
Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
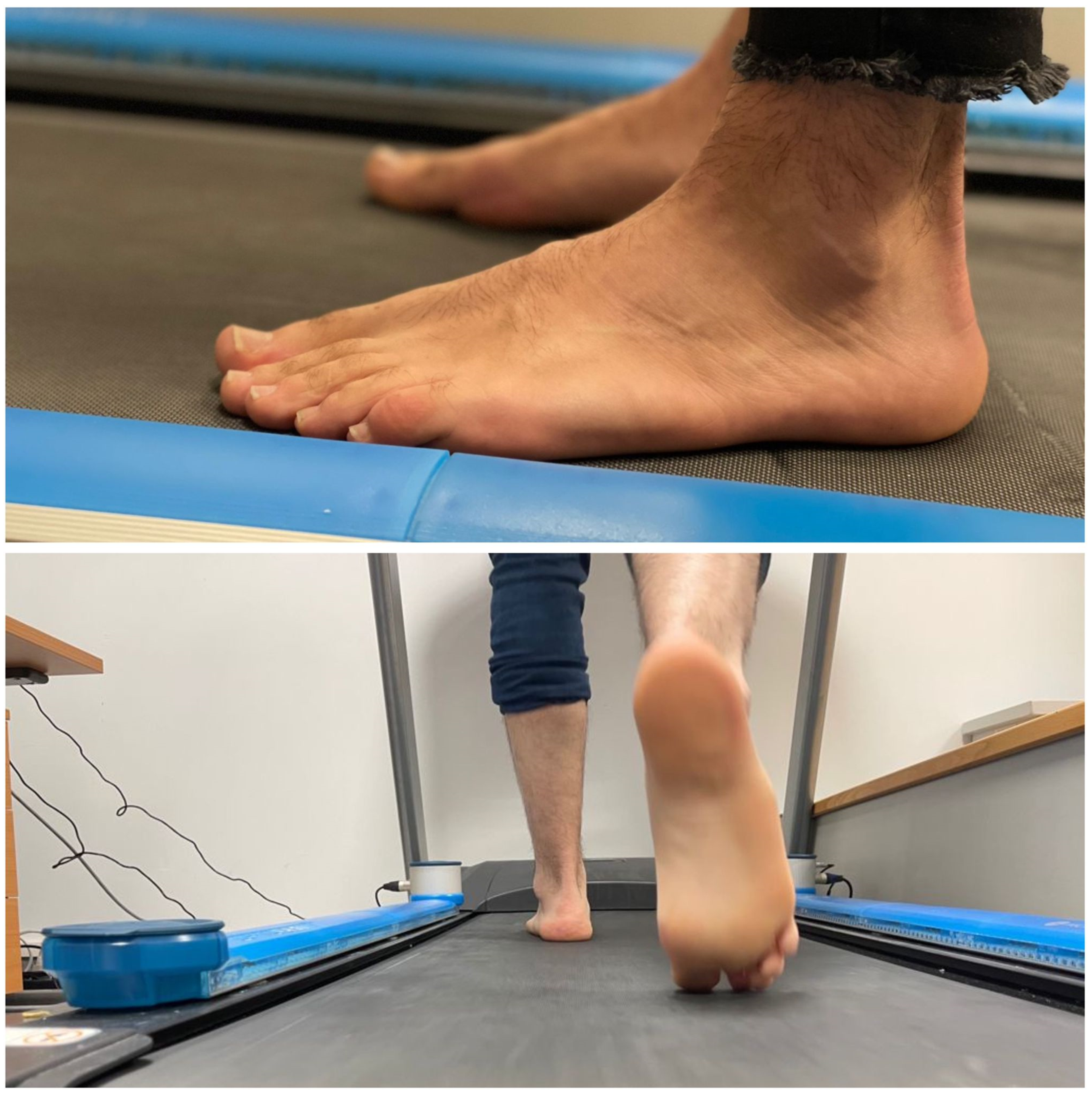
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Description of the Total Sample and by Groups
3.2. Statistical Analysis
4. Discussion
5. Conclusions
5.1. Limitations
5.2. Practical Implications of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, R.; Sosnoff, J.J. Novel sensing technology in fall risk assessment in older adults: A systematic review. BMC Geriatr. 2018, 18, 14. [Google Scholar] [CrossRef]
- Stevens, J.A. Falls among older adults—Risk factors and prevention strategies. J. Safety Res. 2005, 36, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Hanatsu, N.H.; Begg, R.K. Shoe-Insole Technology for Injury Prevention in Walking. Sensors 2018, 18, 1468. [Google Scholar] [CrossRef]
- Menz, H.B.; Maria, A.; Martin, J.S. Foot problems as a risk factor for falls in community-dwelling older people: A systematic review and meta-analysis. Maturitas 2018, 118, 14. [Google Scholar] [CrossRef]
- Shengwu, Y.L. Effects of Step Retraining on impact forces, lower limb biomechanics and leg stiffness. J. Biomed. Eng. 2020, 35, 665–671. [Google Scholar]
- Lee, M.; Song, C.; Lee, K.; Shin, D.; Shin, S. Agreement between the spatio-temporal gait parameters from treadmill-based photoelectric cell and the instrumented treadmill system in healthy young adults and stroke patients. Med. Sci. Monit. 2014, 20, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Jaén-Carrillo, D.; García-Pinillos, F.; Cartón-Llorente, A.; Almenar-Arasanz, A.J.; Bustillo-Pelayo, J.A.; Roche-Seruendo, L.E. Prueba-reprueba la confiabilidad del Sistema OptoGait para el análisis de los parámetros de la marcha en Carrera espacio-temporal y la rigidez de la parte inferior del cuerpo en adultos sanos. Actas Inst. Ing. Mecánicos Parte P Rev. Ing. Tecnol. Deport. 2020, 234, 154–161. [Google Scholar] [CrossRef]
- User Manual. Microgate, Bolzano, Italia OptoGait. Available online: http://www.optogait.com/OptoGaitPortal/Media/Manuals/Manual-ES.PDF (accessed on 21 January 2021).
- Demirel, A.; Onan, D.; Oz, M.; Ozel, A.Y.; Ulger, O. Moderate disability has negative effect on spatiotemporal parameters in patients with chronic low back pain. Gait Posture 2020, 79, 251–255. [Google Scholar] [CrossRef]
- Canuel-Laurenson, É. Effect of foot orthoses on walking performance and quality in the elderly. Rev. Du Podol. 2020, 16, 16–20. [Google Scholar] [CrossRef]
- Calvo-Lobo, C.; Painceira-Villar, R.; García-Paz, V.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Munuera-Martínez, P.V.; López-López, D. Falls rate increase and foot dorsal flexion limitations are exhibited in patients who suffer from asthma: A novel case-control study. Int. J. Med. Sci. 2019, 16, 607–613. Available online: https://www.medsci.org/v16p0607.htm (accessed on 24 January 2021). [CrossRef]
- Sánchez-Rodríguez, R.; Valle-Estévez, S.; Fraile-García, P.A.; Martínez-Nova, A.; Gómez-Martín, B.; Escamilla-Martínez, E. Modification of Pronated Foot Posture after a Program of Therapeutic Exercises. Int. J. Environ. Res. Public Health 2020, 17, 8406. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Kumar, N. Investigations on postural stability and spatiotemporal parameters of human gait using developed wearable smart insole. J. Med. Eng. Technol. 2014, 39, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Redmond, A.C.; Crane, Y.Z.; Menz, H.B. Normative values for the Foot Posture Index. J. Foot. Ankle Res. 2008, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Declaración de Helsinki de la AMM—Principios éticos Para Las Investigaciones Médicas en Seres Humanos Asamblea General de la AMM, Fortaleza, Brasil, Octubre de 2013. Available online: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/ (accessed on 25 December 2019).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S. Strengthening the Reporting of Observational etudies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [PubMed]
- User Manual. Microgate, Bolzano, Italia OptoGait, Gait Parameters. Available online: http://www.optogait.com/Aplicaciones/Ritmo-optimo-de-marcha (accessed on 3 February 2021).
- Muchna, A.; Najafi, B.; Wendel, C.S.; Schwenk, M.; Armstrong, D.G.; Mohler, J. Foot problems in older adults: Associations with incident falls, frailty syndrome and sensor-derived gait, balance, and physical activity measures. J. Am. Podiatr. Med. Assoc. 2017, 108, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Khan, T.; Wrobel, J. Laboratory in a box: Wearable sensors and its advantages for gait analysis. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 6507–6510. [Google Scholar] [CrossRef]
- Dodelin, D.; Tourny, C.; L’Hermette, M. The biomechanical effects of pronated foot function on gait. An experimental study. Scand. J. Med. Sci. Sports 2020, 30, 2167–2177. [Google Scholar] [CrossRef]
- Buldt, A.K.; Allan, J.J.; Landorf, K.B.; Menz, H.B. The relationship between foot posture and plantar pressure during walking in adults: A systematic review. Gait Posture 2018, 62, 56–67. [Google Scholar] [CrossRef]
- Mattacola, C.G.; Dwyer, M.K.; Miller, A.K.; Uhl, T.L.; McCrory, J.L.; Malone, T.R. Effect of orthoses on postural stability in asymptomatic subjects with rearfoot malalignment during a 6-week acclimation period. Arch. Phys. Med. Rehabil. 2007, 88, 653–660. [Google Scholar] [CrossRef]
- Rome, K.; Marrón, C.L. Randomized clinical trial into the impact of rigid foot orthoses on balance parameters in excessively pronated feet. Reh. Clin. 2004, 18, 624–630. [Google Scholar] [CrossRef]
- Gross, M.T.; Mercer, V.S.; Lin, F.C. Effects of foot orthoses on balance in older adults. J. Orthop. Sports Phys. Ther. 2012, 42, 649–657. [Google Scholar] [CrossRef]
- Banwell, H.A.; Mackintosh, S.; Thewlis, D. Foot orthoses for adults with flexible pes planus: A systematic review. J. Foot Ankle Res. 2014, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Chaiwanichsiri, D.; Janchai, S.; Tantisiriwat, N. Foot Disorders and Falls in Older Persons. Gerontology 2009, 55, 296–302. [Google Scholar] [CrossRef]
- Menz, H.B.; Auhl, M.; Tan, J.M.; Andrew, K.B.; Shannon, E.M. Centre of pressure characteristics during walking in individuals with and without first metatarsophalangeal joint osteoarthritis. Gait Posture 2018, 63, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Hua, R.; Wang, Y. Monitoring Insole (MONI): A Low Power Solution toward Daily Gait Monitoring and Analysis. IEEE Sens. J. 2019, 19, 6410–6420. [Google Scholar] [CrossRef]
- Hollman, J.; McDade, E.; Petersen, R. Normative spatiotemporal gait parameters in older adults. Gait Posture 2010, 34, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Wong, I.K.-K.; Chen, T.L.-W.; Hong, T.T.-H.; Wong, D.W.-C.; Peng, Y.; Yan, F.; Wang, Y.; Tan, Q.; Zhang, M. Identifying Fatigue Indicators Using Gait Variability Measures: A Longitudinal Study on Elderly Brisk Walking. Sensors 2020, 20, 6983. [Google Scholar] [CrossRef]
- Tong, J.W.; Kong, P.W. Association between Foot Type and Lower Extremity Injuries: Systematic Literature Review with Meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 700–714. [Google Scholar] [CrossRef]
- Jafarnezhadgero, A.; Alavi-Mehr, S.M.; Granacher, U. Effects of anti-pronation shoes on lower limb kinematics and kinetics in female runners with pronated feet: The role of physical fatigue. PLoS ONE 2019, 14, e0216818. [Google Scholar] [CrossRef]
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine 2019, 98, 16218. [Google Scholar] [CrossRef]
- Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 10 February 2021).
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–22. [Google Scholar] [CrossRef]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Foot and ankle risk factors for falls in older people: A prospective study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 866–870. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample N = 142 | Group | |||
|---|---|---|---|---|
| Case n = 70 | Control n = 72 | p-Value | ||
| Gender Female | 75 (52.8%) | 38 (54.32%) | 37 (51.38%) | p = 0.427 a |
| BMI | 22.55 (3.11) | 23.00 (3.54) | 22.00 (4.40) | p = 0.082 b |
| FPI right foot | 4.65 (3.00) | 7.00 (1.00) | 4.00 (4.00) | p = 0.001 b |
| FPI left foot | 4.30 (4.00) | 7.00 (1.20) | 4.00 (3.80) | p = 0.001 b |
| Sample n = 142 p-Value | Group | |||
|---|---|---|---|---|
| Case n = 70 | Control n = 72 | p-Value | ||
| Right foot stride length | 60.70 (4.60) | 62.50 (7.75) | 60.40 (1.70) | p = 0.022 |
| Left foot stride length | 60.85 (4,48) | 62.70 (5.75) | 60.30 (2.75) | p = 0.019 |
| Ground contact time, | ||||
| right foot sec | 0.54 (0.05) | 0.59 (0.06) | 0.54 (0.01) | p = 0.001 |
| Step % | 70.90 (6.63) | 71.10 (4.55) | 70.50 (6.75) | p = 0.460 |
| Ground contact time, | ||||
| left foot sec | 0.54 (0.03) | 0.57(0.06) | 0.54 (0.03) | p = 0.001 |
| Step % | 70.60 (6.00) | 70.90(5.00) | 70.40 (7.40) | p = 0.081 |
| Gait cycle sec | 1.11 (0.09) | 1.16 (0.09) | 1.09 (0.05) | p = 0.001 |
| Gait cadence | 107.90 (8.83) | 102.40 (13.20) | 109.00 (3.70) | p = 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requelo-Rodríguez, I.; Castro-Méndez, A.; Jiménez-Cebrián, A.M.; González-Elena, M.L.; Palomo-Toucedo, I.C.; Pabón-Carrasco, M. Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study. Sensors 2021, 21, 2805. https://doi.org/10.3390/s21082805
Requelo-Rodríguez I, Castro-Méndez A, Jiménez-Cebrián AM, González-Elena ML, Palomo-Toucedo IC, Pabón-Carrasco M. Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study. Sensors. 2021; 21(8):2805. https://doi.org/10.3390/s21082805
Chicago/Turabian StyleRequelo-Rodríguez, Inmaculada, Aurora Castro-Méndez, Ana María Jiménez-Cebrián, María Luisa González-Elena, Inmaculada C. Palomo-Toucedo, and Manuel Pabón-Carrasco. 2021. "Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study" Sensors 21, no. 8: 2805. https://doi.org/10.3390/s21082805
APA StyleRequelo-Rodríguez, I., Castro-Méndez, A., Jiménez-Cebrián, A. M., González-Elena, M. L., Palomo-Toucedo, I. C., & Pabón-Carrasco, M. (2021). Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study. Sensors, 21(8), 2805. https://doi.org/10.3390/s21082805