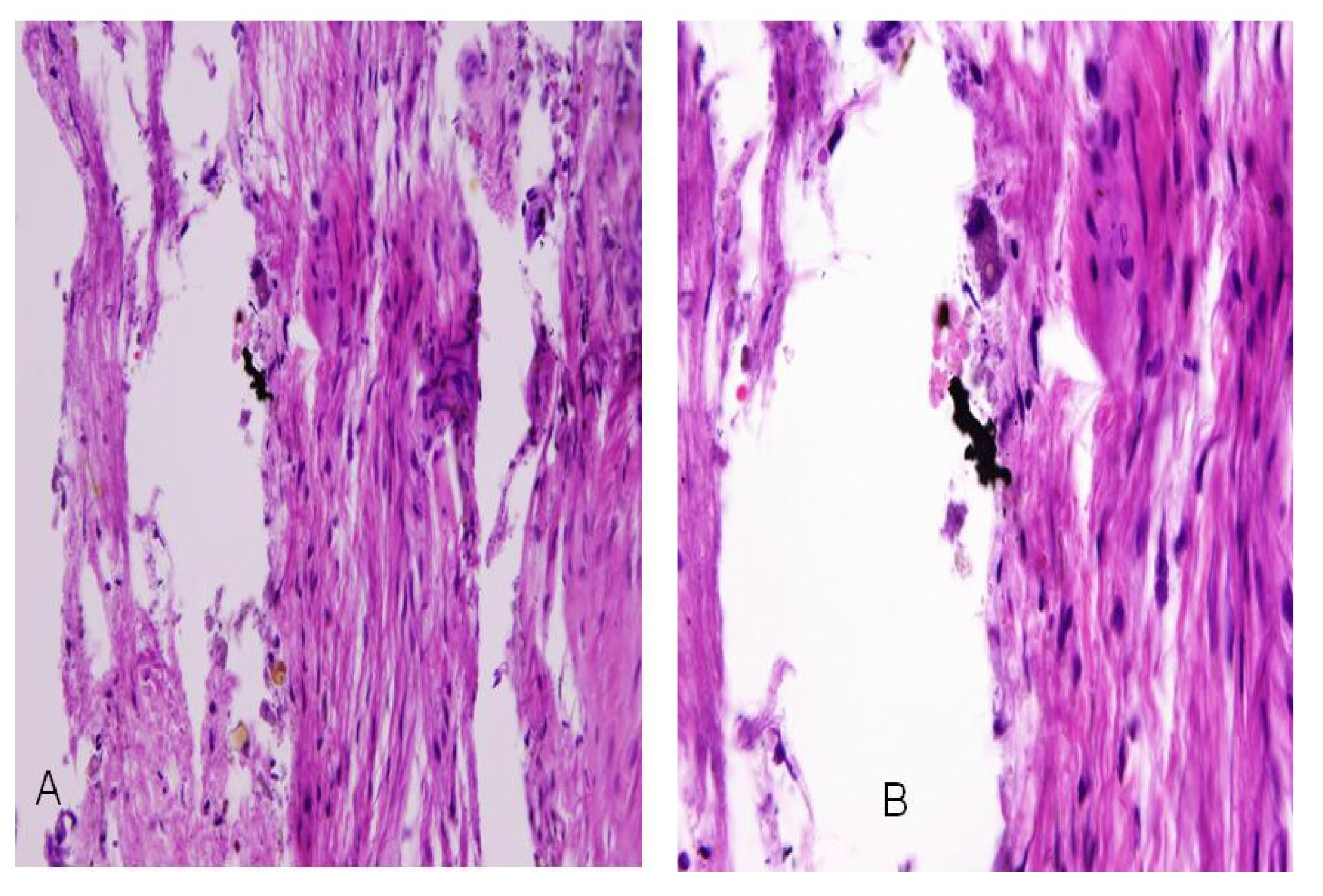
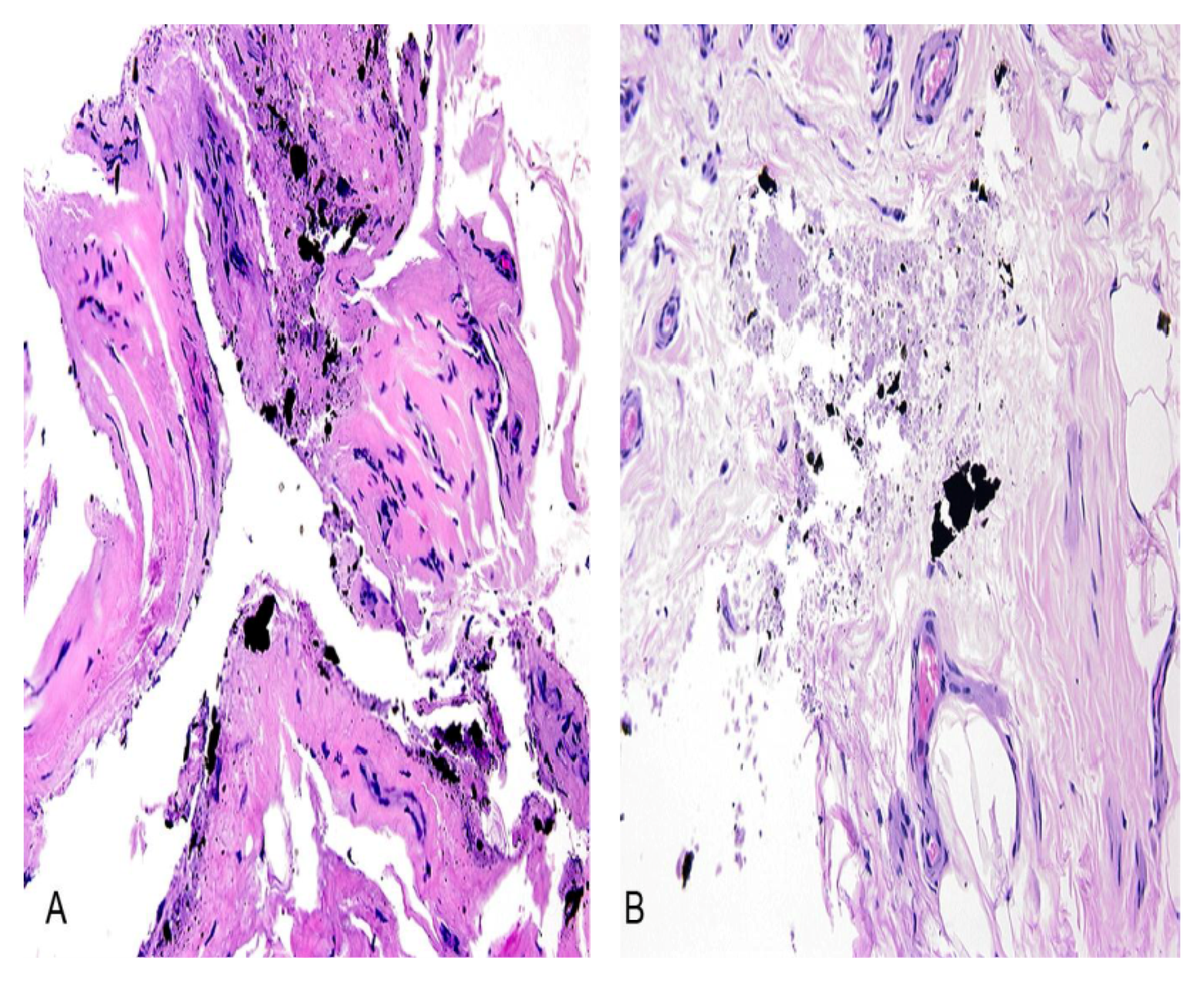
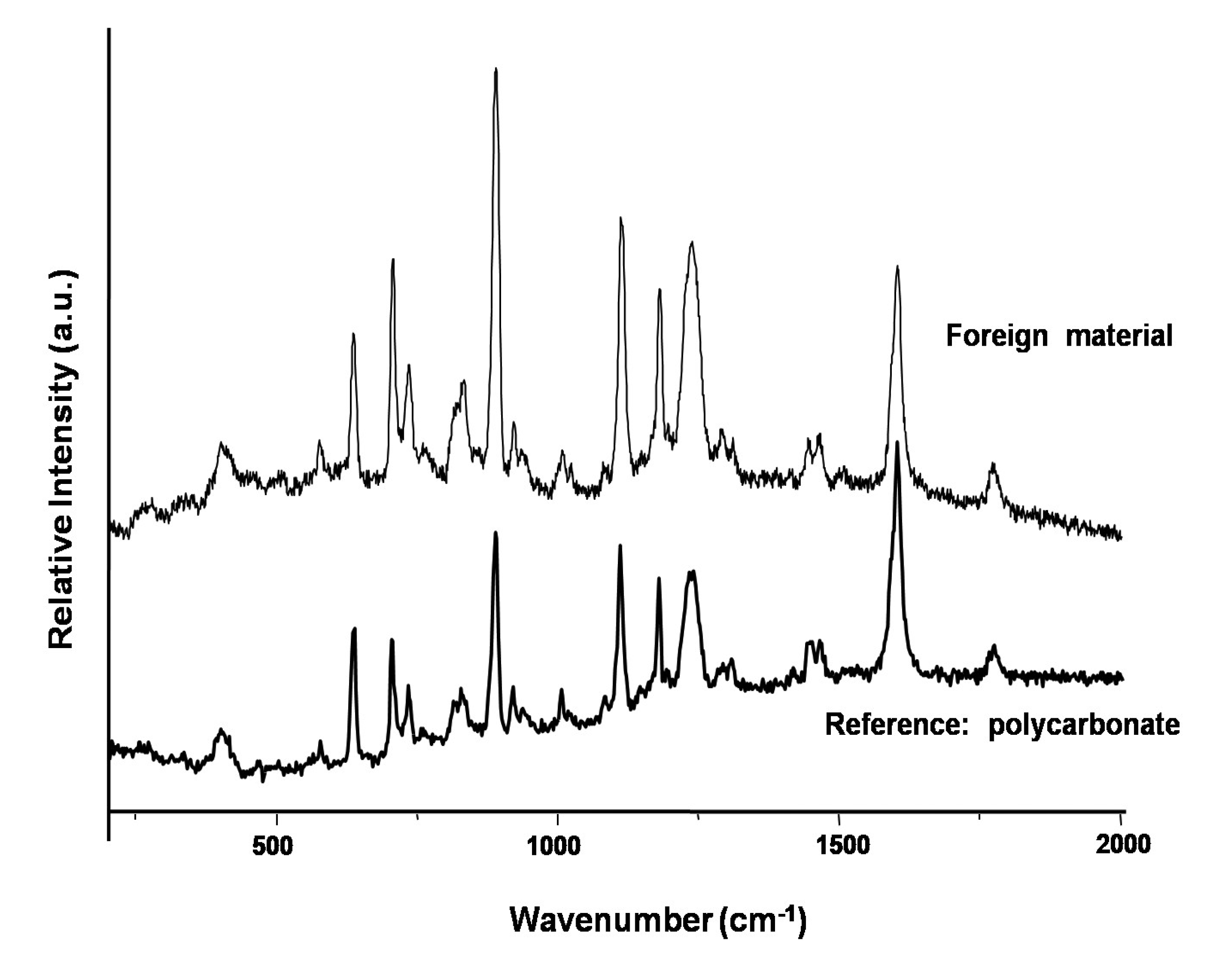
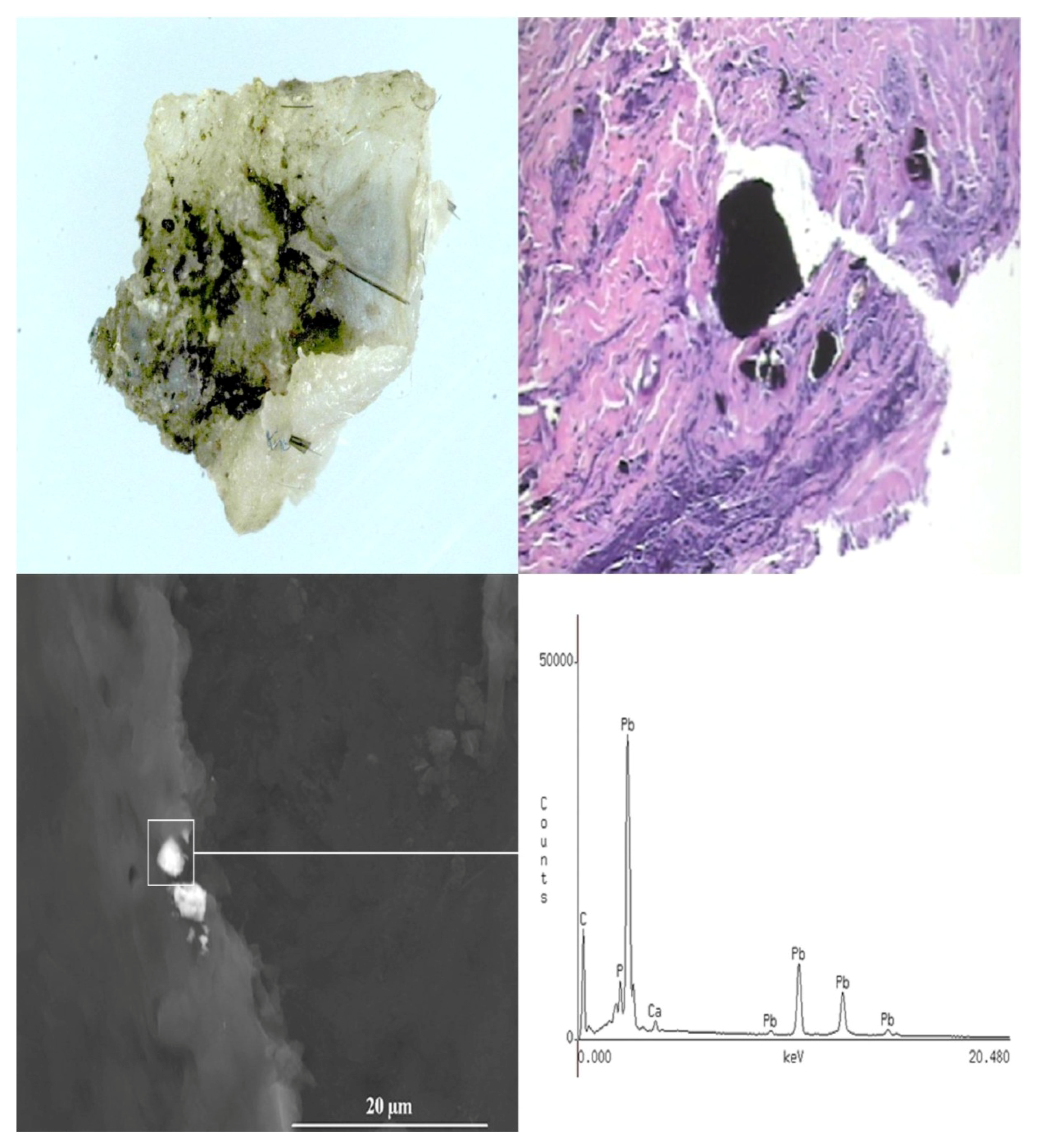
3.2. Case Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Fragments | |
|---|---|
| Total number of fragments received: | 831 |
| Non-Metals: | 112 |
| Organic materials | 26 |
| Plastic and polymers | 12 |
| Fabric | 2 |
| Wood | 2 |
| Geological (rocks, stones) | 10 |
| Others | 60 |
| Metals:* | 719 |
| Fe (>50%) | 274 |
| (10%–50%) | 37 |
| Cu (>50%) | 174 |
| (10%–50%) | 27 |
| Al (>50%) | 76 |
| (10%–50%) | 24 |
| Zn (>50%) | 26 |
| (10%–50%) | 36 |
| Pb (>50%) | 15 |
| (10%–50%) | 1 |
| Ni (>50%) | 1 |
| (10%–50%) | 14 |
| Cr (>50%) | 1 |
| (10%–50%) | 12 |
| DU ** (>80% U) | 1 |
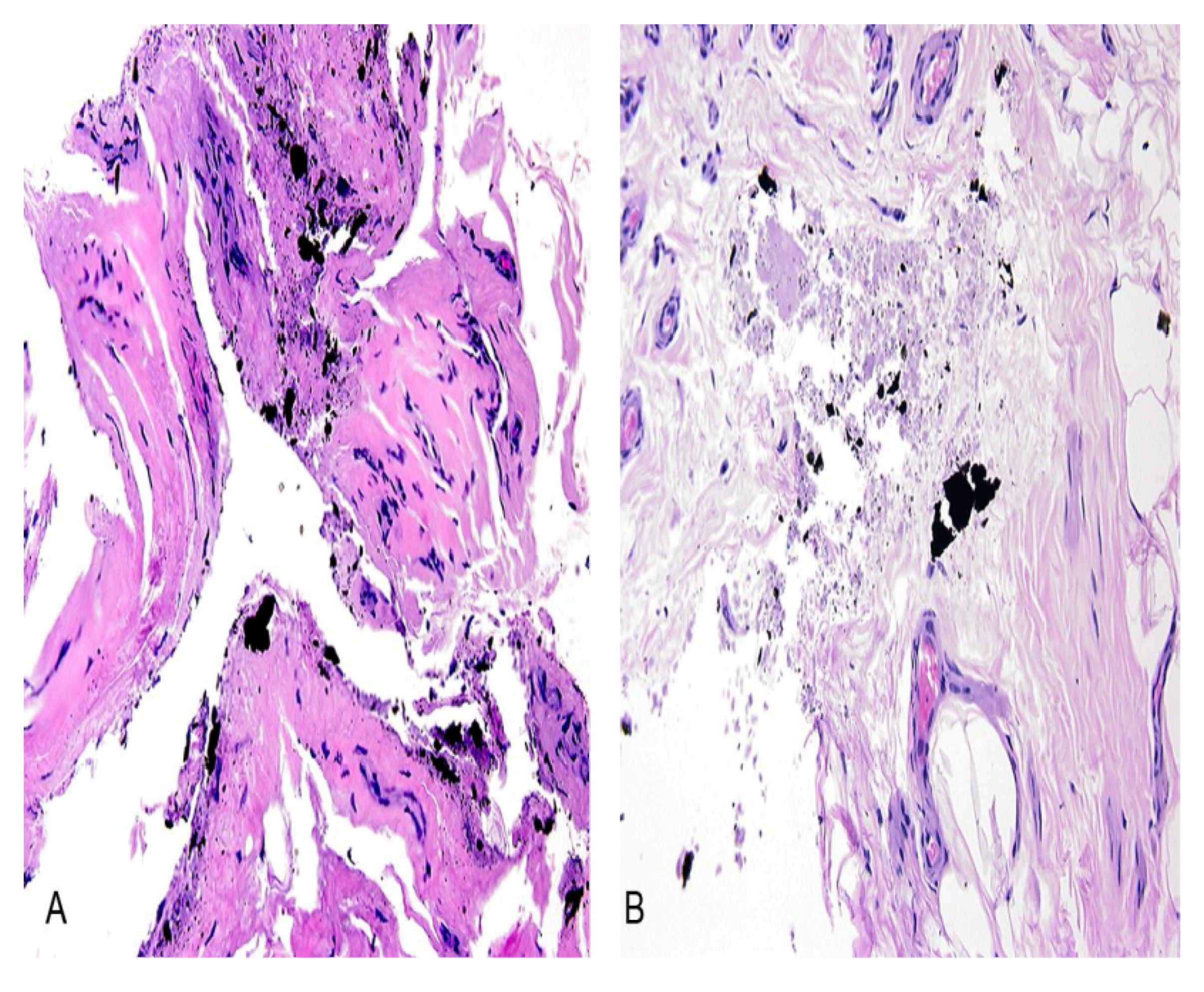
3.2.1. Case Number 1

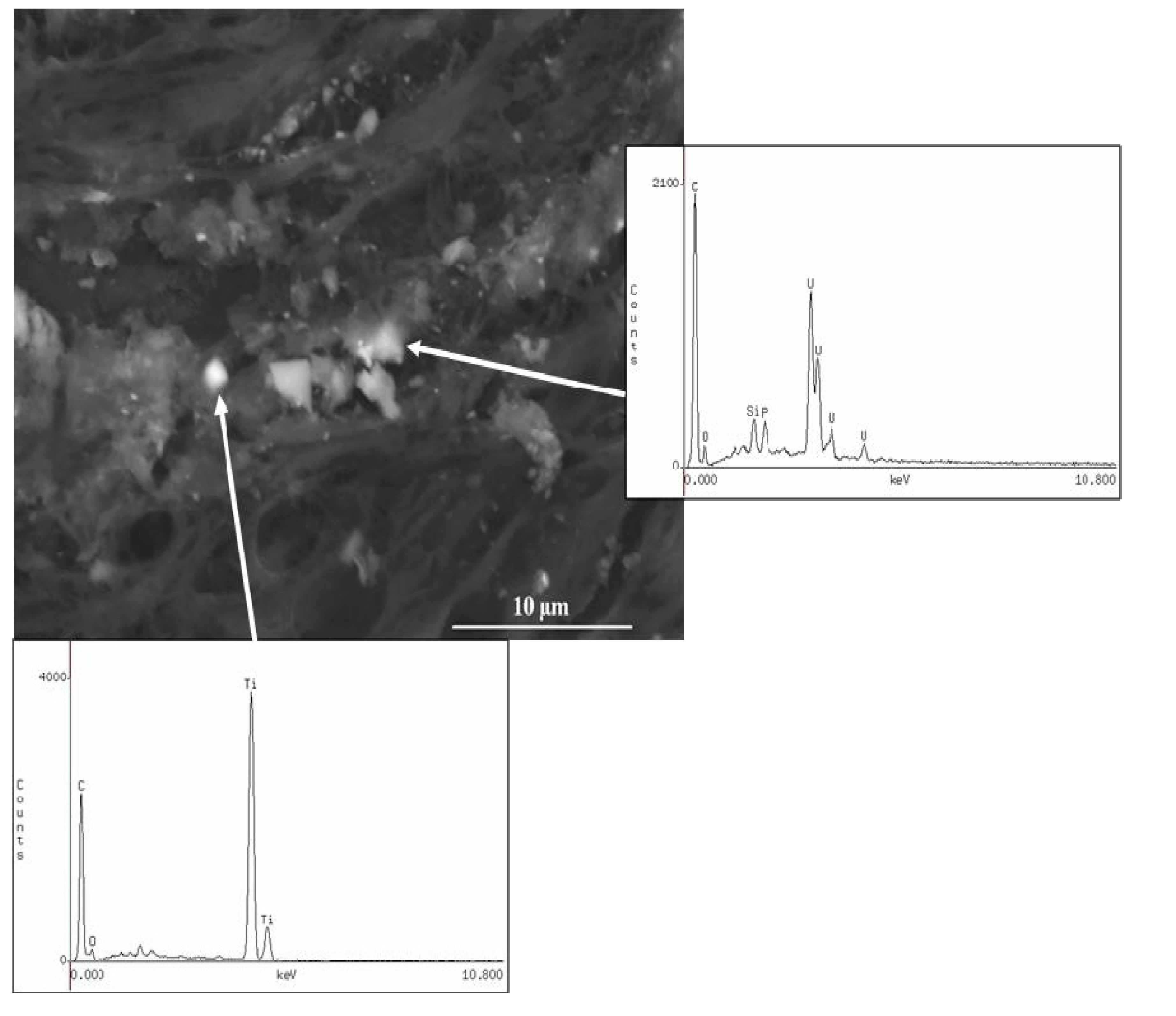
3.2.2. Case Number 2
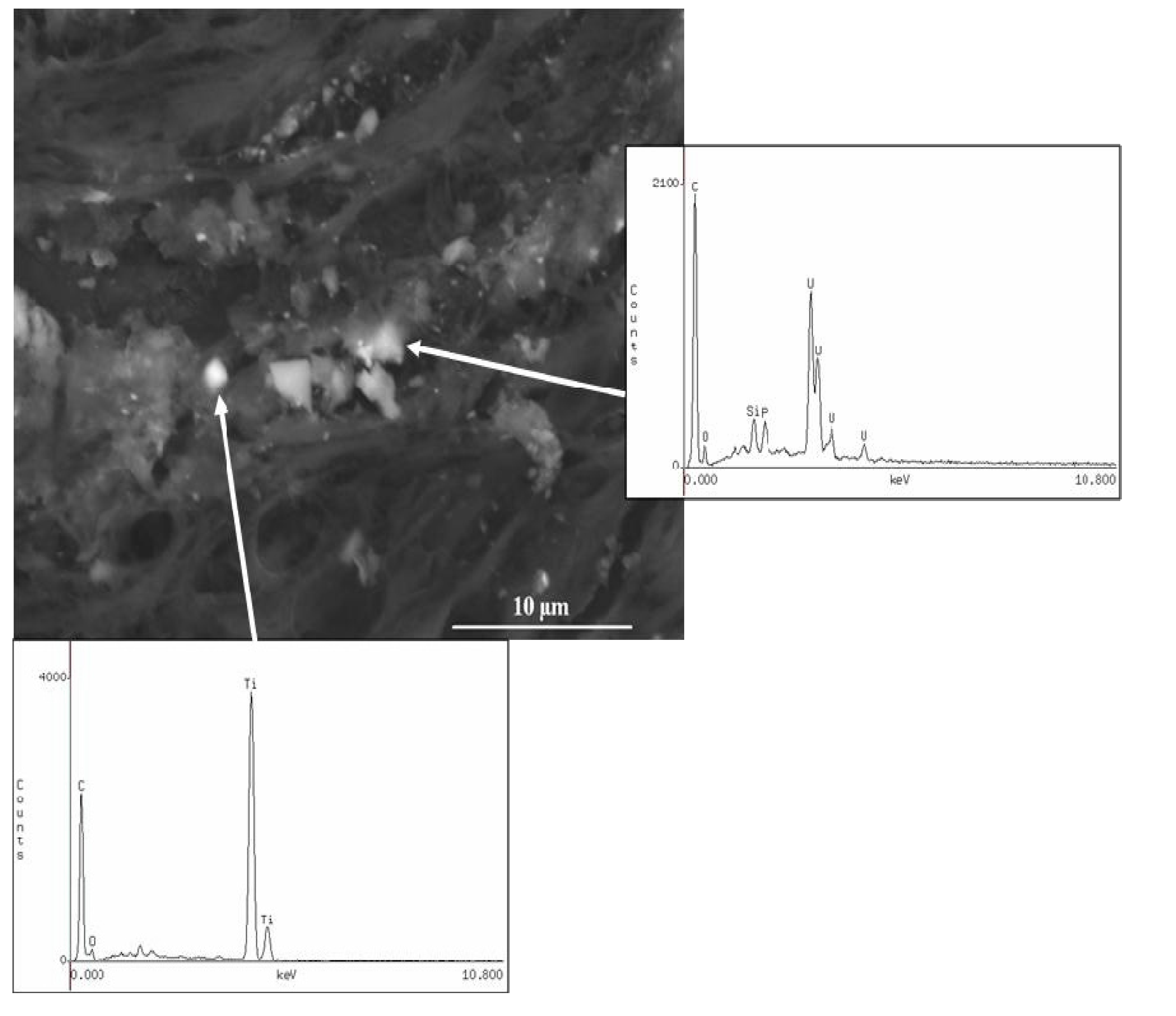
| Element | Fragment #1 (µg/g, ppm) | Fragment #2 (µg/g, ppm) | Fragment #3 |
|---|---|---|---|
| U | 204,179 | 15,659 | 924,872 |
| 235U/238U *** | 0.0022 * | 0.0023 * | 0.0022 * |
| W | 194 | 81 | <DL ** |
| Ti | 1,993 | 199 | 1,340 |
| Cu | 378 | 112 | 12 |
| Al | 738 | 15,030 | <DL |
| Mg | 305 | 517 | 14 |
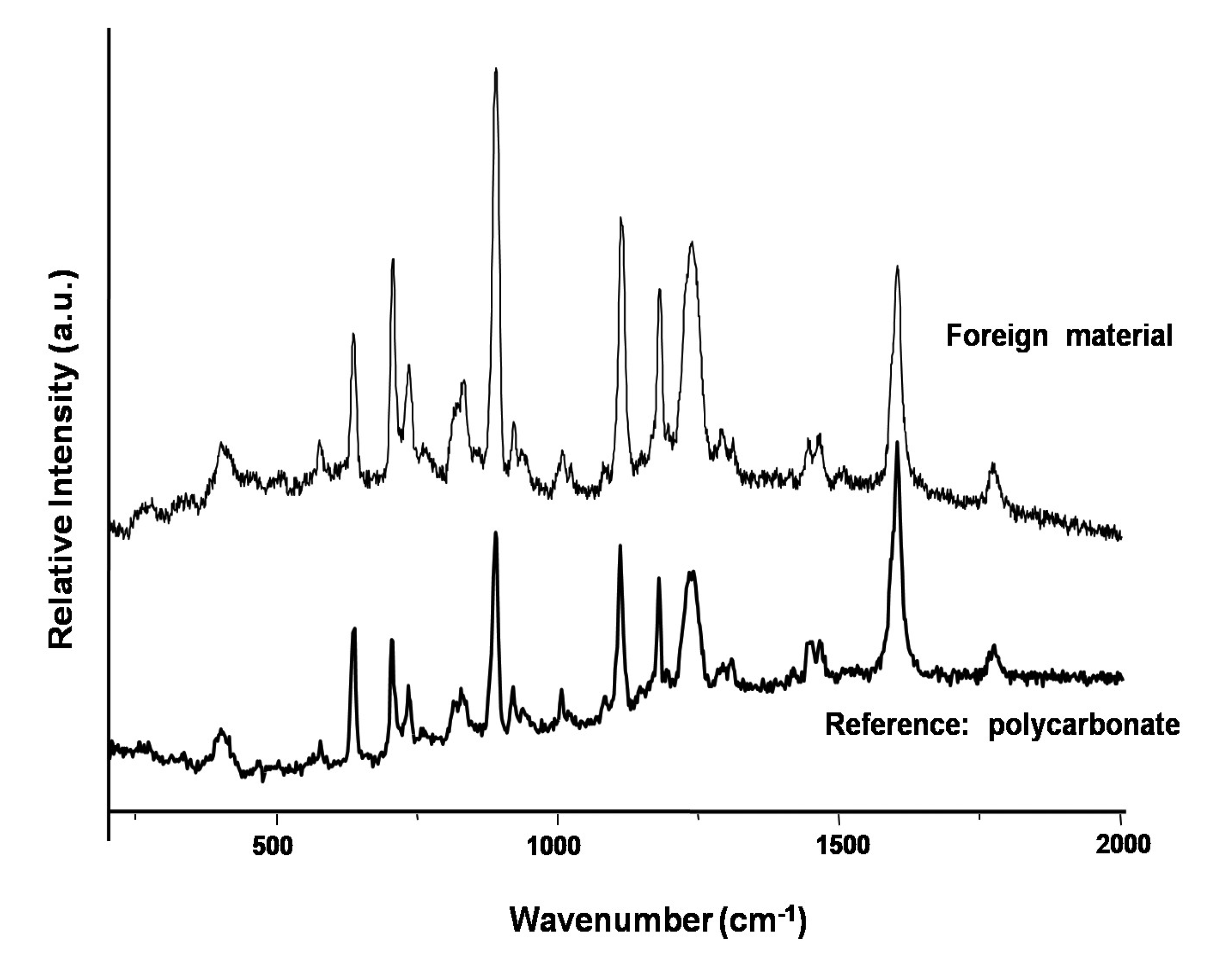
3.2.3. Case Number 3

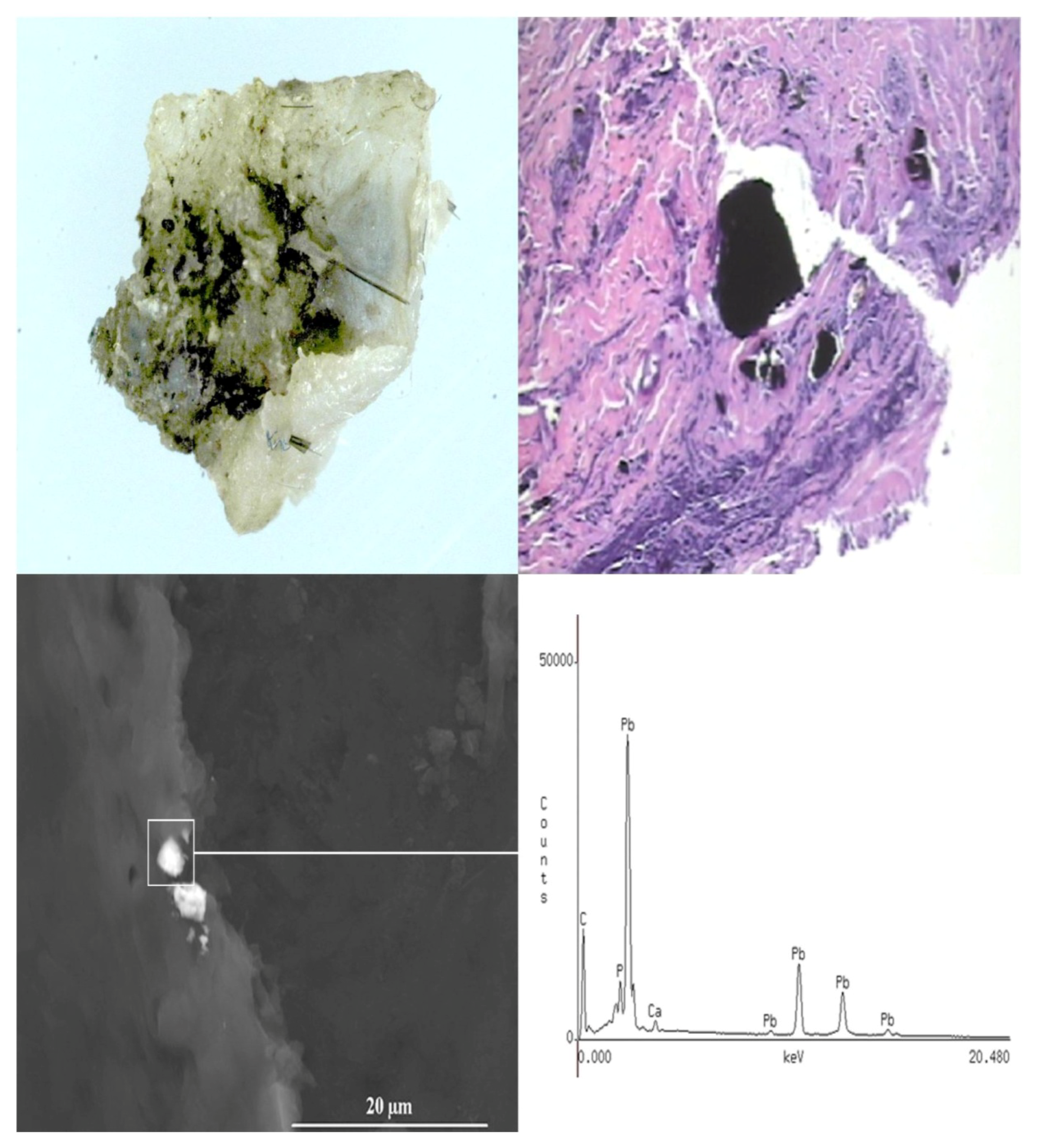
3.2.4. Case Number 4

4. Discussion
5. Conclusions
Acknowledgments
Disclaimer
Conflicts of Interest
References
- Champion, H.R.; Bellamy, R.F.; Roberts, C.P.; Leppaniemi, A. A profile of combat injury. J. Trauma 2003, 54, S13–S19. [Google Scholar]
- Spalding, T.J.; Stewart, M.P.; Tulloch, D.N.; Stephens, K.M. Penetrating missile injuries in the Gulf War 1991. Br. J. Surg. 1991, 78, 1102–1104. [Google Scholar] [CrossRef]
- Giannou, C.; Baldan, M. War Surgery—Working with Limited Resources in Armed Conflict and Other Situations of Violence 2011; ICRC: Geneva, Switzerland, 2011; Volume I, p. 224. [Google Scholar]
- Depleted Uranium—Properties, Uses and Health Consequences; Miller, A.C. (Ed.) CRC Press: Boca Raton, FL, USA, 2007.
- Bleise, A.; Danesi, P.R.; Burkart, W. Properties, use and health effects of depleted uranium (DU): A general overview. J. Environ. Radioact. 2003, 64, 93–112. [Google Scholar] [CrossRef]
- Van der Voet, G.B.; Todorov, T.I.; Centeno, J.A.; Jonas, W.; Ives, J.; Mullick, F.G. Metals and health: A clinical toxicological perspective on tungsten and review of the literature. Mil. Med. 2007, 179, 1002–1005. [Google Scholar]
- Miller, A.C.; Mog, S.; McKinney, L.; Luo, L.; Allen, J.; Xu, J.; Page, N. Neoplastic transformation of human osteoblast cells to the tumorigenic phenotype of heavy metal-tungsten alloy particles—Induction of genotoxic effects. Carcinogenesis 2001, 22, 115–125. [Google Scholar] [CrossRef]
- Miller, A.C.; Brooks, K.; Smith, J.; Page, N. Effects of the military-relevant heavy metals, depleted uranium and heavy metal tungsten-alloy on gene expression in human liver carcinoma cells (HepG2). Mol. Cell. Biochem. 2004, 255, 247–256. [Google Scholar] [CrossRef]
- Kalinich, J.F.; Emond, C.A.; Dalton, T.K.; Mog, S.R.; Coleman, G.D.; Kordell, J.E.; Miller, A.C.; McClain, D.E. Embedded weapons-grade tungsten alloy shrapnel rapidly induces metastatic high-grade rhabdomyosarcomas in F344 rats. Environ. Health Perspect. 2005, 113, 729–734. [Google Scholar] [CrossRef]
- Schuster, B.E.; Roszell, L.E.; Murr, L.E.; Ramirez, D.A.; Demaree, J.D.; Klotz, B.R.; Rosencrance, A.B.; Dennis, W.E.; Bao, W.; Perkins, E.J.; et al. In vivo corosion, tumor outcome, and micrarray gene expression for two types of muscle-implanted tunsgten alloys. Toxicol. Appl. Pharmacol. 2012, 265, 128–138. [Google Scholar] [CrossRef]
- Eylon, S.; Mosheiff, R.; Liebergall, M.; Wolf, E.; Brocke, L.; Peyser, A. Delayed reaction to shrapnel retained in soft tissue. Injury 2005, 36, 275–281. [Google Scholar] [CrossRef]
- Policy on Analysis of Metal Fragments Removed from Department of Defense Personnel. Available online: http://www.health.mil/Content/docs/pdfs/policies/2007/07-029.pdf (accessed on 4 March 2013).
- Centeno, J.A.; Mullick, F.G.; Panos, R.G.; Miller, F.W.; Velenzuela-Espinoza, A. Laser Raman microprobe identification of inclusions in capsules associated with silicone gel breast implants. Med. Pathol. 1999, 12, 714–721. [Google Scholar]
- Baydur, A.; Koss, M.N.; Sharma, O.P.; Dalgleish, G.E.; Nguyen, D.V.; Mullick, F.G.; Murakata, L.A.; Centeno, J.A. Microscopic pulmonary embolization of an indwelling central venous catheter with granulomatous inflammatory response. Eur. Respir. J. 2005, 26, 351–353. [Google Scholar] [CrossRef]
- Ejnik, J.W.; Todorov, T.I.; Squibb, K.; McDiarmid, M.A.; Centeno, J.A. Uranium analysis in urine by inductively coupled plasma dynamic reaction cell mass spectrometry. Anal. Bioanal. Chem. 2005, 382, 73–79. [Google Scholar] [CrossRef]
- Todorov, T.I.; Xu, H.; Ejnik, J.W.; Mullick, F.G.; Squibb, K.; McDiarmid, M.A.; Centeno, J.A. Depleted uranium in blood by inductively coupled plasma mass spectrometry. J. Anal. At. Spectrom. 2009. [Google Scholar] [CrossRef]
- Burgio, L.; Clark, R.J.H.; Firth, S. Raman spectroscopy as a means for the identification of plattnerite (PbO2) of lead pigments and of their degradation products. Analyst 2001, 126, 222–227. [Google Scholar] [CrossRef]
- Petersen, K.; Riddle, M.S.; Danko, J.R.; Blazes, D.L.; Hayden, R.; Tasker, S.A.; Dunne, J.R. Trauma-related infections from battlefield casualties from Iraq. Ann. Surg. 2007, 245, 803–811. [Google Scholar] [CrossRef]
- Bowyer, G.W.; Cooper, G.J.; Rice, P. Management of small fragment wounds in war: Current research. Ann. R. Coll. Surg. Engl. 1995, 77, 131–134. [Google Scholar]
- Bowyer, G.W. Management of small fragment wounds: Experience from the Afghan border. J. Trauma 1996, 40, S170–S172. [Google Scholar] [CrossRef]
- Bowyer, G.W. Management of small fragment wounds in modern warfare: A return to Hunterian principles? Ann. R. Coll. Surg. Engl. 1997, 79, 175–182. [Google Scholar]
- Hoffer, M.M.; Johnson, B. Shrapnel wounds in children. J. Bone Joint Surg. Am. 1992, 74, 766–769. [Google Scholar]
- Nikolic, D.; Jovanovic, Z.; Popovic, Z.; Vulovic, R.; Mladenovic, M. Primary surgical treatment of war injuries of major joints of the limbs. Injury 1999, 30, 129–134. [Google Scholar] [CrossRef]
- Weigl, D.M.; Bar-On, E.; Katz, K. Small-fragment wounds from explosive devices: Need for and timing of fragment removal. J. Pediatr. Orthop. 2005, 25, 158–161. [Google Scholar] [CrossRef]
- Biddau, F.; Fioriti, M.; Benelli, G. Migration of a broken cerclage wire from the patella into the heart: A case report. J. Bone Joint Surg. Am. 2006, 88, 2057–2059. [Google Scholar] [CrossRef]
- Wirth, M.A.; Lakoski, S.G.; Rockwood, C.A., Jr. Migration of a broken cerclage wire from the shoulder girdle into the heart: A case report. J. Should. Elb. Surg. 2000, 9, 543–544. [Google Scholar] [CrossRef]
- Foster, G.T.; Chetty, K.G.; Mahutte, K.; Kim, J.B.; Sasse, S.A. Hemoptysis due to migration of a fractured Kirschner wire. Chest 2001, 119, 1285–1286. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. In Surgical Implants and Other Foreign Bodies 1999; IARC: Lyon, France, 1999; Volume 74, pp. 113–229.
- Lindeman, G.; McKay, M.J.; Taubman, K.L.; Bilous, A.M. Malignant fibrous histiocytoma developing in bone 44 years after shrapnel trauma. Cancer 1990, 66, 2229–22232. [Google Scholar] [CrossRef]
- Silverman, W.B. Sclerosing cholangitis caused by old shrapnel injury. Gastrointest. Endosc. 2003, 58, 420–423. [Google Scholar] [CrossRef]
- Surov, A.; Taege, C.; Behrmann, C. A delayed complication after injury in World War II. N. Engl. J. Med. 2006, 354, 1963–1964. [Google Scholar] [CrossRef]
- Hayman, J.; Huygens, H. Angiosarcoma developing around a foreign body. J. Clin. Pathol. 1983, 36, 515–518. [Google Scholar] [CrossRef]
- Philip, J. Squamous cell carcinoma arising at the site of an underlying bullet. J. R. Coll. Surg. Edinb. 1982, 27, 365–366. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Centeno, J.A.; Rogers, D.A.; Van der Voet, G.B.; Fornero, E.; Zhang, L.; Mullick, F.G.; Chapman, G.D.; Olabisi, A.O.; Wagner, D.J.; Stojadinovic, A.; et al. Embedded Fragments from U.S. Military Personnel—Chemical Analysis and Potential Health Implications. Int. J. Environ. Res. Public Health 2014, 11, 1261-1278. https://doi.org/10.3390/ijerph110201261
Centeno JA, Rogers DA, Van der Voet GB, Fornero E, Zhang L, Mullick FG, Chapman GD, Olabisi AO, Wagner DJ, Stojadinovic A, et al. Embedded Fragments from U.S. Military Personnel—Chemical Analysis and Potential Health Implications. International Journal of Environmental Research and Public Health. 2014; 11(2):1261-1278. https://doi.org/10.3390/ijerph110201261
Chicago/Turabian StyleCenteno, José A., Duane A. Rogers, Gijsbert B. Van der Voet, Elisa Fornero, Lingsu Zhang, Florabel G. Mullick, Gail D. Chapman, Ayodele O. Olabisi, Dean J. Wagner, Alexander Stojadinovic, and et al. 2014. "Embedded Fragments from U.S. Military Personnel—Chemical Analysis and Potential Health Implications" International Journal of Environmental Research and Public Health 11, no. 2: 1261-1278. https://doi.org/10.3390/ijerph110201261