Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Data Acquisition
2.2. Statistical Analysis
3. Results
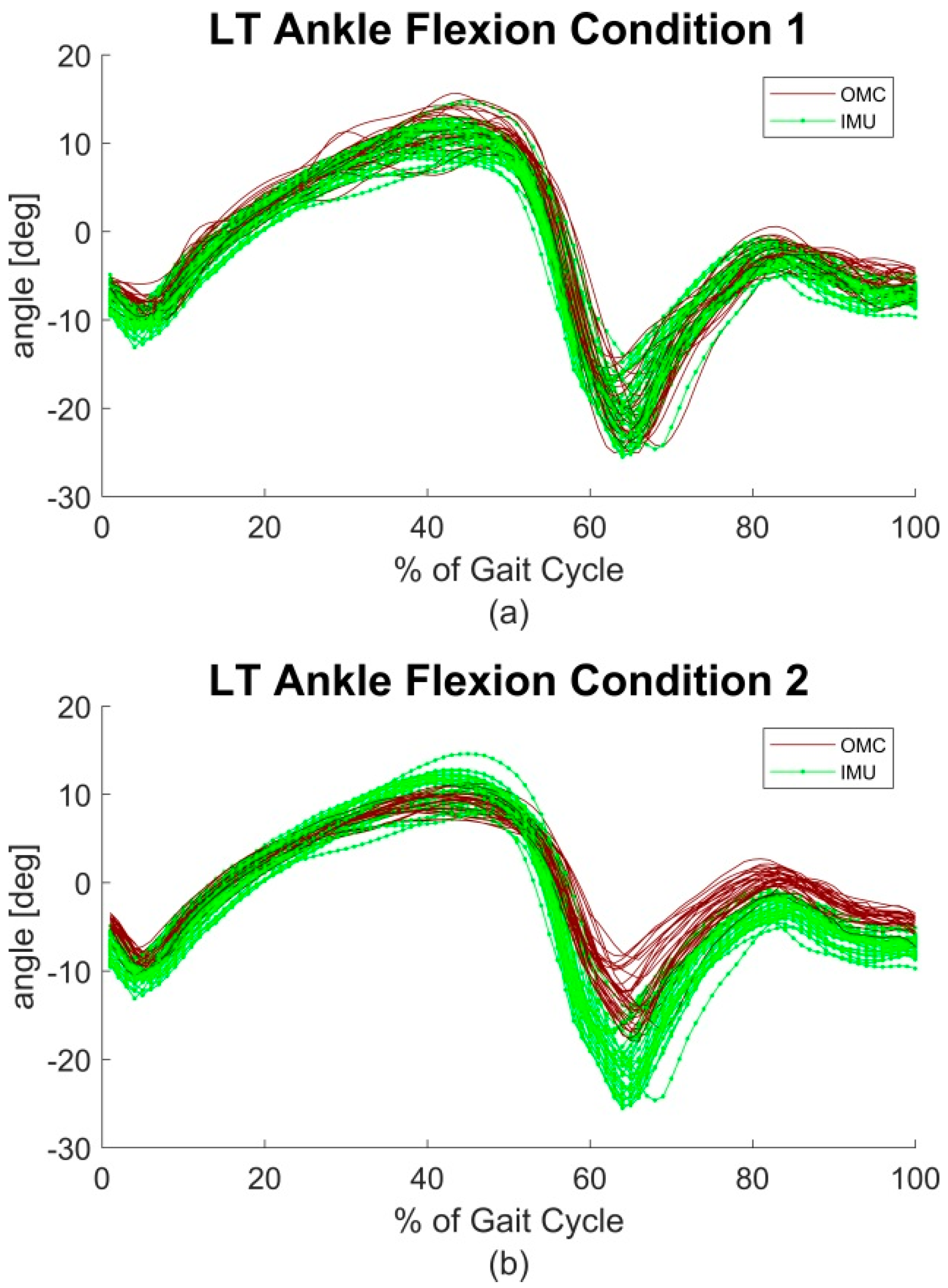
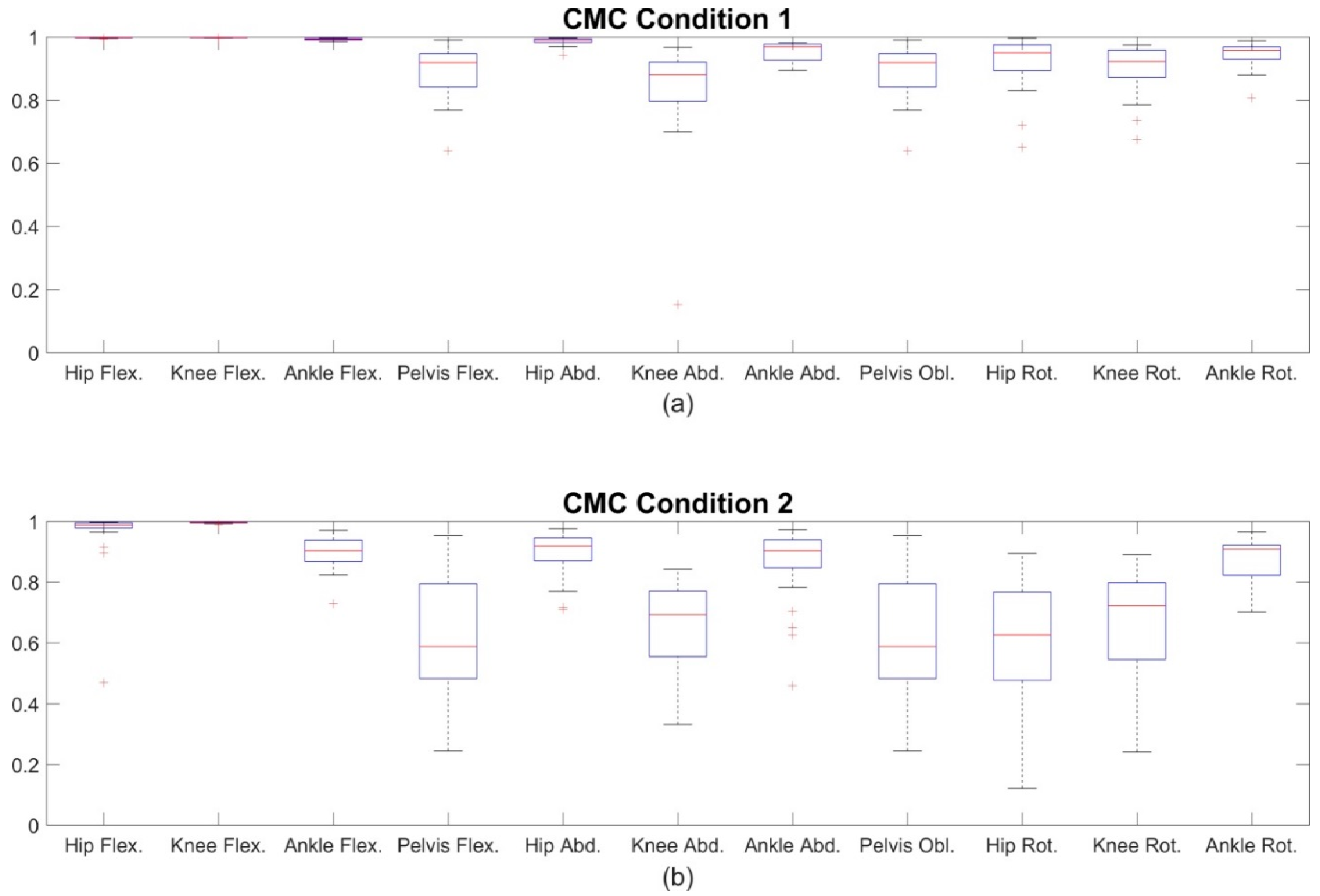
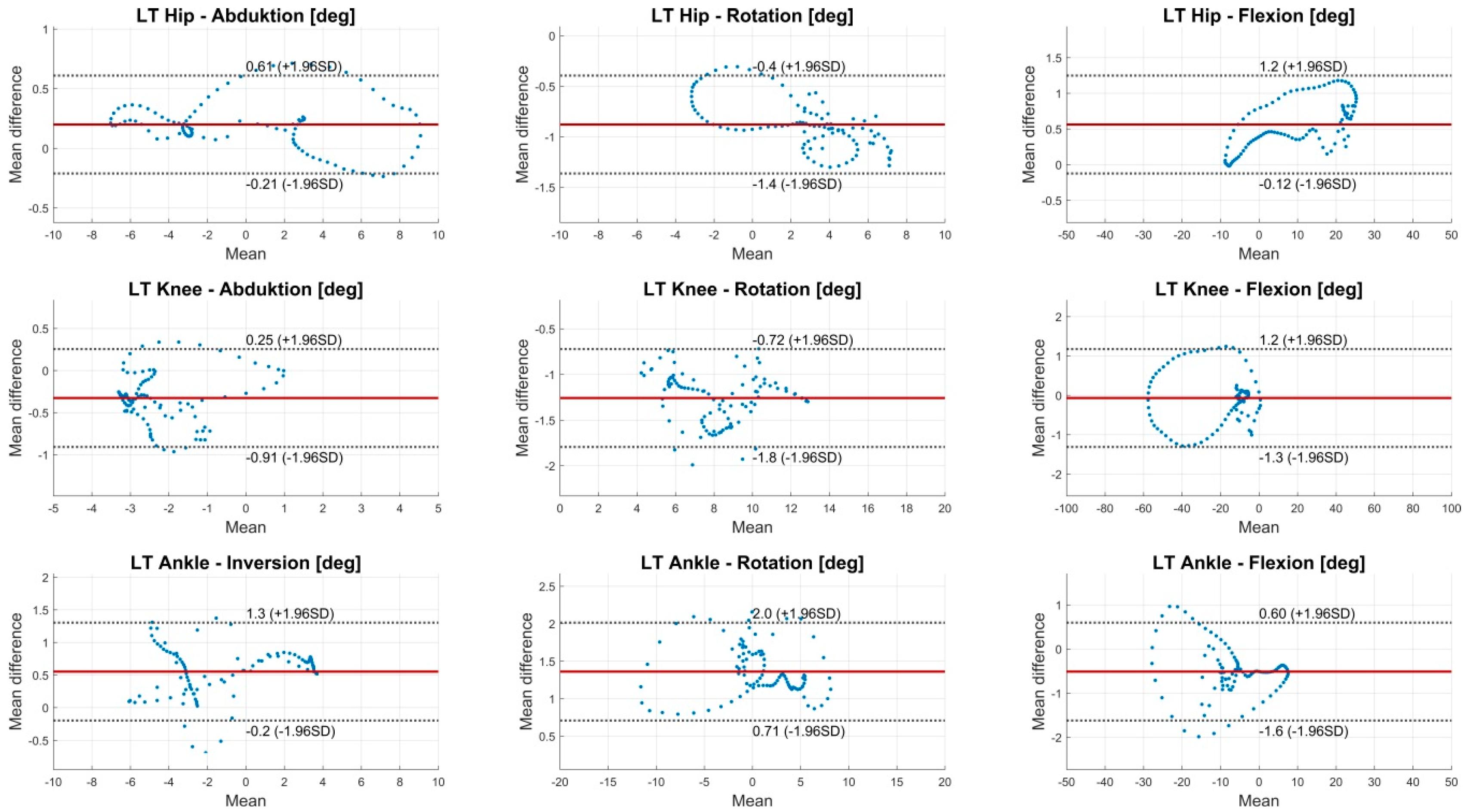
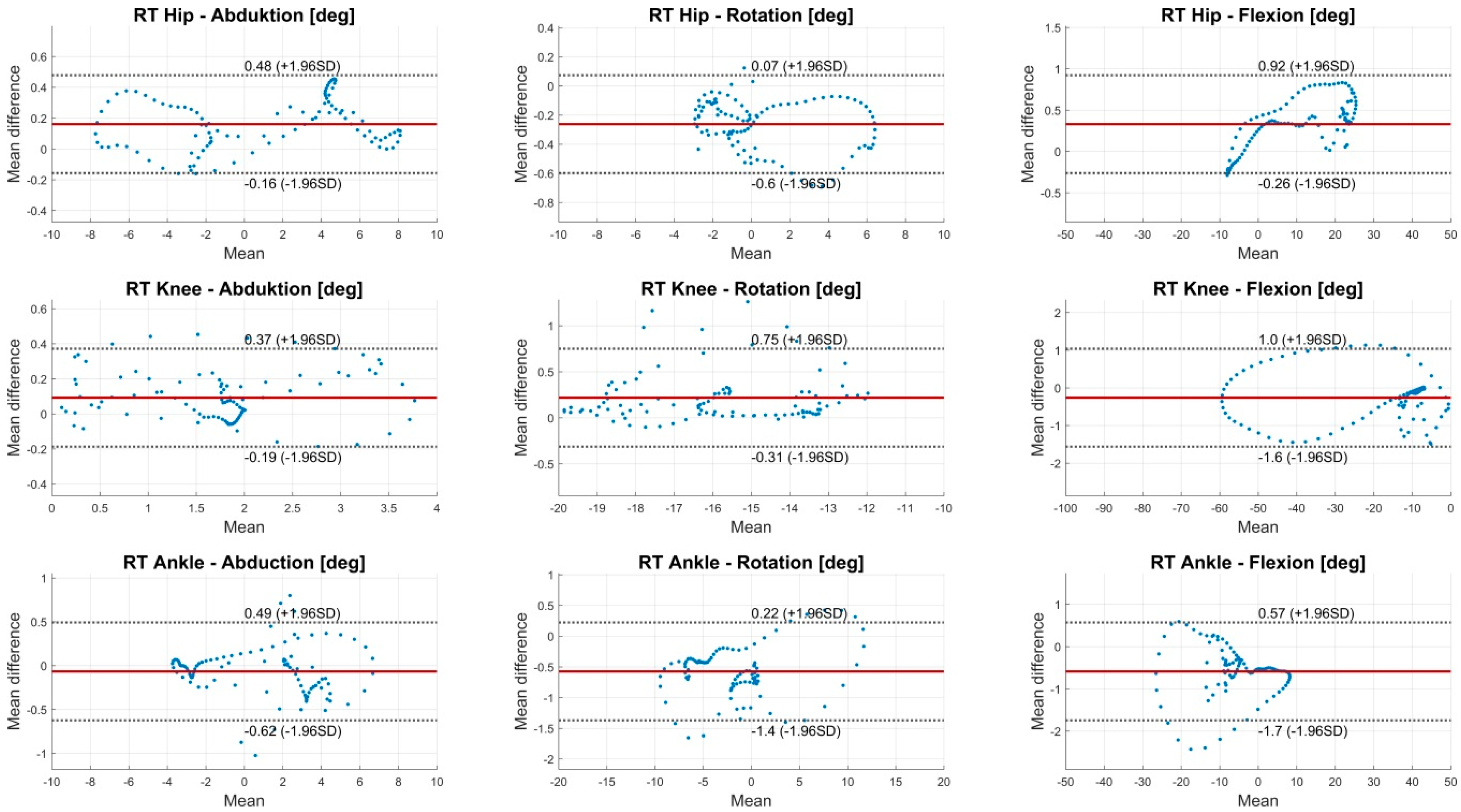
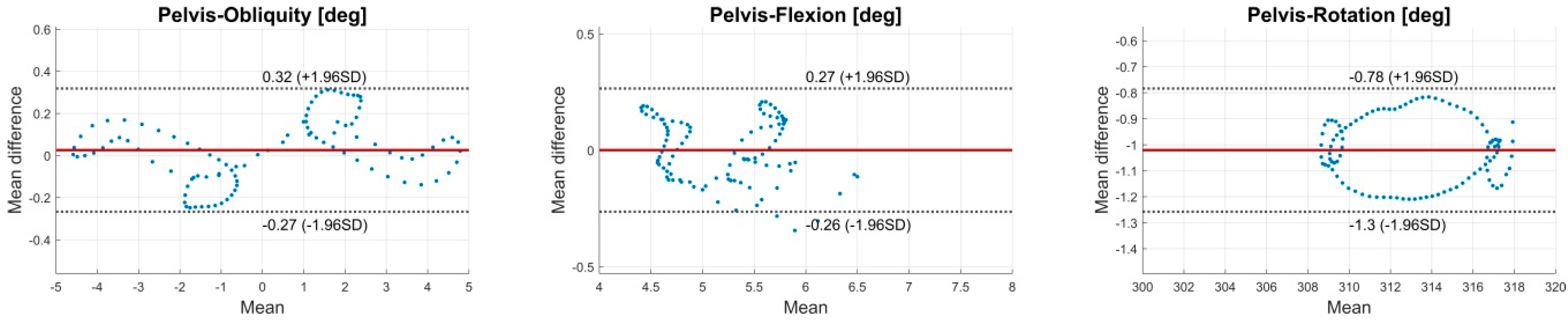
3.1. Condition 1—Marker Clusters
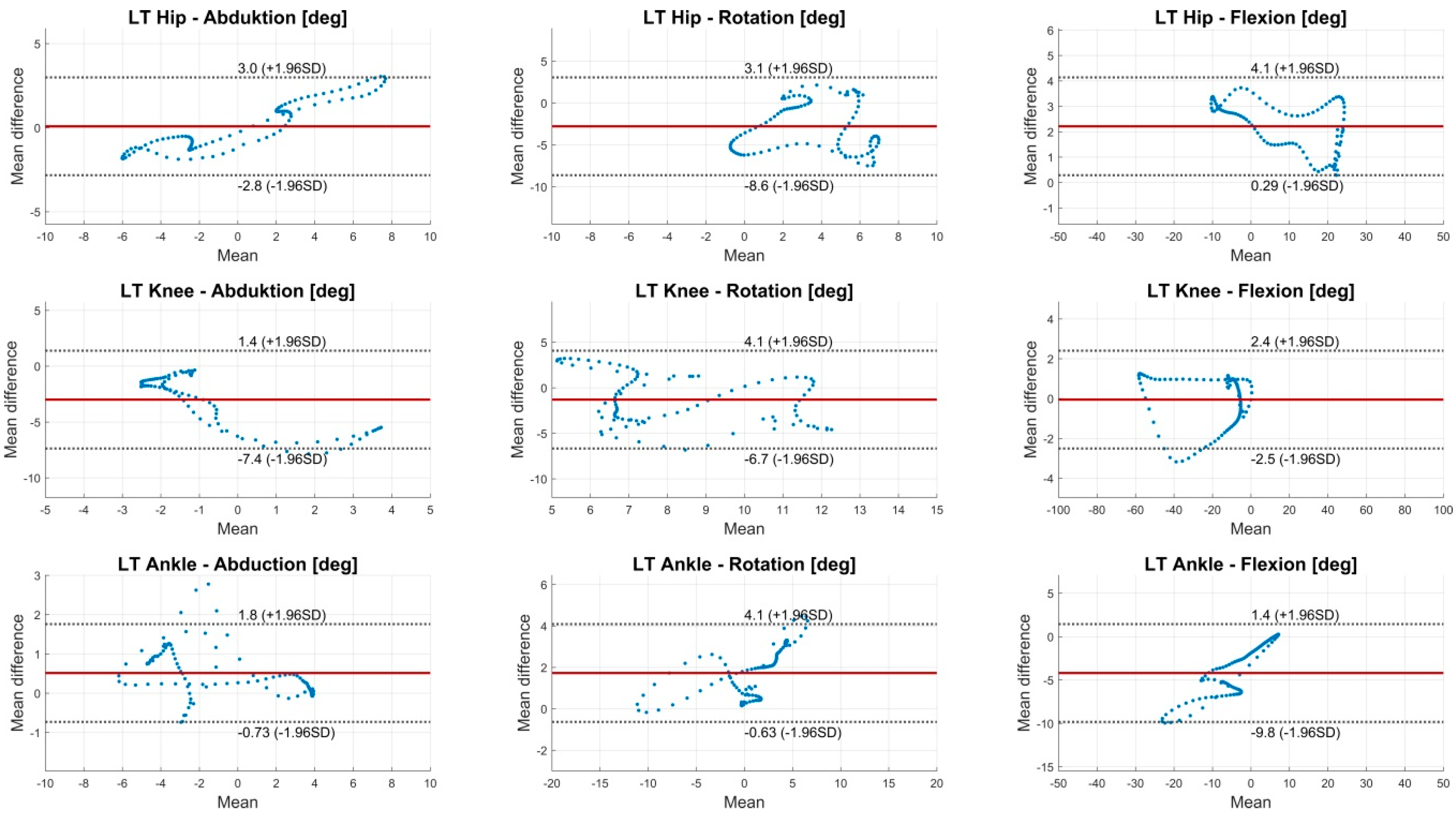
3.2. Condition 2—Skin Markers
3.3. Test-Retest Reliability
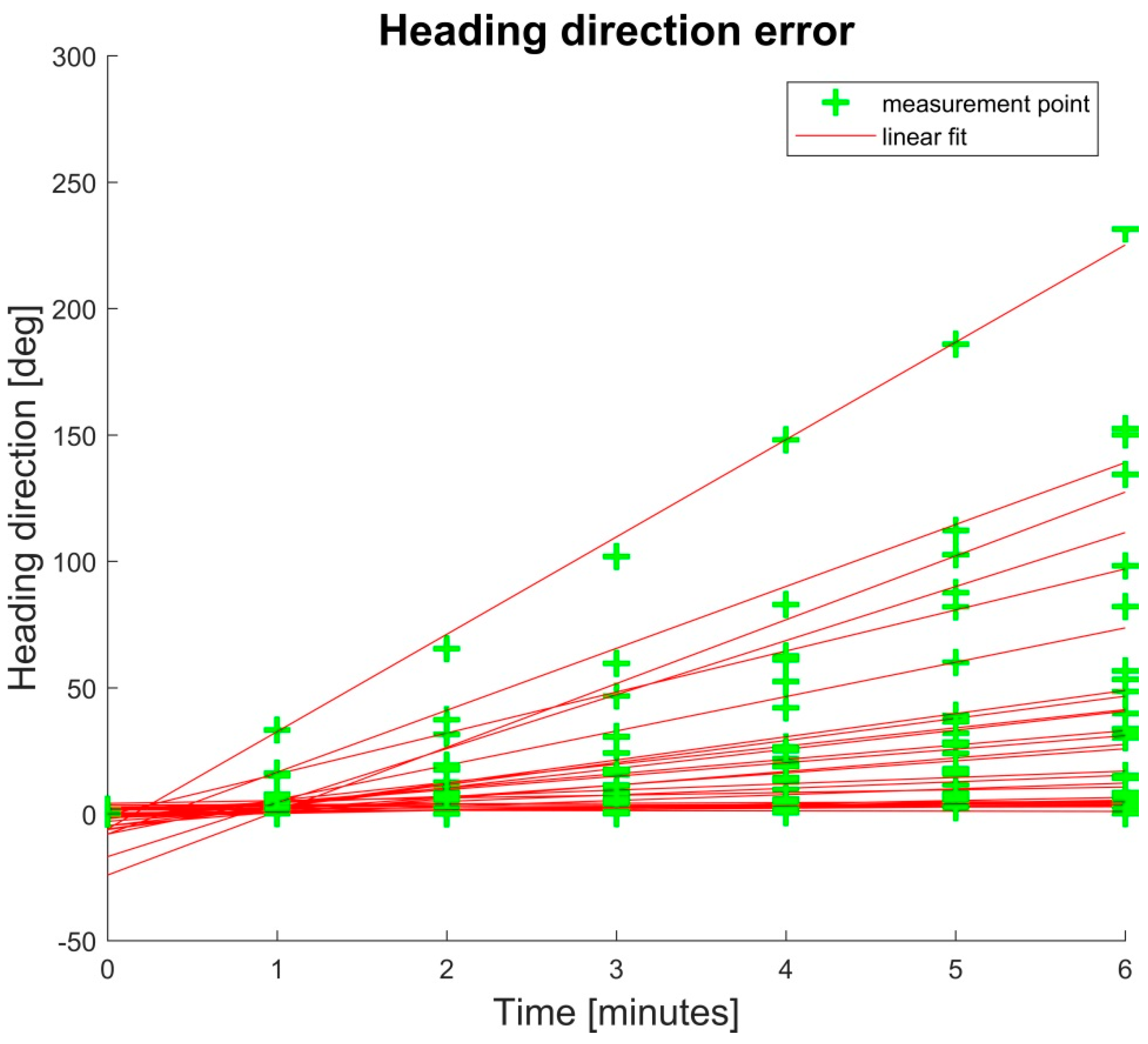
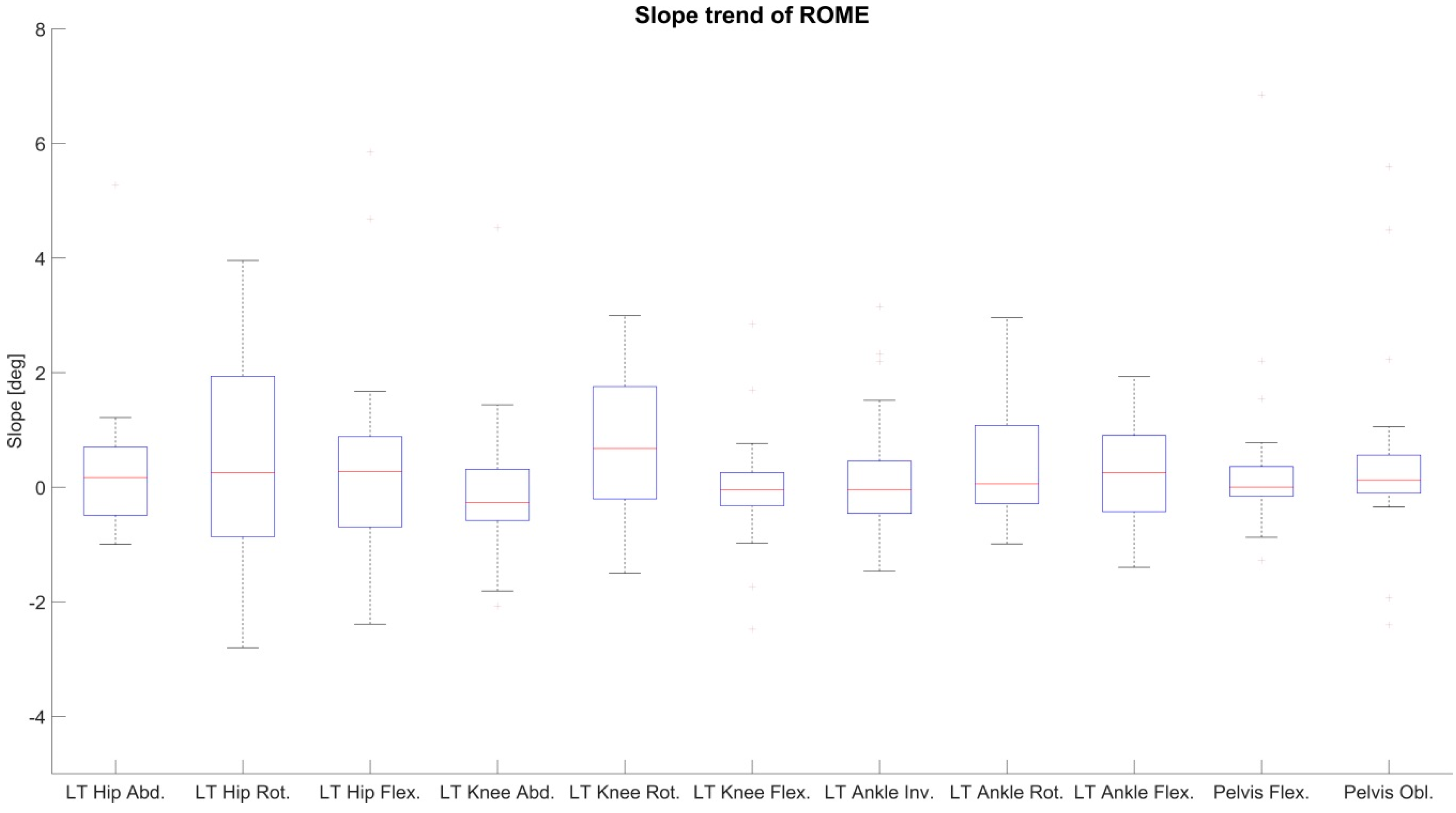
3.4. Drift
4. Discussion
4.1. Condition 1—Marker Clusters
4.2. Condition 2—Skin Markers
4.3. Test-Retest Reliability
4.4. Drift
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Appendix A.1. Biomechanical Model

Appendix A.2. Segment Kinematics Estimation Method

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Value | 10−5 | 0.7 |
Appendix B






References
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Miezal, M.; Taetz, B.; Bleser, G. On Inertial Body Tracking in the Presence of Model Calibration Errors. Sensors 2016, 16, 1132. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, A.M. Kalman-Filter-Based Orientation Determination Using Inertial/Magnetic Sensors: Observability Analysis and Performance Evaluation. Sensors 2011, 11, 9182–9206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippeschi, A.; Schmitz, N.; Miezal, M.; Bleser, G.; Ruffaldi, E.; Stricker, D. Survey of Motion Tracking Methods Based on Inertial Sensors: A Focus on Upper Limb Human Motion. Sensors 2017, 17, 1257. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Hou, B.; Lin, Z.; Guo, M. Modeling and Compensation of Random Drift of MEMS Gyroscopes Based on Least Squares Support Vector Machine Optimized by Chaotic Particle Swarm Optimization. Sensors 2017, 17, 2335. [Google Scholar] [CrossRef] [PubMed]
- De Vries, W.H.K.; Veeger, H.E.J.; Baten, C.T.M.; van der Helm, F.C.T. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Ligorio, G.; Sabatini, A. Dealing with Magnetic Disturbances in Human Motion Capture: A Survey of Techniques. Micromachines 2016, 7, 43. [Google Scholar] [CrossRef]
- Harada, T.; Mori, T.; Sato, T. Development of a Tiny Orientation Estimation Device to Operate under Motion and Magnetic Disturbance. Int. J. Robot. Res. 2007, 26, 547–559. [Google Scholar] [CrossRef]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; de Guise, J.A.; Aminian, K. Functional calibration procedure for 3D knee joint angle description using inertial sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- El-Gohary, M.; McNames, J. Human Joint Angle Estimation with Inertial Sensors and Validation with A Robot Arm. IEEE Trans. Biomed. Eng. 2015, 62, 1759–1767. [Google Scholar] [CrossRef] [PubMed]
- Fasel, B.; Spörri, J.; Schütz, P.; Lorenzetti, S.; Aminian, K. Validation of functional calibration and strap-down joint drift correction for computing 3D joint angles of knee, hip, and trunk in alpine skiing. PLoS ONE 2017, 12, e0181446. [Google Scholar] [CrossRef] [PubMed]
- Fasel, B.; Sporri, J.; Chardonnens, J.; Kroll, J.; Muller, E.; Aminian, K. Joint Inertial Sensor Orientation Drift Reduction for Highly Dynamic Movements. IEEE J. Biomed. Health Inform. 2017. [Google Scholar] [CrossRef] [PubMed]
- Miezal, M.; Taetz, B.; Bleser, G. Real-time inertial lower body kinematics and ground contact estimation at anatomical foot points for agile human locomotion. In Proceedings of the 2017 IEEE International Conference on Robotics and Automation (ICRA), Singapore, 29 May–3 June 2017; pp. 3256–3263. [Google Scholar]
- Kluge, F.; Gaßner, H.; Hannink, J.; Pasluosta, C.; Klucken, J.; Eskofier, B.M. Towards Mobile Gait Analysis: Concurrent Validity and Test-Retest Reliability of an Inertial Measurement System for the Assessment of Spatio-Temporal Gait Parameters. Sensors 2017, 17, 1522. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Buckley, C.J.; Mazzà, C. Gait event detection in laboratory and real life settings: Accuracy of ankle and waist sensor based methods. Gait Posture 2016, 50, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-T.; Novak, A.C. Concurrent validation of Xsens and MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Cutti, A.G.; Garofalo, P.; Raggi, M.; Heijboer, M.; Cappello, A.; Davalli, A. First in vivo assessment of “Outwalk”: A novel protocol for clinical gait analysis based on inertial and magnetic sensors. Med. Biol. Eng. Comput. 2010, 48, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors 2014, 14, 18625–18649. [Google Scholar] [CrossRef] [PubMed]
- Kainz, H.; Modenese, L.; Lloyd, D.G.; Maine, S.; Walsh, H.P.J.; Carty, C.P. Joint kinematic calculation based on clinical direct kinematic versus inverse kinematic gait models. J. Biomech. 2016, 49, 1658–1669. [Google Scholar] [CrossRef] [PubMed]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring joint kinematics of treadmill walking and running: Comparison between an inertial sensor based system and a camera-based system. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vreede, K.; Henriksson, J.; Borg, K.; Henriksson, M. Gait characteristics and influence of fatigue during the 6-min walk test in patients with post-polio syndrome. J. Rehabil. Med. 2013, 45, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Sawacha, Z.; Paolini, G.; Ingrosso, S.; Nativo, R.; Benedetti, M.G. A new anatomically based protocol for gait analysis in children. Gait Posture 2007, 26, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Cappozzo, A.; Catani, F.; Croce, U.D.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Bleser, G.; Stricker, D. Advanced tracking through efficient image processing and visual-inertial sensor fusion. In Proceedings of the 2008 IEEE Virtual Reality Conference, Reno, NE, USA, 8–12 March 2008; pp. 137–144. [Google Scholar]
- Eie, M.; Wei, C.-S. Generalizations of Euler decomposition and their applications. J. Number Theory 2013, 133, 2475–2495. [Google Scholar] [CrossRef]
- Banks, J.J.; Chang, W.-R.; Xu, X.; Chang, C.-C. Using horizontal heel displacement to identify heel strike instants in normal gait. Gait Posture 2015, 42, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Cutti, A.G.; Cappello, A. A new formulation of the coefficient of multiple correlation to assess the similarity of waveforms measured synchronously by different motion analysis protocols. Gait Posture 2010, 31, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Mcgraw, K.; Wong, S.P. Forming Inferences about Some Intraclass Correlation Coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Røislien, J.; Skare, Ø.; Opheim, A.; Rennie, L. Evaluating the properties of the coefficient of multiple correlation (CMC) for kinematic gait data. J. Biomech. 2012, 45, 2014–2018. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, N.M.; Atkins, P.R.; Kutschke, M.J.; Goebel, J.M.; Foreman, K.B.; Anderson, A.E. Soft tissue artifact causes significant errors in the calculation of joint angles and range of motion at the hip. Gait Posture 2017, 55, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Mills, P.M.; Morrison, S.; Lloyd, D.G.; Barrett, R.S. Repeatability of 3D gait kinematics obtained from an electromagnetic tracking system during treadmill locomotion. J. Biomech. 2007, 40, 1504–1511. [Google Scholar] [CrossRef] [PubMed]
- Kailath, T.; Sayed, A.H.; Hassibi, B. Linear Estimation; Prentice Hall: Upper Saddle River, NJ, USA, 2000; ISBN 978-0-13-022464-4. [Google Scholar]
- Thrun, S.; Burgard, W.; Fox, D. Probabilistic Robotics (Intelligent Robotics and Autonomous Agents); The MIT Press: Cambridge, MA, USA, 2005; ISBN 978-0-262-20162-9. [Google Scholar]







| RMSE (deg) ± SD (95% CI) | ROME (deg) ± SD (95% CI) | |||||
|---|---|---|---|---|---|---|
| A | B | C | A | B | C | |
| LT Hip—Abduction | 1.05 ± 0.42 (0.78–1.11) | 1.14 ± 0.55 (0.75–1.17) | 1.06 ± 0.45 (0.77–1.12) | 0.54 ± 0.21 (0.43–0.59) | 0.57 ± 0.29 (0.38–0.60) | 0.57 ± 0.27 (0.44–0.64) |
| LT Hip—Rotation | 1.94 ± 0.92 (1.49–2.20) | 2.29 ± 1.36 (1.85–2.91) | 2.25 ± 1.16 (1.80–2.70) | 0.68 ± 0.27 (0.53–0.74) | 0.70 ± 0.28 (0.55–0.77) | 0.68 ± 0.28 (0.56–0.75) |
| LT Hip—Flexion | 1.02 ± 0.35 (0.79–1.06) | 0.99 ± 0.29 (0.83–1.06) | 1.00 ± 0.32 (0.78–1.02) | 0.93 ± 0.36 (0.71–1.00) | 0.89 ± 0.36 (0.72–0.99) | 0.85 ± 0.37 (0.70–0.99) |
| LT Knee—Abduction | 1.59 ± 0.48 (1.22–1.59) | 1.58 ± 0.50 (1.26–1.65) | 1.57 ± 0.51 (1.31–1.71) | 1.58 ± 0.79 (1.20–1.81) | 1.54 ± 0.92 (0.97–1.68) | 1.54 ± 0.83 (1.09–1.73) |
| LT Knee—Rotation | 2.34 ± 1.08 (1.63–2.48) | 2.34 ± 1.16 (1.43–2.33) | 2.27 ± 1.10 (1.37–2.23) | 1.09 ± 0.32 (0.92–1.16) | 1.09 ± 0.39 (0.93–1.23) | 1.16 ± 0.41 (0.98–1.30) |
| LT Knee—Flexion | 1.47 ± 0.34 (1.25–1.51) | 1.44 ± 0.31 (1.29–1.53) | 1.41 ± 0.34 (1.17–1.44) | 0.70 ± 0.27 (0.57–0.78) | 0.67 ± 0.27 (0.51–0.72) | 0.72 ± 0.33 (0.60–0.86) |
| LT Ankle—Abduction | 1.61 ± 0.39 (1.42–1.73) | 1.63 ± 0.36 (1.50–1.78) | 1.62 ± 0.43 (1.35–1.68) | 1.29 ± 0.51 (0.96–1.35) | 1.43 ± 0.43 (1.29–1.62) | 1.22 ± 0.39 (0.97–1.27) |
| LT Ankle—Rotation | 2.16 ± 0.68 (1.80–2.33) | 2.12 ± 0.65 (1.70–2.21) | 2.13 ± 0.68 (1.69–2.19) | 1.56 ± 0.57 (1.18–1.63) | 1.51 ± 0.61 (1.13–1.59) | 1.53 ± 0.45 (1.35–1.69) |
| LT Ankle—Flexion | 1.55 ± 0.34 (1.46–1.72) | 1.54 ± 0.36 (1.41–1.69) | 1.61 ± 0.47 (1.35–1.72) | 0.97 ± 0.38 (0.73–1.03) | 0.98 ± 0.38 (0.73–1.02) | 1.08 ± 0.44 (0.85–1.19) |
| RT Hip—Abduction | 1.09 ± 0.54 (0.63–1.05) | 1.09 ± 0.55 (0.68–1.11) | 1.12 ± 0.54 (0.69–1.11) | 0.56 ± 0.22 (0.42–0.59) | 0.55 ± 0.26 (0.32–0.52) | 0.53 ± 0.25 (0.38–0.57) |
| RT Hip—Rotation | 1.64 ± 1.00 (1.00–1.77) | 1.78 ± 1.76 (0.68–2.04) | 2.07 ± 1.72 (0.92–2.25) | 0.65 ± 0.47 (0.40–0.76) | 0.56 ± 0.19 (0.46–0.60) | 0.51 ± 0.20 (0.42–0.57) |
| RT Hip—Flexion | 0.98 ± 0.51 (0.68–1.07) | 0.89 ± 0.30 (0.68–0.91) | 0.86 ± 0.28 (0.69–0.91) | 0.98 ± 1.26 (0.21–1.18) | 0.73 ± 0.40 (0.52–0.83) | 0.69 ± 0.43 (0.44–0.77) |
| RT Knee—Abduction | 1.26 ± 0.51 (0.90–1.30) | 1.26 ± 0.44 (1.08–1.43) | 1.24 ± 0.48 (0.90–1.27) | 1.11 ± 0.54 (0.79–1.21) | 1.12 ± 0.59 (0.77–1.23) | 1.19 ± 0.70 (0.69–1.23) |
| RT Knee—Rotation | 1.75 ± 0.63 (1.38–1.87) | 1.91 ± 0.72 (1.38–1.93) | 1.93 ± 0.84 (1.49–2.14) | 1.03 ± 0.57 (0.65–1.09) | 0.90 ± 0.42 (0.67–1.00) | 1.00 ± 0.45 (0.69–1.04) |
| RT Knee—Flexion | 1.51 ± 0.43 (1.31–1.64) | 1.40 ± 0.28 (1.28–1.50) | 1.37 ± 0.27 (1.26–1.47) | 0.76 ± 0.41 (0.43–0.75) | 0.75 ± 0.30 (0.56–0.79) | 0.71 ± 0.31 (0.47–0.71) |
| RT Ankle—Abduktion | 1.33 ± 0.35 (1.09–1.36) | 1.27 ± 0.33 (1.07–1.33) | 1.30 ± 0.29 (1.13–1.35) | 1.02 ± 0.48 (0.70–1.07) | 1.08 ± 0.49 (0.79–1.06) | 0.97 ± 0.35 (0.79–1.06) |
| RT Ankle—Rotation | 1.52 ± 0.41 (1.27–1.59) | 1.56 ± 0.46 (1.26–1.62) | 1.63 ± 0.51 (1.29–1.68) | 1.27 ± 0.57 (0.90–1.34) | 1.18 ± 0.48 (0.89–1.27) | 1.18 ± 0.48 (0.92–1.29) |
| RT Ankle—Flexion | 1.60 ± 0.36 (1.43–1.71) | 1.60 ± 0.38 (1.44–1.74) | 1.60 ± 0.42 (1.32–1.65) | 1.02 ± 0.37 (0.78–1.07) | 0.97 ± 0.38 (0.78–1.07) | 0.91 ± 0.38 (0.68–0.97) |
| Pelvis—Flexion | 0.64 ± 0.18 (0.55–0.69) | 0.62 ± 0.21 (0.52–0.68) | 0.62 ± 0.21 (0.51–0.67) | 0.32 ± 0.15 (0.22–0.34) | 0.35 ± 0.20 (0.25–0.40) | 0.33 ± 0.20 (0.25–0.41) |
| Pelvis—Obliquity | 0.62 ± 0.16 (0.57–0.69) | 0.61 ± 0.20 (0.51–0.67) | 0.59 ± 0.18 (0.47–0.61) | 0.31 ± 0.11 (0.23–0.32) | 0.32 ± 0.12 (0.24–0.33) | 0.33 ± 0.10 (0.28–0.36) |
| Pelvis—Rotation | x | x | x | 0.42 ± 0.15 (0.32–0.43) | 0.47 ± 0.22 (0.35–0.52) | 0.51 ± 0.29 (0.29–0.51) |
| RMSE (deg) ± SD (95% CI) | ROME (deg) ± SD (95% CI) | |||||
|---|---|---|---|---|---|---|
| A | B | C | A | B | C | |
| LT Hip—Abduction | 2.57 ± 0.88 (2.14–2.83) | 2.69 ± 1.05 (2.11–2.92) | 2.69 ± 1.03 (2.05–2.85) | 4.91 ± 2.14 (3.74–5.40) | 4.85 ± 2.24 (3.84–5.57) | 4.94 ± 2.14 (3.93–5.58) |
| LT Hip—Rotation | 5.37 ± 1.66 (4.36–5.64) | 5.60 ± 2.16 (4.52–6.20) | 5.54 ± 2.10 (4.37–6.00) | 3.98 ± 2.63 (2.48–4.52) | 4.17 ± 2.61 (3.27–5.29) | 4.24 ± 2.82 (3.12–5.31) |
| LT Hip—Flexion | 3.53 ± 3.37 (1.25–3.87) | 3.64 ± 3.47 (1.39–4.08) | 3.67 ± 3.53 (1.26–4.00) | 1.67 ± 1.22 (0.88–1.82) | 1.42 ± 0.94 (0.76–1.50) | 1.42 ± 0.96 (0.71–1.45) |
| LT Knee—Abduction | 4.19 ± 1.15 (3.63–4.53) | 4.14 ± 1.22 (3.53–4.48) | 4.13 ± 1.20 (3.45–4.38) | 2.89 ± 1.74 (1.83–3.18) | 2.76 ± 1.93 (1.68–3.18) | 2.85 ± 1.98 (1.83–3.37) |
| LT Knee—Rotation | 4.56 ± 1.33 (3.80–4.83) | 4.70 ± 1.40 (4.02–5.11) | 4.72 ± 1.44 (4.02–5.13) | 3.53 ± 2.08 (2.11–3.72) | 3.78 ± 2.05 (2.43–4.02) | 3.69 ± 2.33 (2.00–3.81) |
| LT Knee—Flexion | 2.38 ± 0.63 (2.16–2.64) | 2.38 ± 0.61 (2.03–2.50) | 2.40 ± 0.64 (2.05–2.55) | 1.48 ± 1.07 (0.78–1.62) | 1.58 ± 1.15 (0.87–1.76) | 1.59 ± 1.14 (0.95–1.84) |
| LT Ankle—Abduction | 2.92 ± 1.31 (1.93–2.95) | 3.01 ± 1.41 (1.97–3.06) | 3.00 ± 1.37 (1.91–2.97) | 2.49 ± 1.40 (1.80–2.88) | 2.52 ± 1.61 (1.32–2.57) | 2.53 ± 1.47 (1.54–2.68) |
| LT Ankle—Rotation | 3.28 ± 1.32 (2.38–3.41) | 3.41 ± 1.37 (2.84–3.91) | 3.45 ± 1.32 (2.85–3.87) | 4.74 ± 2.25 (3.90–5.65) | 5.02 ± 2.52 (3.75–5.70) | 4.94 ± 2.56 (3.59–5.57) |
| LT Ankle—Flexion | 5.30 ± 1.56 (4.52–5.73) | 5.42 ± 1.61 (4.55–5.79) | 5.48 ± 1.65 (4.60–5.88) | 10.07 ± 2.18 (8.94–10.63) | 10.63 ± 2.50 (9.51–11.44) | 10.66 ± 2.65 (9.62–11.68) |
| RT Hip—Abduction | 2.58 ± 0.64 (2.35–2.85) | 2.62 ± 0.63 (2.34–2.83) | 2.63 ± 0.65 (2.47–2.98) | 4.80 ± 1.44 (4.41–5.53) | 4.71 ± 1.48 (4.15–5.30) | 4.68 ± 1.53 (4.05–5.24) |
| RT Hip—Rotation | 5.01 ± 1.37 (4.44–5.51) | 4.97 ± 1.26 (4.20–5.18) | 5.01 ± 1.07 (4.60–5.43) | 3.01 ± 1.83 (1.77–3.19) | 2.93 ± 1.54 (1.98–3.17) | 3.12 ± 1.50 (2.15–3.31) |
| RT Hip—Flexion | 3.57 ± 3.23 (1.27–3.77) | 3.76 ± 3.34 (1.54–4.13) | 3.83 ± 3.33 (1.61–4.19) | 1.48 ± 0.62 (1.00–1.49) | 1.52 ± 0.77 (1.00–1.59) | 1.53 ± 0.86 (1.10–1.76) |
| RT Knee—Abduction | 3.83 ± 1.72 (2.52–3.85) | 3.79 ± 1.69 (2.53–3.84) | 3.72 ± 1.68 (2.45–3.75) | 3.16 ± 1.66 (2.07–3.35) | 3.21 ± 1.77 (2.27–3.65) | 3.21 ± 1.86 (2.22–3.66) |
| RT Knee—Rotation | 4.41 ± 1.01 (3.76–4.54) | 4.48 ± 1.06 (3.71–4.53) | 4.54 ± 1.22 (3.71–4.66) | 4.14 ± 2.13 (3.05–4.69) | 4.09 ± 1.85 (3.02–4.46) | 4.12 ± 2.10 (3.37–5.00) |
| RT Knee—Flexion | 2.59 ± 0.90 (2.00–2.70) | 2.66 ± 0.90 (2.00–2.70) | 2.65 ± 1.01 (1.99–2.77) | 1.76 ± 1.05 (0.97–1.78) | 1.67 ± 1.07 (1.05–1.89) | 1.58 ± 1.10 (0.86–1.71) |
| RT Ankle—Abduktion | 2.90 ± 1.62 (1.90–3.16) | 2.97 ± 1.88 (1.59–3.05) | 2.99 ± 1.97 (1.52–3.05) | 2.10 ± 1.03 (1.46–2.26) | 2.25 ± 1.10 (1.60–2.45) | 2.05 ± 1.34 (1.10–2.15) |
| RT Ankle—Rotation | 3.46 ± 1.10 (2.76–3.61) | 3.58 ± 1.22 (2.68–3.63) | 3.74 ± 1.30 (2.83–3.84) | 5.78 ± 1.88 (4.96–6.42) | 6.01 ± 2.13 (5.26–6.91) | 6.03 ± 2.09 (5.36–6.98) |
| RT Ankle—Flexion | 4.49 ± 1.27 (4.03–5.02) | 4.50 ± 1.19 (4.09–5.01) | 4.45 ± 1.30 (4.16–5.17) | 9.08 ± 2.95 (8.15–10.43) | 9.52 ± 2.71 (8.34–10.44) | 9.49 ± 2.63 (8.27–10.31) |
| Pelvis—Flexion | 1.69 ± 0.76 (1.17–1.76) | 1.77 ± 0.79 (1.26–1.87) | 1.81 ± 0.82 (1.28–1.91) | 1.91 ± 1.11 (1.49–2.35) | 1.98 ± 1.29 (1.47–2.47) | 2.07 ± 1.34 (1.33–2.37) |
| Pelvis—Obliquity | 2.52 ± 2.83 (0.68–2.88) | 2.60 ± 3.02 (0.49–2.83) | 2.57 ± 3.00 (0.51–2.83) | 1.02 ± 0.60 (0.56–1.02) | 1.02 ± 0.68 (0.48–1.01) | 0.96 ± 0.65 (0.54–1.05) |
| Pelvis—Rotation | x | x | x | 1.40 ± 1.21 (0.51–1.44) | 1.42 ± 1.26 (0.36–1.34) | 1.38 ± 1.17 (0.55–1.45) |
| RMSE | ROME | |||||
|---|---|---|---|---|---|---|
| A | B | C | A | B | C | |
| p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | |
| LT Hip—Abduction | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| LT Hip—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| LT Hip—Flexion | <0.001 | <0.001 | <0.001 | 0.004 | 0.011 | 0.006 |
| LT Knee—Abduction | <0.001 | <0.001 | <0.001 | 0.002 | <0.001 | 0.005 |
| LT Knee—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| LT Knee—Flexion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| LT Ankle—Abduction | <0.001 | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 |
| LT Ankle—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| LT Ankle—Flexion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Hip—Abduction | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Hip—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Hip—Flexion | <0.001 | <0.001 | <0.001 | 0.081 | <0.001 | <0.001 |
| RT Knee—Abduction | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Knee—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Knee—Flexion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Ankle—Abduktion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Ankle—Rotation | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| RT Ankle—Flexion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Pelvis—Flexion | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Pelvis—Obliquity | 0.001 | 0.002 | 0.002 | <0.001 | <0.001 | <0.001 |
| Pelvis—Rotation | x | x | x | <0.001 | <0.001 | <0.001 |
| ICC ± SD (95% CI) | |||
|---|---|---|---|
| A | B | C | |
| LT Hip—Abduction | 0.92 ± 0.07 (0.90–0.96) | 0.91 ± 0.07 (0.91–0.96) | 0.92 ± 0.06 (0.91–0.96) |
| LT Hip—Rotation | 0.75 ± 0.20 (0.70–0.86) | 0.76 ± 0.18 (0.73–0.87) | 0.76 ± 0.16 (0.72–0.84) |
| LT Hip—Flexion | 0.98 ± 0.01 (0.98–0.99) | 0.99 ± 0.01 (0.98–0.99) | 0.99 ± 0.01 (0.99–0.99) |
| LT Knee—Abduction | 0.57 ± 0.26 (0.53–0.73) | 0.58 ± 0.27 (0.54–0.75) | 0.57 ± 0.30 (0.52–0.75) |
| LT Knee—Rotation | 0.69 ± 0.13 (0.65–0.75) | 0.71 ± 0.13 (0.64–0.74) | 0.71 ± 0.12 (0.66–0.76) |
| LT Knee—Flexion | 0.98 ± 0.01 (0.97–0.98) | 0.98 ± 0.01 (0.98–0.99) | 0.98 ± 0.01 (0.98–0.99) |
| LT Ankle—Abduction | 0.79 ± 0.09 (0.75–0.81) | 0.79 ± 0.10 (0.77–0.84) | 0.80 ± 0.08 (0.78–0.84) |
| LT Ankle—Rotation | 0.82 ± 0.06 (0.81–0.86) | 0.84 ± 0.07 (0.82–0.88) | 0.85 ± 0.05 (0.85–0.89) |
| LT Ankle—Flexion | 0.94 ± 0.02 (0.94–0.96) | 0.94 ± 0.03 (0.94–0.96) | 0.94 ± 0.03 (0.94–0.96) |
| RT Hip—Abduction | 0.93 ± 0.05 (0.92–0.97) | 0.92 ± 0.06 (0.91–0.96) | 0.91 ± 0.07 (0.91–0.97) |
| RT Hip—Rotation | 0.76 ± 0.20 (0.75–0.90) | 0.76 ± 0.20 (0.74–0.90) | 0.75 ± 0.22 (0.75–0.92) |
| RT Hip—Flexion | 0.99 ± 0.01 (0.98–0.99) | 0.98 ± 0.01 (0.98–0.99) | 0.98 ± 0.01 (0.98–0.99) |
| RT Knee—Abduction | 0.56 ± 0.34 (0.56–0.83) | 0.56 ± 0.35 (0.57–0.84) | 0.56 ± 0.34 (0.52–0.78) |
| RT Knee—Rotation | 0.69 ± 0.14 (0.67–0.78) | 0.69 ± 0.14 (0.64–0.75) | 0.68 ± 0.16 (0.64–0.76) |
| RT Knee—Flexion | 0.98 ± 0.01 (0.98–0.99) | 0.98 ± 0.01 (0.98–0.99) | 0.98 ± 0.01 (0.98–0.99) |
| RT Ankle—Abduktion | 0.76 ± 0.13 (0.75–0.85) | 0.77 ± 0.13 (0.76–0.86) | 0.76 ± 0.16 (0.75–0.87) |
| RT Ankle—Rotation | 0.85 ± 0.05 (0.83–0.87) | 0.86 ± 0.05 (0.85–0.89) | 0.86 ± 0.06 (0.84–0.88) |
| RT Ankle—Flexion | 0.94 ± 0.02 (0.94–0.95) | 0.95 ± 0.02 (0.94–0.96) | 0.95 ± 0.03 (0.93–0.96) |
| Pelvis—Flexion | 0.90 ± 0.06 (0.89–0.94) | 0.90 ± 0.07 (0.89–0.95) | 0.90 ± 0.08 (0.90–0.96) |
| Pelvis—Obliquity | 0.52 ± 0.19 (0.50–0.64) | 0.52 ± 0.20 (0.51–0.67) | 0.52 ± 0.23 (0.47–0.65) |
| Pelvis—Rotation | 0.82 ± 0.12 (0.82–0.91) | 0.81 ± 0.12 (0.79–0.88) | 0.78 ± 0.15 (0.79–0.91) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics. Sensors 2018, 18, 1980. https://doi.org/10.3390/s18071980
Teufl W, Miezal M, Taetz B, Fröhlich M, Bleser G. Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics. Sensors. 2018; 18(7):1980. https://doi.org/10.3390/s18071980
Chicago/Turabian StyleTeufl, Wolfgang, Markus Miezal, Bertram Taetz, Michael Fröhlich, and Gabriele Bleser. 2018. "Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics" Sensors 18, no. 7: 1980. https://doi.org/10.3390/s18071980
APA StyleTeufl, W., Miezal, M., Taetz, B., Fröhlich, M., & Bleser, G. (2018). Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics. Sensors, 18(7), 1980. https://doi.org/10.3390/s18071980