
Parametric Cognitive Modeling of Information and Computer Technology Usage by People with Aging- and Disability-Derived Functional Impairments

 ,
,  and
and 
Abstract
:1. Introduction
1.1. User Modeling
1.2. VERITAS Project Overview
- VIDEO SENSING: a motion detection system based on three cameras positioned all around the subject.
- WEARABLE: constituted by a set of systems that can be used to collect data from about movements of several body parts of body or joints, such as: gloves, knee electro-goniometers and accelerometers.
- MOTION TRAKING: using commercial stereoscopic cameras to analyze gait activity, identify specific irregular walking patterns and to extract parameters like height, step and stride length and width, step asymmetries, cadence, body oscillation (width shift) during gait as well as hip, knee and hand range of motion.
- ENVIRONMENTAL SENSORS: to capture and analyze user interaction with objects and interfaces in order to complement the vision given by the wearable sensors and cameras system.
2. Study Design and Methodology
2.1. Study Description
2.2. Methodology
- -
- Identify which are the cognitive functions and their corresponding parameters (e.g., reaction time, perception, attention, working memory, etc.) that are relevant to each type of cognitive impairment of interest: elderly people, Alzheimer’s disease patients, Parkinson’s disease patients, and people with visual, hearing and speech impairments.
- -
- Analyze and characterize specific target users’ needs.
- -
- Define the recommendations, guidelines and values that will support the designers and developers’ decisions during the designing process of new ICT health products and services.
- -
- Evaluate the final parameterized cognitive user models by simulating them in a real application.
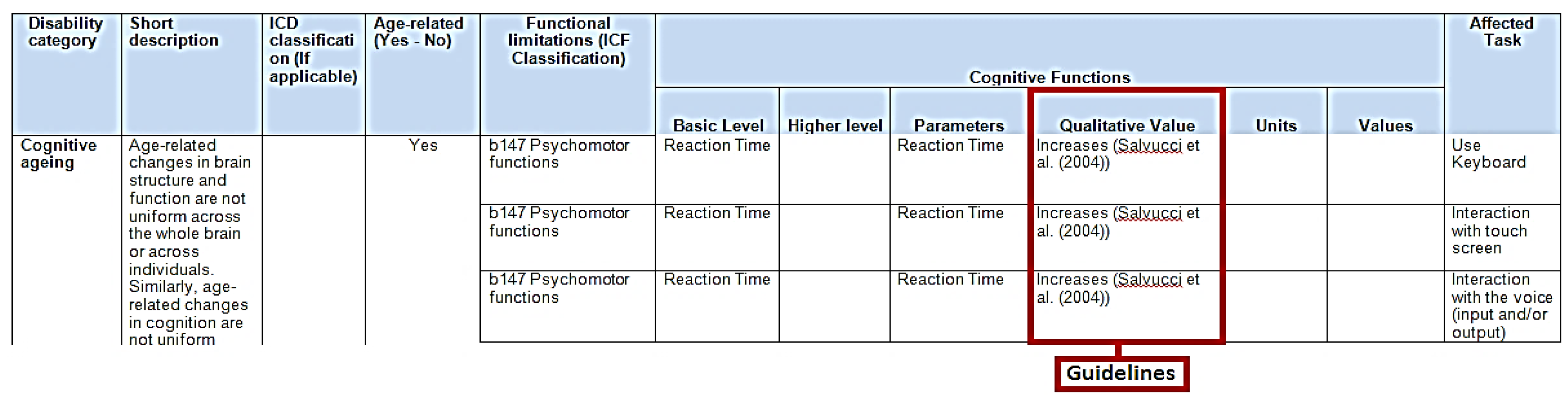
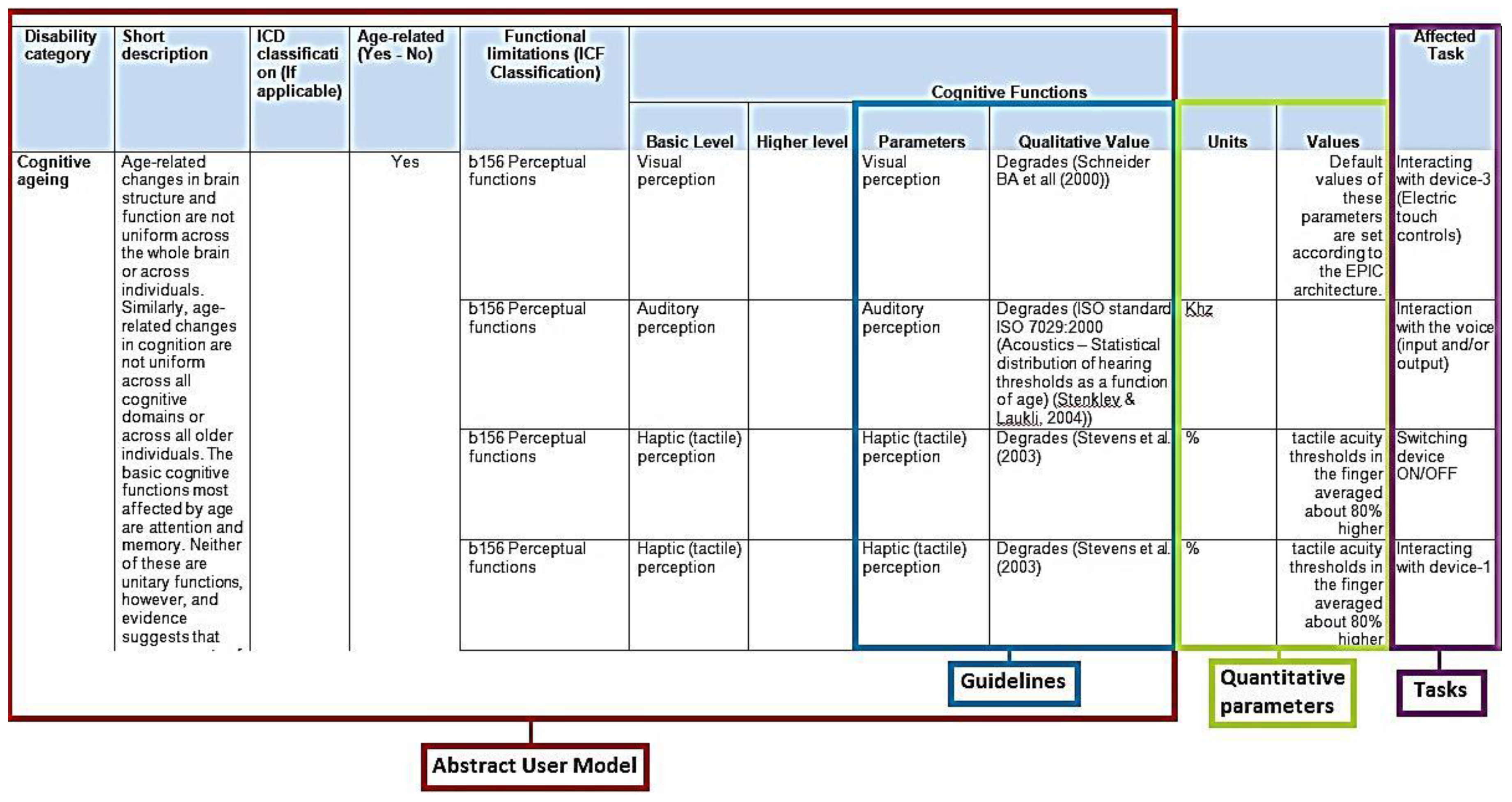
- Generation of an Abstract User Model (AUM), based on the analysis of existing models, medical studies, guidelines, real user measurements, methodologies and existing practices, user needs, as well as known accessibility guidelines and standards. The Cognitive AUM represents the different facets of each disability or cognitive state.
- Mapping between the defined parameters and the affected ACT-R framework modules.
- Task Models implementation to represent users while performing specific tasks and interactions.
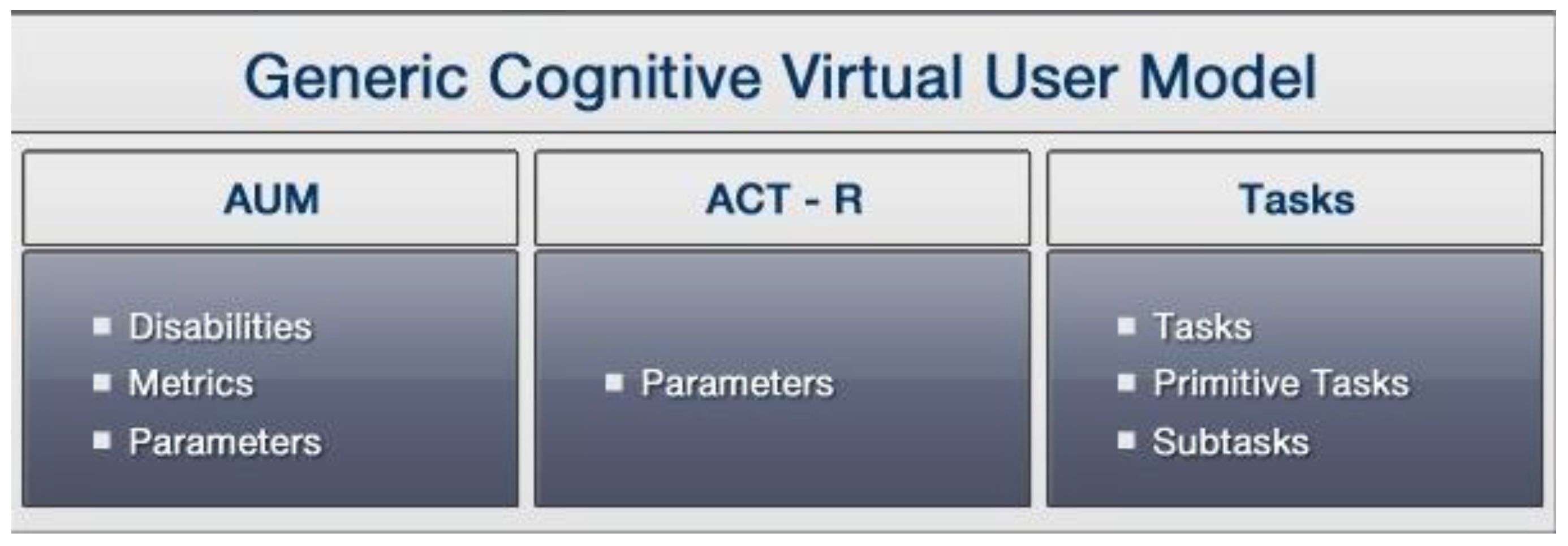
- Generic Cognitive Virtual User Model (GCVUM) generation, by merging the cognitive AUM with the affected tasks per disability/cognitive state.
- Cognitive Virtual User Model generation, by instantiating the GCVUM.
- Simulation and evaluation of the final parameterized Cognitive Virtual User Models on a real remote health monitoring application.
2.2.1. Cognitive Abstract User Modeling
2.2.2. ACT-R User Model Structure
2.2.3. Affected Task Analysis
2.2.4. Generic Cognitive Virtual User Model
2.2.5. Evaluation Methodology of the Parameterized Cognitive Virtual User Model
- -
- People who are healthy and, in most cases, can still lead busy and active lives, but who have just started to experience slight deteriorations in their quality of life due to ageing.
- -
- People who are healthy, but are more likely to experience mild cognitive and physical problems due to ageing.
- -
- People who are very likely to experience cognitive and physical deteriorations due to ageing.
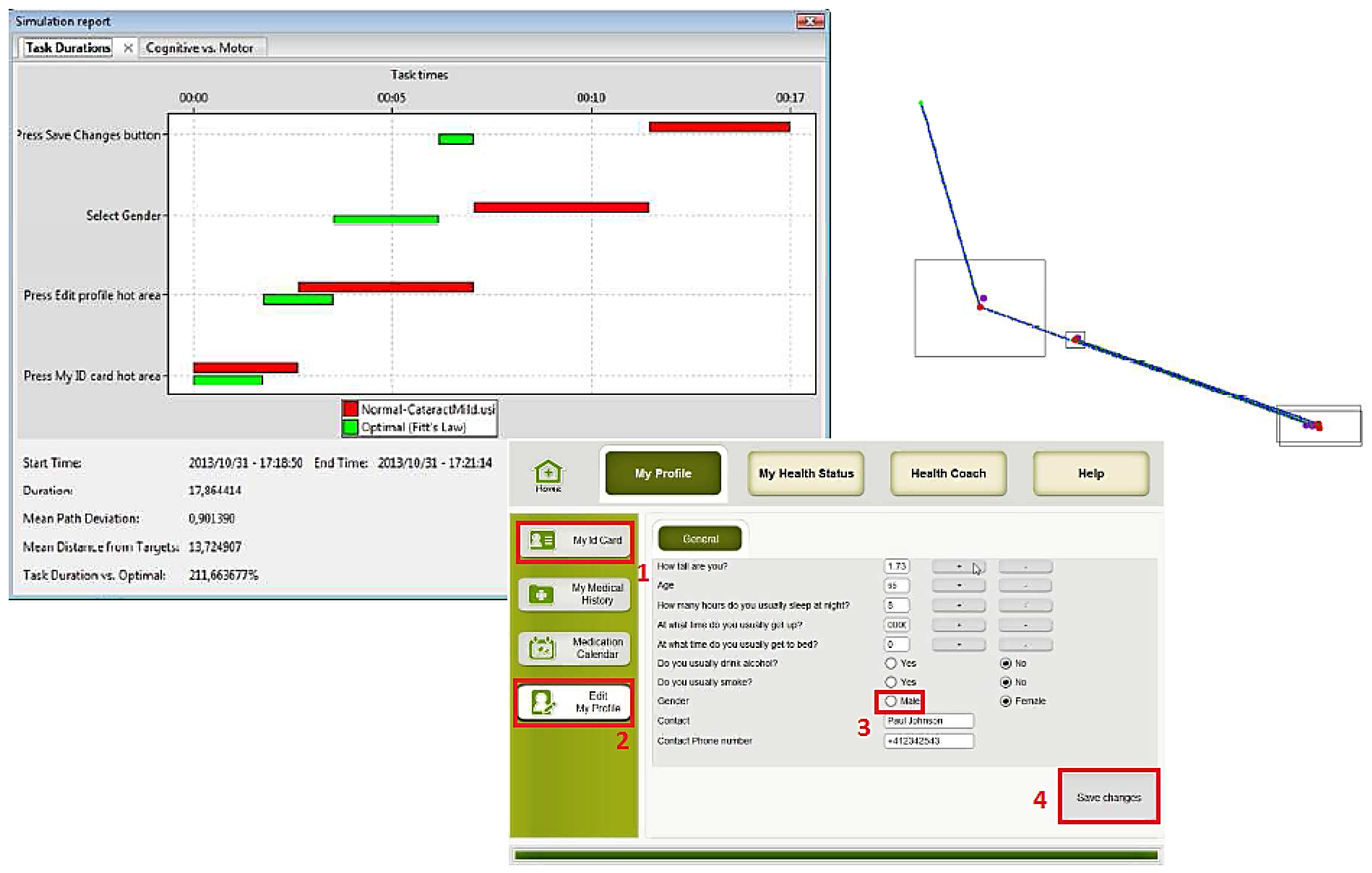
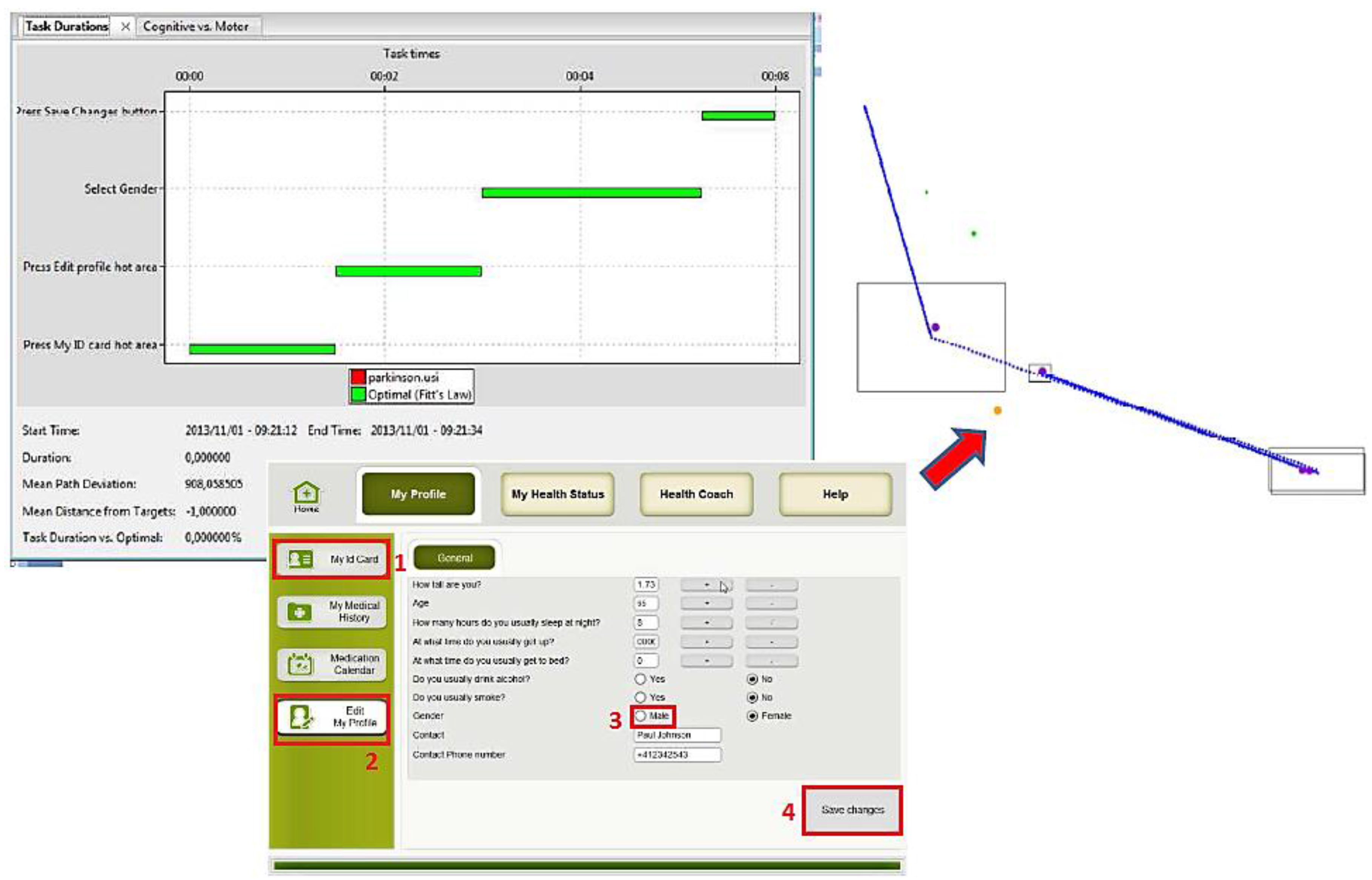
- Edit health profile: the user goes into “My ID card Menu”, selects “modify profile”, changes the “gender” (from male to female or vice versa), and “saves” the modification.
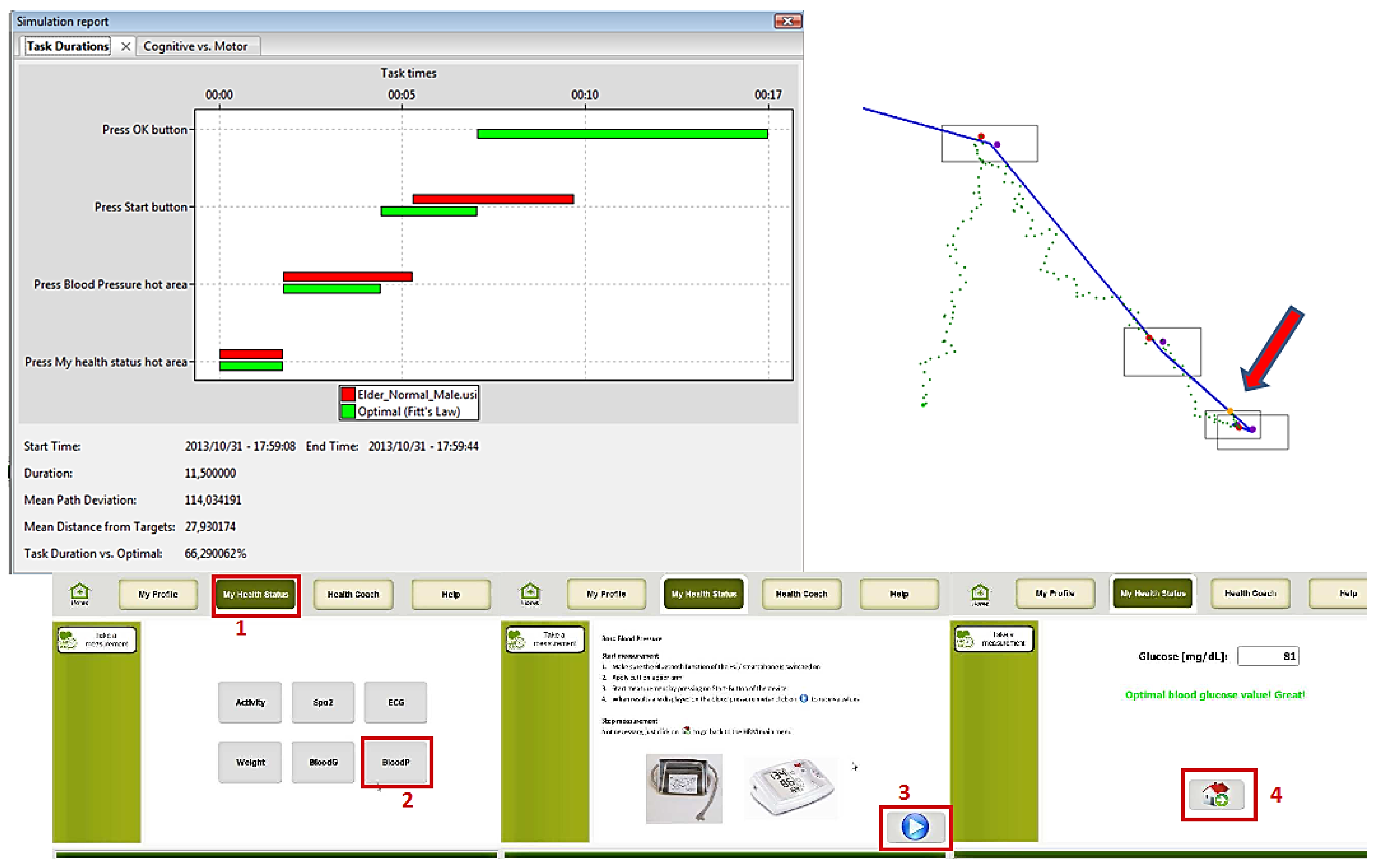
- Take measurement (blood pressure): the user goes to “My Health Status Menu”, selects “measure Blood pressure”, read the instructions to use the blood pressure sensor, “starts” the measurement and waits for the results.
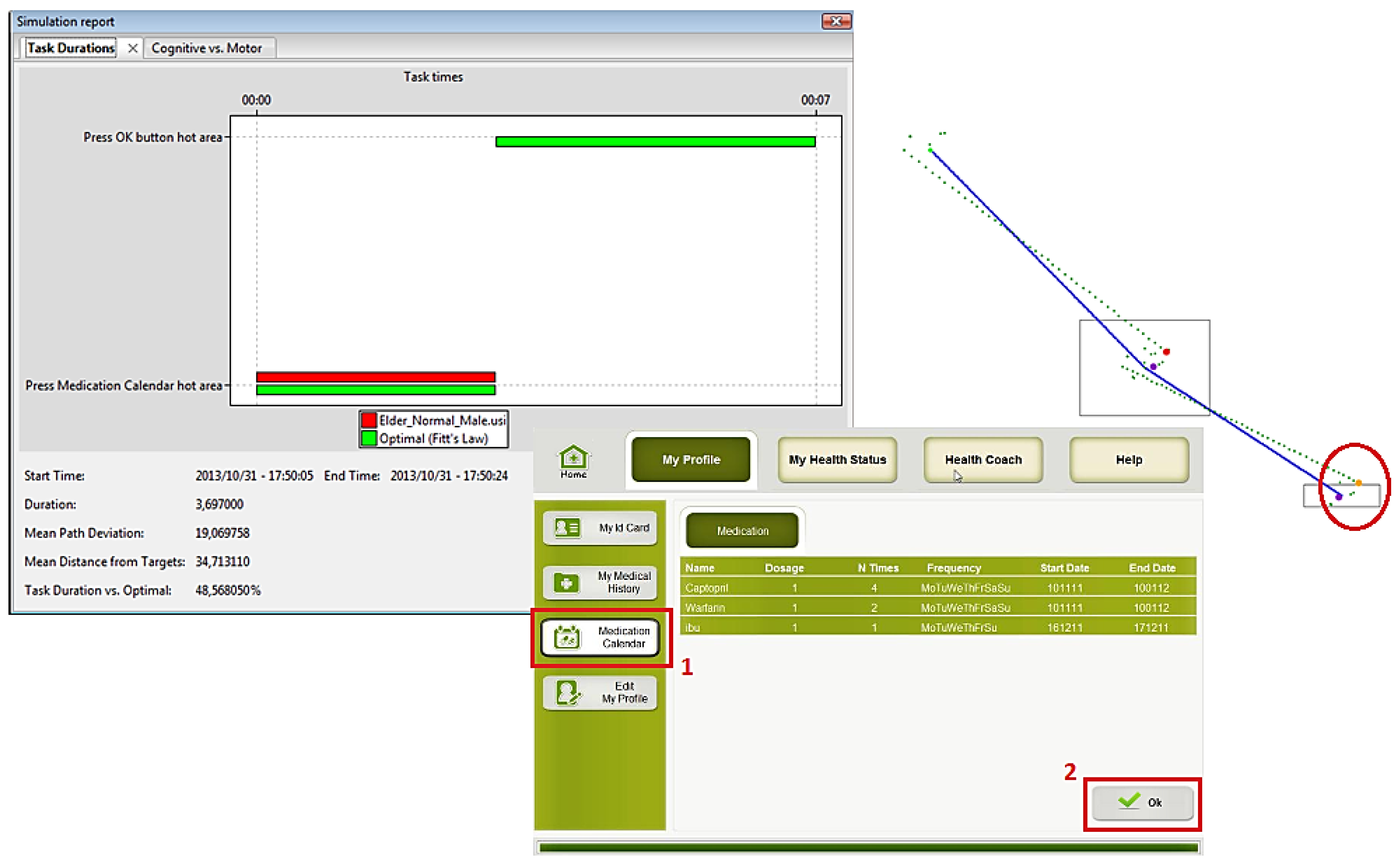
- Check Medication Calendar: the user selects the option “Medication Calendar” from the main screen, reads the information about the schedules and dosage of each medication, and presses “ok”.
3. Framework Results
3.1. Cognitive Abstract User Modeling Representation
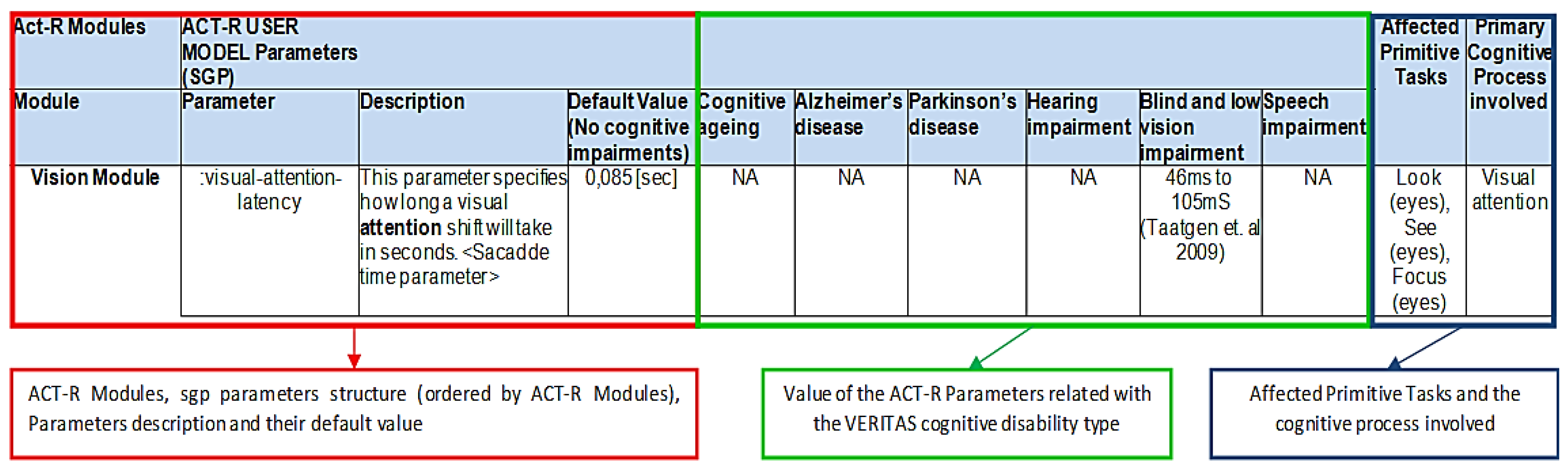
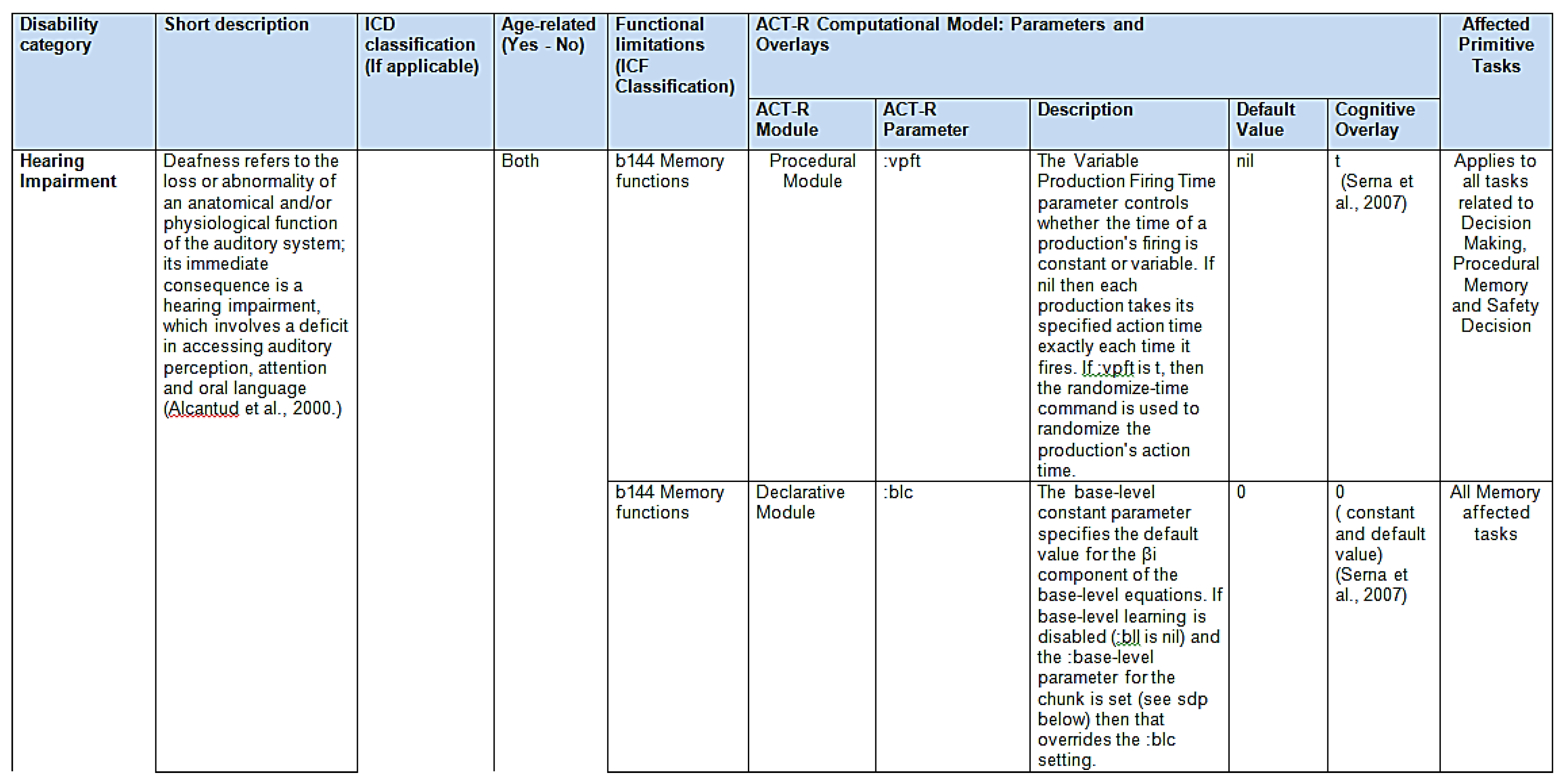
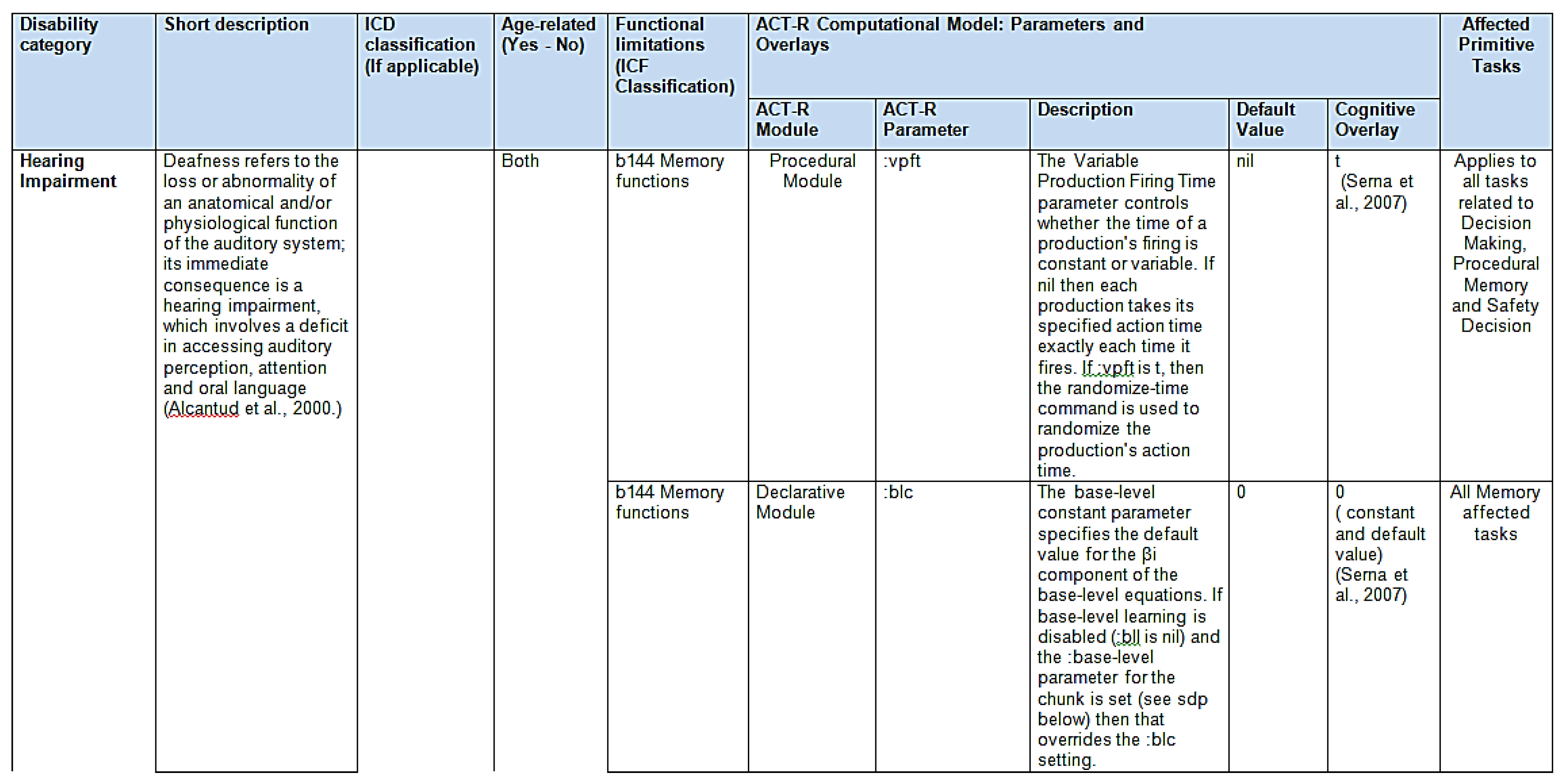
3.2. ACT-R Cognitive Parameters and Modules
- -
- Vision Module: primitive tasks: look (eyes), see (eyes), and focus (eyes); cognitive process: visual attention.
- -
- Audio Module: primitive tasks: listening (ears)/attention; cognitive process: aural attention.
- -
- Motor Module: primitive tasks: grasp, touch, reach, pull upwards, position, pull, hit and push (hands); cognitive process: procedural.
- -
- Speech Module: primitive tasks: speak (voice); cognitive process: speech.
- -
- Declarative Module: primitive tasks: memory; cognitive process: explicit memory.
- -
- Goal and Imaginal Modules: primitive tasks: those related to procedural memory; cognitive process: procedural memory.
- -
- Device Module: primary tasks: those related to the use of the mouse; cognitive process: visual attention.
- -
- Procedural, Utility and Production compilation Modules: primitive tasks: decision making, procedural memory and safety decision; cognitive process: procedural (implicit) memory.
- -
- The ACT-R module involved.
- -
- The ACT-R (sgp) parameters, description, default values, and specific values for each defined cognitive impairment (cognitive Ageing, Alzheimer’s disease, Parkinson’s disease, hearing impairment, blind and low vision impairment and speech impairment).
- -
- The affected primitive tasks per each ACT-R (sgp) parameter.
- -
- The primary cognitive process involved (e.g., visual attention, reaction time, etc.)
3.3. Task Model Implementation
3.4. Generic Cognitive Virtual User Model Representation
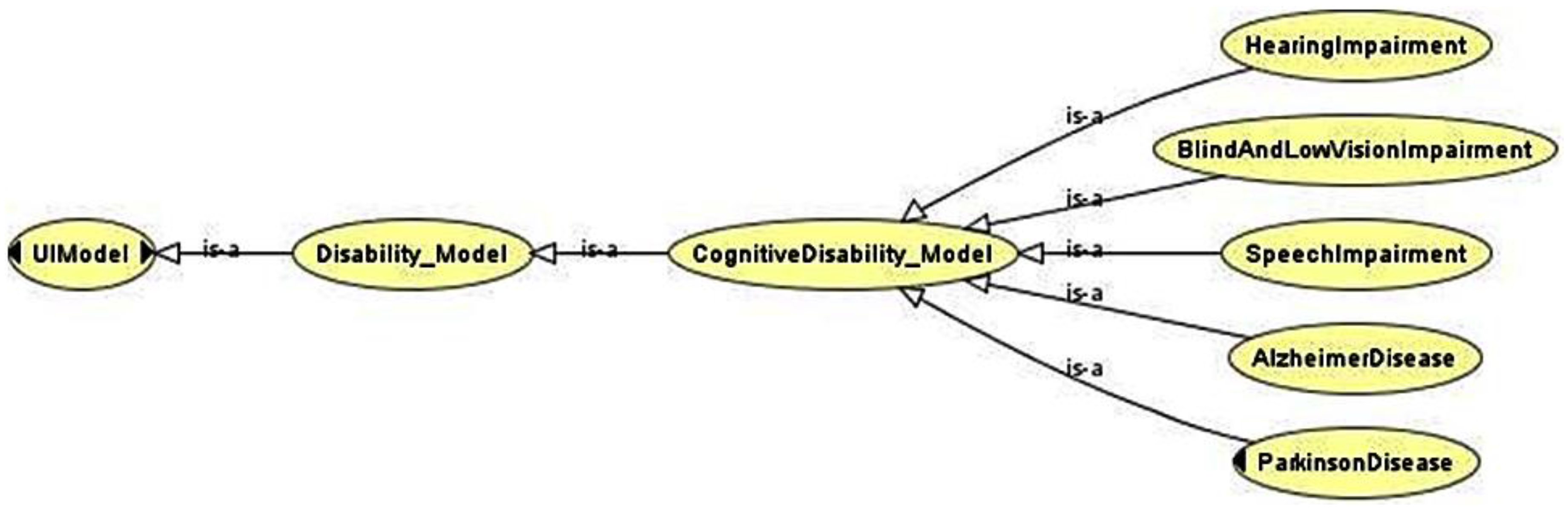
3.5. Representation of the GCVUM through Ontology
4. Evaluation through Simulation Results
Evaluation of the Parameterized Cognitive Virtual User Model Results
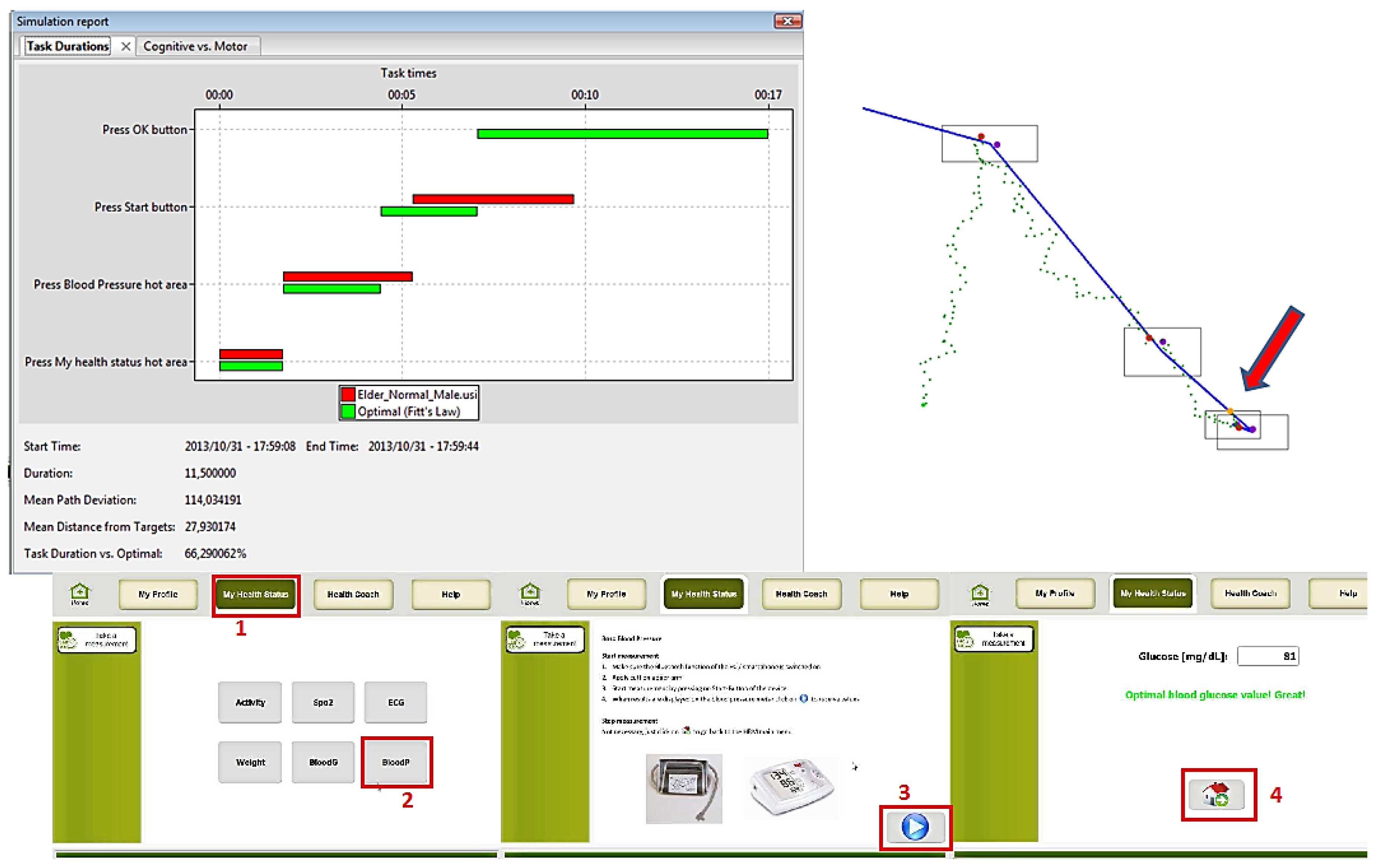
User 1: Elderly
User 2: Low Vision
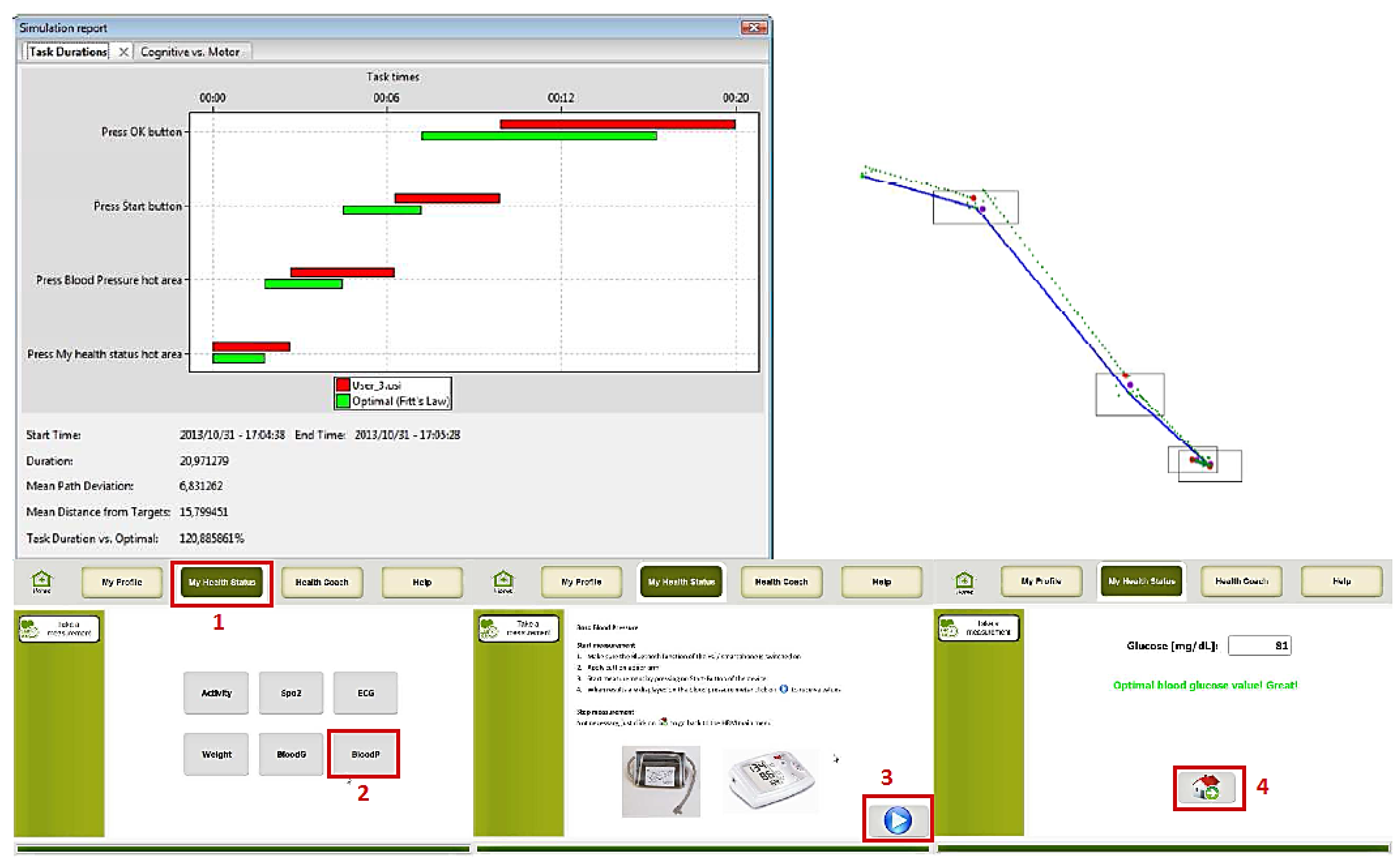
User 3: Motor Impairment
5. Discussion and Conclusions
Limitations and Future Work
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wagner, N.; Hassanein, K.; Head, M. Computer use by older adults: A multi-disciplinary review. Comput. Hum. Behav. 2010, 26, 870–882. [Google Scholar] [CrossRef]
- European Commission. Eurostat Regional Yearbook. 2013. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php/Online_publications (accessed on 25 June 2015).
- European Commission. Active Ageing and Solidarity between Generations: A Statistical Portrait of the European Union; European Union: Brussels, Belgium, 2011. [Google Scholar]
- Microsoft Corporation. The Wide Range of Abilities and Its Impact on Computer Technology; Forrester Research, Inc.: Cambridge, MA, USA, 2003. [Google Scholar]
- Daydé, A. Facts and Figures about Disability. European Disability Forum, 2013. Available online: http://www.edf-feph.org/Page_Generale.asp?DocID=12534 (accessed on 25 June 2015).
- Heart, T.; Kalderon, E. Older adults: Are they ready to adopt health-related ICT? Int. J. Med. Inform. 2013, 82, e209–e231. [Google Scholar] [CrossRef] [PubMed]
- Peissner, M.; Edlin-White, R. User Control in Adaptive User Interfaces for Accessibility. Hum. Comput. Interact. 2013, 8117, 623–640. [Google Scholar]
- Atkinson, M.T.; Li, Y.; Machin, C.; Sloan, D. Towards Accessible Interaction with Pervasive Interfaces, Based on Human Capabilities. Comput. Help. People Spec. Needs 2010, 6179, 162–169. [Google Scholar]
- United Nations. General Assembly “Convention on the Rights of Persons with Disabilities”. Available online: http://www.un.org/disabilities/convention/conventionfull.shtml (accessed on 15 May 2015).
- Eberle, P.; Schwarzinger, C.; Stary, C. User modelling and cognitive user support: Towards structured development. Univers. Access Inf. Soc. 2011, 10, 275–293. [Google Scholar] [CrossRef]
- LeRouge, C.; Ma, J.; Sneha, S.; Tolle, K. User profiles and personas in the design and development of consumer health technologies. Int. J. Med. Inform. 2013, 82, e251–e268. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.; Almeida, N.; Rosa, A.F.; Oliveira, A.; Casimiro, J.; Silva, S.; Teixeira, A. Elderly centered design for Interaction—The case of the S4S Medication Assistant. Proc. Comput. Sci. 2014, 27, 398–408. [Google Scholar] [CrossRef]
- Kurschl, W.; Augstein, M.; Burger, T.; Pointner, C. User modeling for people with special needs. Int. J. Pervasive Comput. Commun. 2014, 10, 313–336. [Google Scholar] [CrossRef]
- Alm, N.; Nakamura, K. Designing for ordinary and extraordinary users. ACM SIGCAPH Comput. Phys. Handicap. 2001. [Google Scholar] [CrossRef]
- Newell, A.F.; Gregor, P. Human computer interfaces for people with disabilities. In Handbook of Human-Computer Interaction; Helander, M.G., Landauer, T.K., Prabhu, P.V., Eds.; Elsevier Science: Amsterdam, The Netherlands, 1997; pp. 813–824. [Google Scholar]
- Gregor, P.; Newell, A.F.; Zajicek, M. Designing for dynamic diversity: Interfaces for older people. In Proceedings of the Fifth Annual ACM Conference on Assistive Technologies, Edinburgh, UK, 8–10 July 2002; ACM Press: New York, NY, USA, 2002; pp. 151–156. [Google Scholar]
- Fischer, G. User modeling in human-computer interaction. User Model. User-Adapt. Interact. 2001, 11, 65–86. [Google Scholar] [CrossRef]
- Adaptive Control of Thought-Rational (ACT-R) Cognitive Architecture. Available online: http://act-r.psy.cmu.edu/ (accessed on 20 September 2015).
- Budde, S.H.; Barkowsky, T. A framework for individual cognitive performance assessment in real-time for elderly users. In Proceedings of the AAAI Fall Symposium on AI in Eldercare: New Solutions to Old Problems, Chicago, IL, USA, 13–17 July 2008.
- Serna, A.; Pigot, H.; Rialle, V. Modeling the progression of Alzheimer’s disease for cognitive assistance in smart homes. User Model. User-Adapt. Interact. 2007, 17, 415–438. [Google Scholar] [CrossRef]
- Cooper, A. Inmates are Running the Asylum: Why High-tech Products Drive Us Crazy and How to Restore the Sanity; Sams: Indianapolis, IN, USA, 2004. [Google Scholar]
- Castillejo, E.; Almeida, A.; López-de-Ipiña, D. Modelling users, context and devices for adaptive user interface systems. Int. J. Pervasive Comput. Commun. 2014, 10, 69–91. [Google Scholar]
- Casas, R.; Marin, R.B.; Robinet, A.; Delgado, A.R.; Yarza, A.R.; McGinn, J.; Picking, R.; Grout, V. User modelling in ambient intelligence for elderly and disabled people. Comput. Help. People Spec. Needs 2008, 5105, 114–122. [Google Scholar]
- Aoyama, M. Persona-Scenario-Goal Methodology for User-Centered Requirements Engineering. In Proceedings of the 15th IEEE International Requirements Engineering Conference, Delhi, India, 15–19 October 2007; pp. 185–194.
- World Health Organization. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification to the Consequences of Disease. Published in Accordance with Resolution WHA29.35 of the 29th World Health Assembly. 1980. Available online: http://apps.who.int/iris/handle/10665/41003 (accessed on 15 May 2015).
- World Health Organization. International Classification of Functioning, Disability and Health (IFC). 2001. Available online: http://www.disabilitaincifre.it/documenti/ICF_18.pdf (accessed on 15 May 2015).
- Castillejo, E.; Almeida, A.; López-de-Ipiña, D.; Chen, L. Modeling users, context and devices for ambient assisted living environments. Sensors 2014, 14, 5354–5391. [Google Scholar] [CrossRef] [PubMed]
- Harte, R.P.; Glynn, L.G.; Broderick, B.J.; Rodriguez-Molinero, A.; Baker, P.M.; McGuiness, B.; O’Sullivan, L.; Diaz, M.; Quinlan, L.R.; Laighin, G.O. Human centered design considerations for connected health devices for the older adult. J. Pers. Med 2014, 4, 245–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubey, A.K.; Gualabani, K.; Mewara, H.S.; Trivedi, P. Challenges in Design & Deployment of Assistive Technology. In Proceedings of the International Conference on Signal Propagation and Computer Technology, Ajmer, India, 12–13 July 2014; pp. 466–469.
- VERITAS EU Project-247765. Available online: http://veritas-project.eu/ (accessed on 15 May 2015).
- Rugnonel, A.; Foresti, F.; Tamburini, E.; Forconi, T.; Arca, A.; Fico, G.; Diaz, C.; Navarro, A.M.; Chalkia, E.; Tsakiris, T. Simulation Models for the P. Healthcare Scenario, VERITAS EU Project. Available online: http://veritas-project.eu/deliverables/VERITAS_D2.6.1.pdf (accessed on 15 May 2015).
- Cassenti, D.N.; Kerick, S.E.; McDowell, K. Observing and modeling cognitive events through event-related potentials and ACT-R. Cogn. Syst. Res. 2011, 12, 56–65. [Google Scholar] [CrossRef]
- Ron, S. Theoretical status of computational cognitive modeling. Cogn. Syst. Res. 2009, 10, 124–140. [Google Scholar]
- Jie, C.; Hong, W. Vision navigation for driver cognitive model in ACT-R architecture. In Proceedings of the 9th IEEE International Conference on Cognitive Informatics (ICCI), Beijing, China, 7–9 July 2010; pp. 946–951.
- Anderson, J.R. How Can the Human Mind Occur in the Physical Universe? Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Kolodyazhniy, V.; Delahaye, M.; Valkova, M.G.; Van Isacker, K.; Lazarov, A.; Fernandez-Rodriguez, M.M.; Aguilar, T.; Zaragoza, R.; Navarro, A.; Naranjo, J.C.; Galán, H. Abstract Cognitive User Models Definition, VERITAS EU Project. Available online: http://veritas-project.eu/deliverables/ (accessed on 15 May 2015).
- Web Ontology Language (OWL) Ontologies. Available online: https://www.w3.org/standards/techs/owl#w3c_all (accessed on 15 June 2015).
- VERITAS Virtual User Model Repository. Available online: http://veritas-project.eu/VirtualUserModels.html (accessed on 15 May 2015).
- Jimenez-Mixco, V.; Cabrera-Umpierrez, M.F.; Arredondo, M.T.; Panou, A.M.; Struck, M.; Bonfiglio, S. Feasibility of a wireless health monitoring system for prevention and health assessment of elderly people. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 7306–7309.
- Tsakiris, A.; Moschonas, P.; Kaklanis, N.; Paliokas, I.; Stavropoulos, G.; Tzovaras, D. Cognitive impairments simulation in a holistic GUI accessibility assessment framework. In Assistive Technology: From Research to Practice, 33rd ed.; Encarnação, P., Azevedo, L., Gelderblom, G.J., Newell, A., Mathiassen, N.-E., Eds.; IOS Press: Amsterdam, The Netherlands, 2013; pp. 489–493. [Google Scholar]
- VERITAS Tools & Resource Finder. Available online: http://www.veritas-project.eu/toolfinder/index.html (accessed on 15 May 2015).
- Salvucci, D.D.; Chavez, A.K.; Lee, F.J. Modeling effects of age in complex tasks: A case study in driving. In Proceedings of the 26th Annual Conference of the Cognitive Science Society, Hillsdale, NJ, USA, 4–7 August 2004.
- Taatgen, N.A.; Anderson, J.R. The Past, Present, and Future of Cognitive Architectures. Top. Cogn. Sci. 2009, 2, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.A.; Daneman, M.; Murphy, D.R.; Kwong, S.S. Listening to discourse in distracting settings: The effects of aging. Psychol. Aging 2000, 15, 110–125. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.C.; Alvarez-Reeves, M.; Dipietro, L.; Mack, G.W.; Green, B.G. Decline of tactile acuity in aging: A study of body site, blood flow, and lifetime habits of smoking and physical activity. Somatosens. Motor Res. 2003, 20, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Stenklev, N.C.; Laukli, E. Presbyacusis-hearing thresholds and the ISO 7029. Int. J. Audiol. 2004, 43, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Alcantud, F.; Ferrer, A.; Romero, R. Analysis of computer access systems for physically disabled users. In Assistive Technologies Integration-Network (Rapport Final ATIN Projet Horizon); Applied Psychology Center: Brussels, Belgium, 2000; pp. 134–148. [Google Scholar]
- USer Interface eXtended Markup Language (UsiXML). Available online: http://www.usixml.org/en/home.html?IDC=221 (accessed on 15 May 2015).
- Serra, A.; Naranjo, J.C.; Navarro, A.M.; Chalkia, E. UIML/USIXML Task Modelling Definition. Available online: http://veritas-project.eu/wp-content/uploads/2011/02/VERITAS_D1.6.2_final_last.pdf (accessed on 15 May 2015).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User Type | User Name | Motor Disability | Vision Disability | Hearing Disability | Cognitive Disability |
|---|---|---|---|---|---|
| User 1: Elderly | Elder motor | Elder | Normal | Normal | Normal |
| User 2: Low vision | Cataract 50 | Normal | Cataract | Normal | Normal |
| Glaucoma 50 | Normal | Glaucoma | Normal | Normal | |
| User 3: Motor impairment | Parkinson 50 | Parkinson | Normal | Normal | Normal |
| Parkinson 90 |
| Basic Functions | Higher-Level Functions |
|---|---|
| Reaction Time | Decision Making |
| Measure of the overall cognitive performance speed. | Selection of a belief or a course of action among several alternative possibilities. |
| Attention | Orientation |
| Involved in virtually all cognitive tasks. Subdivided in: selective, divided, and sustained. | Awareness of three dimensions: time, place and being. |
| Memory | Speech and Language |
| Ability to store, retain, and recall information. Subdivided in: semantic, episodic, procedural, and working. | The faculty or act of expressing thoughts, feelings, or perceptions by the articulation of words. |
| Perception | Cognitive flexibility |
| Recognition and interpretation of sensory stimuli. Subdivided in: visual, auditory, and haptic. | Ability to switch attention from one aspect of an object to another. |
| Task | Subtasks | Primitive Tasks |
|---|---|---|
|
|
|
| Elder | Low Vision | Motor Impairment | |||||
|---|---|---|---|---|---|---|---|
| Elder Motor 50 | Elder Motor75 | Cataract 50 | Glaucoma 75 | Parkinson 50 | Parkinson 90 | ||
| Check Medication | Accuracy | 0,25 | 0 | 1 | 1 | 0 | 1 |
| Duration (sec.) | 34 | Failed | 154 | 57 | Failed | 45 | |
| N° events | 404 | Failed | 295 | 295 | Failed | 365 | |
| Take a measurement | Accuracy | 0 | 0 | 1 | 1 | 1 | 1 |
| Duration (sec.) | Failed | Failed | 212 | 78 | 62 | 68 | |
| N° events | Failed | Failed | 412 | 412 | 527 | 546 | |
| Edit profile | Accuracy | 0 | 0 | 1 | 1 | 0 | 0 |
| Duration (sec.) | Failed | Failed | 231 | 68 | Failed | Failed | |
| N° events | Failed | Failed | 343 | 343 | Failed | Failed | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Betances, R.I.; Cabrera-Umpiérrez, M.F.; Ottaviano, M.; Pastorino, M.; Arredondo, M.T. Parametric Cognitive Modeling of Information and Computer Technology Usage by People with Aging- and Disability-Derived Functional Impairments. Sensors 2016, 16, 266. https://doi.org/10.3390/s16020266
García-Betances RI, Cabrera-Umpiérrez MF, Ottaviano M, Pastorino M, Arredondo MT. Parametric Cognitive Modeling of Information and Computer Technology Usage by People with Aging- and Disability-Derived Functional Impairments. Sensors. 2016; 16(2):266. https://doi.org/10.3390/s16020266
Chicago/Turabian StyleGarcía-Betances, Rebeca I., María Fernanda Cabrera-Umpiérrez, Manuel Ottaviano, Matteo Pastorino, and María T. Arredondo. 2016. "Parametric Cognitive Modeling of Information and Computer Technology Usage by People with Aging- and Disability-Derived Functional Impairments" Sensors 16, no. 2: 266. https://doi.org/10.3390/s16020266
APA StyleGarcía-Betances, R. I., Cabrera-Umpiérrez, M. F., Ottaviano, M., Pastorino, M., & Arredondo, M. T. (2016). Parametric Cognitive Modeling of Information and Computer Technology Usage by People with Aging- and Disability-Derived Functional Impairments. Sensors, 16(2), 266. https://doi.org/10.3390/s16020266