
Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients †

 ,
, 
Abstract
:
1. Introduction
2. Results
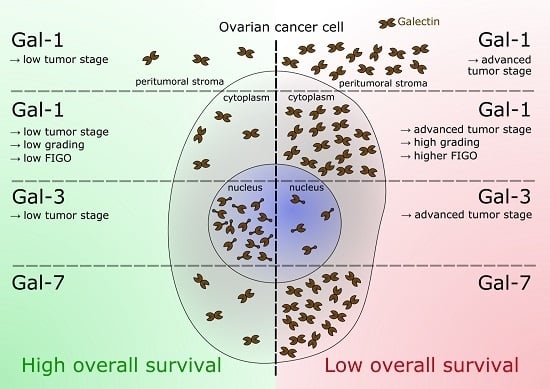
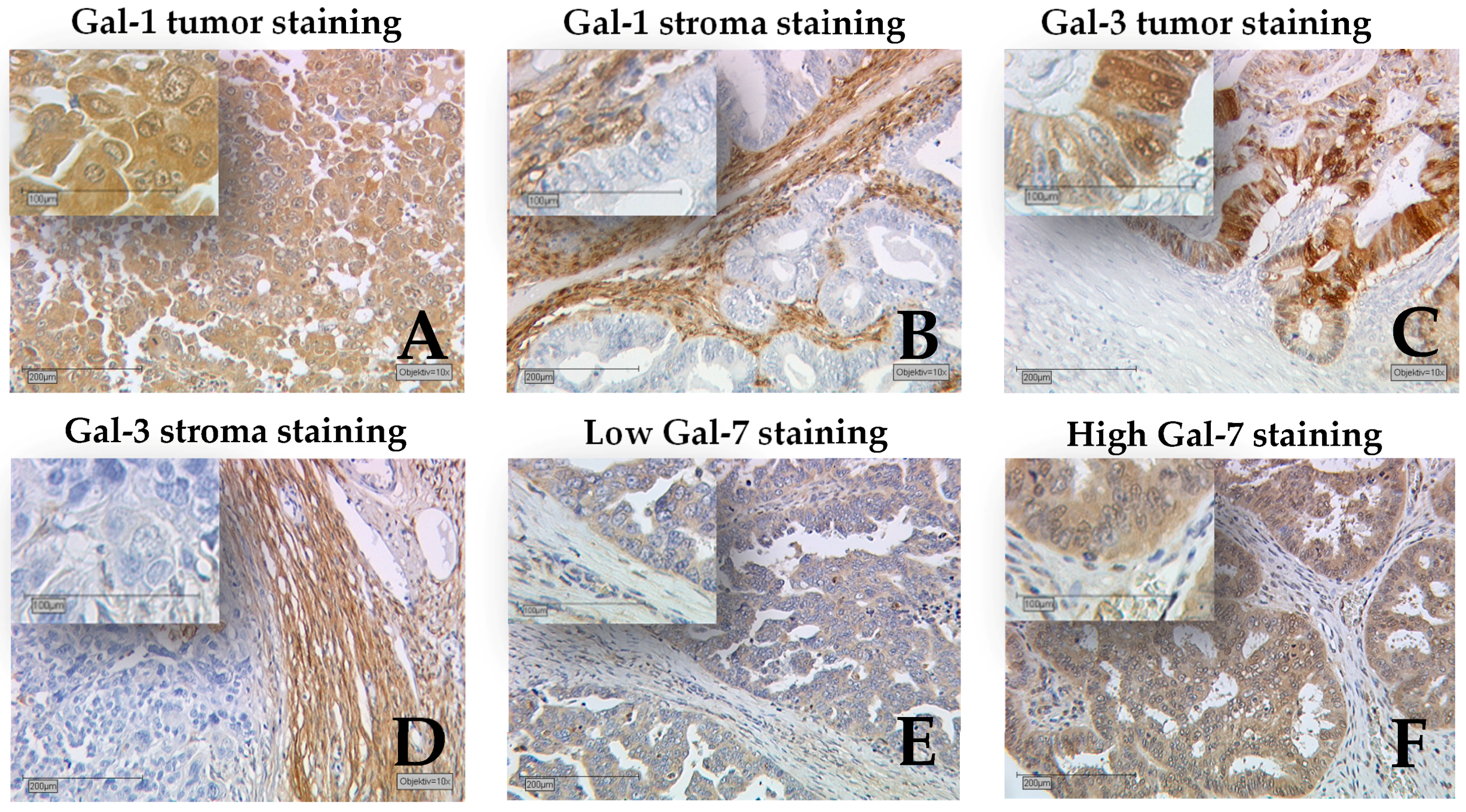
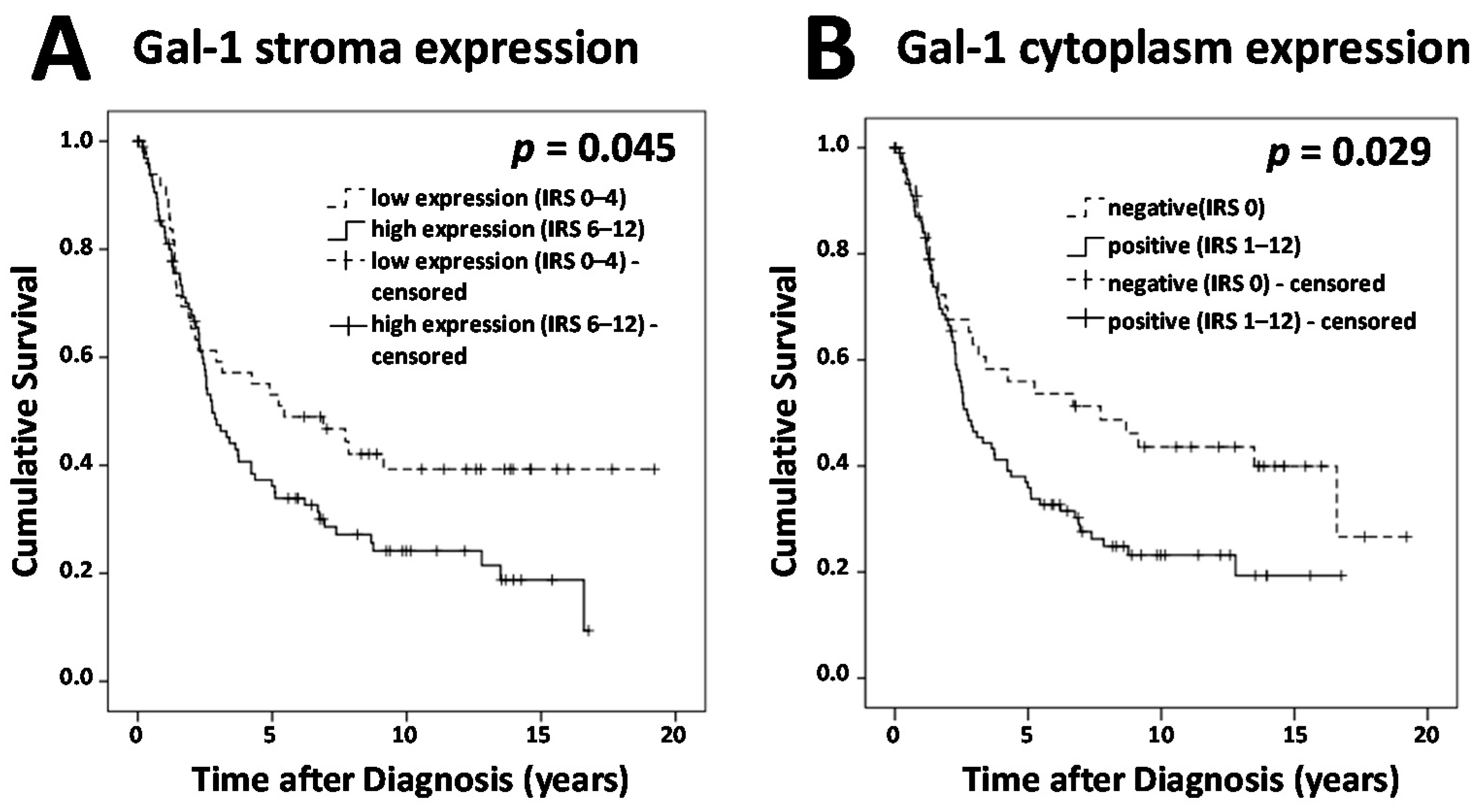
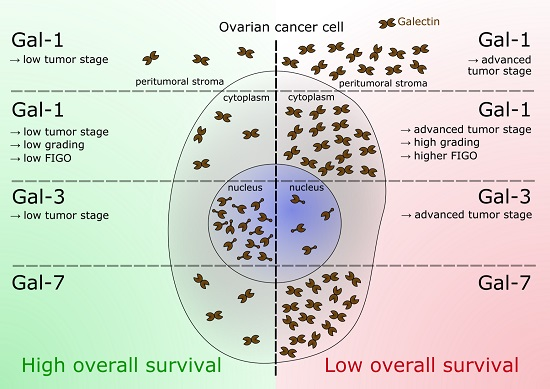
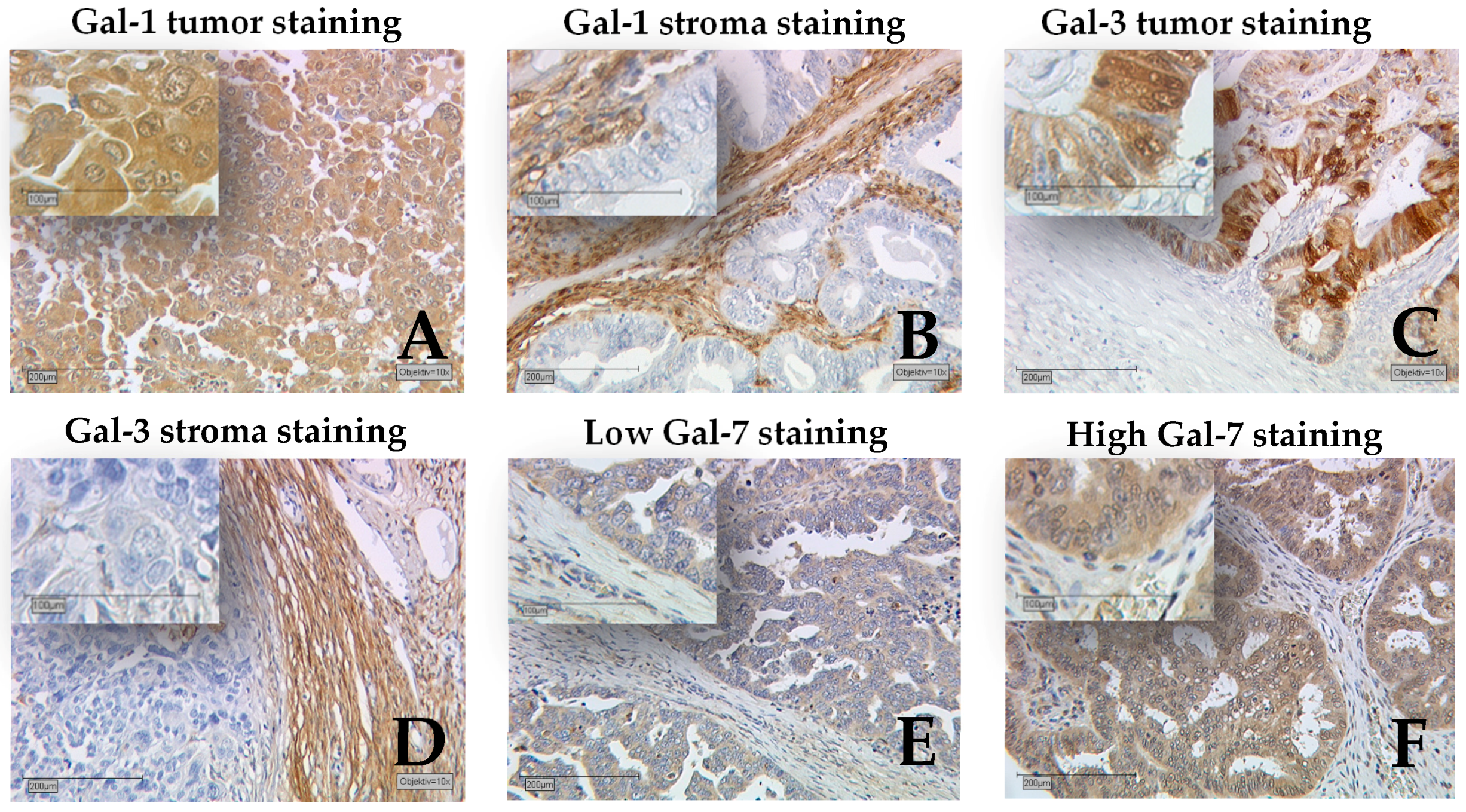
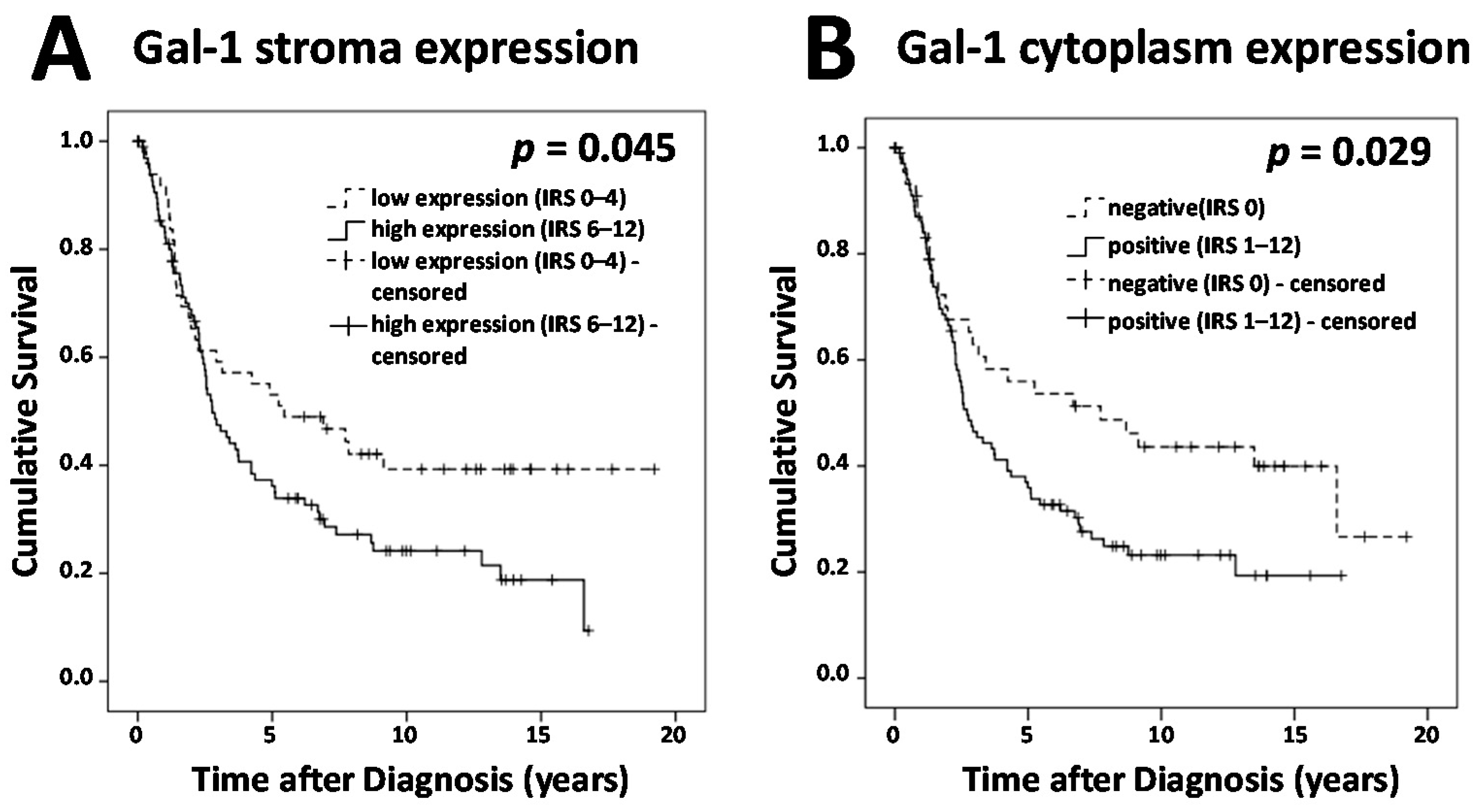
2.1. Gal-1 Tumor and Stroma Staining Is Negative Prognostic for Overall Survival
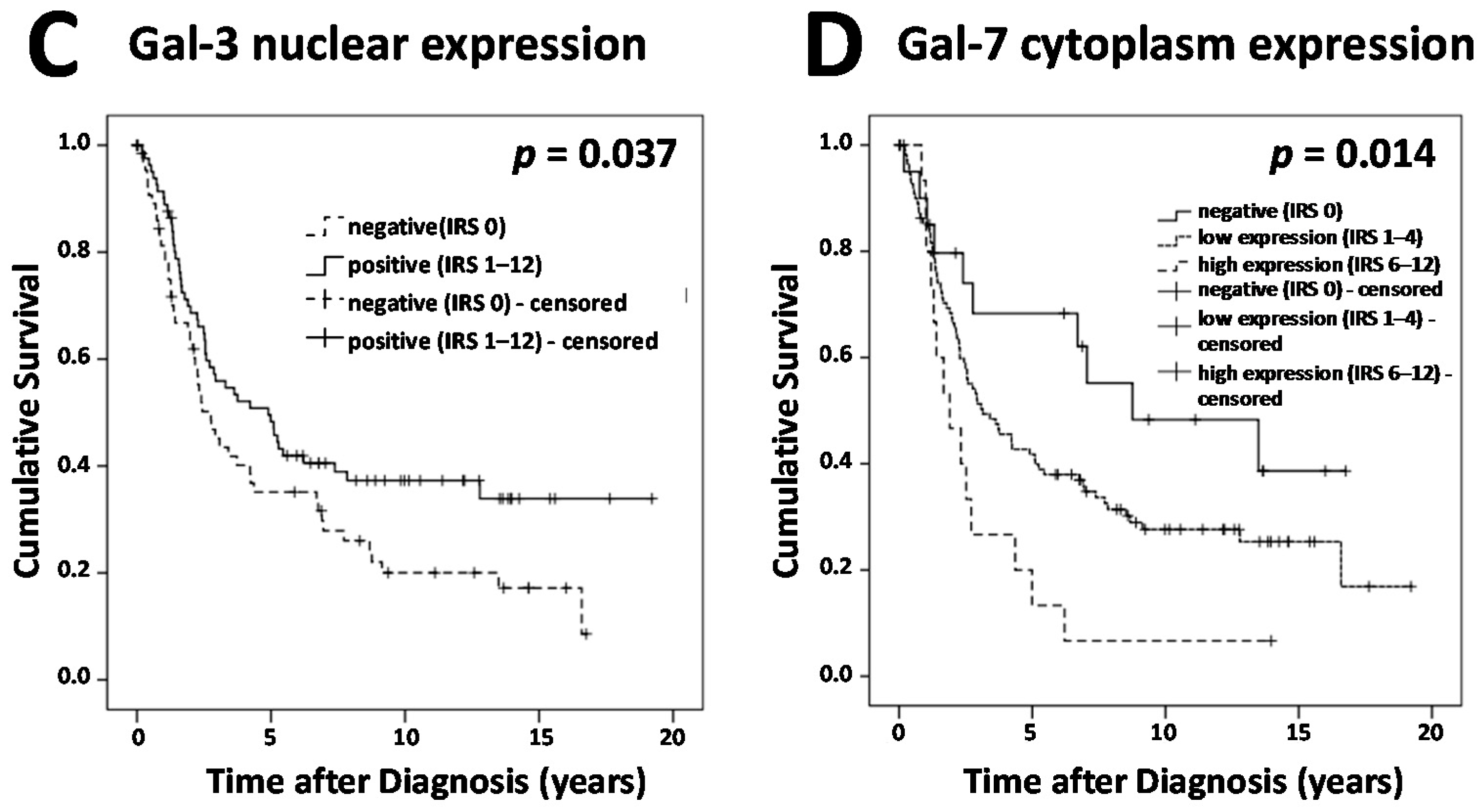
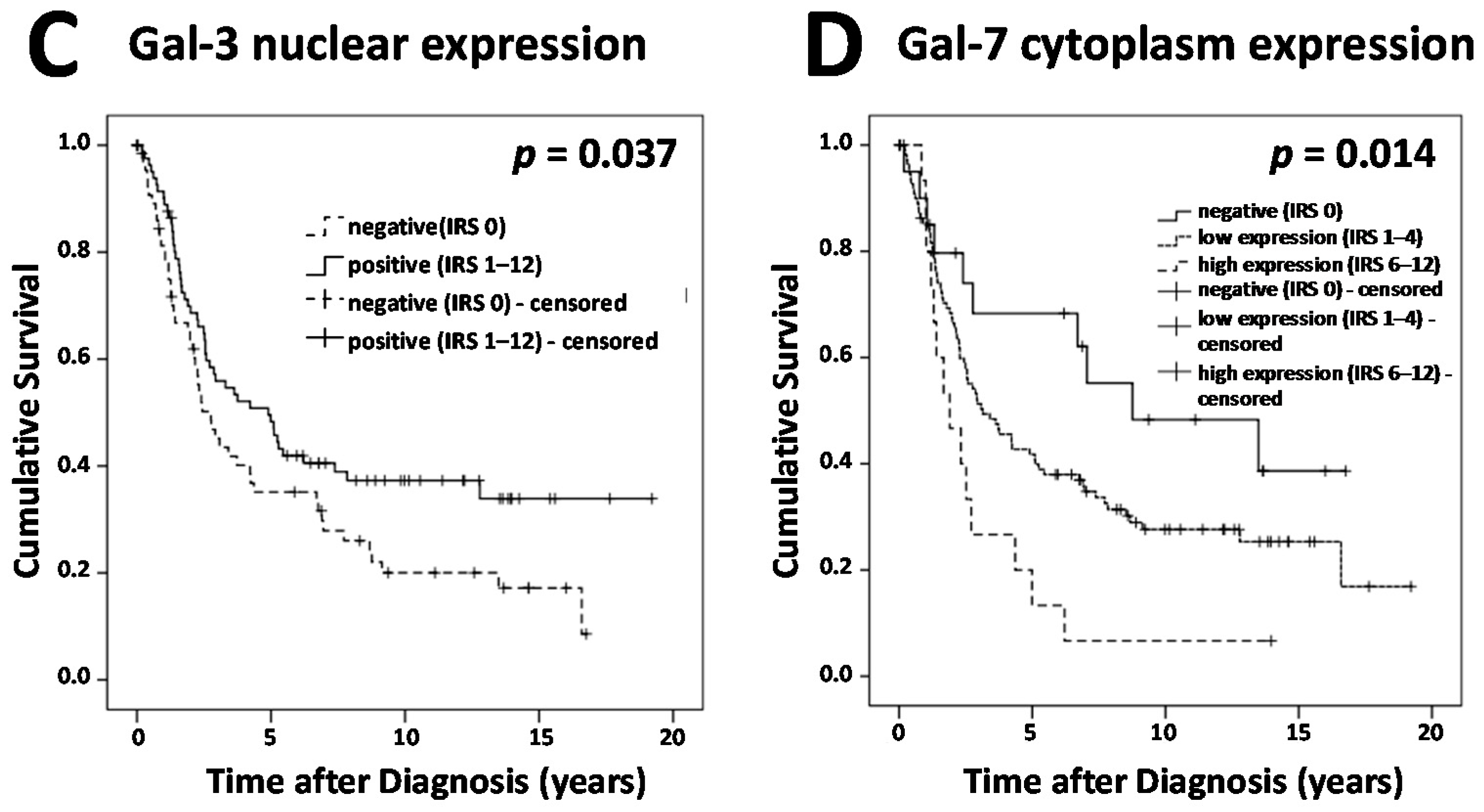
2.2. Presence of Gal-3 in Nuclei Is A Positive Prognosticator in Ovarian Cancer
2.3. Gal-7 Expression Level Predicts Shortened Overall Survival in Ovarian Cancer
2.4. Correlation Analysis
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunochemistry
4.3. Statistical Analysis
4.4. Ethics Statement
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Gal | Galectin |
| BRCA | Breast cancer gene |
| CRD | Carbohydrate-recognition domain |
| UICC | Union for International Cancer Control |
| FIGO | Fédération Internationale de Gynécologie et d’Obstétrique |
| IRS | Remmele score |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Du Bois, A.; Quinn, M.; Thigpen, T.; Vermorken, J.; Avall-Lundqvist, E.; Bookman, M.; Bowtell, D.; Brady, M.; Casado, A.; Cervantes, A.; et al. 2004 consensus statements on the management of ovarian cancer: Final document of the 3rd International Gynecologic Cancer Intergroup Ovarian Cancer Consensus Conference (GCIG OCCC 2004). Ann. Oncol. 2005, 16, viii7–viii12. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, L.A.; Huang, B.; Miller, R.W.; Tucker, T.; Goodrich, S.T.; Podzielinski, I.; DeSimone, C.P.; Ueland, F.R.; van Nagell, J.R.; Seamon, L.G. Ten-year relative survival for epithelial ovarian cancer. Obstet. Gynecol. 2012, 120, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.; Trope, C.G. Ovarian cancer: Diagnostic, biological and prognostic aspects. Womens Health 2014, 10, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Heublein, S.; Sabina, K.P.; Doris, M.; Nina, D.; Udo, J. p53 determines prognostic significance of the carbohydrate stem cell marker TF1 (CD176) in ovarian cancer. J. Cancer Res. Clin. Oncol. 2016, 142, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Kirn, V.; Heublein, S.; Knabl, J.; Guenthner-Biller, M.; Andergassen, U.; Fridrich, C.; Malter, W.; Harder, J.; Friese, K.; Mayr, D. Estrogen receptor promoter methylation predicts survival in low-grade ovarian carcinoma patients. J. Cancer Res. Clin. Oncol. 2014, 140, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Barondes, S.H.; Robbins, B.A.; Liu, F.T. Galectins: A family of animal β-galactoside-binding lectins. Cell 1994, 76, 597–608. [Google Scholar] [CrossRef]
- Barondes, S.H.; Cooper, D.N.; Gitt, M.A.; Leffler, H. Galectins. Structure and function of a large family of animal lectins. J. Biol. Chem. 1994, 269, 20807–20810. [Google Scholar] [PubMed]
- Ebrahim, A.H.; Alalawi, Z.; Mirandola, L.; Rakhshanda, R.; Dahlbeck, S.; Nguyen, D.; Jenkins, M.; Grizzi, F.; Cobos, E.; Figueroa, J.A.; et al. Galectins in cancer: Carcinogenesis, diagnosis and therapy. Ann. Transl Med. 2014, 2, 88. [Google Scholar] [PubMed]
- Cummings, R.D.; Liu, F.T. Galectins. In Essentials of Glycobiology, 2nd ed.; Varki, A., Cummings, R.D., Eds.; Cold Spring Harbor: New York, NY, USA, 2009. [Google Scholar]
- Leffler, H.; Carlsson, S.; Hedlund, M.; Qian, Y.; Poirier, F. Introduction to galectins. Glycoconj. J. 2004, 19, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Danguy, A.; Camby, I.; Kiss, R. Galectins and cancer. Biochim. Biophys. Acta 2002, 1572, 285–293. [Google Scholar] [CrossRef]
- Freydanck, M.K.; Laubender, R.P.; Rack, B.; Schuhmacher, L.; Jeschke, U.; Scholz, C. Two-marker combinations for preoperative discrimination of benign and malignant ovarian masses. Anticancer Res. 2012, 32, 2003–2008. [Google Scholar] [PubMed]
- Zhang, P.; Shi, B.; Zhou, M.; Jiang, H.; Zhang, H.; Pan, X.; Gao, H.; Sun, H.; Li, Z. Galectin-1 overexpression promotes progression and chemoresistance to cisplatin in epithelial ovarian cancer. Cell Death Dis. 2014, 5, e991. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Jeon, H.K.; Cho, Y.J.; Park, Y.A.; Choi, J.J.; Do, I.G.; Song, S.Y.; Lee, Y.Y.; Choi, C.H.; Kim, T.J.; et al. High galectin-1 expression correlates with poor prognosis and is involved in epithelial ovarian cancer proliferation and invasion. Eur. J. Cancer 2012, 48, 1914–1921. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Jeon, H.K.; Lee, J.K.; Sung, C.O.; Do, I.G.; Choi, C.H.; Kim, T.J.; Kim, B.G.; Bae, D.S.; Lee, J.W. Clinical significance of galectin-7 in epithelial ovarian cancer. Anticancer Res. 2013, 33, 1555–1561. [Google Scholar] [PubMed]
- Brustmann, H. Epidermal growth factor receptor expression in serous ovarian carcinoma: An immunohistochemical study with galectin-3 and cyclin D1 and outcome. Int. J. Gynecol. Pathol. 2008, 7, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Labrie, M.; Vladoiu, M.C.; Grosset, A.A.; Gaboury, L.; St-Pierre, Y. Expression and functions of galectin-7 in ovarian cancer. Oncotarget 2014, 5, 7705–7721. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Yao, Y.; Sun, L.; Zhou, J.; Liu, J.; Wang, J.; Li, J.; Tang, J. Clinical implication of the serum galectin-1 expression in epithelial ovarian cancer patients. J. Ovarian Res. 2015, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Astorgues-Xerri, L.; Riveiro, M.E.; Tijeras-Raballand, A.; Serova, M.; Neuzillet, C.; Albert, S.; Raymond, E.; Faivre, S. Unraveling galectin-1 as a novel therapeutic target for cancer. Cancer Treatment Rev. 2014, 40, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Dings, R.P.M.; Miller, M.C.; Nesmelova, I.; Astorgues-Xerri, L.; Kumar, N.; Serova, M.; Chen, X.; Raymond, E.; Hoye, T.R.; Mayo, K.H. Anti-tumor agent calixarene 0118 targets human galectin-1 as an allosteric inhibitor of carbohydrate binding. J. Med. Chem. 2012, 5, 5121–5129. [Google Scholar] [CrossRef] [PubMed]
- Astorgues-Xerri, L.; Riveiro, M.E.; Tijeras-Raballand, A.; Serova, M.; Rabinovich, G.A.; Bieche, I.; Vidaud, M.; de Gramont, A.; Martinet, M.; Cvitkovic, E.; et al. OTX008, a selective small-molecule inhibitor of galectin-1, downregulates cancer cell proliferation, invasion and tumour angiogenesis. Eur. J. Cancer 2014, 50, 2463–2477. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.C.; El -Naggar, A.K.; Lotan, R. Differential expression of galectin-1 and galectin-3 in thyroid tumors. Potential diagnostic implications. Am. J. Pathol. 1995, 147, 815–822. [Google Scholar] [PubMed]
- Gillenwater, A.; Xu, X.C.; El-Naggar, A.K.; Clayman, G.L.; Lotan, R. Expression of galectins in head and neck squamous cell carcinoma. Head Neck 1996, 18, 422–432. [Google Scholar] [CrossRef]
- Sanjuan, X.; Fernandez, P.L.; Castells, A.; Castronovo, V.; Van den Brule, F.; Liu, F.T.; Cardesa, A.; Campo, E. Differential expression of galectin 3 and galectin 1 in colorectal cancer progression. Gastroenterology 1997, 113, 1906–1915. [Google Scholar] [CrossRef]
- Van den Brule, F.; Califice, S.; Garnier, F.; Fernandez, P.L.; Berchuck, A.; Castronovo, V. Galectin-1 accumulation in the ovary carcinoma peritumoral stroma is induced by ovary carcinoma cells and affects both cancer cell proliferation and adhesion to laminin-1 and fibronectin. Lab. Investig. 2003, 83, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Sung, C.O.; Do, I.G.; Jeon, H.K.; Song, T.J.; Park, H.S.; Lee, Y.Y.; Kim, B.G.; Lee, J.W.; Bae, D.S. Overexpression of Galectin-3 and its clinical significance in ovarian carcinoma. Int. J. Clin. Oncol. 2011, 16, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.J.; Wang, W.; Wang, J.L. Understanding the biochemical activities of galectin-1 and galectin-3 in the nucleus. Glycoconj. J. 2004, 19, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.J.; Haudek, K.C.; Voss, P.G.; Wang, J.R. Examination of the role of galectins in pre-mRNA splicing. In Galectin; Stowel, S.R., Cummings, R.D., Eds.; Springer: New York, NY, USA, 2015; pp. 431–449. [Google Scholar]
- Carvalho, R.S.; Fernandes, V.C.; Nepomuceno, T.C.; Rodrigues, D.C.; Woods, N.T.; Suarez-Kurtz, G.; Chammas, R.; Monteiro, A.N.; Carvalho, M.A. Characterization of LGALS3 (galectin-3) as a player in DNA damage response. Cancer Biol. Ther. 2014, 15, 840–850. [Google Scholar] [CrossRef] [PubMed]
- Okada, K.; Shimura, T.; Suehiro, T.; Mochiki, E.; Kuwano, H. Reduced galectin-3 expression is an indicator of unfavorable prognosis in gastric cancer. Anticancer Res. 2006, 26, 1369–1376. [Google Scholar] [PubMed]
- Kramer, M.W.; Kuczyk, M.A.; Hennenlotter, J.; Serth, J.; Schilling, D.; Stenzl, A.; Merseburger, A.S. Decreased expression of galectin-3 predicts tumour recurrence in pTa bladder cancer. Oncol. Rep. 2008, 20, 1403–1408. [Google Scholar] [CrossRef]
- Lu, H.; Liu, Y.; Wang, D.; Wang, L.; Zhou, H.; Xu, G.; Xie, L.; Wu, M.; Lin, Z.; Yu, Y.; et al. Galectin-3 regulates metastatic capabilities and chemotherapy sensitivity in epithelial ovarian carcinoma via NF-κB pathway. Tumour Biol. 2016, 37, 11469–11477. [Google Scholar] [CrossRef] [PubMed]
- Hossein, G.; Keshavarz, M.; Ahmadi, S.; Naderi, N. Synergistic effects of PectaSol-C modified citrus pectin an inhibitor of Galectin-3 and paclitaxel on apoptosis of human SKOV-3 ovarian cancer cells. Asian Pac. J. Cancer Prev. 2013, 14, 7561–7568. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical and Pathological Variables | Gal-1 Expression Cytoplasm | p | Gal-1 Expression Stroma | p | Gal-1 Expression Nucleus | p | |||
|---|---|---|---|---|---|---|---|---|---|
| negative | positive | low | high | negative | positive | ||||
| Histology | |||||||||
| Serous | 26 | 79 | 0.008 | 34 | 71 | NS | 27 | 78 | 0.002 |
| Clear cell | 5 | 7 | 6 | 6 | 3 | 9 | |||
| Endometrioid | 8 | 12 | 7 | 13 | 11 | 9 | |||
| Mucinous | 9 | 4 | 3 | 10 | 9 | 4 | |||
| Tumor Stage | |||||||||
| pT1 | 22 | 17 | <0.001 | 20 | 19 | 0.006 | 19 | 20 | 0.020 |
| pT2+ | 26 | 84 | 30 | 80 | 31 | 79 | |||
| Lymph node | |||||||||
| pN0/pNX | 36 | 65 | NS | 34 | 67 | NS | 43 | 58 | 0.001 |
| pN1 | 12 | 37 | 16 | 33 | 7 | 42 | |||
| Distant Metastasis | |||||||||
| pM0/pMX | 47 | 97 | NS | 49 | 95 | NS | 49 | 95 | NS |
| pM1 | 1 | 5 | 1 | 5 | 1 | 5 | |||
| Grading | |||||||||
| G1 | 20 | 16 | <0.001 | 13 | 23 | NS | 14 | 22 | NS |
| G2+ | 22 | 80 | 31 | 71 | 31 | 71 | |||
| FIGO | |||||||||
| I/II | 22 | 21 | 0.001 | 17 | 26 | NS | 21 | 22 | 0.013 |
| III/IV | 24 | 78 | 31 | 71 | 28 | 74 | |||
| Age | |||||||||
| ≤60 years | 27 | 52 | NS | 28 | 51 | NS | 24 | 55 | NS |
| ≤60 years | 21 | 50 | 22 | 49 | 26 | 45 | |||
| Covariate | Coefficient (bi) | HR Exp (bi) | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Histology (serous vs. other) | 0.211 | 1.235 | 0.658 | 2.317 | 0.511 |
| Grade (G1 vs. G2, G3) | 0.942 | 2.565 | 1.290 | 5.100 | 0.007 |
| FIGO (I, II vs. III, IV) | 1.140 | 3.126 | 1.537 | 6.357 | 0.002 |
| Patients’ age (≤60 vs. >60 years) | 0.312 | 1.367 | 0.861 | 2.169 | 0.185 |
| Gal-1 stroma (low vs. high) | 0.571 | 1.770 | 1.044 | 2.999 | 0.034 |
| Gal-1 cytoplasm (neg. vs. pos.) | −0.187 | 0.830 | 0.423 | 1.626 | 0.586 |
| Gal-3 nucleus (neg. vs. pos.) | −0.265 | 0.767 | 0.480 | 1.227 | 0.269 |
| Gal-7 cytoplasm (neg. vs. pos.) | 0.636 | 1.889 | 1.160 | 3.077 | 0.011 |
| Clinical and Pathological Variables | Gal-3 Expression Cytoplasm | p | Gal-3 Expression Stroma | p | Gal-3 Expression Nucleus | p | |||
|---|---|---|---|---|---|---|---|---|---|
| neg. | pos. | neg. | pos. | neg. | pos. | ||||
| Histology | |||||||||
| Serous | 37 | 69 | NS | 42 | 64 | 0.008 | 44 | 62 | 0.013 |
| Clear cell | 3 | 9 | 2 | 10 | 3 | 9 | |||
| Endometrioid | 12 | 9 | 13 | 8 | 16 | 5 | |||
| Mucinous | 3 | 9 | 9 | 3 | 5 | 7 | |||
| Tumor Stage | |||||||||
| pT1 | 12 | 27 | NS | 21 | 18 | NS | 12 | 27 | 0.042 |
| pT2+ | 43 | 68 | 44 | 67 | 55 | 56 | |||
| Lymph node | |||||||||
| pN0/pNX | 39 | 62 | NS | 47 | 54 | NS | 48 | 53 | NS |
| pN1 | 16 | 34 | 19 | 31 | 20 | 30 | |||
| Distant Metastasis | |||||||||
| pM0/pMX | 53 | 92 | NS | 64 | 81 | NS | 65 | 80 | NS |
| pM1 | 2 | 4 | 2 | 4 | 3 | 3 | |||
| Grading | |||||||||
| G1 | 9 | 28 | NS | 16 | 21 | NS | 13 | 24 | NS |
| G2+ | 40 | 62 | 44 | 58 | 51 | 51 | |||
| FIGO | |||||||||
| I/II | 13 | 30 | NS | 21 | 22 | NS | 15 | 28 | NS |
| III/IV | 41 | 62 | 43 | 60 | 51 | 52 | |||
| Age | |||||||||
| ≤60 years | 22 | 57 | 0.022 | 33 | 46 | NS | 28 | 51 | 0.013 |
| >60 years | 33 | 39 | 33 | 39 | 40 | 32 | |||
| Clinical and Pathological Variables | Gal-7 Expression Cytoplasm | p | ||
|---|---|---|---|---|
| neg. | low | high | ||
| Histology | ||||
| Serous | 10 | 83 | 12 | 0.026 |
| Clear cell | 0 | 10 | 2 | |
| Endometrioid | 7 | 13 | 0 | |
| Mucinous | 3 | 8 | 1 | |
| Tumor Stage | ||||
| pT1 | 4 | 29 | 5 | NS |
| pT2+ | 15 | 85 | 10 | |
| Lymph node | ||||
| pN0/pNX | 15 | 75 | 8 | NS |
| pN1 | 5 | 39 | 7 | |
| Distant Metastasis | ||||
| pM0/pMX | 19 | 110 | 14 | NS |
| pM1 | 1 | 4 | 1 | |
| Grading | ||||
| G1 | 6 | 25 | 3 | NS |
| G2+ | 12 | 80 | 11 | |
| FIGO | ||||
| I/II | 8 | 29 | 4 | NS |
| III/IV | 11 | 81 | 11 | |
| Age | ||||
| ≤60 years | 12 | 59 | 8 | NS |
| >60 years | 8 | 55 | 7 | |
| Staining | Gal-1 Cytoplasm | Gal-1 Stroma | Gal-1 Nucleus | Gal-3 Cytoplasm | Gal-3 Stroma | Gal-3 Nucleus | Gal-7 Cytoplasm | |
|---|---|---|---|---|---|---|---|---|
| Gal-1 cytoplasm | ||||||||
| cc | 1.000 | 0.382 | 0.748 | 0.356 | 0.263 | 0.282 | 0.272 | |
| p | . | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | 0.001 | |
| n | 150 | 150 | 150 | 149 | 149 | 149 | 146 | |
| Gal-1 stroma | ||||||||
| cc | 0.382 | 1.000 | 0.231 | 0.123 | 0.280 | −0.006 | −0.040 | |
| p | <0.001 | . | 0.004 | 0.135 | 0.001 | 0.937 | 0.633 | |
| n | 150 | 150 | 150 | 149 | 149 | 149 | 146 | |
| Gal-1 nucleus | ||||||||
| cc | 0.748 | 0.231 | 1.000 | 0.302 | 0.315 | 0.329 | 0.249 | |
| p | <0.001 | 0.004 | . | <0.001 | <0.001 | <0.001 | 0.002 | |
| n | 150 | 150 | 150 | 149 | 149 | 149 | 146 | |
| Gal-3 cytoplasm | ||||||||
| cc | 0.356 | 0.123 | 0.302 | 1.000 | 0.293 | 0.839 | 0.276 | |
| p | <0.001 | 0.135 | <0.001 | . | <0.001 | <0.001 | 0.001 | |
| n | 149 | 149 | 149 | 151 | 151 | 151 | 146 | |
| Gal-3 stroma | ||||||||
| cc | 0.263 | 0.280 | 0.315 | 0.293 | 1.000 | 0.267 | 0.231 | |
| p | 0.001 | 0.001 | <0.001 | <0.001 | . | 0.001 | 0.005 | |
| n | 149 | 149 | 149 | 151 | 151 | 151 | 146 | |
| Gal-3 nucleus | ||||||||
| cc | 0.282 | −0.006 | 0.329 | 0.839 | 0.267 | 1.000 | 0.335 | |
| p | <0.001 | 0.937 | <0.001 | <0.001 | 0.001 | . | <0.001 | |
| n | 149 | 149 | 149 | 151 | 151 | 151 | 146 | |
| Gal-7 cytoplasm | ||||||||
| cc | 0.272 | −0.040 | 0.249 | 0.276 | 0.231 | 0.335 | 1.000 | |
| p | 0.001 | 0.633 | 0.002 | 0.001 | 0.005 | <0.001 | . | |
| n | 146 | 146 | 146 | 146 | 146 | 146 | 149 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, H.; Schmoeckel, E.; Kuhn, C.; Hofmann, S.; Mayr, D.; Mahner, S.; Jeschke, U. Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients. Int. J. Mol. Sci. 2017, 18, 1230. https://doi.org/10.3390/ijms18061230
Schulz H, Schmoeckel E, Kuhn C, Hofmann S, Mayr D, Mahner S, Jeschke U. Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients. International Journal of Molecular Sciences. 2017; 18(6):1230. https://doi.org/10.3390/ijms18061230
Chicago/Turabian StyleSchulz, Heiko, Elisa Schmoeckel, Christina Kuhn, Simone Hofmann, Doris Mayr, Sven Mahner, and Udo Jeschke. 2017. "Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients" International Journal of Molecular Sciences 18, no. 6: 1230. https://doi.org/10.3390/ijms18061230
APA StyleSchulz, H., Schmoeckel, E., Kuhn, C., Hofmann, S., Mayr, D., Mahner, S., & Jeschke, U. (2017). Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients. International Journal of Molecular Sciences, 18(6), 1230. https://doi.org/10.3390/ijms18061230