Real-Time Monitoring in Home-Based Cardiac Rehabilitation Using Wrist-Worn Heart Rate Devices

 ,
, 

Abstract
:1. Introduction
1.1. Home-Based Cardiac Rehabilitation
1.2. Related Works
- Wear and play devices. Wrist-worn devices are noninvasive because of the heart rate sensor is embedded. In addition, they do not require placement of electrodes on the body prior to physical activity. Moreover, they are worn as a watch in an everyday manner.
- Modeling a theoretical high-quality CRP. A standardized CRP, which was developed by the CRU of Hospital Complex of Jaen (Spain) was introduced in the home-base approach for each patient’s care in a personalized way. A linguistic approach based on fuzzy logic [7] is included to model the CRP and the expert knowledge from the cardiac rehabilitation team.
- Real-time smart monitoring is embedded in the wrist-worn device in order to: (1) show patients the adherence to CRP during physical activity; and (2) prevent unsuitable and inadequate HR ranges.
- Practical methods are described for applying the theoretical model to wearable computing.
2. Methodology
2.1. Setting a Cardiac Rehabilitation Program
- The maximal or peak heart rate (), that is, the number of contractions of the heart per minute (bpm) when it is working at its maximum capacity without severe problems.
- The basal or resting heart rate (), that is, the bpm when the patient is awake, relaxed, and has not recently exercised.
- The first ventilatory threshold (), that is, the bpm which represents a level of intensity when blood lactate accumulates faster than it can be cleared, this being related to the aerobic threshold.
- The second ventilatory threshold (), that is, the bpm which represents the point where lactate is rapidly increasing with an intensity that generates hyperventilation; this being related to the anaerobic threshold.
- Duration range. The exercise duration of sessions, which is increased from initial sessions in an interval of (15–20) min to an interval of (30–40) min for trained patients [35].
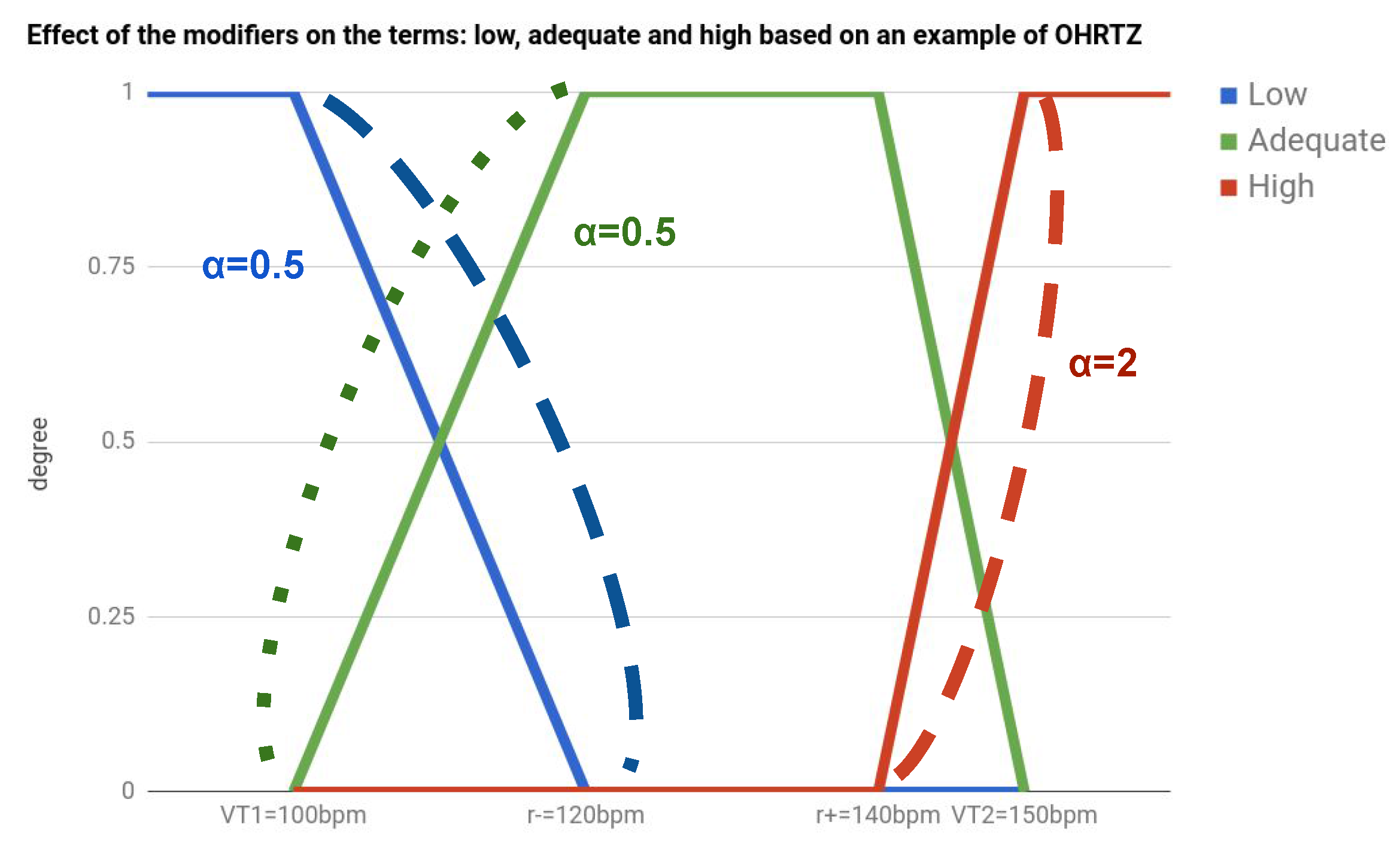
- The optimal heart rate training zones (OHRTZs). These are defined by the clinical protocol in each session, as percentage ranges from and . The methodology of Marvonen [33] allows translating the percentage range to absolute bpm that is defined by .The middle point between is known as target heart rate , which is related to the ideal heart rate to maintain in the session.
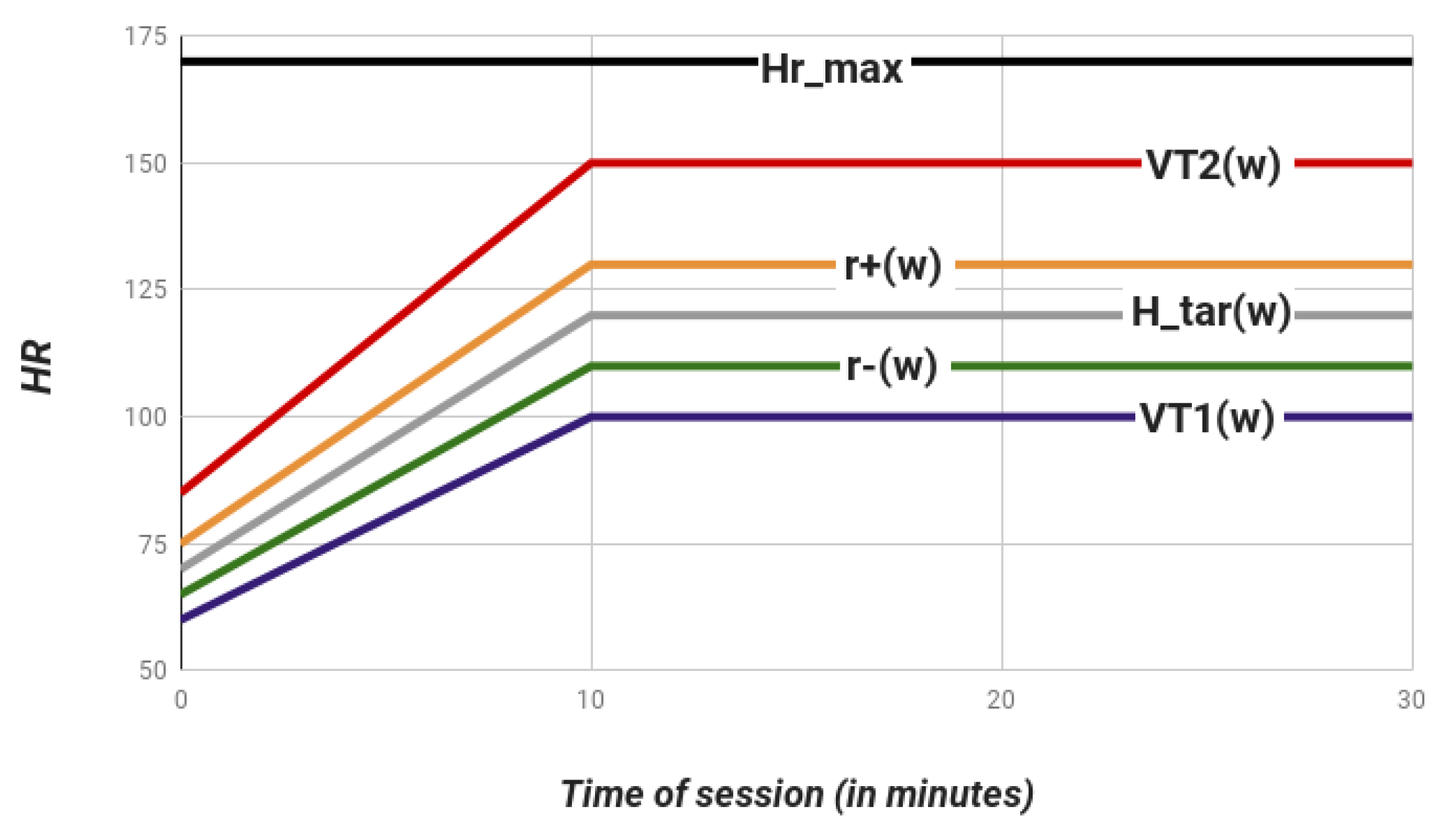
- Duration of the progressive stage (). The progression of HR within from basal state needs for a lineal increase, which starts from the resting point until reaching the OHRTZ. The duration of this progressive stage is defined in minutes.
2.2. A Fuzzy Model for Real-Time Monitoring and Evaluation of Cardiac Rehabilitation Sessions
2.2.1. Fuzzification of Heart Rate Measures by Optimal Heart Rate Training Zones
2.2.2. Fuzzy Transformation from the Progressive to Maintenance Stage
- Basal ranges in bmp, where the HRs of patient are adequate in order to start the session.
- Lower basal threshold in bmp . This represents a minimal value of HR not recommended before starting the session.
- Upper basal threshold in bmp . This represents a maximal value of HR not recommended before starting the session.
2.2.3. Fuzzy Temporal Aggregation of the Heart Rate Stream
2.2.4. Evaluating the Cardiac Rehabilitation Sessions
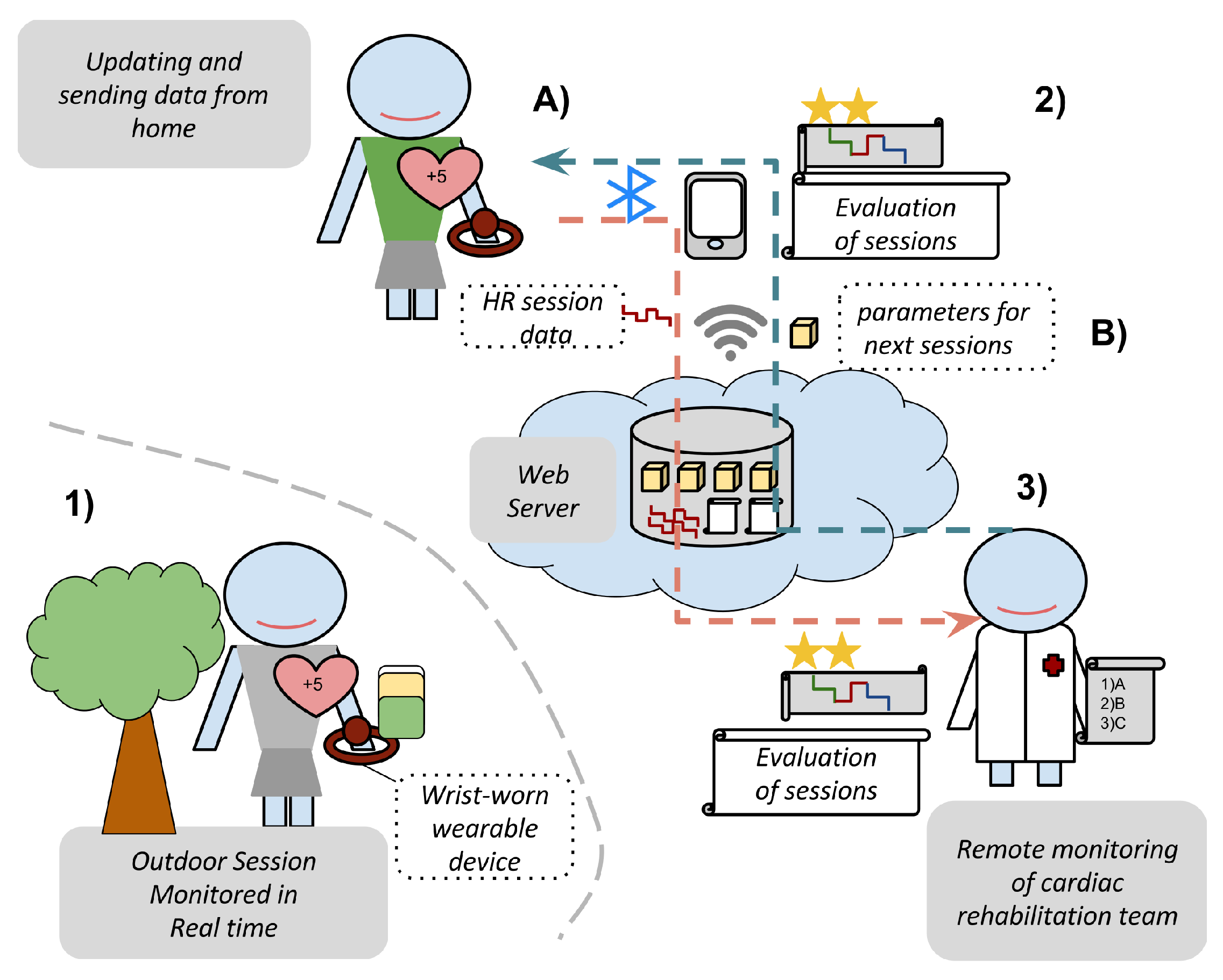
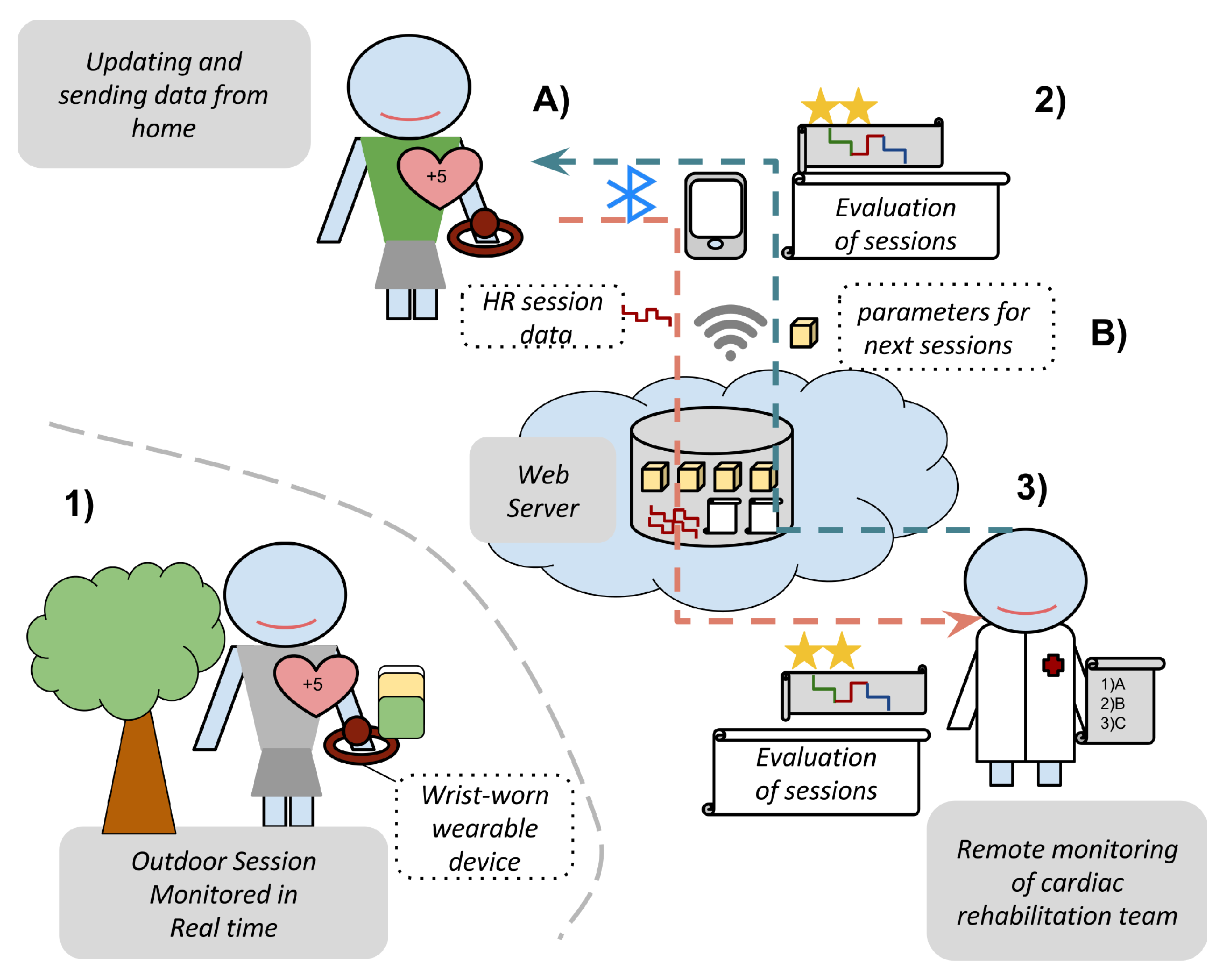
3. Development as a Wearable Mobile Cloud Platform
- A cloud web application for the cardiac rehabilitation team. Requiring previous authentication through login credentials, this includes the next use cases:
- -
- Registration and updating of patient data, including the thresholds for CRP: maximal heart rate , ventilatory thresholds , basal ranges and basal limits .
- -
- Creation and modification of the parameters of the sessions in the rehabilitation programs. They are: optimal heart rate training zones , duration range , and duration of progressive stage .
- -
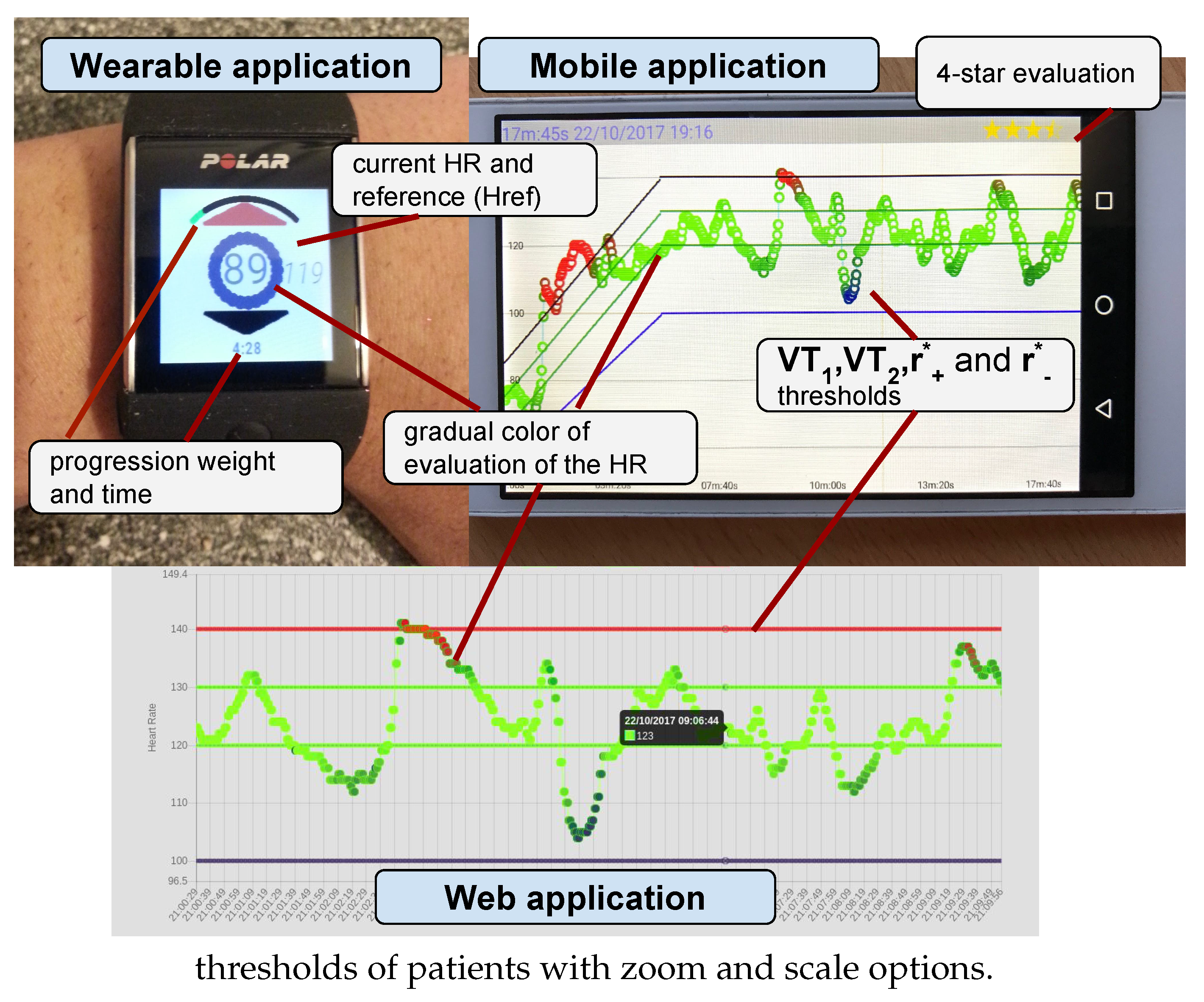
- Showing the CRSs from patients. The sessions developed by patients are synchronized from the mobile application to the web server. From them, the cardiac rehabilitation team can observe: (1) the raw data from the HR of the session in a timeline (with an option to zoom and scale); (2) the real-time monitoring provided for the patient using gradual colors: blue, green, red based on the degree of the terms , respectively; and (3) a summarized indicator which evaluates the session using a 4-star scale.
- A mobile application for patients in order to show the sessions and communicate the data between the web server and the wearable devices. It has been developed for Android and included the next use cases:
- -
- Synchronization of the parameters of the next sessions from the CRP, which are defined by the cardiac rehabilitation team and are collected in the web server, in the mobile device using a web service under wireless network technology (3G/4G or WiFi).
- -
- Synchronization of the session data from the wrist-worn wearable device into the mobile device using an ad-hoc Bluetooth connection.
- -
- Uploading of the session data from the mobile device into the web server using a web service under wireless network technology (3G/4G or WiFi).
- -
- Showing and evaluating the CRSs. In the same way as the cardiac rehabilitation team, patients can observe the following information in their mobile devices for each session: (1) the raw data from the HR of sessions in a timeline; (2) the real-time monitoring provided using gradually changing colors blue, green, red; and (3) a summarized indicator of the session using a 4-star scale.
- A wearable application for patient in order to develop the sessions with regard to the CRP. This has been developed for Android to include the next use cases:
- -
- Updating the the parameters of sessions from the mobile device into the wrist-worn wearable device using an ad-hoc Bluetooth connection.
- -
- Monitoring the session in the wearable device with regard to the CRP providing a real-time monitoring by means of showing (1) the current HR of the patient; (2) the target HR; (3) a graphical evaluation using gradually changing colors blue, green, red based on the degree of the terms respectively; and (4) the time of session and the graphical time progression in proportion to the proposed duration.
- -
- To synchronize the data of sessions, which contains the monitoring and raw HR, from the wrist-worn wearable device into the mobile device using an ad hoc Bluetooth connection.
4. Results
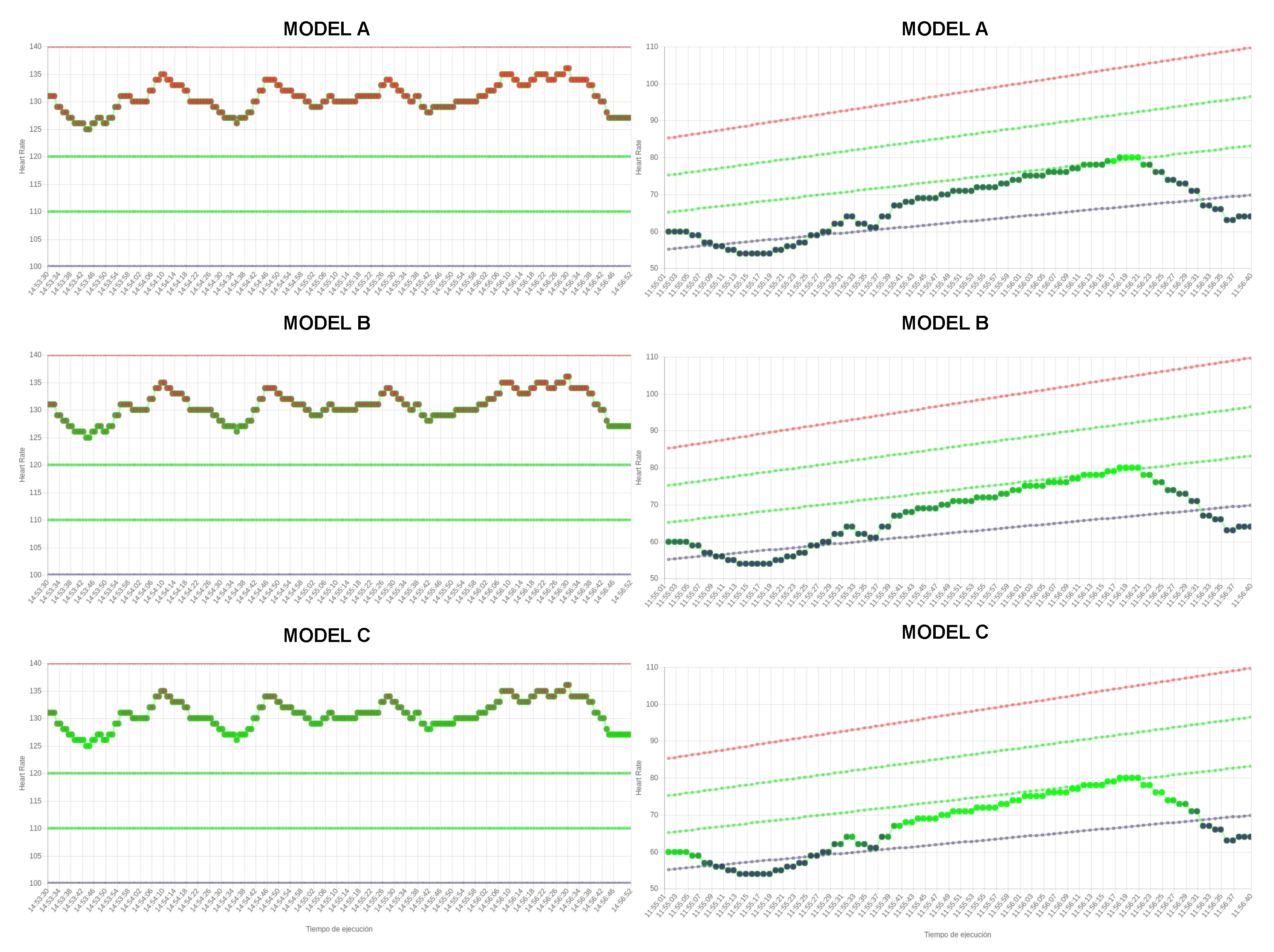
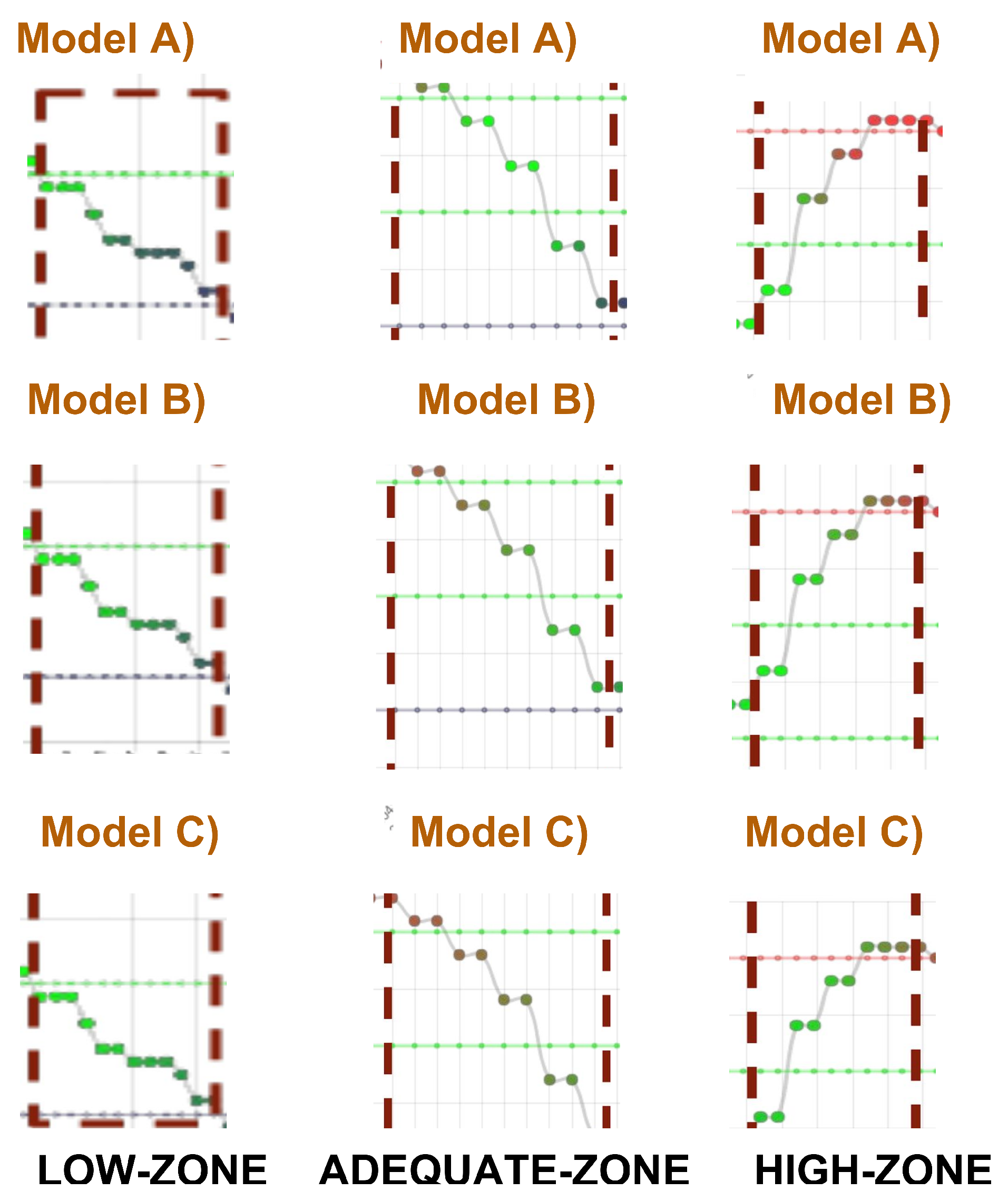
4.1. Impact of Modifiers over Linguistic Terms
4.2. Impact of Temporal Window over Linguistic Terms
4.3. Discussion
5. Conclusions and Future Work
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CR | Cardiac Rehabilitation |
| CRU | Cardiac Rehabilitation Units |
| CRP | Cardiac Rehabilitation Program |
| CRS | Cardiac Rehabilitation Sessions |
| ECG | Electrocardiogram |
| VT1 | First Ventilatory Threshold |
| VT2 | Second Ventilatory Threshold |
| HR | Heart Rate |
| bpm | Number of contractions of the heart per minute |
| OHRTZ | Optimal Heart Rate Training Zone |
References
- Butte, N.F.; Ekelund, U.; Westerterp, K.R. Assessing physical activity using wearable monitors: Measures of physical activity. Med. Sci. Sports Exerc. 2012, 44 (Suppl. S1), S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Espinilla, M.; Liu, J.; Garcia-Chamizo, J.M. Recent Advancements in Ubiquitous Computing. J. Ambient Intell. Humaniz. Comput. 2017, 8, 467–468. [Google Scholar] [CrossRef]
- Gouaux, F.; Simon-Chautemps, L.; Fayn, J.; Adami, S.; Arzi, M.; Assanelli, D.; Forlini, M.C.; Malossi, C.; Martinez, A.; Placide, J.; et al. Ambient intelligence and pervasive systems for the monitoring of citizens at cardiac risk: New solutions from the EPI-MEDICS project. In Proceedings of the IEEE Computers in Cardiology, Memphis, TN, USA, 22–25 September 2002; pp. 289–292. [Google Scholar]
- Case, M.A.; Burwick, H.A.; Volpp, K.G.; Patel, M.S. Accuracy of smartphone applications and wearable devices for tracking physical activity data. JAMA 2015, 313, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Krupinski, E.A.; Bernard, J. Standards and guidelines in telemedicine and telehealth. Healthcare 2014, 2, 74–93. [Google Scholar] [CrossRef] [PubMed]
- Chiauzzi, E.; Rodarte, C.; DasMahapatra, P. Patient-centered activity monitoring in the self-management of chronic health conditions. BMC Med. 2015, 13, 77. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Medina, J.; Martinez, L.; Espinilla, M. Subscribing to fuzzy temporal aggregation of heterogeneous sensor streams in real—Time distributed environments. Int. J. Commun. Syst. 2017, 30. [Google Scholar] [CrossRef]
- Medina, J.; Espinilla, M.; Garcia-Fernandez, A.L.; Martinez, L. Intelligent multi-dose medication controller for fever: From wearable devices to remote dispensers. Comput. Electr. Eng. 2017, in press. [Google Scholar] [CrossRef]
- Espinilla, M.; Medina, J.; Garcia-Fernandez, Á.L.; Campaña, S.; Londoño, J. Fuzzy Intelligent System for Patients with Preeclampsia in Wearable Devices. Mob. Inf. Syst. 2017, 2017, 7838464. [Google Scholar] [CrossRef]
- Shewell, C.; Medina, J.; Espinilla, M.; Nugent, C.; Donnelly, M.; Wang, H. Comparison of Fiducial Marker Detection and Object Interaction in Activities of Daily Living Utilising a Wearable Vision Sensor. Int. J. Commun. Syst. 2017, 30. [Google Scholar] [CrossRef]
- Espinilla, M.; Nugent, C. Computational Intelligence for Smart Environments. Int. J. Comput. Intell. Syst. 2017, 10, 1250–1251. [Google Scholar] [CrossRef]
- Oliveira, C.C.; Dias, R.; da Silva, J.M. A Fuzzy Logic Approach for a Wearable Cardiovascular and Aortic Monitoring System. In ICT Innovations 2015; Springer: Cham, Switzerland, 2016; pp. 265–274. [Google Scholar]
- World Health Organization. Needs and Action Priorities in Cardiac Rehabilitation and Secondary Prevention in Patients with Coronary Heart Disease; WHO Regional Office for Europe: Geneva, Switzerland, 1993; Volume 6. [Google Scholar]
- Baig, M.M.; Gholamhosseini, H. Smart health monitoring systems: An overview of design and modeling. J. Med. Syst. 2013, 37, 9898. [Google Scholar] [CrossRef] [PubMed]
- De la Cuerda, R.C.; Diego, I.M.A.; Martín, J.J.A.; Sánchez, A.M.; Page, J.C.M. Cardiac rehabilitation programs and health-related quality of life. State of the art. Rev. Esp. Cardiol. (Engl. Ed.) 2012, 65, 72–79. [Google Scholar] [CrossRef]
- Grima-Serrano, A.; García-Porrero, E.; Luengo-Fernández, E.; León, L.M. Preventive cardiology and cardiac rehabilitation. Rev. Esp. Cardiol. 2011, 64, 66–72. [Google Scholar] [CrossRef]
- Balady, G.J.; Ades, P.A.; Bittner, V.A.; Franklin, B.A.; Gordon, N.F.; Thomas, R.J.; Tomaselli, G.F.; Yancy, C.W. Association Science Advisory and Coordinating Committee. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centers and beyond. Circulation 2011, 124, 2951–2960. [Google Scholar] [CrossRef] [PubMed]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 7, CD001800. [Google Scholar]
- Yue, C.S.S. Barriers to participation in a phase II cardiac rehabilitation programme. Hong Kong Med. J. 2005, 11, 472–475. [Google Scholar]
- Daly, J.; Sindone, A.P.; Thompson, D.R.; Hancock, K.; Chang, E.; Davidson, P. Barriers to participation in and adherence to cardiac rehabilitation programs: A critical literature review. Prog. Cardiovasc. Nurs. 2002, 17, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Dalal, H.; Jolly, K.; Zawada, A.; Dean, S.G.; Cowie, A.; Norton, R.J. Home—Based versus Centre—Based Cardiac Rehabilitation; The Cochrane Library: London, UK, 2015. [Google Scholar]
- Taylor, R.S.; Dalal, H.; Jolly, K.; Moxham, T.; Zawada, A. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst. Rev. 2010, 1, CD007130. [Google Scholar]
- Kraal, J.J.; Peek, N.; van den Akker-Van, M.E.; Kemps, H.M. Effects and costs of home-based training with telemonitoring guidance in low to moderate risk patients entering cardiac rehabilitation: The FITA Home study. BMC Cardiovasc. Disord. 2013, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- Worringham, C.; Rojek, A.; Stewart, I. Development and feasibility of a smartphone, ECG and GPS based system for remotely monitoring exercise in cardiac rehabilitation. PLoS ONE 2011, 6, e14669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, G.; Custodio, V.; Moreno, J.I. LOBIN: E-textile and wireless-sensor-network-based platform for healthcare monitoring in future hospital environments. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1446–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawstorn, J.C.; Gant, N.; Meads, A.; Warren, I.; Maddison, R. Remotely delivered exercise-based cardiac rehabilitation: Design and content development of a novel mHealth platform. JMIR mHealth uHealth 2016, 4, e57. [Google Scholar] [CrossRef] [PubMed]
- Kitsiou, S.; Thomas, M.; Marai, G.E.; Maglaveras, N.; Kondos, G.; Arena, R.; Gerber, B. Development of an innovative mHealth platform for remote physical activity monitoring and health coaching of cardiac rehabilitation patients. In Proceedings of the 2017 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Orlando, FL, USA, 16–19 February 2017; pp. 133–136. [Google Scholar]
- Lee, E.S.; Lee, J.S.; Joo, M.C.; Kim, J.H.; Noh, S.E. Accuracy of Heart Rate Measurement Using Smartphones During Treadmill Exercise in Male Patients with Ischemic Heart Disease. Ann. Rehabil. Med. 2017, 41, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Shcherbina, A.; Mattsson, C.M.; Waggott, D.; Salisbury, H.; Christle, J.W.; Hastie, T.; Wheeler, M.T.; Ashley, E.A. Accuracy in wrist-worn, sensor-based measurements of heart rate and energy expenditure in a diverse cohort. J. Personalized Med. 2017, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Rawassizadeh, R.; Price, B.A.; Petre, M. Wearables: Has the age of smartwatches finally arrived? Commun. ACM 2015, 58, 45–47. [Google Scholar] [CrossRef]
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Anari, L.M.; Ghanbari-Firoozabadi, M.; Ansari, Z.; Emami, M.; Nasab, M.V.; Nemaiande, M.; Boostany, F.; Neishaboury, M. Effect of cardiac rehabilitation program on heart rate recovery in coronary heart disease. J. Tehran Univ. Heart Cent. 2015, 10, 176–181. [Google Scholar]
- Holldobler, S.; Khang, T.D.; Storr, H.P. A fuzzy description logic with hedges as concept modifiers. In Proceedings of the Third International Conference on Intelligent Technologies and Third Vietnam-Japan Symposium on Fuzzy Systems and Applications (InTech/VJFuzzy), Hanoi, Vietnam, 3–5 December 2002; pp. 25–34. [Google Scholar]
- Kerre, E.E.; De Cock, M. Linguistic modifiers: An overview. Fuzzy Log. Soft Comput. 1999, 9, 69–85. [Google Scholar]
- Baños, O.; Galvez, J.M.; Damas, M.; Pomares, H.; Rojas, I. Window size impact in human activity recognition. Sensors 2014, 14, 6474–6499. [Google Scholar] [CrossRef] [PubMed]
- Medina, J.; Espinilla, M.; Nugent, C. Real-time fuzzy linguistic analysis of anomalies from medical monitoring devices on data streams. In Proceedings of the 10th EAI International Conference on Pervasive Computing Technologies for Healthcare, Cancun, Mexico, 16–19 May 2016; ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering): Brussels, Belgium, 2016; pp. 300–303. [Google Scholar]
- Dong, W.M.; Wong, F.S. Fuzzy weighted averages and implementation of the extension principle. Fuzzy Sets Syst. 1987, 21, 183–199. [Google Scholar] [CrossRef]
- Paez, D.G.; de Buenaga Rodríguez, M.; Sánz, E.P.; Villalba, M.T.; Gil, R.M. Big data processing using wearable devices for wellbeing and healthy activities promotion. In Proceedings of the International Workshop on Ambient Assisted Living, Puerto Varas, Chile, 1–4 December 2015; Springer: Cham, Switzerland, 2015; pp. 196–205. [Google Scholar]
- Meier, R. Professional Android 4 Application Development; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Horton, J.F.; Stergiou, P.; Fung, T.S.; Katz, L. Comparison of Polar M600 Optical Heart Rate and Ecg Heart Rate during Exercise. Med. Sci. Sports Exerc. 2017, 49, 2600–2607. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.L.; Owen, H.; Reynolds, K.J. Heart rate variability indices for very short-term (30 beat) analysis. Part 2: Validation. J. Clin. Monit. Comput. 2013, 27, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Avila, A.; Goetschalckx, K.; Vanhees, L.; Cornelissen, V. A randomized controlled study comparing home-based training with telemonitoring guidance versus center-based training in patients with coronary heart disease: Rationale and design of the tele-rehabilitation in coronary heart disease (TRiCH) Study. J. Clin. Trials 2014, 4, 1–5. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Survey | Model | Modifiers | Value −2 | Value −1 | Value 0 | Value +1 | Value +2 |
|---|---|---|---|---|---|---|---|
| High values | severe | 0 | 0.2 | 0.6 | 0.2 | 0 | |
| neutral | 0 | 0 | 0.2 | 0.5 | 0.3 | ||
| yielding | 0.3 | 0.4 | 0.3 | 0.0 | 0 | ||
| Low values | severe | 0 | 0.3 | 0.3 | 0.3 | 0.1 | |
| neutral | 0 | 0 | 0.2 | 0.4 | 0.4 | ||
| yielding | 0 | 0.4 | 0.5 | 0.1 | 0 |
| Term | Model | Value −2 | Value −1 | Value 0 | Value +1 | Value +2 |
|---|---|---|---|---|---|---|
| High | 0 | 0 | 0.3 | 0.3 | 0.4 | |
| 0 | 0 | 0.3 | 0.4 | 0.3 | ||
| 0.3 | 0.4 | 0.3 | 0 | 0 | ||
| Adequate | 0 | 0 | 0.3 | 0.4 | 0.3 | |
| 0 | 0 | 0.2 | 0.2 | 0.6 | ||
| 0 | 0.2 | 0.4 | 0.4 | 0 | ||
| Low | 0 | 0 | 0.3 | 0.4 | 3.0 | |
| 0 | 0 | 0.3 | 0.3 | 0.4 | ||
| 0 | 0 | 0.3 | 0.4 | 3.0 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medina Quero, J.; Fernández Olmo, M.R.; Peláez Aguilera, M.D.; Espinilla Estévez, M. Real-Time Monitoring in Home-Based Cardiac Rehabilitation Using Wrist-Worn Heart Rate Devices. Sensors 2017, 17, 2892. https://doi.org/10.3390/s17122892
Medina Quero J, Fernández Olmo MR, Peláez Aguilera MD, Espinilla Estévez M. Real-Time Monitoring in Home-Based Cardiac Rehabilitation Using Wrist-Worn Heart Rate Devices. Sensors. 2017; 17(12):2892. https://doi.org/10.3390/s17122892
Chicago/Turabian StyleMedina Quero, Javier, María Rosa Fernández Olmo, María Dolores Peláez Aguilera, and Macarena Espinilla Estévez. 2017. "Real-Time Monitoring in Home-Based Cardiac Rehabilitation Using Wrist-Worn Heart Rate Devices" Sensors 17, no. 12: 2892. https://doi.org/10.3390/s17122892