Assessment of Aspergillus fumigatus in Guinea Pig Bronchoalveolar Lavages and Pulmonary Tissue by Culture and Realtime Polymerase Chain Reaction Studies

 ,
,
Abstract
:1. Introduction
2. Results and Discussion
3. Experimental Section
3.1. Animals and Immunosuppression
3.2. Preparation of Inoculate and Inhalational Challenge
3.3. Fungal Burden Assessment
3.4. AF Qualitative Realtime PCR Detection Limits
3.5. Extraction and Qualitative Realtime PCR assessment of AF
3.6. Assay Controls and Reaction Details
3.7. Histological Evaluation
3.8. BAL and Lung Homogenate Evaluation
4. Conclusions
References
- Patterson, T.F.; Kirkpatrick, W.R.; White, M.; Himenez, J.W.; Wingard, J.R.; Dupont, B.; Rinaldi, M.G.; Stevens, D.A.; Graybill, J.R. Invasive aspergillosis. Disease spectrum, treatment practices, and outcomes. Medicine 2000, 79, 250–260. [Google Scholar]
- Chandrasekar, P.H.; Alangaden, G.; Manavathu, E. Aspergillosis: An increasing problem in tertiary care hospitals? Clin. Infect. Dis 2000, 30, 984–985. [Google Scholar]
- Patterson, T.F. Advances and challenges in management of invasive mycoses. Lancet 2005, 366, 1013–1025. [Google Scholar]
- Singh, N.; Paterson, D.L. Aspergillus infections in transplant recipients. Clin. Microbiol. Rev 2005, 18, 44–69. [Google Scholar]
- Scientific Registry of Transplant Recipients. OPTN/SRTR Annual Report; US Department of Health & Human Services: Washington, DC, USA, 2009. Available online: http://www.ustransplant.org/annual_reports/current/chapter_I_AR_CD.htm#0 accessed on 22 February 2010.
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive fungal infections among organ transplant recipients: Results of the transplant-associated infection surveillance network (TRANSNET). Clin. Infect. Dis 2010, 50, 1101–1111. [Google Scholar]
- Patterson, T.F. Clinical utility and development of biomarkers in invasive aspergillosis. Trans. Am. Clin. Climatol. Assoc 2010, 122, 174–183. [Google Scholar]
- Maertens, J.; Verhaegen, J.; Lagrou, K. Screening for circulating galactomannan as a noninvasive diagnostic tool for invasive aspergillosis in prolonged neutropenic patients and stem cell transplantation recipients: A prospective evaluation. Blood 2001, 97, 1604–1610. [Google Scholar]
- Boonsarngsuk, V.; Niyompattama, A.; Teosirimongkol, C.; Sriwanichrak, K. False-positive serum and bronchoalveolar lavage Aspergillus galactomannan assays caused by different antibiotics. Scand. J. Infect. Dis 2010, 42, 461–468. [Google Scholar]
- Pinel, C.; Fricker-Hidalgo, H.; Lebeau, B. Detection of circulating Aspergillus fumigatus galactomannan: Value and limits of the Platelia test for diagnosis invasive aspergillosis. J. Clin. Microbiol 2003, 41, 2184–2186. [Google Scholar]
- Wolk, D.; Mitchell, S.; Patel, R. Principles of molecular microbiology testing methods. Infect. Dis. Clin. N. Am 2001, 15, 1157–1204. [Google Scholar]
- Buchheidt, D. M.; Hummel, D.; Schleiermacher, B.; Spiess, H.; Skladny, R.; Schwerdtfeger, O. A.; Cornely, S.; Wilhelm, S.; Reuter, W. V.; Kern, T.; et al. Prospective multicenter clinical evaluation of a nested PCR assay, a lightcycler mediated PCR assay and a galactomannan ELISA for detection of invasive aspergillosis in neutropenic high risk patients. Abstr. M-2057. Proceedings of the 43rd Interscience Conference of Antimicrobial Agents and Chemotherapy, Chicago, IL, USA, 14–17 September 2003.
- Krajden, M.; Ziermann, R.; Khan, A.; Mak, A.; Leung, K.; Hendricks, D.; Comanor, L. Qualitative detection of hepatitis C virus RNA: Comparison of analytical sensitivity, clinical performance, and workflow of the Cobas Amplicor HCV test version 2.0 and the HCV RNA transcription-mediated amplification qualitative assay. J. Clin. Microbiol 2002, 40, 2903–2907. [Google Scholar]
- Caliendo, A.M.; Schuurman, R.; Yen-Lieberman, B.; Spector, S.A.; Andersen, J.; Manjiry, R.; Crumpacker, C.; Lurain, N.S.; Erice, A. Comparison of quantitative and qualitative PCR assays for Cytomegalovirus DNA in plasma. J. Clin Microbiol 2001, 39, 1334–1338. [Google Scholar]
- Qualitative assays. In Smart Cycler II, Operator Manual; Cepheid: Sunnyvale, CA, USA, 1999–2004; Volume Chapter 5, pp. 157–158.
- Arya, M.; Shergill, I.S.; Williamson, M.; Gommersall, L.; Arya, N.; Patel, H.R. Basic principles of Realtime PCR. Expert Rev. Mol. Diagn 2005, 5, 209–219. [Google Scholar]
- Watson, D.E.; Li, B. TaqMan applications in genetic and molecular toxicology. Int. J. Toxicol 2005, 24, 39–45. [Google Scholar]
- Protocols for Determination of Limits of Detection and Limits of Quantitation; Approved Guideline-Second Edition CLSI Document EP17; Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2004.
- Evaluation of Precision Performance of Quantitative Measurement Methods; Approved Guideline-Second Edition CLSI Document EP5-A2; Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2004.
- User Verification of Performance for Precision and Trueness; Approved Guideline-Second Edition CLSI Document EP15-A2; Clinical and laboratory standards institute (CLSI): Wayne, PA, USA, 2006.
- Vallor, A.E.; Kirkpatrick, W.R.; Najvar, L.K.; Bocanegra, R.; Kinney, M.C.; Fothergill, A.W.; Herrera, M.L.; Wickes, B.L.; Graybill, J.R.; Patterson, T.F. Assessment of Aspergillus fumigatus burden in pulmonary tissue of guinea pigs by quantitative PVR, galactomannan enzyme immunoassay, and quantitative culture. Antimicrobiol. Agents Chemother 2008, 52, 2593–2598. [Google Scholar]
- Sheppard, D.C.; Marr, K.A.; Fredricks, D.N.; Chiang, L.Y.; Doedt, T.; Filler, S.G. Comparison of three methodologies for the determination of pulmonary fungal burden in experimental murine aspergillosis. Clin. Microbiol. Infect 2006, 12, 376–380. [Google Scholar]
- Sheppard, D.C.; Rieg, G.; Chiang, L.Y.; Filler, S.G.; Edwards, J.E., Jr; Ibrahim, A.S. Novel inhalation murine model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother 2004, 48, 1908–1911. [Google Scholar]
- Steinbach, W.J.; Benjamin, D.K., Jr; Trasi, S.A.; Miller, J.L.; Schell, W.A.; Zaas, A.K.; Faster, W.M.; Perfect, J.R. Value of an inhalational l model of invasive aspergillosis. Med. Mycol 2004, 42, 417–425. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
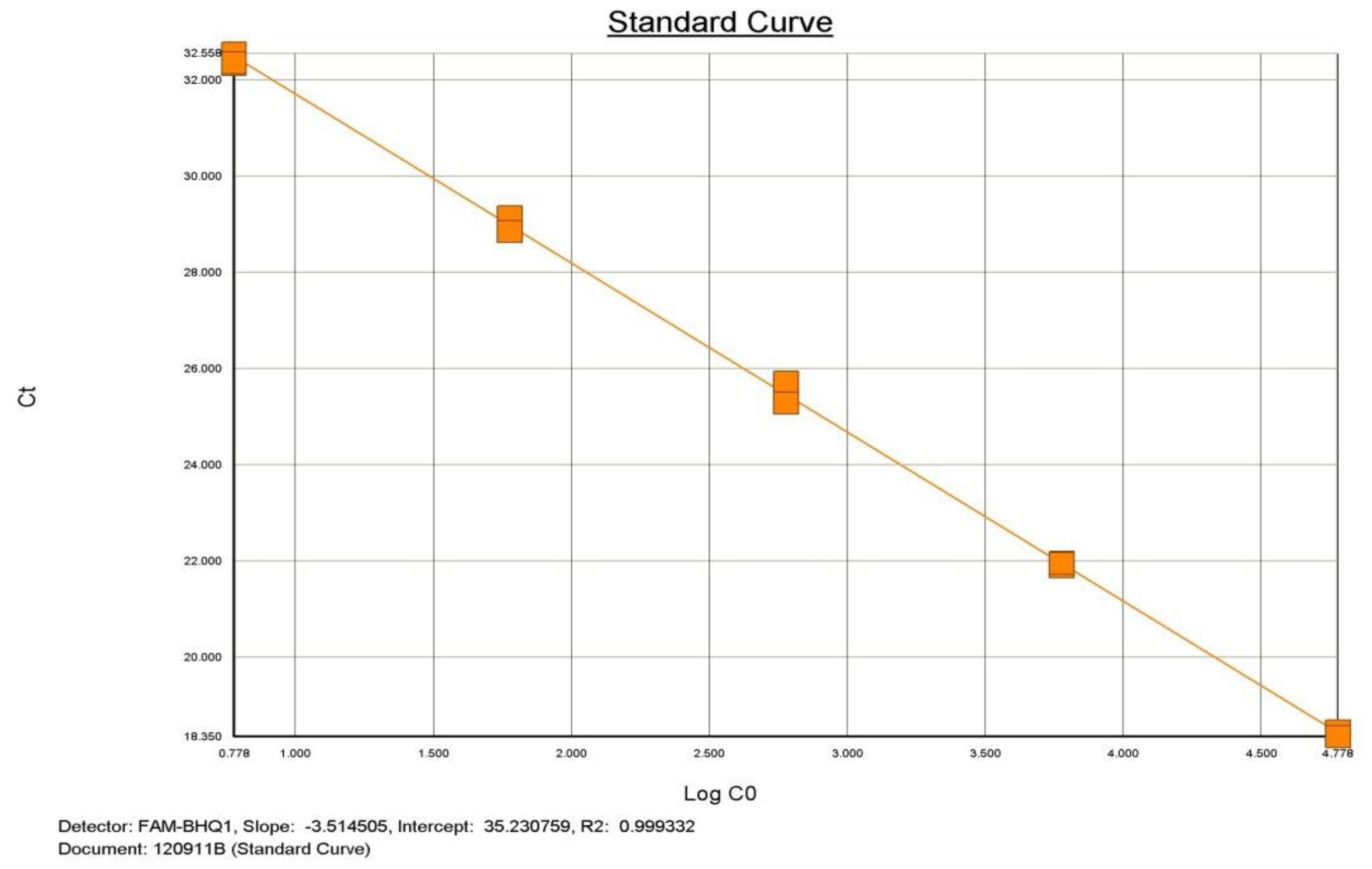
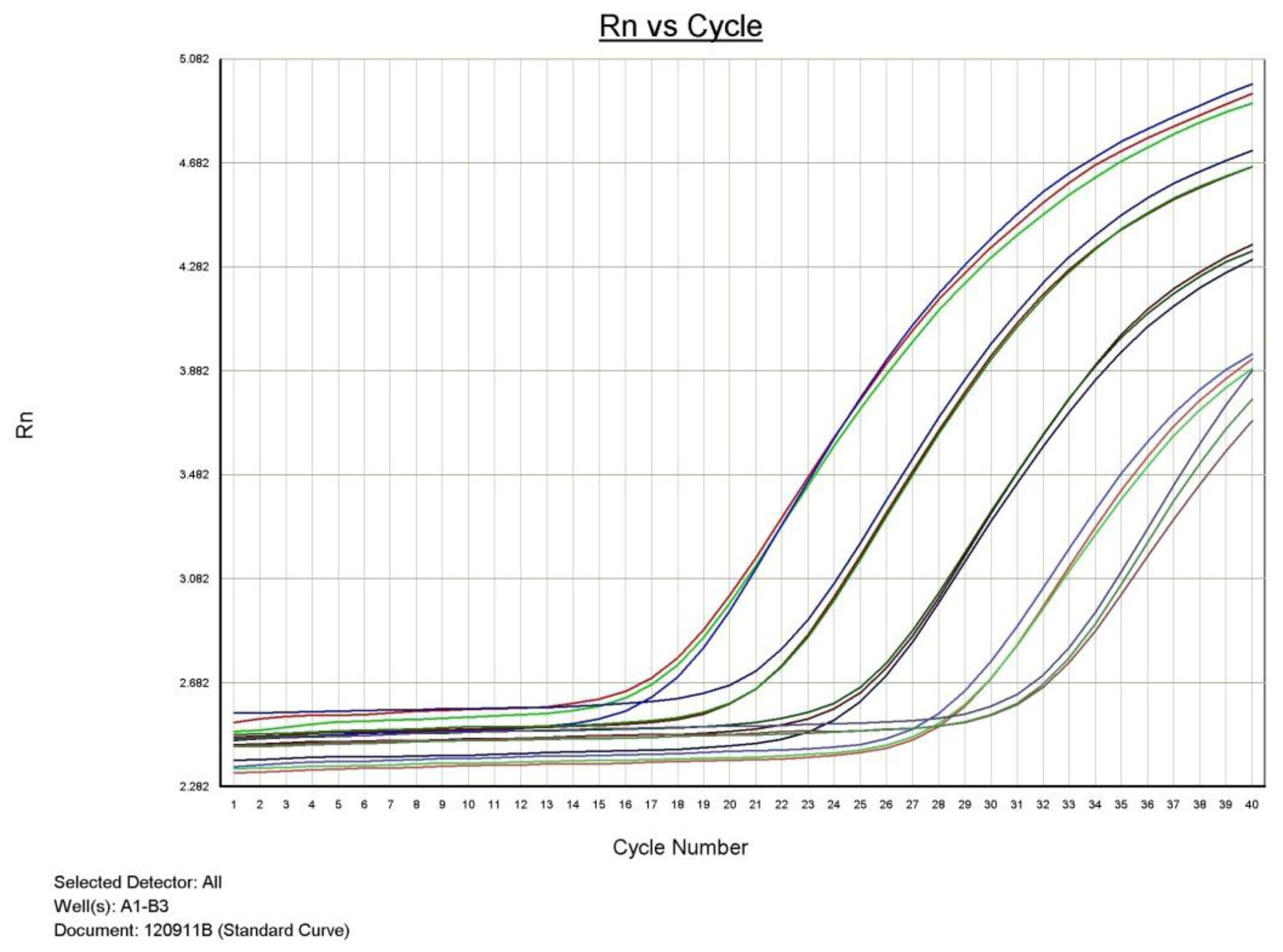
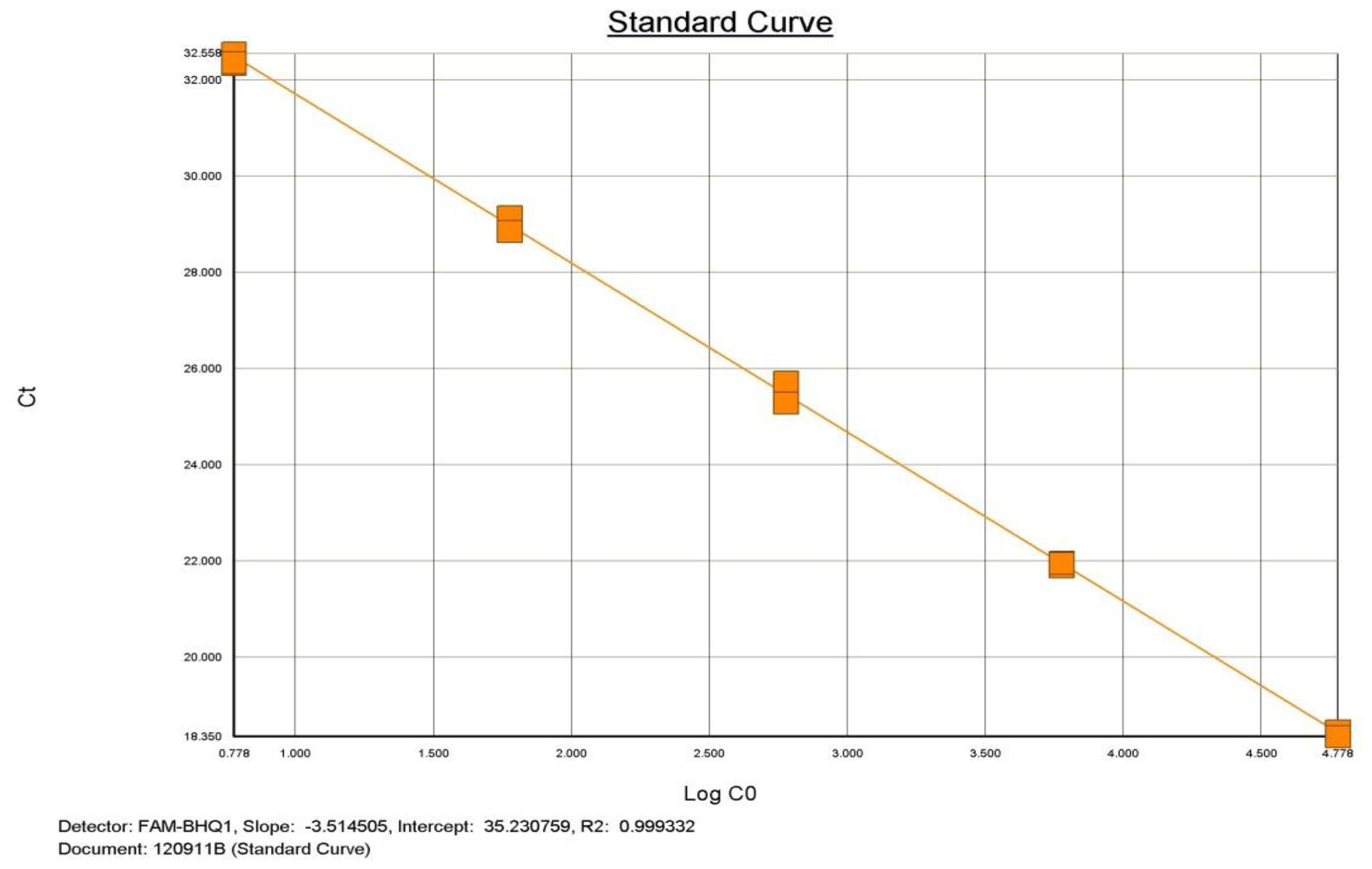
| Points | Approximate concentration of each Point | Result |
|---|---|---|
| 1 | 6 × 104 Copies | Detected |
| 2 | 6 × 103 Copies | Detected |
| 3 | 6 × 102 Copies | Detected |
| 4 | 6 × 10 Copies | Detected |
| 5 | 6 Copies | Detected |
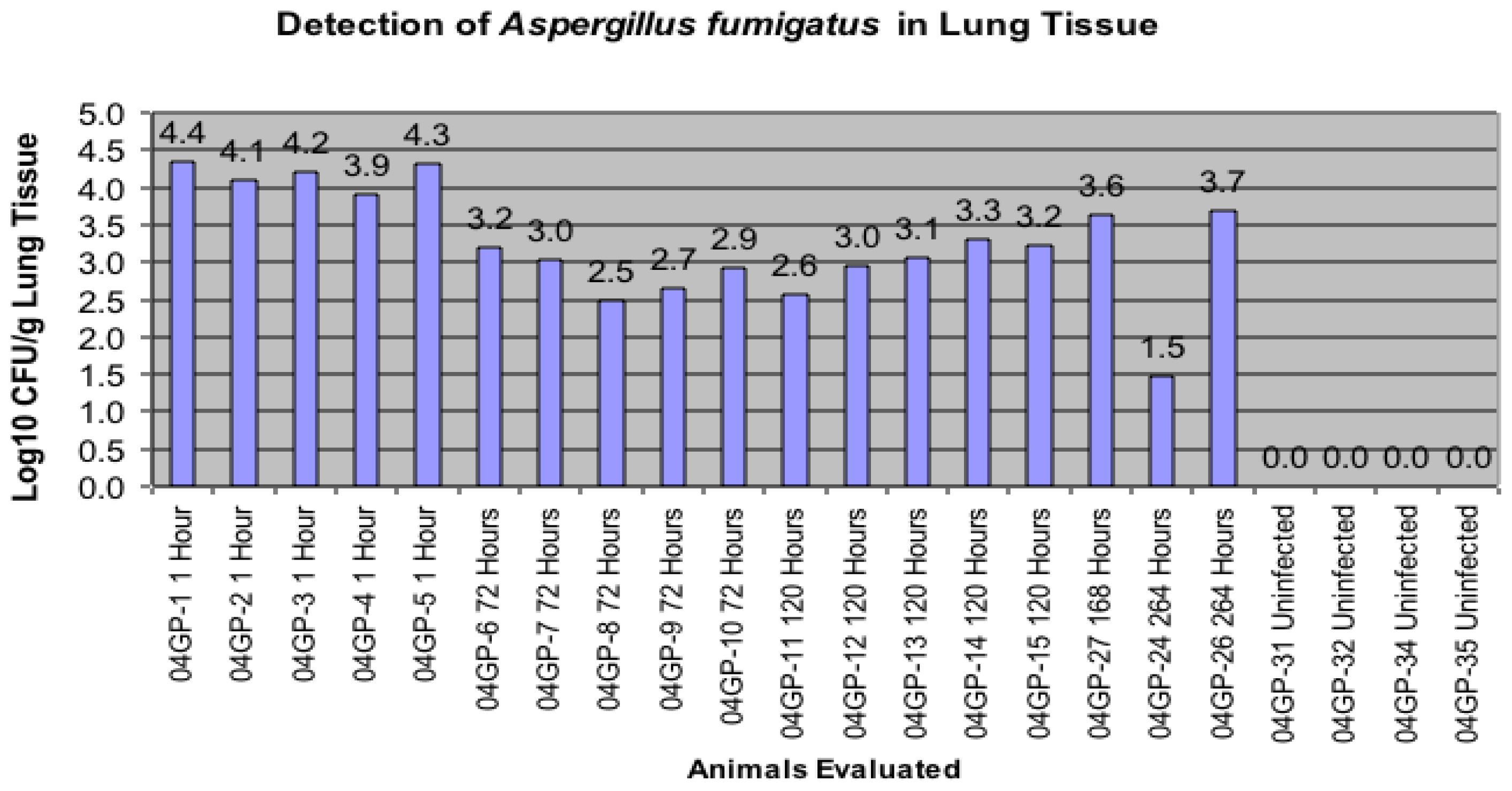
| Animal Identification | Infection Group | Time Animals Sacrificed After infection | A. fumigatus DNA Detected in Lung homogenates | A. fumigatus DNA Detected in BAL |
|---|---|---|---|---|
| 04GP-1 | Infected | At 1 hour | Positive | Positive |
| 04GP-2 | Infected | At 1 hour | Positive | Positive |
| 04GP-3 | Infected | At 1 hour | Positive | Positive |
| 04GP-4 | Infected | At 1 hour | Positive | Positive |
| 04GP-5 | Infected | At 1 hour | Positive | Positive |
| 04GP-6 | Infected | At 72 hours | Positive | Positive |
| 04GP-7 | Infected | At 72 hours | Positive | Positive |
| 04GP-8 | Infected | At 72 hours | Positive | Positive |
| 04GP-9 | Infected | At 72 hours | Positive | Positive |
| 04GP-10 | Infected | At 72 hours | Positive | Positive |
| 04GP-11 | Infected | At 120 hours | Positive | Positive |
| 04GP-12 | Infected | At 120 hours | Positive | Positive |
| 04GP-13 | Infected | At 120 hours | Positive | Positive |
| 04GP-14 | Infected | At 120 hours | Positive | Positive |
| 04GP-15 | Infected | At 120 hours | Positive | Positive |
| 04GP-27 | Infected | At 168 hours | Positive | Positive |
| 04GP-24 | Infected | At 264 hours | Positive | Positive |
| 04GP-26 | Infected | At 264 hours | Positive | Positive |
| 04GP-31 | Not infected | At 264 hours | Not detected | Not detected |
| 04GP-32 | Not infected | At 264 hours | Not detected | Not detected |
| 04GP-34 | Not infected | At 264 hours | Not detected | Not detected |
| 04GP-35 | Not infected | At 264 hours | Not detected | Not detected |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hooper, D.G.; Bolton, V.E.; Sutton, J.S.; Guilford, F.T.; Straus, D.C.; Najvar, L.K.; Wiederhold, N.P.; Kirkpatrick, W.R.; Patterson, T.F. Assessment of Aspergillus fumigatus in Guinea Pig Bronchoalveolar Lavages and Pulmonary Tissue by Culture and Realtime Polymerase Chain Reaction Studies. Int. J. Mol. Sci. 2012, 13, 726-736. https://doi.org/10.3390/ijms13010726
Hooper DG, Bolton VE, Sutton JS, Guilford FT, Straus DC, Najvar LK, Wiederhold NP, Kirkpatrick WR, Patterson TF. Assessment of Aspergillus fumigatus in Guinea Pig Bronchoalveolar Lavages and Pulmonary Tissue by Culture and Realtime Polymerase Chain Reaction Studies. International Journal of Molecular Sciences. 2012; 13(1):726-736. https://doi.org/10.3390/ijms13010726
Chicago/Turabian StyleHooper, Dennis G., Vincent E. Bolton, John S. Sutton, Frederick T. Guilford, David C. Straus, Laura K. Najvar, Nathan P. Wiederhold, William R. Kirkpatrick, and Thomas F. Patterson. 2012. "Assessment of Aspergillus fumigatus in Guinea Pig Bronchoalveolar Lavages and Pulmonary Tissue by Culture and Realtime Polymerase Chain Reaction Studies" International Journal of Molecular Sciences 13, no. 1: 726-736. https://doi.org/10.3390/ijms13010726