Low-Cost Tracking Systems Allow Fine Biomechanical Evaluation of Upper-Limb Daily-Life Gestures in Healthy People and Post-Stroke Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim
2.2. Settings
2.3. Participants
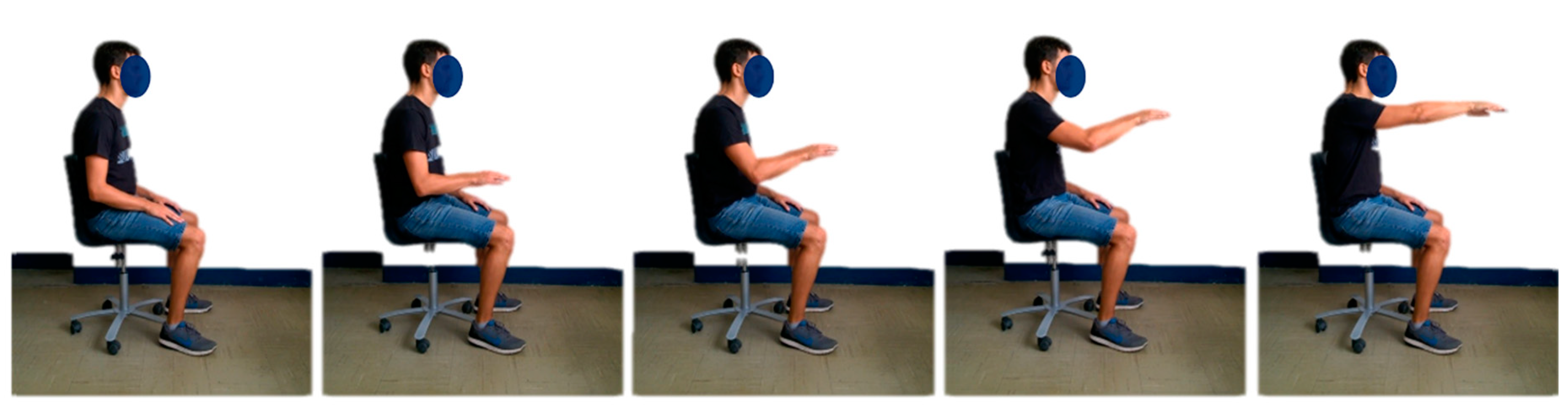
2.4. Experimental Set-up
- A Microsoft Kinect V2 sensor version 2.0, mounted on an easel and placed at about a 2.0 m distance from the torso of the subject. The 2.0 m distance was chosen since it is halfway from 0.8 and 3.2 m, which were indicated by Microsoft as the range of distances to use for exploiting the tracking functions of the device. The Kinect V2 was placed about 10 cm under shoulder height, and precisely in front of the subject, about halfway between the limbs. A tolerance of some centimeters had to be accepted, due to the patients’ different anthropometry and sitting postures. Considering that the use of Kinect V2 was meant for future use, even in environments that are non-supervised by medical personnel (such as the patient’s home), where even less-controlled conditions are found, this approximations were considered as reasonable.
- In house software C# for on-line feedback and data logging;
- A PC with Microsoft Windows 8.1, USB 3.0, and Microsoft Kinect One S.D.K. version 2.0;
- A screen providing on-line visual feedback to the operator to visually monitor the correctness of the kinematic tracking.
2.5. Patient Clinical Assessment: The Reaching Performance Scale
2.6. Data Sources and Measurements
2.7. Outcome Measures
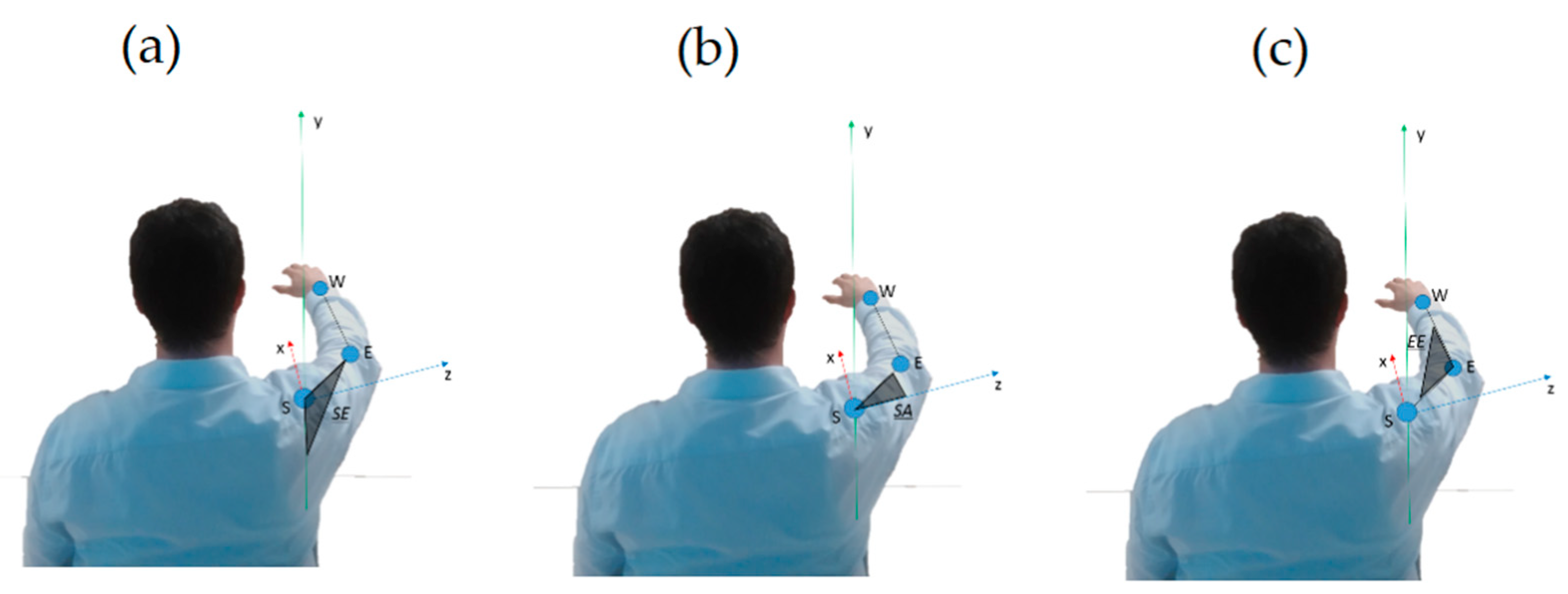
2.7.1. Kinematics and Range of Motion
- Shoulder Elevation angle (SE, °)
- Shoulder Rotation along Vertical Axis angle (SA, °)
- Elbow Extension angle (EE, °)
2.7.2. Compensatory Strategies
- Trunk Compensus (TC, [])
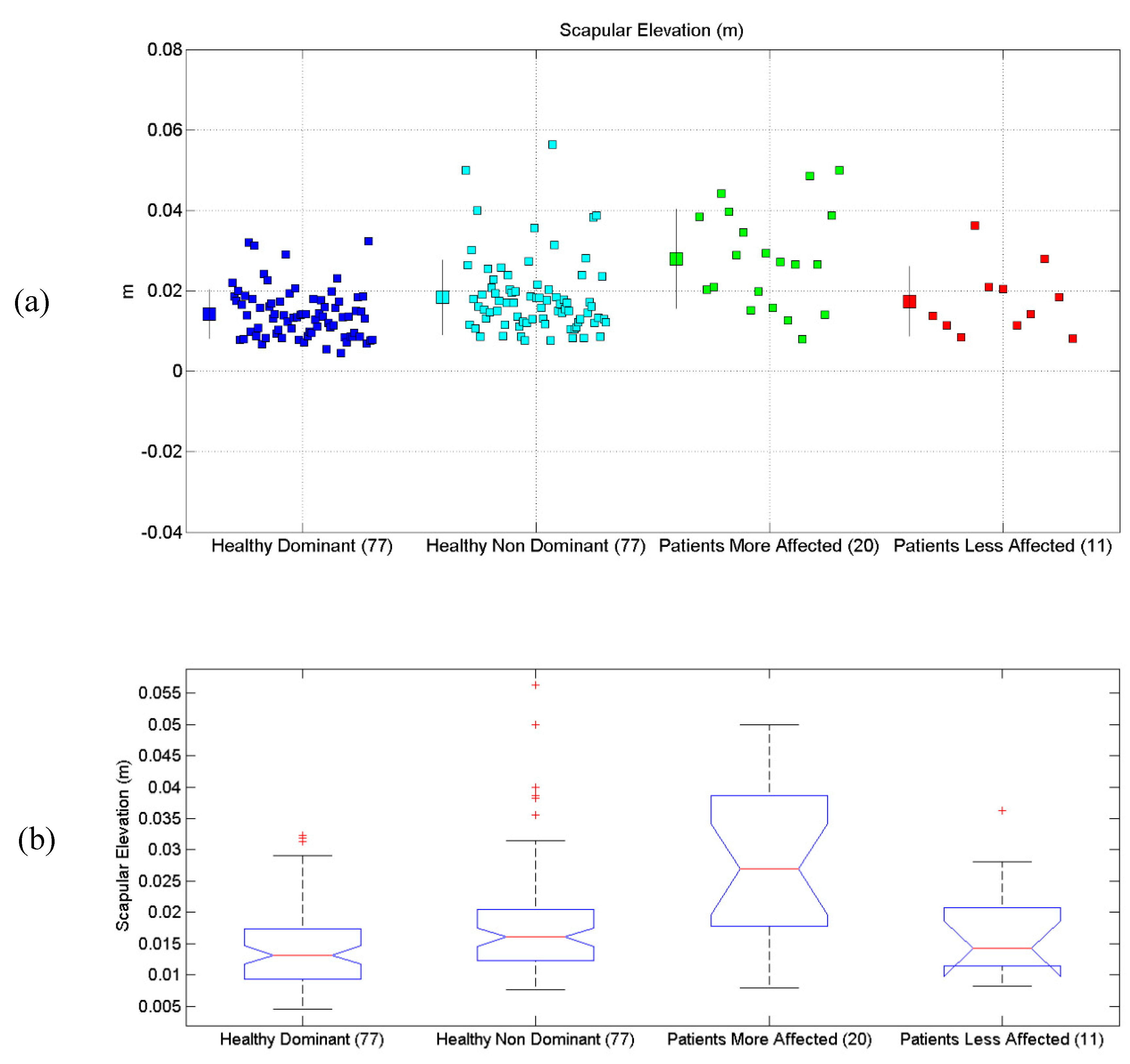
- Scapular Elevation (ScE, m)
2.7.3. Motor Control and Motion Quality
2.8. Study Design
2.9. Statistics
3. Results
3.1. Shoulder Elevation Angle
3.2. Shoulder Rotation Angle (Along Vertical Axis)
3.3. Elbow Extension Angle
3.4. Scapular Elevation
3.5. Trunk Compensus
3.6. Average Number of Velocity Peaks
4. Discussion
4.1. On the Biomechanical Results
4.2. Kinect in Real Applications
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statements
References
- Hobart, J.; Cano, S. Rating scales for clinical studies in neurology—Challenges and opportunities. US Neurol. 2008, 4, 12–18. [Google Scholar] [CrossRef]
- World Health Organization. Towards a Common Language for Functioning, Disability and Health ICF. Int. Classif. Funct. Disabil. Health 2002, 1149, 1–22. [Google Scholar]
- Della Mea, V.; Simoncello, A. An ontology-based exploration of the concepts and relationships in the activities and participation component of the international classification of functioning, disability and health. J. Biomed. Semant. 2012, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, K.; Fulk, G.D.; Salem, Y.; Sullivan, J. Outcome measures in neurological physical therapy practice: Part I. Making sound decisions. J. Neurol. Phys. Ther. 2011, 35, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.K.; McArthur, K.S.; Quinn, T.J. Assessment scales in stroke: Clinimetric and clinical considerations. Clin. Interv. Aging 2013, 8, 201–211. [Google Scholar] [PubMed]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative assessment of upper limb motor function in Multiple Sclerosis using an instrumented Action Research Arm Test. J. Neuroeng. Rehabil. 2014, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Roux, E.; Bouilland, S.; Godillon-Maquinghen, A.-P.; Bouttens, D. Evaluation of the GO Method within the Upper Limb Kinematics Analysis. J. Biomech. 2002, 35, 1279–1283. [Google Scholar] [CrossRef]
- Petuskey, K.; Bagley, A.; Abdala, E.; James, M.A.; Rab, G. Upper extremity kinematics during functional activities: Three-dimensional studies in a normal pediatric population. Gait Posture 2007, 25, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Cappozzo, A.; Catani, F.; Leardini, A.; Benedetti, M.G.; Della Croce, U. Position and orientation in space of bones during movement: Experimental artefacts. Clin. Biomech. 1996, 11, 90–100. [Google Scholar] [CrossRef]
- Lobo-Prat, J.; Font-Llagunes, J.M.; Gómez-Pérez, C.; Medina-Casanovas, J.; Angulo-Barroso, R.M. New biomechanical model for clinical evaluation of the upper extremity motion in subjects with neurological disorders: An application case. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 1144–1156. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Leone, A. Training modalities in robot-mediated upper limb rehabilitation in stroke: A framework for classification based on a systematic review. J. Neuroeng. Rehabil. 2014, 11, 111. [Google Scholar]
- Schmidt, R. A Schema Theory of Discrete Motor Skill Learning. Psychol. Rev. 1975, 82, 225–260. [Google Scholar] [CrossRef]
- Cameirão, M.S.; Smailagic, A.; Miao, G.; Siewiorek, D.P. Coaching or gaming? Implications of strategy choice for home based stroke rehabilitation. J. Neuroeng. Rehabil. 2016, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Beacon, J.F.; Comeau, G.; Payeur, P.; Russell, D. Assessing the suitability of Kinect for measuring the impact of a week-long Feldenkrais method workshop on pianists’ posture and movement. J. Music Technol. Educ. 2017, 10, 51–72. [Google Scholar] [CrossRef]
- Chang, Y.J.; Chen, S.F.; da Huang, J. A Kinect-based system for physical rehabilitation: A pilot study for young adults with motor disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.J.; Han, W.Y.; Tsai, Y.C. A Kinect-based upper limb rehabilitation system to assist people with cerebral palsy. Res. Dev. Disabil. 2013, 34, 3654–3659. [Google Scholar] [CrossRef] [PubMed]
- González-Ortega, D.; Díaz-Pernas, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M. A Kinect-based system for cognitive rehabilitation exercises monitoring. Comput. Methods Programs Biomed. 2014, 113, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Jonsdottir, J.; Bertoni, R.; Lawo, M.; Montesano, A.; Bowman, T.; Gabrielli, S. Serious games for arm rehabilitation of persons with multiple sclerosis. A randomized controlled pilot study. Mult. Scler. Relat. Disord. 2018, 19, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Pedraza-Hueso, M.; Martín-Calzón, S.; Díaz-Pernas, F.J.; Martínez-Zarzuela, M. Rehabilitation Using Kinect-based Games and Virtual Reality. Procedia Comput. Sci. 2015, 75, 161–168. [Google Scholar] [CrossRef] [Green Version]
- Lange, B.; Chang, C.Y.; Suma, E.; Newman, B.; Rizzo, S.; Bolas, M. Development and evaluation of low cost game-based balance rehabilitation tool using the Microsoft Kinect sensor. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2011, 2011, 1831–1834. [Google Scholar] [PubMed]
- Gotsis, M.; Lympouridis, V.; Requejo, P.; Haubert, L.L.; Poulos, I.C.; Frangoudes, F.; Jordan-Marsh, M. Skyfarer: Design Case Study of a Mixed Reality Rehabilitation Video Game. In International Conference of Design, User Experience, and Usability; Springer: Berlin, Germany, 2014; pp. 699–710. [Google Scholar]
- Brokaw, E.B.; Eckel, E.; Brewer, B.R. Usability evaluation of a kinematics focused Kinect therapy program for individuals with stroke. Technol. Heal. Care 2015, 23, 143–151. [Google Scholar]
- Scano, A.; Caimmi, M.; Malosio, M.; Tosatti, L.M. Using Kinect for upper-limb functional evaluation in home rehabilitation: A comparison with a 3D stereoscopic passive marker system. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 561–566. [Google Scholar]
- Scano, A.; Caimmi, M.; Chiavenna, A.; Malosio, M.; Tosatti, L.M. Kinect One-based biomechanical assessment of upper-limb performance compared to clinical scales in post-stroke patients. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5720–5723. [Google Scholar]
- Hondori, H.M.; Khademi, M. A Review on Technical and Clinical Impact of Microsoft Kinect on Physical Therapy and Rehabilitation. J. Med. Eng. 2014, 2014, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Da Gama, A.; Fallavollita, P.; Teichrieb, V.; Navab, N. Motor Rehabilitation Using Kinect: A Systematic Review. Games Health J. 2015, 4, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Bonnechere, B.; Jansen, B.; Salvia, P.; Bouzahouene, H.; Omelina, L.; Moiseev, F.; Jan, S.V.S. Validity and reliability of the Kinect within functional assessment activities: Comparison with standard stereophotogrammetry. Gait Posture 2014, 39, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Kurillo, G.; Chen, A.; Bajcsy, R.; Han, J.J. Evaluation of upper extremity reachable workspace using Kinect camera. Technol. Heal. Care 2013, 21, 641–656. [Google Scholar]
- Lee, S.H.; Yoon, C.; Chung, S.G.; Kim, H.C.; Kwak, Y.; Park, H.W.; Kim, K. Measurement of shoulder range of motion in patients with adhesive capsulitis using a kinect. PLoS ONE 2015, 10, e0129398. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.E.; Seitz, A.L.; Leeser, M.; Sternad, D. Validity and reliability of Kinect skeleton for measuring shoulder joint angles: A feasibility study. Physiotherapy 2015, 101, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.; Gabriel, J.; Melo, C.; Machado, J. Kinect system in home-based cardiovascular rehabilitation. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 231, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Grugnetti, M.; Iarlori, S.; Longhi, S.; Verdini, F. An instrumental approach for monitoring physical exercises in a visual markerless scenario: A proof of concept. J. Biomech. 2018, 69, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Dolatabadi, E.; Taati, B.; Mihailidis, A. Concurrent validity of the Microsoft Kinect for Windows v2 for measuring spatiotemporal gait parameters. Med. Eng. Phys. 2016, 38, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Darby, J.; Sánchez, M.B.; Butler, P.B.; Loram, I.D. An evaluation of 3D head pose estimation using the Microsoft Kinect v2. Gait Posture 2016, 48, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Lee, H.J.; Lin, K.H. Measurement of body joint angles for physical therapy based on mean shift tracking using two low cost Kinect images. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 703–706. [Google Scholar]
- Scano, A.; Caimmi, M.; Chiavenna, A.; Malosio, M.; Tosatti, L.M. A Kinect-Based Biomechanical Assessment of Neurological Patients’ Motor Performances for Domestic Rehabilitation. In Virtual Reality Enhanced Robotic Systems for Disability Rehabilitation; IGI: Antwerp, Belgium, 2016; pp. 252–279. [Google Scholar]
- Otte, K.; Kayser, B.; Mansow-Model, S.; Verrel, J.; Paul, F.; Brandt, A.U.; Schmitz-Hübsch, T. Accuracy and reliability of the Kinect version 2 for clinical measurement of motor function. PLoS ONE 2016, 11, e0166532. [Google Scholar] [CrossRef] [PubMed]
- Giancola, S.; Corti, A.; Molteni, F.; Sala, R. Motion Capture: An Evaluation of Kinect V2 Body Tracking for Upper Limb Motion Analysis. In Proceedings of the MobiHealth 2016—Wireless Mobile Communication and Healthcare, Milan, Italy, 14–16 November 2016; Springer: Cham, Switzerland, 2017; Volume 192. [Google Scholar]
- Rocha, A.P.; Choupina, H.; Fernandes, J.M.; Rosas, M.J.; Vaz, R.; Cunha, J.P.S. Kinect v2 based system for Parkinson’s disease assessment. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 1279–1282. [Google Scholar]
- Eltoukhy, M.; Oh, J.; Kuenze, C.; Signorile, J. Gait & Posture Improved kinect-based spatiotemporal and kinematic treadmill gait assessment. Gait Posture 2017, 51, 77–83. [Google Scholar] [PubMed]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Iarlori, S.; Longhi, S.; Romeo, L.; Verdini, F. Accuracy evaluation of the Kinect v2 sensor during dynamic movements in a rehabilitation scenario. In Proceedings of the IEEE 38th Annual International Conference of the Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 5409–5412. [Google Scholar]
- Ozturk, A.; Tartar, A.; Huseyinsinoglu, B.E.; Ertas, A.H. A clinically feasible kinematic assessment method of upper extremity motor function impairment after stroke. Meas. J. Int. Meas. Confed. 2016, 80, 207–216. [Google Scholar] [CrossRef]
- Chen, X.; Siebourg-Polster, J.; Wolf, D.; Czech, C.; Bonati, U.; Fischer, D.; Strahm, M. Feasibility of Using Microsoft Kinect to Assess Upper Limb Movement in Type III Spinal Muscular Atrophy Patients. PLoS ONE 2017, 12, e0170472. [Google Scholar] [CrossRef] [PubMed]
- Kutlu, M.; Freeman, C.; Spraggs, M. Functional electrical stimulation for home-based upper-limb stroke rehabilitation. Curr. Dir. Biomed. Eng. 2017, 3, 25–29. [Google Scholar]
- Pagliari, D.; Pinto, L. Calibration of Kinect for Xbox One and comparison between the two generations of Microsoft sensors. Sensors 2015, 15, 27569–27589. [Google Scholar] [CrossRef] [PubMed]
- Bakhti, K.K.A.; Mottet, D.; Schweighofer, N.; Froger, J.; Laffont, I. Proximal arm non-use when reaching after a stroke. Neurosci. Lett. 2017, 657, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Bakhti, K.K.A.; Laffont, I.; Muthalib, M.; Froger, J.; Mottet, D. Validation of a kinect-based system to quantify proximal arm non-use after a stroke. Ann. Phys. Rehabil. Med. 2018, 61, e27. [Google Scholar] [CrossRef]
- Kim, W.S.; Cho, S.; Baek, D.; Bang, H.; Paik, N.J. Upper extremity functional evaluation by Fugl-Meyer assessment scoring using depth-sensing camera in hemiplegic stroke patients. PLoS ONE 2016, 11, e0158640. [Google Scholar] [CrossRef] [PubMed]
- Scano, A.; Chiavenna, A.; Malosio, M.; Tosatti, L.M.; Molteni, F. Kinect V2 implementation and testing of the reaching performance scale for motor evaluation of patients with neurological impairment. Med. Eng. Phys. 2018, 56, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Scano, A.; Chiavenna, A.; Malosio, M.; Molinari Tosatti, L. Kinect V2 performance assessment in daily-life gestures: Cohort study on healthy subjects for a reference database for automated instrumental evaluations on neurological patients. Appl. Bionics Biomech. 2017, 2017, 8567084. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.F.; Desrosiers, J.; Beauchemin, D.; Bergeron, N.; Rochette, A. Development and validation of a scale for rating motor compensations used for reaching in patients with hemiparesis: The reaching performance scale. Phys. Ther. 2004, 84, 8–22. [Google Scholar] [PubMed]
- Bagesteiro, L.B.; Sainburg, R.L. Handedness: Dominant arm advantages in control of limb dynamics. J. Neurophysiol. 2002, 88, 2408–2421. [Google Scholar] [CrossRef] [PubMed]
- Sainburg, R.L.; Schaefer, S.Y. Interlimb differences in control of movement extent. J. Neurophysiol. 2004, 92, 1374–1383. [Google Scholar] [CrossRef] [PubMed]
- Heuer, H. Control of the dominant and nondominant hand: Exploitation and taming of nonmuscular forces. Exp. Brain Res. 2007, 178, 363–373. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males | Females | Right Dominant | Left Dominant | Mean Age | Total |
| 46 | 31 | 72 | 6 | 41.77 ± 19.29 | 77 |
| Males | Females | Right Impairment | Left Impairment | Mean Age | Total |
| 11 | 9 | 12 | 8 | 52.21 ± 16.43 | 20 |
| Patient | Gender | Age Range | Impaired Limb |
|---|---|---|---|
| Pt1 | Male | 70–80 | Right |
| Pt2 | Female | 60–70 | Right |
| Pt3 | Male | 50–60 | Right |
| Pt4 | Male | 50–60 | Right |
| Pt5 | Female | 30–40 | Right |
| Pt6 | Male | 40–50 | Right |
| Pt7 | Female | 60–70 | Left |
| Pt8 | Female | 20–30 | Left |
| Pt9 | Male | 60–70 | Right |
| Pt10 | Male | 60–70 | Right |
| Pt11 | Female | 20–30 | Left |
| Pt12 | Female | 20–30 | Right |
| Pt13 | Male | 60–70 | Left |
| Pt14 | Male | 50–60 | Left |
| Pt15 | Male | 50–60 | Right |
| Pt16 | Male | 60–70 | Left |
| Pt17 | Male | 60–70 | Right |
| Pt18 | Female | 40–50 | Right |
| Pt19 | Female | 40–50 | Left |
| Pt20 | Female | 70–80 | Left |
| Patient ID | Trunk | Smoothness | Shoulder | Elbow | Prehension | Global | Total |
|---|---|---|---|---|---|---|---|
| Pt1 | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Pt2 | 3 | 2 | 2 | 3 | 3 | 3 | 16 |
| Pt3 | 1 | 1 | 1 | 0 | 1 | 0 | 4 |
| Pt4 | 3 | 1 | 3 | 1 | 2 | 2 | 12 |
| Pt5 | 3 | 3 | 2 | 3 | 3 | 3 | 17 |
| Pt6 | 2 | 2 | 3 | 3 | 0 | 1 | 11 |
| Pt7 | 3 | 0 | 3 | 3 | 1 | 2 | 12 |
| Pt8 | 3 | 3 | 3 | 1 | 0 | 1 | 11 |
| Pt9 | 3 | 3 | 2 | 3 | 3 | 3 | 17 |
| Pt10 | 2 | 1 | 1 | 2 | 0 | 1 | 7 |
| Pt11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pt12 | 2 | 2 | 2 | 2 | 0 | 1 | 9 |
| Pt13 | 3 | 2 | 1 | 1 | 2 | 1 | 10 |
| Pt14 | 3 | 2 | 2 | 2 | 2 | 2 | 13 |
| Pt15 | 3 | 0 | 0 | 1 | 0 | 0 | 4 |
| Pt16 | 3 | 0 | 0 | 0 | 0 | 0 | 3 |
| Pt17 | 3 | 2 | 2 | 2 | 3 | 2 | 14 |
| Pt18 | 2 | 3 | 2 | 3 | 3 | 2 | 15 |
| Pt19 | 2 | 2 | 1 | 2 | 0 | 1 | 8 |
| Pt20 | 3 | 3 | 3 | 3 | 3 | 3 | 18 |
| Measure | Healthy Dominant (°) | Healthy Non-Dominant (°) | Patients Impaired (°) | Patient Less Impaired (°) | Have Groups Different Mean? |
|---|---|---|---|---|---|
| SE | 101.9(8.0) | 105.6(6.6) | 88.8(26.3) | 103.8(14.7) | p < 10−6 |
| SA | 79.9(6.3) | 81.2(6.0) | 90.2(22.2) | 80.2(12.1) | p = 0.0004 |
| EE | 15.3(7.1) | 16.1(6.1) | 38.7(32.5) | 15.9(10.4) | p < 10−10 |
| ScE | 0.0139(0.062) | 0.0184(0.093) | 0.0280(0.0124) | 0.017(0.08) | p < 10−10 |
| TC | 0.0146(0.0302) | 0.0157(0.073) | 0.0736(0.0981) | 0.0418(0.0628) | p < 10−8 |
| VP | 1.1743(0.2624) | 1.1037(0.2401) | 1.7618(0.0339) | 1.3189(0.3197) | p < 10−8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scano, A.; Molteni, F.; Molinari Tosatti, L. Low-Cost Tracking Systems Allow Fine Biomechanical Evaluation of Upper-Limb Daily-Life Gestures in Healthy People and Post-Stroke Patients. Sensors 2019, 19, 1224. https://doi.org/10.3390/s19051224
Scano A, Molteni F, Molinari Tosatti L. Low-Cost Tracking Systems Allow Fine Biomechanical Evaluation of Upper-Limb Daily-Life Gestures in Healthy People and Post-Stroke Patients. Sensors. 2019; 19(5):1224. https://doi.org/10.3390/s19051224
Chicago/Turabian StyleScano, Alessandro, Franco Molteni, and Lorenzo Molinari Tosatti. 2019. "Low-Cost Tracking Systems Allow Fine Biomechanical Evaluation of Upper-Limb Daily-Life Gestures in Healthy People and Post-Stroke Patients" Sensors 19, no. 5: 1224. https://doi.org/10.3390/s19051224