
Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders


Abstract
:1. Introduction
- The proposed system is completely mobile, requiring only two IMUs and a data-processing notebook, and is usable in non-hospital settings, without the need for infrastructure.
- We propose a robust initial contact/foot-off (IC/FO) detection method that is able to operate under imperfect foot-relative sensor placement and orientation conditions. This method is also adaptive to pathological gait (i.e., foot dragging, the absence of the heel strike or left-right asymmetries), where the typical temporal phases of gait may not be observed.
- The system is able to detect and operate with side, back and turning steps, in contrast to solely walking straight, thanks to a novel particle filter-based foot orientation estimation algorithm.
- A rich set of standard spatio-temporal gait metrics is extracted, which can easily be interpreted by a clinician without the need for professional support. The extracted metrics include stride length, cadence, cycle time, stance time, swing time, stance ratio, speed, maximum/minimum clearance and turning rate.
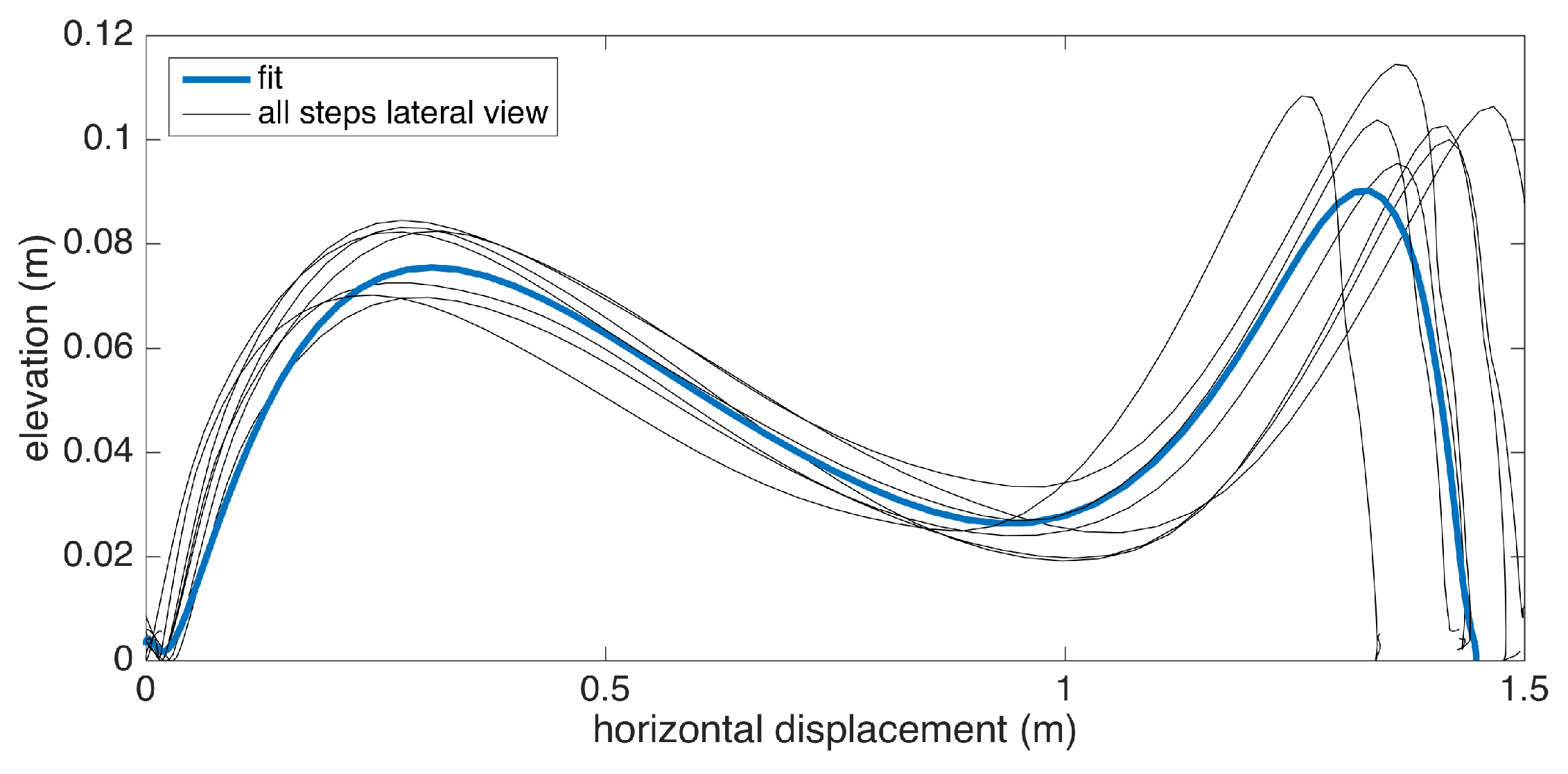
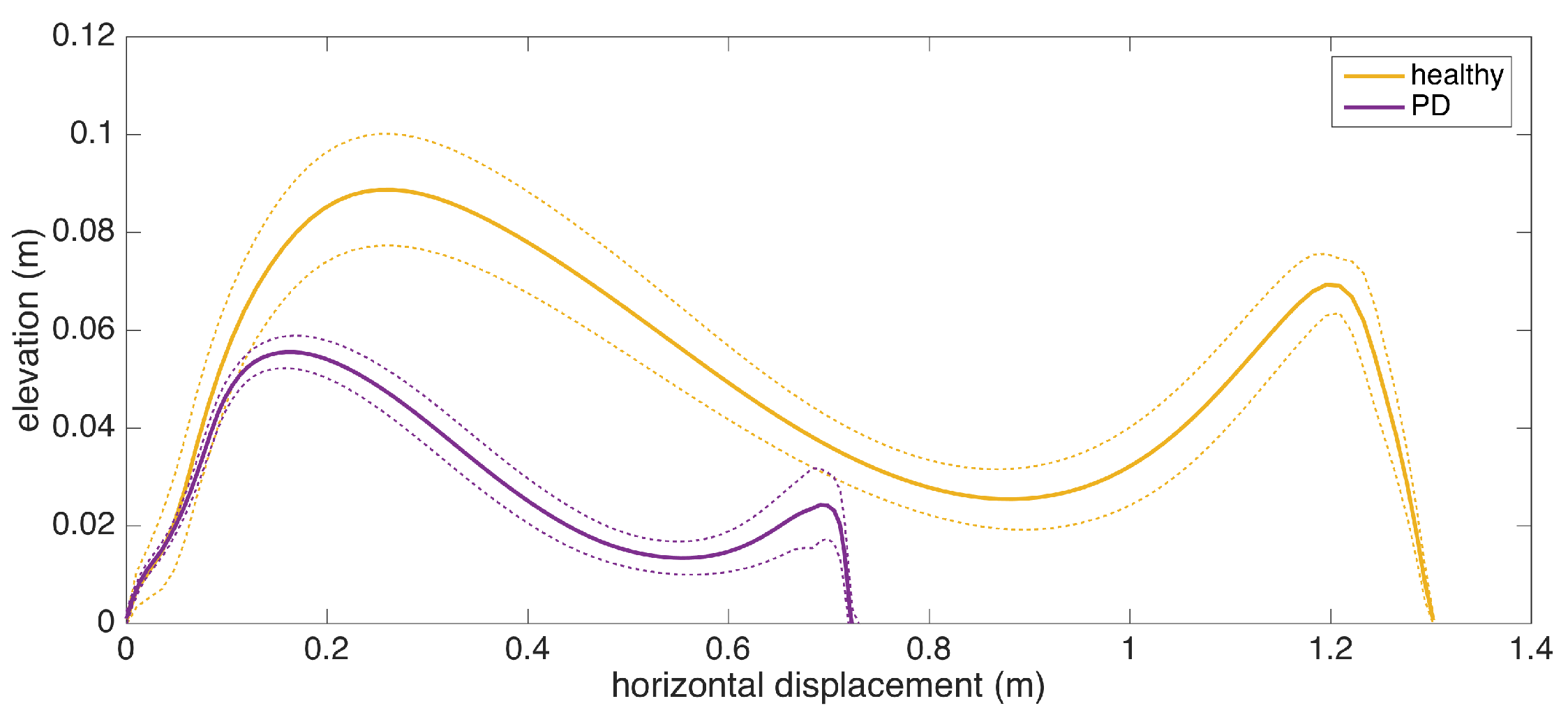
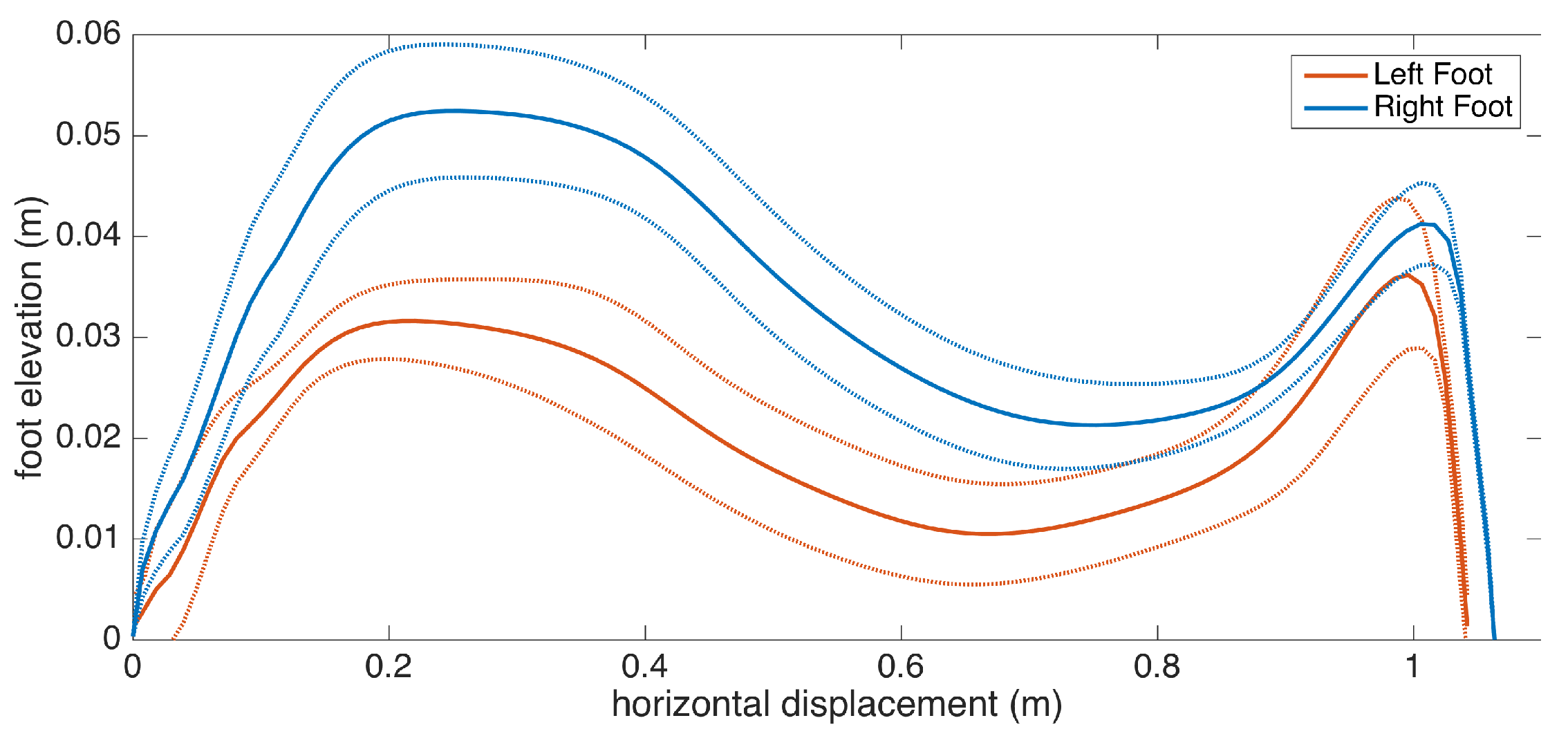
- In addition to numeric metrics, a new lateral stride profile visualization method is proposed, to give instant insight on spatial gait characteristics.
2. Background
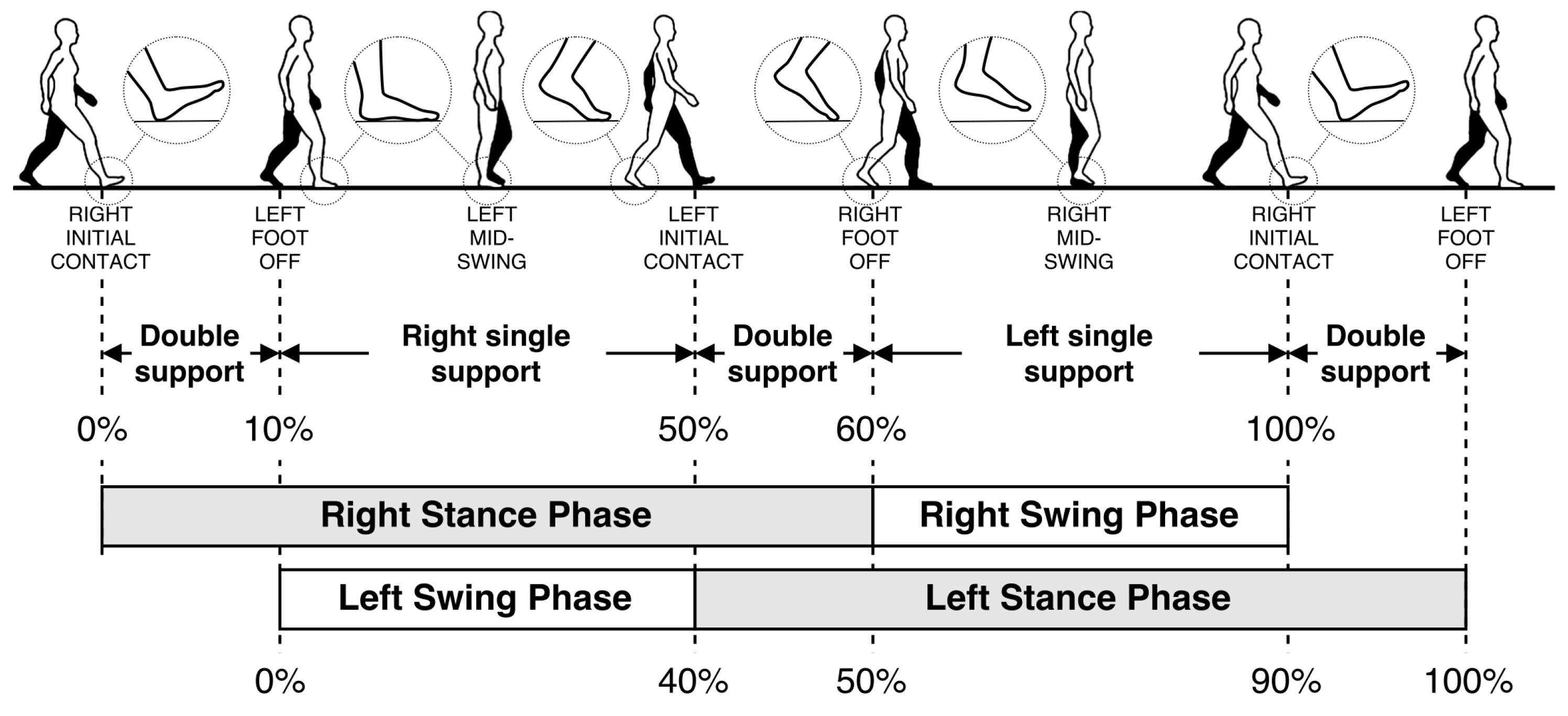
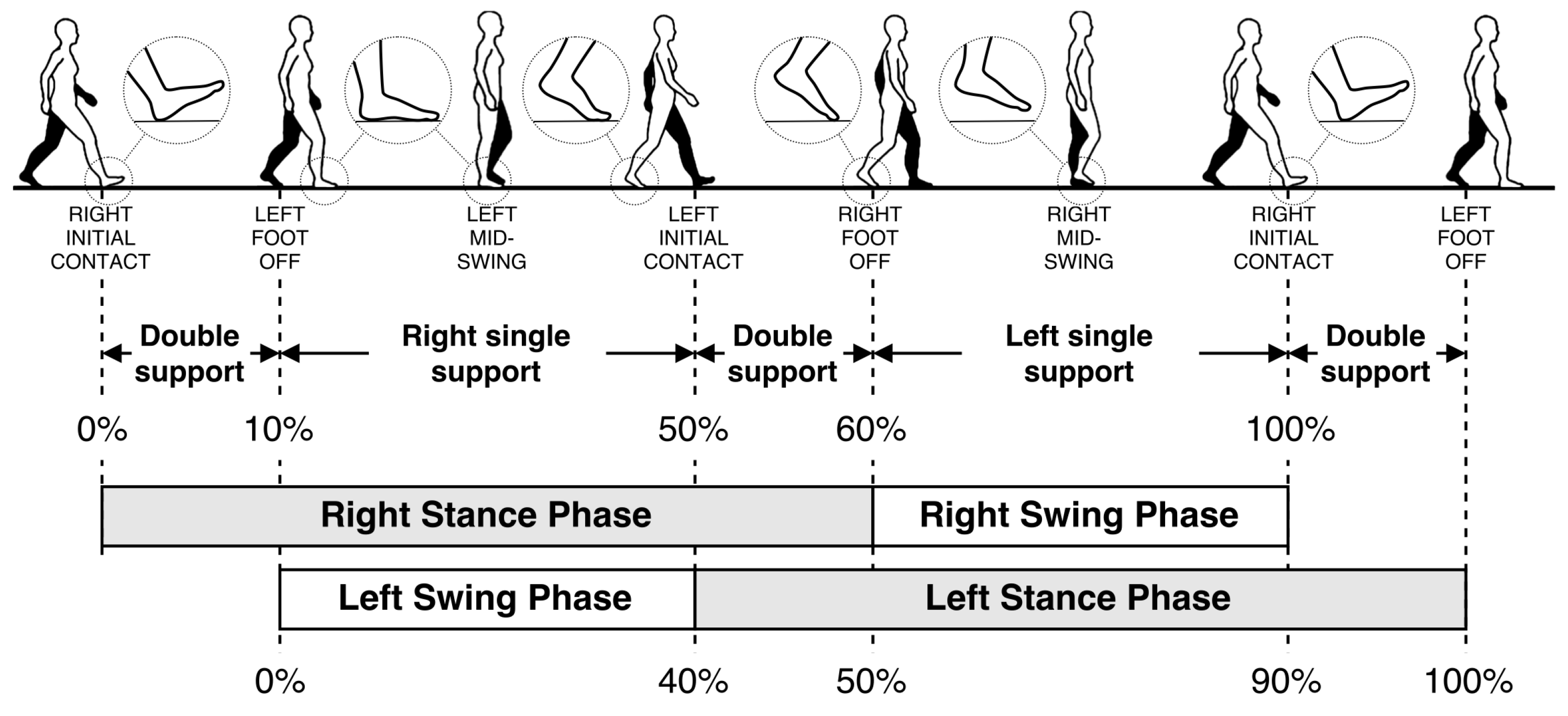
2.1. Human Gait Cycle and Gait Metrics
2.2. Challenges of Working with IMUs
2.2.1. Error Sources in IMUs
2.2.2. Operational Challenges and Difficulties in Data Collection
3. Related Work on Gait Analysis with IMUs
4. System Setup and Data Collection
4.1. Wearable IMU Setup
4.2. Data Collection
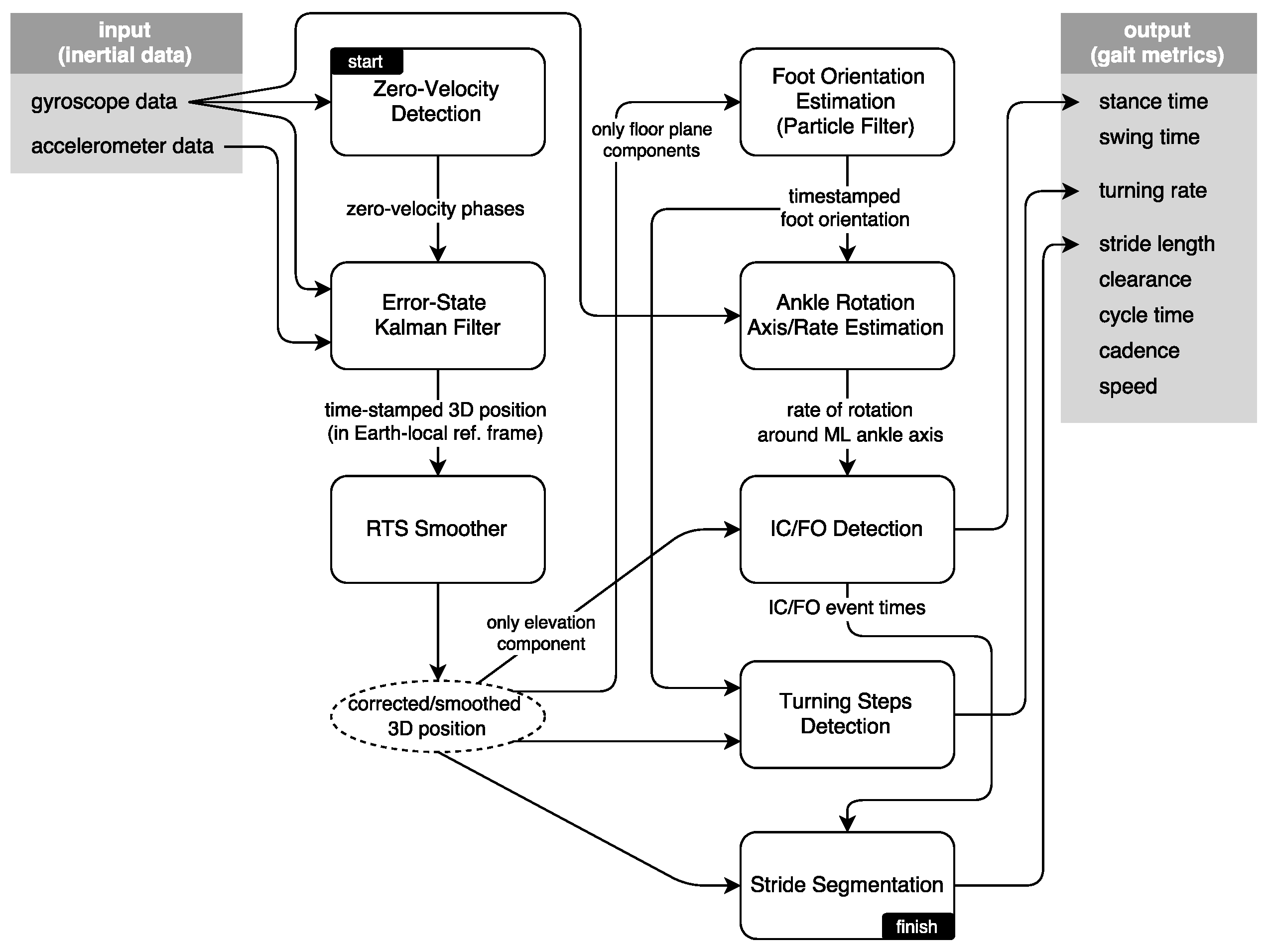
5. Methods
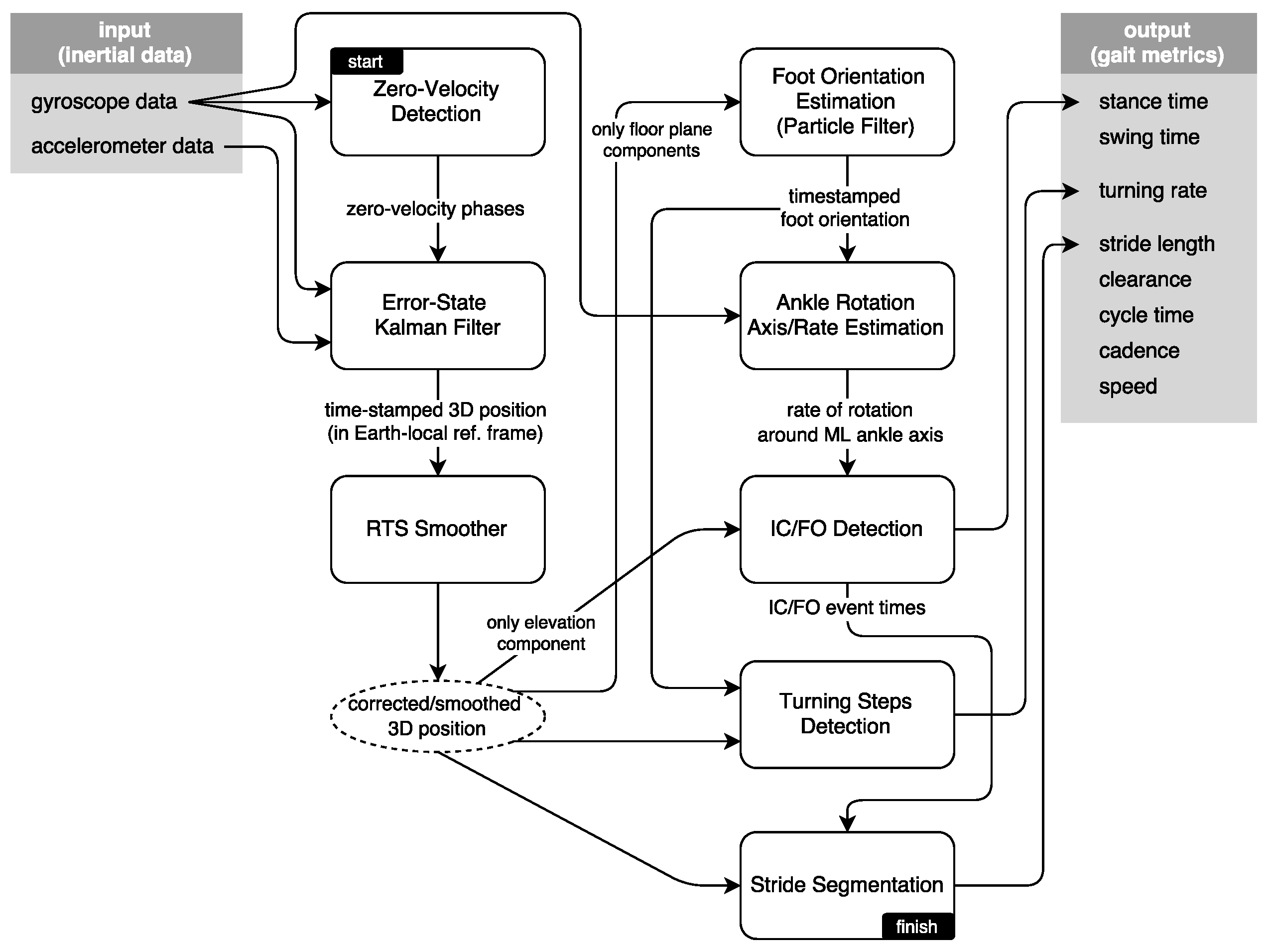
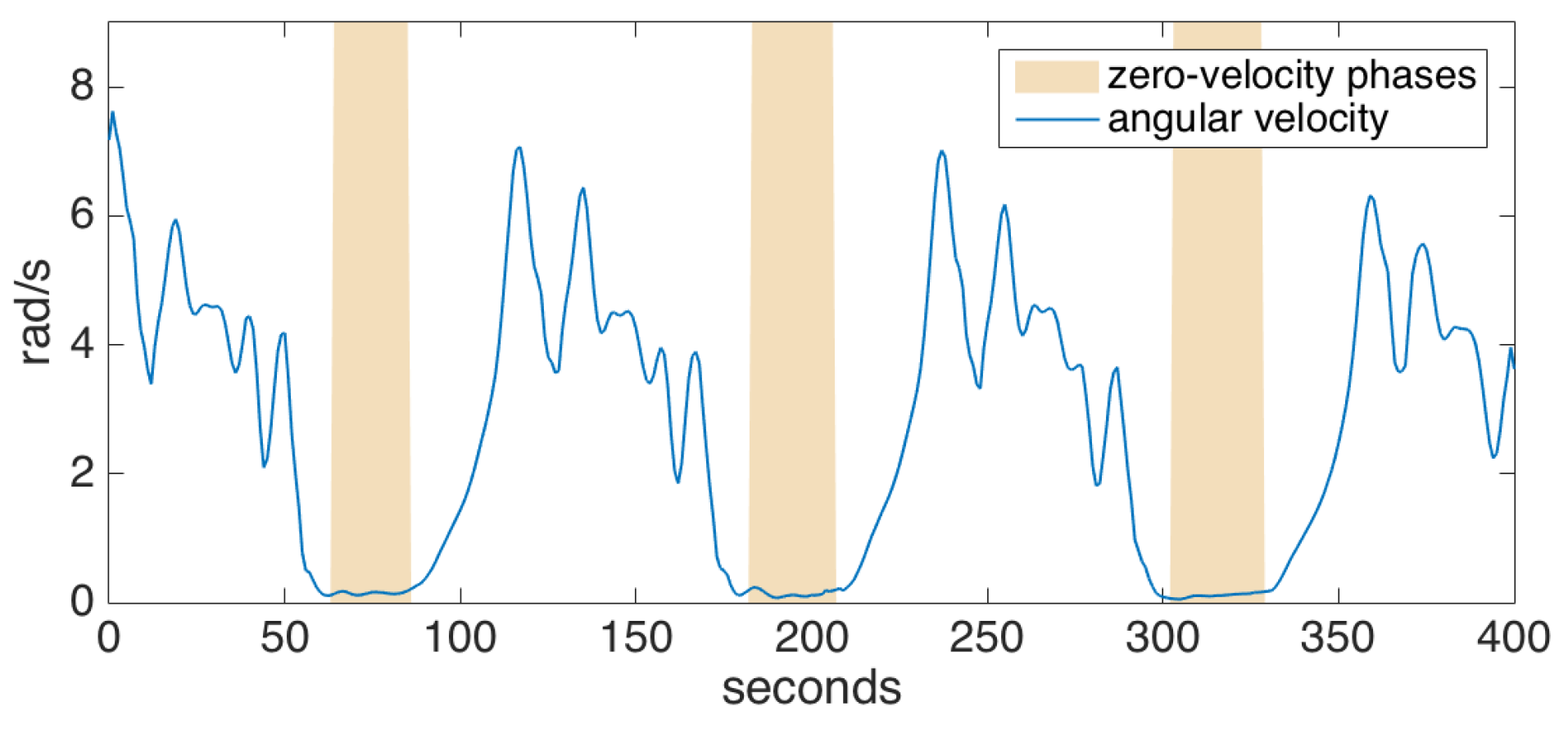
5.1. Zero-Velocity Updates
5.2. Error-State Tracking Kalman Filter
5.3. Smoothing
5.4. Foot Orientation Estimation
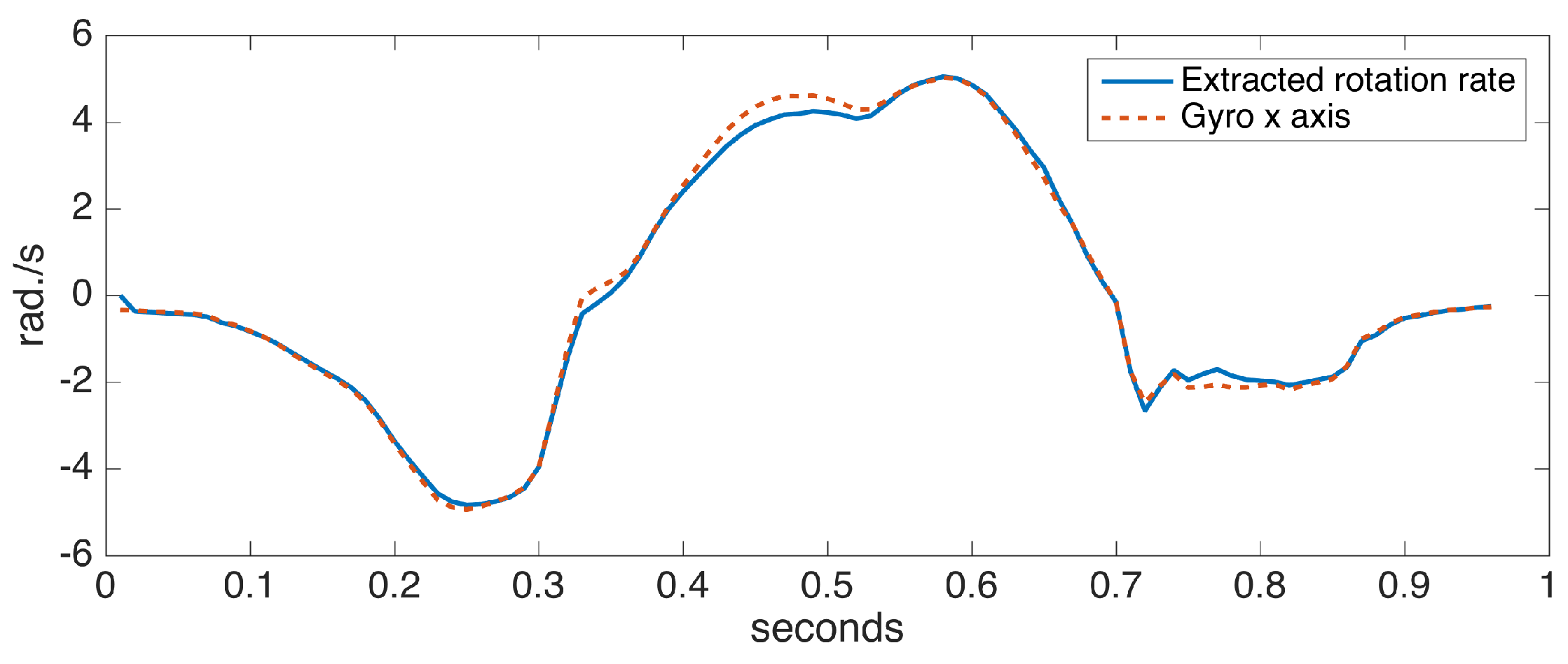
5.5. Foot Ankle Rotation Axis and Rate Estimation
5.6. IC/FO Events Detection
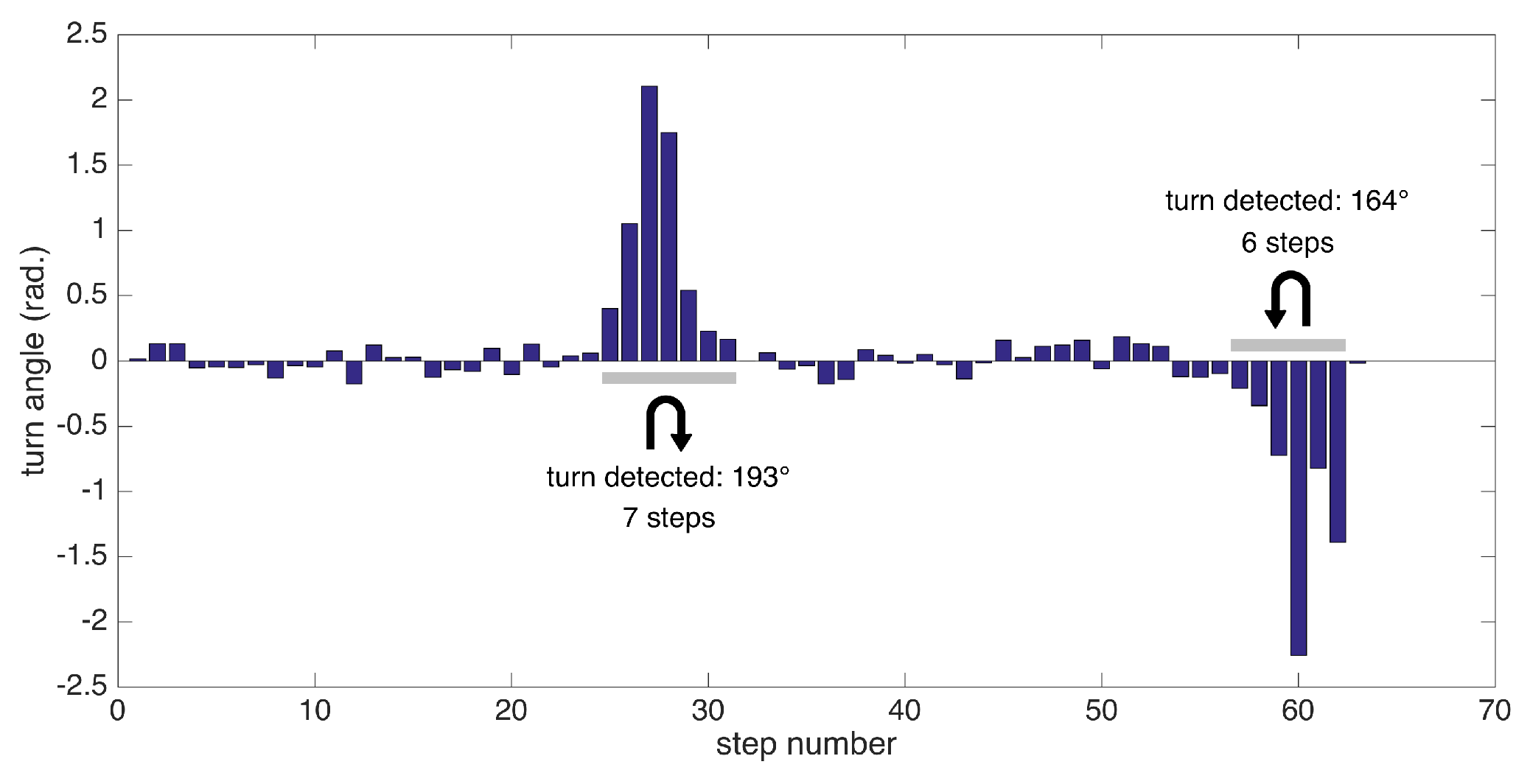
5.7. Detection of Turning Steps
5.8. Extraction of Spatio-Temporal Gait Metrics
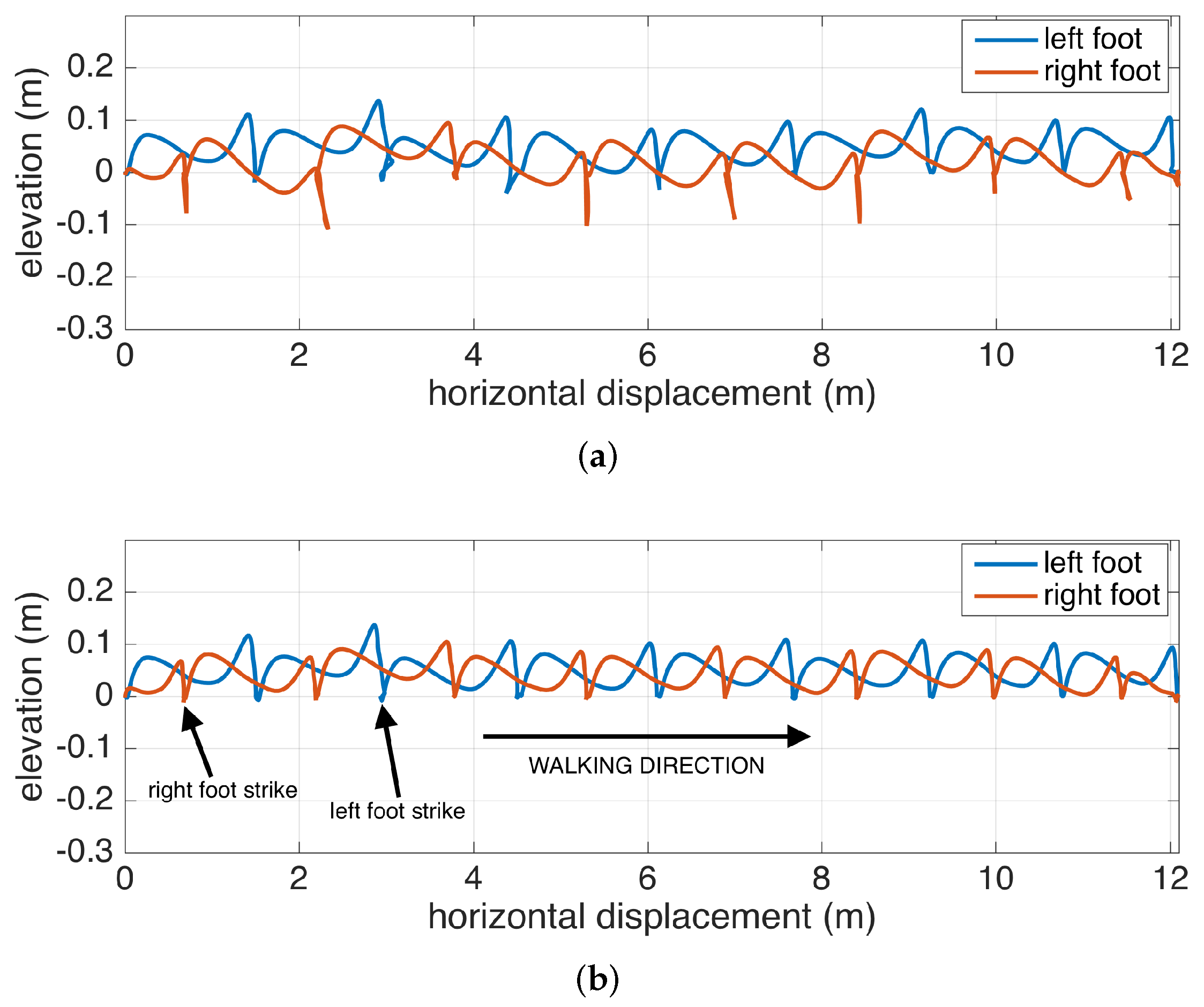
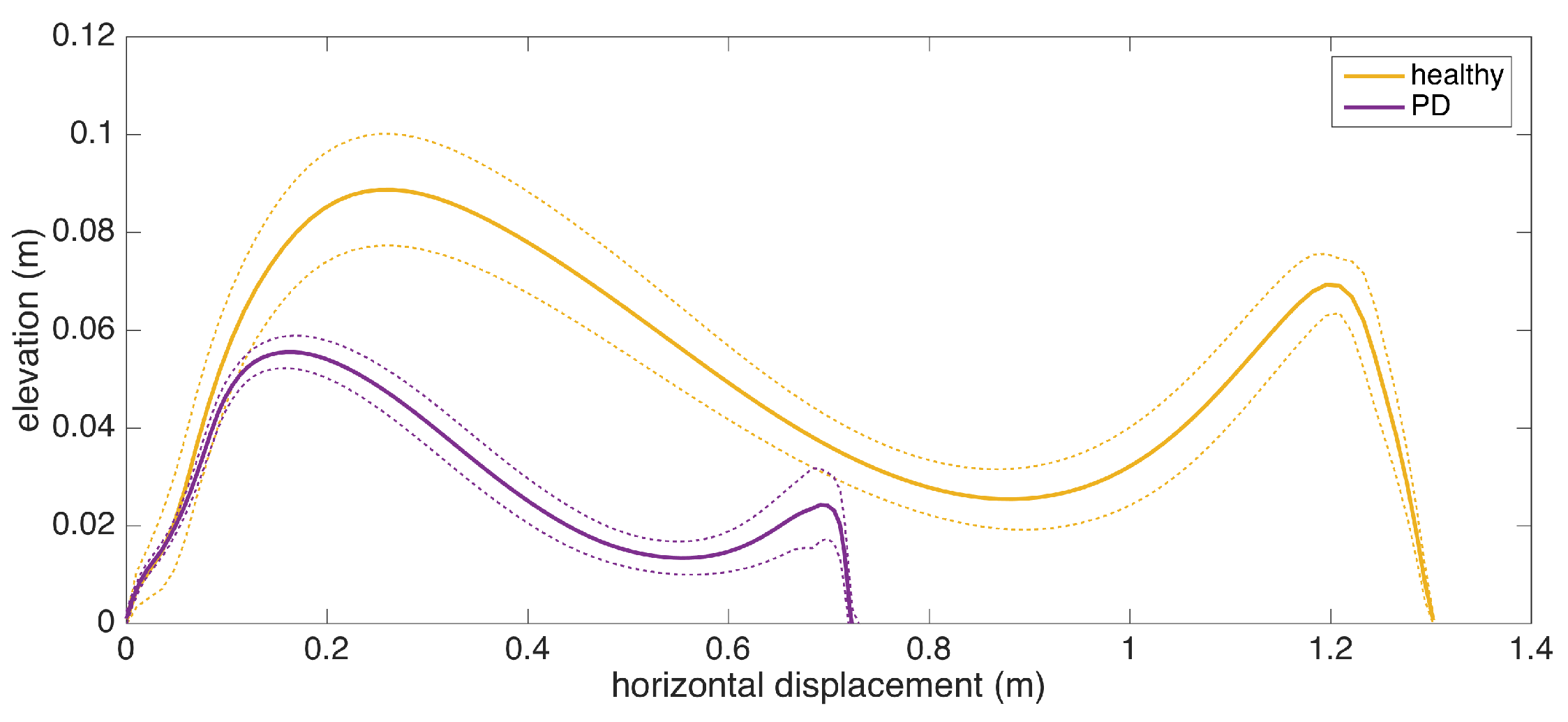
5.9. Average Lateral Stride Profile Visualization
6. Experiments
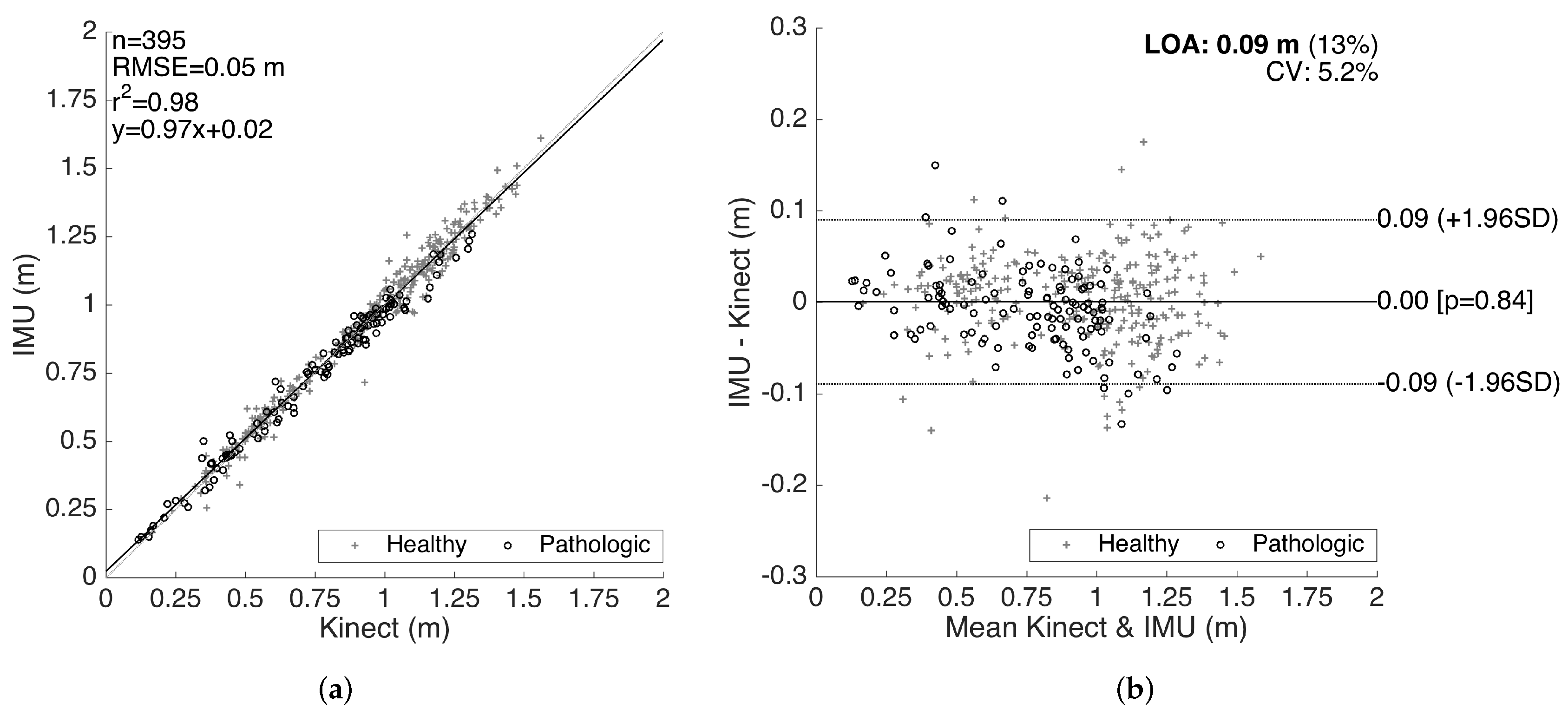
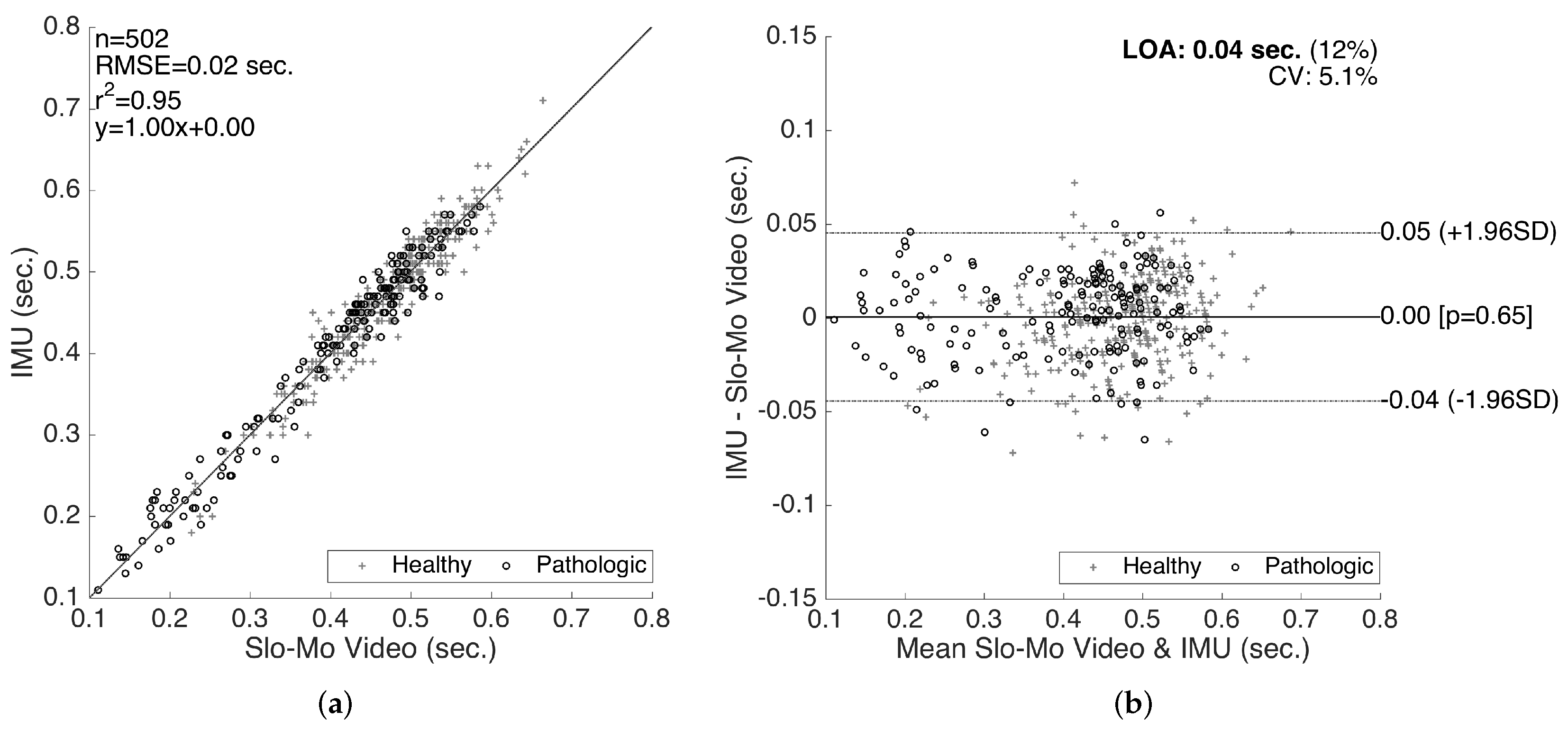
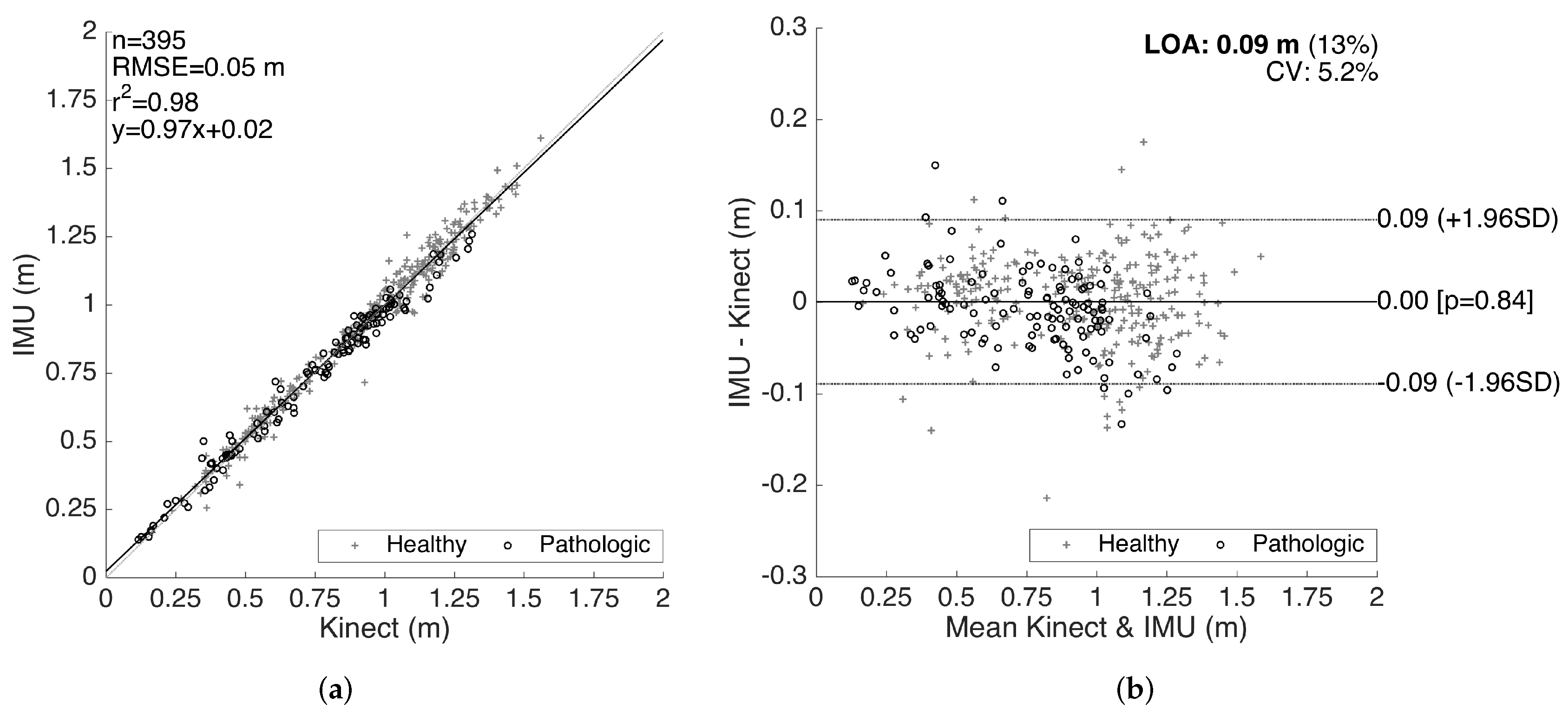
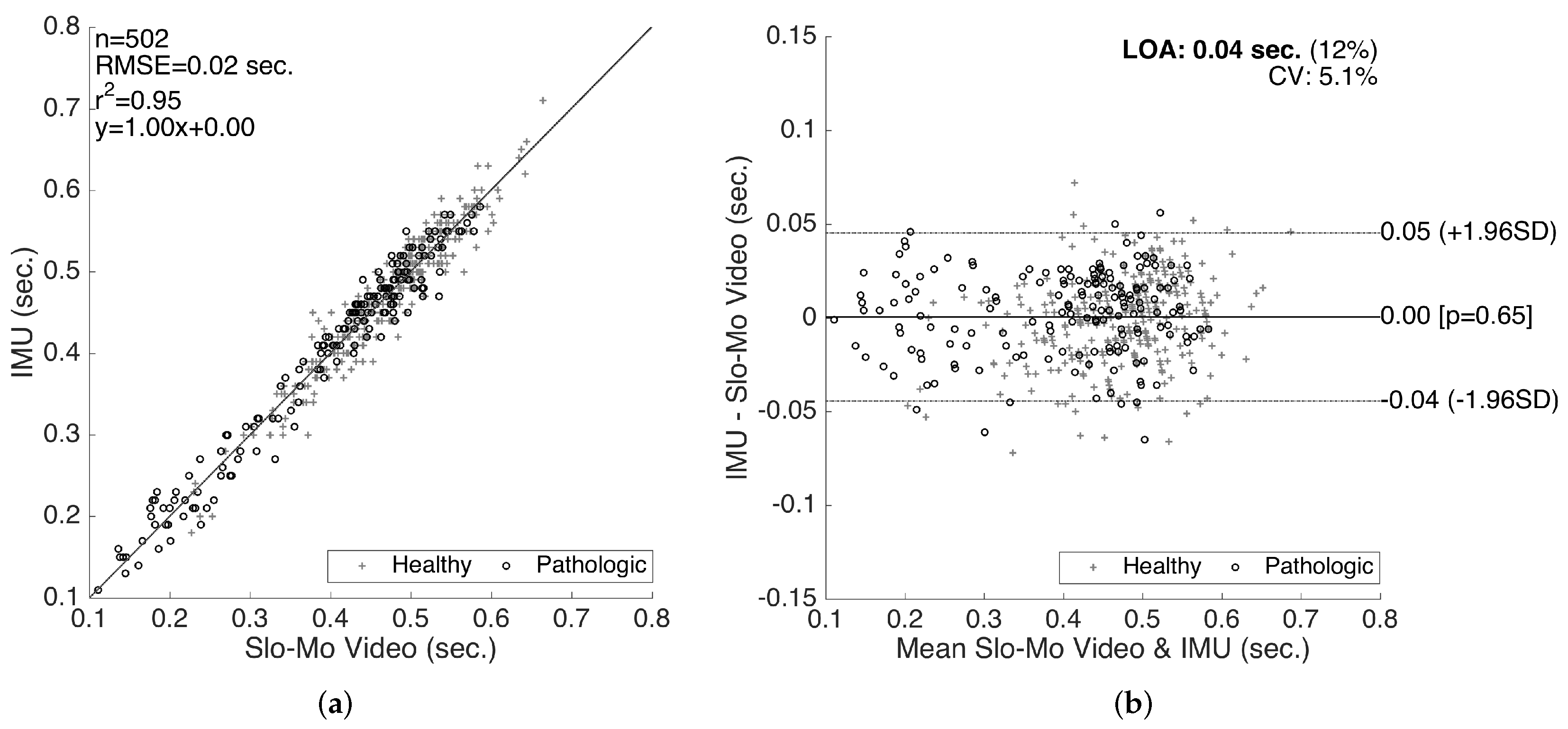
6.1. Comparative System Evaluation with Kinect and Slow Motion Camera
6.2. What Can the Metrics Tell Us?
6.2.1. Healthy Control Subjects
- Stride length is affected by age, height and gender, as well as the intended walking speed of the subject at the moment. Therefore, it is not possible to determine gait abnormality solely by looking at this metric; it has to be assessed with respect to the subject features and other metrics. However, extreme low values may indicate abnormality. The average stride length among the control subjects is m, with the lowest observed value being m. The average is well above 1 m, and extreme low values are uncommon. Therefore, the interpreter should look out for extreme values rather than small inconsistencies.
- Cadence is similar to stride length, as it is also affected by by age, height, gender and the subject’s intended pace. However, the effects are much weaker, suggested by the low variability (the average is ). As a person attempts to increase his/her pace, both the average stride length and cadence increase. Therefore, these two metrics should be interpreted with respect to each other. For instance, a low stride length value combined with high cadence might indicate the attempt to achieve a certain speed by compensating the small steps by a faster rate, which may be a sign of abnormality. The combined effect of these two metrics is reflected in speed. Cycle time is inversely proportional to cadence; thus, similar observations can be made.
- For the metrics that have separate components for each side (left and right), the most important observation for the control subjects is that there are no considerable asymmetries. The normal gait is left-right symmetric, and this property is reflected in the metrics. Asymmetries are mostly observed in the stance ratios and max. clearance values, and these two metrics usually also affect each other.
- In addition to the similarity of the left and right stance ratios (no asymmetry) for the control subjects, we also observe that they are very close to the normal stance ratio value of 0.6 over 1 (). The averages are for the left side and for the right side, with the variability being very low. Any significant deviation from the nominal value may indicate abnormality.
6.2.2. Neurological Disorder Subjects
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fortino, G.; Giannantonio, R.; Gravina, R.; Kuryloski, P.; Jafari, R. Enabling effective programming and flexible management of efficient body sensor network applications. IEEE Trans. Hum.-Mach. Syst. 2013, 43, 115–133. [Google Scholar] [CrossRef]
- Gravina, R.; Alinia, P.; Ghasemzadeh, H.; Fortino, G. Multi-sensor fusion in body sensor networks: State-of-the-art and research challenges. Inf. Fusion 2017, 35, 68–80. [Google Scholar] [CrossRef]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Schwarz, M.; Winkler, J.; Storch, A. Wearable sensor-based objective assessment of motor symptoms in Parkinson’s disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait analysis using wearable sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.N.; Suh, Y.S. Inertial sensor-based two feet motion tracking for gait analysis. Sensors 2013, 13, 5614–5629. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Ginis, P.; Hardegger, M.; Casamassima, F.; Rocchi, L.; Chiari, L. A Mobile Kalman-Filter Based Solution for the Real-Time Estimation of Spatio-Temporal Gait Parameters. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Whittle, M.W. Gait Analysis: An Introduction; Butterworth-Heinemann: Oxford, UK, 2014. [Google Scholar]
- Stolze, H.; Kuhtz-Buschbeck, J.P.; Drücke, H.; Jöhnk, K.; Illert, M.; Deuschl, G. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2001, 70, 289–297. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, G.C.; Brown, S.H.; Rice, R.R.; Thaut, M.H. Rhythmic auditory-motor facilitation of gait patterns in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Nallegowda, M.; Singh, U.; Handa, G.; Khanna, M.; Wadhwa, S.; Yadav, S.L.; Kumar, G.; Behari, M. Role of sensory input and muscle strength in maintenance of balance, gait, and posture in Parkinson’s disease: A pilot study. Am. J. Phys. Med. Rehabil. 2004, 83, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Ghasemzadeh, H.; Panuccio, P.; Trovato, S.; Fortino, G.; Jafari, R. Power-aware activity monitoring using distributed wearable sensors. IEEE Trans. Hum.-Mach. Syst. 2014, 44, 537–544. [Google Scholar] [CrossRef]
- Li, G.; Liu, T.; Gu, L.; Inoue, Y.; Ning, H.; Han, M. Wearable gait analysis system for ambulatory measurement of kinematics and kinetics. In Proceedings of the 2014 IEEE Sensors, Valencia, Spain, 2–5 November 2014; pp. 1316–1319. [Google Scholar]
- Chen, Y.; Hu, W.; Yang, Y.; Hou, J.; Wang, Z. A method to calibrate installation orientation errors of inertial sensors for gait analysis. In Proceedings of the 2014 IEEE International Conference on Information and Automation (ICIA), Hulun Buir, China, 28–30 July 2014; pp. 598–603. [Google Scholar]
- Takeda, R.; Lisco, G.; Fujisawa, T.; Gastaldi, L.; Tohyama, H.; Tadano, S. Drift removal for improving the accuracy of gait parameters using wearable sensor systems. Sensors 2014, 14, 23230–23247. [Google Scholar] [CrossRef] [PubMed]
- Jasiewicz, J.M.; Allum, J.H.; Middleton, J.W.; Barriskill, A.; Condie, P.; Purcell, B.; Li, R.C.T. Gait event detection using linear accelerometers or angular velocity transducers in able-bodied and spinal-cord injured individuals. Gait Posture 2006, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Ferster, M.L.; Mazilu, S.; Tröster, G. Gait Parameters Change Prior to Freezing in Parkinson’s Disease: A Data-driven Study with Wearable Inertial Units. In Proceedings of the 10th EAI International Conference on Body Area Networks (BodyNets ’15), Sydeny, Australia, 28–30 September 2015; ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering): Brussels, Belgium, 2015; pp. 159–166. [Google Scholar]
- Raveendranathan, N.; Galzarano, S.; Loseu, V.; Gravina, R.; Giannantonio, R.; Sgroi, M.; Jafari, R.; Fortino, G. From modeling to implementation of virtual sensors in body sensor networks. IEEE Sens. J. 2012, 12, 583–593. [Google Scholar] [CrossRef]
- Hundza, S.R.; Hook, W.R.; Harris, C.R.; Mahajan, S.V.; Leslie, P.A.; Spani, C.A.; Spalteholz, L.G.; Birch, B.J.; Commandeur, D.T.; Livingston, N.J. Accurate and reliable gait cycle detection in Parkinson’s disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Burkhard, P.R.; Vingerhoets, F.J.; Jolles, B.M.; Aminian, K. A novel approach to reducing number of sensing units for wearable gait analysis systems. IEEE Trans. Biomed. Eng. 2013, 60, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, S.J.M.; Benbasat, A.Y.; Scarborough, D.M.; Krebs, D.E.; Paradiso, J.A. Gait analysis using a shoe-integrated wireless sensor system. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ji, R. Estimate spatial-temporal parameters of human gait using inertial sensors. In Proceedings of the 2015 IEEE International Conference on Cyber Technology in Automation, Control, and Intelligent Systems (CYBER), Shenyang, China, 8–12 June 2015; pp. 1883–1888. [Google Scholar]
- González, I.; Fontecha, J.; Hervás, R.; Bravo, J. An ambulatory system for gait monitoring based on wireless sensorized insoles. Sensors 2015, 15, 16589–16613. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zheng, H.; Wang, H.; McClean, S.; Newell, D. iGAIT: An interactive accelerometer based gait analysis system. Comput. Methods Programs Biomed. 2012, 108, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.L.; Chung, P.C.; Wang, W.H.; Pai, M.C.; Wang, C.Y.; Lin, C.W.; Wu, H.L.; Wang, J.S. Gait and balance analysis for patients with Alzheimer’s disease using an inertial-sensor-based wearable instrument. IEEE J. Biomed. Health Inform. 2014, 18, 1822–1830. [Google Scholar] [CrossRef] [PubMed]
- Demonceau, M.; Donneau, A.F.; Croisier, J.L.; Skawiniak, E.; Boutaayamou, M.; Maquet, D.; Garraux, G. Contribution of a Trunk Accelerometer System to the Characterization of Gait in Patients with Mild-to-Moderate Parkinson’s Disease. IEEE J. Biomed. Health Inform. 2015, 19, 1803–1808. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: toward clinical and at home use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Suh, Y.S. A zero velocity detection algorithm using inertial sensors for pedestrian navigation systems. Sensors 2010, 10, 9163–9178. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Tsai, Y.S.; Yau, C.S.; Shie, H.H.; Wu, C.M. Test-Retest Reliability of an Automated Infrared-Assisted Trunk Accelerometer-Based Gait Analysis System. Sensors 2016, 16, 1156. [Google Scholar] [CrossRef] [PubMed]
- EXEL ExLs3, 2017. Available online: http://www.exelmicroel.com (accessed on 7 April 2017).
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Titterton, D.; Weston, J.L. Strapdown Inertial Navigation Technology; IET: Stevenage, UK, 2004; Volume 17. [Google Scholar]
- Skog, I.; Nilsson, J.O.; Händel, P. Evaluation of zero-velocity detectors for foot-mounted inertial navigation systems. In Proceedings of the 2010 IEEE International Conference on Indoor Positioning and Indoor Navigation (IPIN), Zurich, Switzerland, 15–17 September 2010; pp. 1–6. [Google Scholar]
- Microsoft Kinect v2. 2017. Available online: https://msdn.microsoft.com/en-us/library/dn758675.aspx (accessed on 7 April 2017).
- Baldewijns, G.; Verheyden, G.; Vanrumste, B.; Croonenborghs, T. Validation of the Kinect for gait analysis using the GAITRite walkway. In Proceedings of the 2014 IEEE 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5920–5923. [Google Scholar]
- Gabel, M.; Gilad-Bachrach, R.; Renshaw, E.; Schuster, A. Full body gait analysis with Kinect. In Proceedings of the 2012 IEEE Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, IL, USA, 28 August–1 September 2012; pp. 1964–1967. [Google Scholar]
- González, I.; López-Nava, I.H.; Fontecha, J.; Muñoz-Meléndez, A.; Pérez-SanPablo, A.I.; Quiñones-Urióstegui, I. Comparison between passive vision-based system and a wearable inertial-based system for estimating temporal gait parameters related to the GAITRite electronic walkway. J. Biomed. Inform. 2016, 62, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Stone, E.E.; Skubic, M. Unobtrusive, continuous, in-home gait measurement using the Microsoft Kinect. IEEE Trans. Biomed. Eng. 2013, 60, 2925–2932. [Google Scholar] [CrossRef] [PubMed]
- Ťupa, O.; Procházka, A.; Vyšata, O.; Schätz, M.; Mareš, J.; Vališ, M.; Mařík, V. Motion tracking and gait feature estimation for recognising Parkinson’s disease using MS Kinect. Biomed. Eng. Online 2015, 14, 97. [Google Scholar] [CrossRef] [PubMed]
- Rocha, A.P.; Choupina, H.; Fernandes, J.M.; Rosas, M.J.; Vaz, R.; Cunha, J.P.S. Parkinson’s disease assessment based on gait analysis using an innovative RGB-D camera system. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Chicago, IL, USA, 26–30 August 2014; pp. 3126–3129. [Google Scholar]
- Procházka, A.; Vyšata, O.; Vališ, M.; Ťupa, O.; Schätz, M.; Mařík, V. Use of the image and depth sensors of the Microsoft Kinect for the detection of gait disorders. Neural Comput. Appl. 2015, 26, 1621–1629. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gait Metric | Definition |
|---|---|
| Stride length (m) | Distance between two successive placements of the same foot. |
| Step length (m) | Distance by which a foot moves in front of the other foot. The sum of two successive step lengths corresponds to stride length. |
| Walking base (cm) | Side to side distance between the motion lines of the two feet. |
| Cadence | Number of steps taken per minute. |
| Cycle time (s) | Duration of a single stride. Cycle time is inversely proportional to cadence and hence can be used as an alternative to it. |
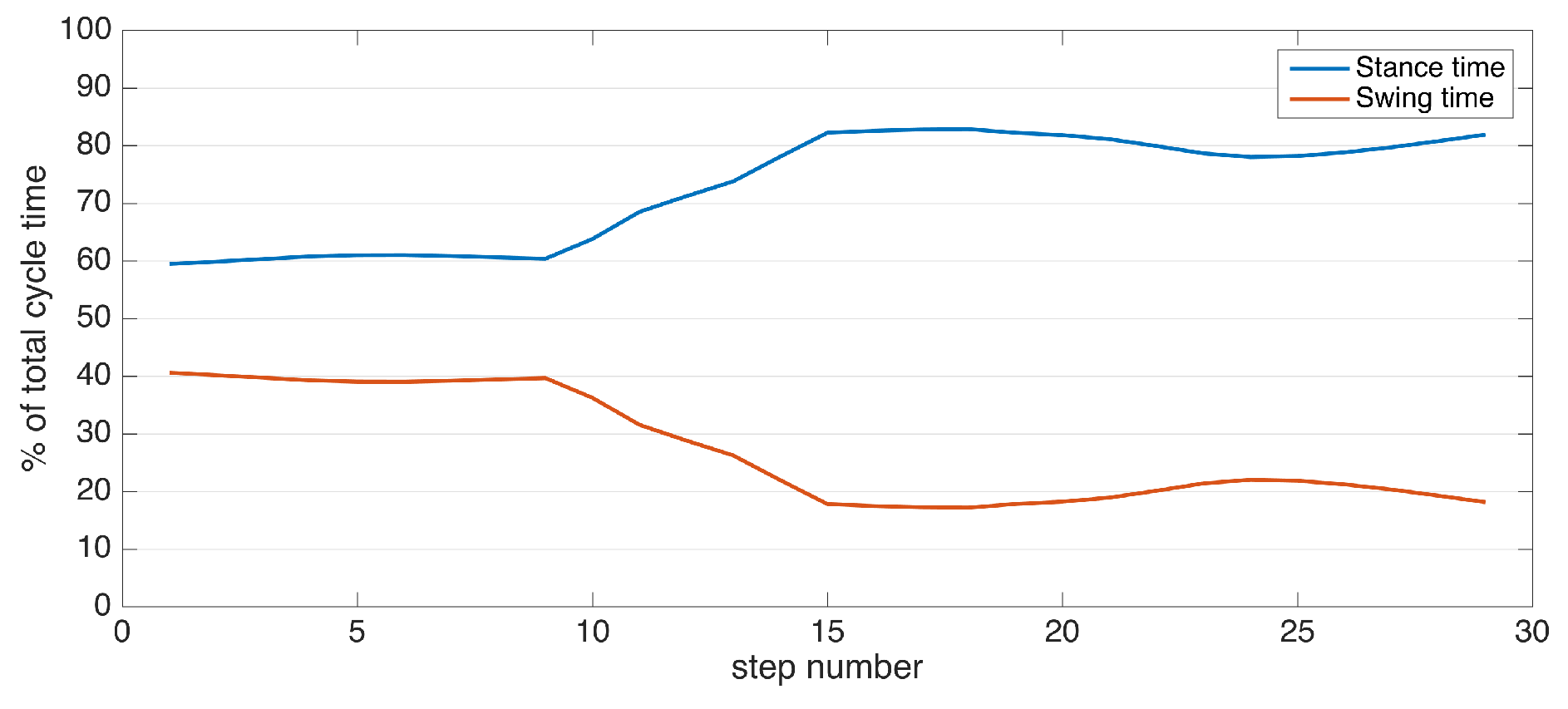
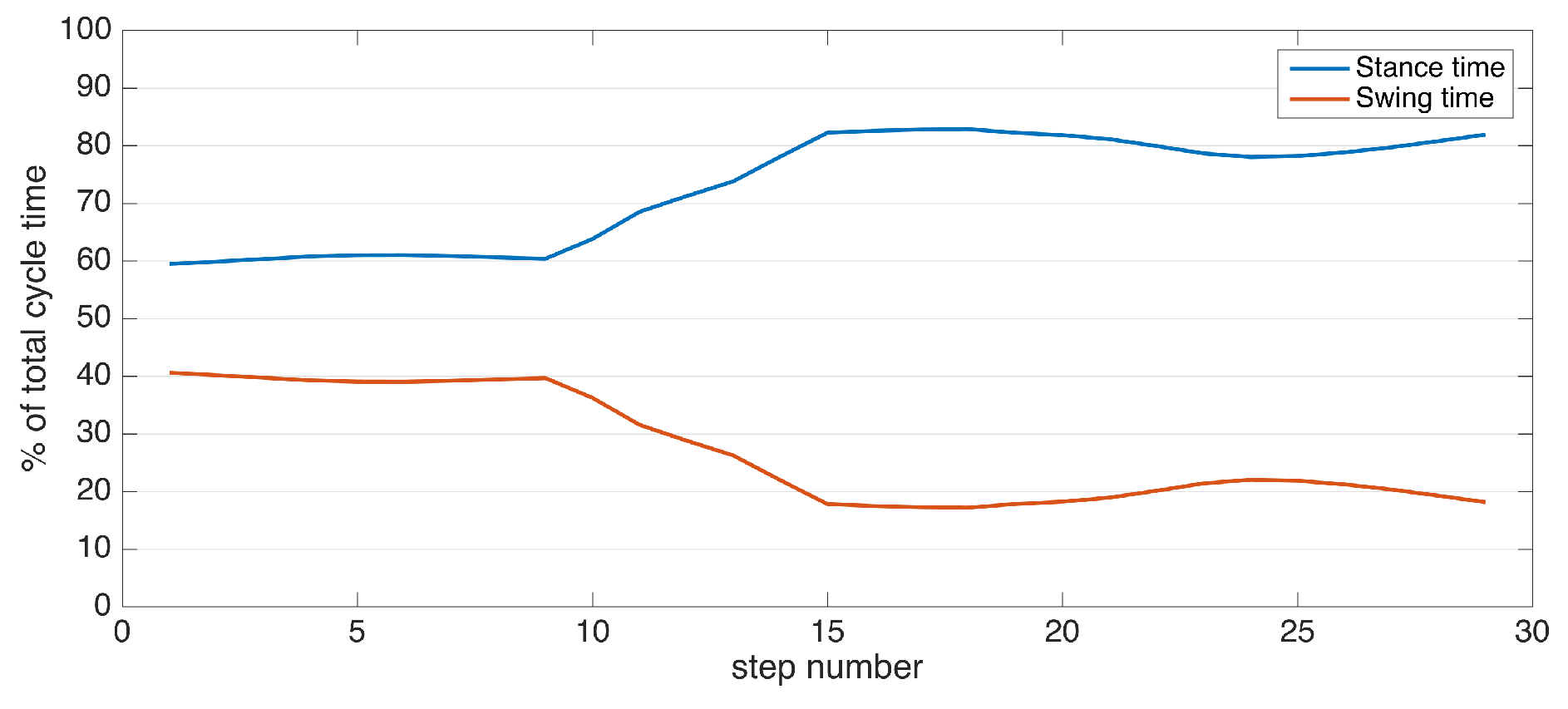
| Stance time (s) | Duration of stance phase, starting with initial-contact (IC) and ending with foot-off (FO) of the same foot. |
| Swing time (s) | Duration of swing phase, starting with FO and ending with IC of the same foot. |
| Speed (m/s) | Stride length/cycle time. |
| Clearance (cm) | elevation of the foot during the swing phase. This metric can be diversified as minimum and maximum foot clearance (elevation). |
| Turning rate (degrees/s) | Rate of the direction change of a foot. Positive values are normally observed during turning steps. |
| Ref. | Aim (Methodology) | Sensors | Subjects | Strengths (Novelty) | Weaknesses |
|---|---|---|---|---|---|
| [12] | Body joint angles’ estimation (3D-orientation differences between sensors). | Force sensors integrated in shoes; IMUs: 2 on ankles, 2 on knees, 1 on trunk | 1 healthy | Multiple sensors of different modalities enabling accurate joint angles information. | Only demonstrative results for a single subject (proof of concept). No gait metrics extracted. Relatively higher cost. |
| [6] | IC/FO detection (peak detection), stride length estimation (Kalman filtering with zero-velocity updates). | 2 IMUs on feet | 16 PD patients (ON state) | High spatial accuracy due to Kalman filtering methodology. Real patients. | IC/FO detection does not consider pathological gait. The patients are in the ON state. No control group. |
| [13] | Calibration to mitigate sensor misplacement (procedure with a set of specific movements), stride length estimation (double integration). | 2 IMUs on ankles | 8 healthy | Considers sensor placement errors and proposes a procedure to mitigate them. | Low spatial accuracy due to double integration. Only healthy subjects. |
| [14] | Drift removal in gyroscope signals. Estimation of cycle time, stride length, step length and cadence (geometric human locomotion model). | IMUs: 1 on pelvis, 2 on thighs, 2 on shanks, 2 on feet | 5 healthy | A comprehensive system with numerous sensors to extract a rich set of gait metrics. Drift removal to increase accuracy. | Only healthy subjects, not targeted towards gait abnormalities. Obtrusive due to the number of sensors. |
| [15] | IC/FO detection (peak detection). | IMUs: 2 on shanks, 2 on feet | 13 spinal cord injury patients, 12 healthy | Considers pathological gait. Experiments with real patients. | Obtrusive: the sensors are wired to a PDA; the sensors on shank are attached to the skin via double-sided tape. No spatial metrics. |
| [16] | IC/FO detection (peak detection), stride length estimation (geometric human locomotion model). | IMUs: 2 on forearms, 2 on shanks, 2 on thighs | 10 PD patients, 10 healthy | Rich set of spatio-temporal metrics. Real patients. | Low accuracy in spatial metrics. Obtrusive due to number of sensors. |
| [17] | Analyzing changes in spatio-temporal metrics prior to freezing of gait. IC/FO detection (peak detection), stride length estimation (double integration). | 2 IMUs on ankles | 5 PD patients | Rich set of spatio-temporal metrics. Real patients. | Low accuracy in spatial metrics. Limited number of subjects. No control group. |
| [18] | IC/FO detection (peak detection complemented with HMM). | 1 IMU alternated between various placements | 1 healthy | A solution adaptive to a variety of placements. | Not targeted for pathological gait. Only one healthy subject. |
| [19] | Estimation of cycle time and stride length (geometric human locomotion model). | IMUs: 2 on shanks, 2 on thighs | 6 PD patients, 7 healthy | Real patients. | Low accuracy in spatial metrics. Stance/swing times are not extracted (only cycle time). |
| [20] | Estimation of stride length and stride velocity (geometric human locomotion model). | 2 IMUs on shanks | 10 PD, 36 hip-replacement, 7 coxarthrosis patients, 18 healthy | High number of real patients with multiple different conditions affecting gait. | The datasets belong to previous studies and are not collected by the authors. Limited temporal metrics (only stride velocity). |
| [21] | IC/FO detection (force sensors), stride length estimation (double integration). | Force sensors and an IMU integrated in a shoe | 5 PD patients, 10 healthy | Different modalities integrated in a shoe. Real patients. | Low spatial accuracy due to double integration. Relatively higher cost. |
| [22] | IC/FO detection (peak detection), stride length estimation (double integration aided with zero-velocity updates). | 2 IMUs on feet | 10 healthy | Increased spatial accuracy due to zero-velocity updates (compared to only double integration). | Obtrusive system: The sensors are wired to a control node. Only healthy subjects. |
| [23] | Classification of different movement patterns, estimation of stance/swing times (naive Bayes classifier). | Force sensors and an IMU integrated in an insole | 5 healthy | Ability to detect different types of steps including lateral and backward walking. | Only healthy subjects, not targeted towards gait abnormalities. Relatively higher cost. |
| [24] | Detection of heel strikes (peak detection), asymmetry indices from raw acceleration intensity (spectral analysis). | 1 IMU on trunk | 15 healthy | Asymmetry indicators computed from raw data. | Only healthy subjects. No standard spatio-temporal metrics extracted. |
| [25] | IC/FO detection (peak detection), balance detection (raw acceleration signal processing). | IMUs: 2 on feet, 1 on waist | 21 AD patients, 50 healthy | Balance features that indicate the intensity of lateral sway. | IC/FO detection methodology is not novel. No spatial metrics extracted. |
| [26] | Regularity and symmetry indices (Fourier analysis on raw acceleration signals). | 1 IMU on waist | 64 PD patients, 32 healthy | The high number of real patients. | The methodology is not clearly explained. |
| [27] | IC/FO detection (wavelet-based time and frequency analysis), stride length estimation (inverted pendulum model with double integration). | 1 IMU on trunk | 30 PD patients, 30 healthy | High number of real patients. | Low accuracy in spatial metrics. |
| [5] | 3D feet position estimation (Kalman filtering with zero-velocity updates, RTS smoothing). | 2 IMUs on feet, 1 camera on foot for spatial sync. | 1 healthy | High spatial accuracy. | No standard spatio-temporal metrics extracted. Not targeted for pathological gait. |
| Subject ID | Gender | Age | Height (m) | Stride Length (m) | Cadence (steps/min) | Cycle Time (s) | L Stance Time (s) | R Stance Time (s) | L Swing Time (s) | R Swing Time (s) | L Stance Ratio | R Stance Ratio | Speed (m/s) | L Max. Clearance (cm) | R Max. Clearance (cm) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C-1 | F | 28 | 1.70 | 1.13 | 92.9 | 1.29 | 0.84 | 0.74 | 0.50 | 0.51 | 0.63 | 0.59 | 0.87 | 7.3 | 7.2 |
| C-2 | F | 49 | 1.55 | 1.17 | 103.6 | 1.16 | 0.74 | 0.70 | 0.44 | 0.44 | 0.63 | 0.61 | 1.01 | 8.5 | 8.3 |
| C-3 | M | 26 | 1.72 | 1.11 | 96.8 | 1.24 | 0.73 | 0.76 | 0.51 | 0.49 | 0.59 | 0.61 | 0.89 | 8.2 | 8.1 |
| C-4 | M | 27 | 1.82 | 1.44 | 96.2 | 1.25 | 0.77 | 0.70 | 0.53 | 0.50 | 0.59 | 0.58 | 1.15 | 8.2 | 8.8 |
| C-5 | F | 25 | 1.68 | 1.16 | 92.1 | 1.30 | 0.82 | 0.80 | 0.47 | 0.52 | 0.64 | 0.61 | 0.89 | 8.5 | 8.5 |
| C-6 | M | 34 | 1.76 | 1.14 | 95.1 | 1.26 | 0.77 | 0.80 | 0.47 | 0.50 | 0.62 | 0.62 | 0.91 | 8.2 | 8.1 |
| C-7 | M | 29 | 1.73 | 1.22 | 92.1 | 1.30 | 0.82 | 0.84 | 0.50 | 0.45 | 0.62 | 0.65 | 0.94 | 9.3 | 8.9 |
| C-8 | M | 39 | 1.65 | 1.18 | 105.0 | 1.14 | 0.70 | 0.71 | 0.44 | 0.44 | 0.62 | 0.62 | 1.03 | 8.7 | 8.6 |
| C-9 | M | 36 | 1.80 | 1.04 | 83.2 | 1.44 | 0.91 | 0.88 | 0.55 | 0.55 | 0.63 | 0.62 | 0.72 | 9.0 | 8.7 |
| C-10 | M | 53 | 1.74 | 1.39 | 88.2 | 1.36 | 0.79 | 0.82 | 0.57 | 0.54 | 0.58 | 0.60 | 1.03 | 9.0 | 8.9 |
| C-11 | F | 76 | 1.55 | 0.93 | 87.1 | 1.38 | 0.86 | 0.88 | 0.50 | 0.52 | 0.63 | 0.63 | 0.68 | 7.0 | 7.2 |
| C-12 | F | 63 | 1.64 | 1.02 | 91.7 | 1.31 | 0.78 | 0.69 | 0.58 | 0.58 | 0.58 | 0.55 | 0.78 | 7.6 | 7.4 |
| C-13 | F | 67 | 1.59 | 1.22 | 96.8 | 1.24 | 0.74 | 0.70 | 0.51 | 0.53 | 0.59 | 0.57 | 0.99 | 7.7 | 7.7 |
| C-14 | M | 48 | 1.73 | 1.37 | 95.2 | 1.26 | 0.76 | 0.76 | 0.49 | 0.51 | 0.61 | 0.60 | 1.09 | 9.1 | 9.0 |
| C-15 | F | 42 | 1.63 | 1.01 | 81.2 | 1.48 | 0.91 | 0.92 | 0.58 | 0.55 | 0.61 | 0.63 | 0.68 | 6.9 | 6.8 |
| C-16 | F | 60 | 1.60 | 1.01 | 100.0 | 1.20 | 0.78 | 0.78 | 0.42 | 0.43 | 0.65 | 0.65 | 0.85 | 6.7 | 6.5 |
| Subject ID | Gender | Age | Height (m) | Condition | Stride Length (m) | Cadence (steps/min) | Cycle Time (s) | L Stance Time (s) | R Stance Time (s) | L Swing Time (s) | R Swing Time (s) | L Stance Ratio | R Stance Ratio | Speed (m/s) | L Max. Clearance (cm) | R Max. Clearance (cm) | Turning Rate (degree/s) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 72 | 1.74 | Mixed | 1.20 | 88.9 | 1.35 | 0.84 | 0.84 | 0.50 | 0.52 | 0.62 | 0.62 | 0.88 | 8.6 | 9.1 | 55.9 |
| 2 | M | 85 | 1.65 | DLB | 0.99 | 109.3 | 1.10 | 0.66 | 0.71 | 0.44 | 0.39 | 0.60 | 0.65 | 0.90 | 7.3 | 6.9 | 45.2 |
| 3 | F | 73 | 1.62 | PD | 1.11 | 99.9 | 1.20 | 0.76 | 0.70 | 0.45 | 0.49 | 0.63 | 0.58 | 0.92 | 3.9 | 5.3 | 50.3 |
| 4 | F | 82 | 1.58 | PD | 0.50 | 72.4 | 1.66 | 1.18 | 1.18 | 0.47 | 0.49 | 0.72 | 0.71 | 0.30 | 4.5 | 4.4 | 29.0 |
| 5 | M | 80 | 1.76 | Mixed | 1.10 | 75.0 | 1.60 | 0.87 | 1.02 | 0.71 | 0.60 | 0.55 | 0.63 | 0.69 | 7.7 | 8.4 | 22.6 |
| 6 | M | 88 | 1.80 | PD | 0.36 | 87.1 | 1.38 | 0.99 | 1.00 | 0.37 | 0.40 | 0.73 | 0.72 | 0.26 | 2.1 | 3.7 | 19.3 |
| 7 | F | 85 | 1.65 | NPH | 0.81 | 88.3 | 1.36 | 0.86 | 0.85 | 0.49 | 0.52 | 0.64 | 0.62 | 0.60 | 5.3 | 6.0 | 28.8 |
| 8 | F | 81 | 1.60 | PD | 0.72 | 70.6 | 1.70 | 1.15 | 1.12 | 0.55 | 0.58 | 0.68 | 0.66 | 0.42 | 5.2 | 5.9 | 32.5 |
| 9 | F | 80 | 1.60 | Mixed | 0.73 | 82.6 | 1.45 | 0.94 | 0.96 | 0.53 | 0.48 | 0.64 | 0.67 | 0.50 | 4.5 | 5.2 | 38.7 |
| 10 | M | 82 | 1.65 | VaD | 1.16 | 88.4 | 1.36 | 0.78 | 0.82 | 0.57 | 0.56 | 0.58 | 0.59 | 0.86 | 9.4 | 10.7 | 41.3 |
| 11 | F | 52 | 1.56 | PD | 0.83 | 123.0 | 0.98 | 0.57 | 0.67 | 0.40 | 0.32 | 0.59 | 0.68 | 0.85 | 3.5 | 6.0 | 59.1 |
| 12 | F | 90 | 1.60 | PD | 0.53 | 119.3 | 1.01 | 0.67 | 0.61 | 0.35 | 0.38 | 0.66 | 0.62 | 0.52 | 3.7 | 4.0 | 18.1 |
| 13 | M | 83 | 1.59 | PD | 0.93 | 95.6 | 1.26 | 0.77 | 0.76 | 0.48 | 0.50 | 0.62 | 0.60 | 0.74 | 6.9 | 6.1 | 45.1 |
| 14 | M | 76 | 1.82 | MCI | 1.31 | 92.2 | 1.30 | 0.76 | 0.76 | 0.56 | 0.53 | 0.58 | 0.59 | 1.01 | 9.0 | 9.3 | 45.1 |
| 15 | M | 84 | 1.69 | VaP | 0.45 | 90.9 | 1.32 | 0.89 | 0.87 | 0.43 | 0.45 | 0.67 | 0.66 | 0.34 | 3.7 | 3.0 | 29.0 |
| 16 | F | 82 | 1.50 | DLB | 0.83 | 83.8 | 1.43 | 0.96 | 0.84 | 0.47 | 0.59 | 0.67 | 0.59 | 0.58 | 5.2 | 4.8 | 35.8 |
| 17-ON | F | 51 | 1.65 | PD | 0.82 | 98.6 | 1.22 | 0.85 | 0.88 | 0.37 | 0.33 | 0.69 | 0.72 | 0.67 | 3.4 | 3.3 | 30.2 |
| 17-OFF | F | 51 | 1.65 | PD | 0.55 | 95.6 | 1.26 | 0.99 | 1.07 | 0.27 | 0.18 | 0.79 | 0.85 | 0.44 | 2.9 | 2.4 | 40.5 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tunca, C.; Pehlivan, N.; Ak, N.; Arnrich, B.; Salur, G.; Ersoy, C. Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders. Sensors 2017, 17, 825. https://doi.org/10.3390/s17040825
Tunca C, Pehlivan N, Ak N, Arnrich B, Salur G, Ersoy C. Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders. Sensors. 2017; 17(4):825. https://doi.org/10.3390/s17040825
Chicago/Turabian StyleTunca, Can, Nezihe Pehlivan, Nağme Ak, Bert Arnrich, Gülüstü Salur, and Cem Ersoy. 2017. "Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders" Sensors 17, no. 4: 825. https://doi.org/10.3390/s17040825
APA StyleTunca, C., Pehlivan, N., Ak, N., Arnrich, B., Salur, G., & Ersoy, C. (2017). Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders. Sensors, 17(4), 825. https://doi.org/10.3390/s17040825