
Investigation on the Cancer Invasion and Metastasis of Skin Squamous Cell Carcinoma by Raman Spectroscopy


Abstract
:1. Introduction
2. Results
3. Materials and Methods
3.1. Sample Preparation
3.2. Raman Microspectroscopy System
3.3. Raman Data Processing
4. Conclusions
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Conflicts of Interest
References
- Alam, M.; Ratner, D. Cutaneous squamous-cell carcinoma. N. Engl. J. Med. 2001, 344, 975–983. [Google Scholar] [CrossRef]
- Black, A.P.; Ogg, G.S. The role of p53 in the immunobiology of cutaneous squamous cell carcinoma. Clin. Exp. Immunol. 2003, 132, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Aldabagh, B.; Angeles, J.G.; Cardones, A.R.; Arron, S.T. Cutaneous squamous cell carcinoma and human papillomavirus: Is there an association? Dermatol Surg. 2013, 39, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Ma, D.; Zhang, Y.; Qiao, J.; Wang, B. Identification of a novel mutation and a genetic polymorphism of ever1 gene in two families with epidermodysplasia verruciformis. J. Dermatol. Sci. 2006, 44, 153–159. [Google Scholar] [CrossRef]
- Wheller, L.; Soyer, H.P.; Wheller, L.; Soyer, H.P. Clinical features of actinic keratoses and early squamous cell carcinoma. Curr. Probl. Dermatol. 2015, 46, 58–63. [Google Scholar]
- Otley, C.C. Non-melanoma skin cancer: Past, present, and future. Curr Probl Derm-US 2001, 13, 109–113. [Google Scholar] [CrossRef]
- Robinson, J.K. Sun Exposure, Sun Protection, and Vitamin, D. JAMA 2005, 294, 1541–1543. [Google Scholar] [CrossRef]
- Wang, H.; Huang, N.; Zhao, J.; Lui, H.; Korbelik, M.; Zeng, H. Depth-resolved in vivo micro-Raman spectroscopy of a murine skin tumor model reveals cancer-specific spectral biomarkers. J. Raman Spectrosc. 2015, 42, 160–166. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, L.; Liu, J.; Li, S.; Wang, Q. Comparison of Cancer Incidence between China and the USA. Cancer Bio. Med. 2012, 9, 128–132. [Google Scholar]
- Stublberg, D.L.; Crandell, B.; Fawcett, R.S. Diagnosis and Treatment of Basal Cell and Squamous Cell Carcinomas. Am. Fam. Physician. 2004, 8, 1481–1488. [Google Scholar]
- Caspers, P.J.; Lucassen, G.W.; Wolthuis, R.; Bruining, H.A.; Puppels, G.J. In vitro and in vivo Raman spectroscopy of human skin. Biospectroscopy 1998, 4, 31–39. [Google Scholar] [CrossRef]
- Harz, M.; Rösch, P.; Popp, J. Vibrational spectroscopy--a powerful tool for the rapid identification of microbial cells at the single-cell level. Cytom. Part A 2009, 75, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Krafft, C.; Steiner, G.; Beleites, C.; Salzer, R. Disease recognition by infrared and Raman spectroscopy. J. Biophotonics. 2009, 2, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Downes, A.; Elfick, A. Raman Spectroscopy and Related Techniques in Biomedicine. Sensors 2010, 10, 1871–1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, C.; Hutchings, J.; Barr, H.; Shepherd, N.; Stone, N. Exploiting the diagnostic potential of biomolecular fingerprinting with vibrational spectroscopy. Faraday Discuss. 2011, 149, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Gong, Y.; Zhang, X.; Li, J.; Wang, K.; He, Q.; Bai, J.; Qing, J.; Wang, S. Raman spectral imaging based histopathology of human skin tissue. J. Appl. Spectrosc. 2018, 85, 518–525. [Google Scholar] [CrossRef]
- Devpura, S.; Thakur, J.S.; Sethi, S.; Naik, V.M.; Naik, R. Diagnosis of head and neck squamous cell carcinoma using Raman spectroscopy: Tongue tissues. J. Raman. Spectrosc. 2012, 43, 490–496. [Google Scholar] [CrossRef]
- Guze, K.; Short, M.; Zeng, H.; Lerman, M.; Sonis, S. Comparison of molecular images as defined by Raman spectra between normal mucosa and squamous cell carcinoma in the oral cavity. J. Raman Spectrosc. 2011, 42, 1232–1239. [Google Scholar] [CrossRef]
- Puppels, G.J.; Demul, F.F.; Otto, C.; Greve, J.; Robert-Nicoud, M.; Arndt-Jovin, D.J.; Jovin, T.M. Studying single living cells and chromosomes by confocal Raman microspectroscopy. Nature 1990, 347, 301–303. [Google Scholar] [CrossRef]
- Chen, M.C.; Lord, R.C. Laser-excited Raman spectroscopy of biomolecules. VIII. Conformational study of bovine serum albumin. J. Am. Chem. Soc. 1976, 98, 990–992. [Google Scholar] [CrossRef]
- Overman, S.A.; Thomas, G.J. Raman spectroscopy of the filamentous virus FF (FD, F1, M13): Structural interpretation for coat protein aromatics. Biochemistry 1995, 34, 5440–5451. [Google Scholar] [CrossRef]
- De Gelder, J.; De Gussem, K.; Vandenabeele, P.; Moens, L. Reference database of Raman spectra of biological molecules. J. Raman Spectrosc. 2007, 38, 1133–1147. [Google Scholar] [CrossRef]
- Ali, S.M.; Bonnier, F.J.; Tfayli, A.; Lambkin, H.; Flynn, K.; McDonagh, V.; Healy, C.; Clive Lee, T.; Lyng, F.M.; Byrne, H.J. Raman spectroscopic analysis of human skin tissue sections ex-vivo: Evaluation of the effects of tissue processing and dewaxing. J. Biomed. Opt. 2012, 18, 061202. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Gobinet, C.; Feru, J.; Brassart, S.; Manfait, M.; Piot, O.; Fre, C. Characterization of type I and IV collagens by Raman microspectroscopy: Identification of spectral markers of the dermo-epidermal junction. Spectroscopy 2012, 27, 421–427. [Google Scholar] [CrossRef]
- Rokos, H.; Moore, J.; Hasse, S.; Gillbro, J.; Wood, J.M.; Schallreuter, K.U. In vivo fluorescence excitation spectroscopy and in vivo Fourier-transform Raman spectroscopy in human skin: Evidence of H2O2 oxidation of epidermal albumin in patients with vitiligo. J. Raman Spectrosc. 2004, 35, 125–130. [Google Scholar] [CrossRef]
- Lieber, C.A.; Nethercott, H.E.; Kabeer, M.H. Cancer field effects in normal tissues revealed by Raman spectroscopy. Biomed. Opt. Express. 2010, 1, 975–982. [Google Scholar] [CrossRef]
- Krafft, C.; Neudert, L.; Simat, T.; Salzer, R. Near infrared Raman spectra of human brain lipids. Spectrochim. Acta A 2005, 61, 1529–1535. [Google Scholar] [CrossRef]
- Flach, C.R.; Moore, D.J. Infrared and Raman imaging spectroscopy of ex vivo skin. Int. J. Cosmet. Sci. 2003, 35, 125–135. [Google Scholar] [CrossRef]
- Tfaili, S.; Gobinet, C.; Josse, G.; Angiboust, J.F.; Manfait, M.; Piot, O. Confocal Raman microspectroscopy for skin characterization: A comparative study between human skin and pig skin. Analyst 2012, 137, 3673–3682. [Google Scholar] [CrossRef]
- Larraona-Puy, M.; Ghita, A.; Zoladek, A.; Perkins, W.; Varma, S.; Leach, I.H.; Koloydenko, A.A.; Williams, H.; Notingher, I. Discrimination between basal cell carcinoma and hair follicles in skin tissue sections by Raman micro-spectroscopy. J. Mol. Struct. 2011, 993, 57–61. [Google Scholar] [CrossRef]
- Van Smeden, J.; Janssens, M.; Gooris, G.S.; Bouwstra, J.A. The important role of stratum corneum lipids for the cutaneous barrier function. BBA–Mol. Cell Biol. L 2014, 1841, 295–313. [Google Scholar] [CrossRef]
- Tankiewicz, A.; Dziemianczyk, D.; Buczko, P.; Szarmach, I.J.; Grabowska, S.Z.; Pawlak, D. Tryptophan and its metabolites in patients with oral squamous cell carcinoma: Preliminary study. Adv. Med. Sci.-Poland 2006, 51, 221–224. [Google Scholar]
- Neurauter, G.; Grahmann, A.V.; Klieber, M.; Zeimet, A.; Ledochowski, M.; Sperner-Unterweger, B.; Fuchs, D. Serum phenylalanine concentrations in patients with ovarian carcinoma correlate with concentrations of immune activation markers and of isoprostane-8. Cancer Lett. 2008, 272, 141–147. [Google Scholar] [CrossRef]
- Huang, Z.; Mcwilliams, A.; Lam, S.; English, J.; McLean, D.I.; Lui, H.; Zeng, H. Effect of formalin fixation on the near-infrared Raman spectroscopy of human bronchial tissues. Int. J. Oncol. 2003, 23, 649–655. [Google Scholar] [CrossRef]
- Shim, M. The effects of ex vivo handling procedures on the near-infrared Raman spectra of normal mammalian tissues. Photochem. Photobiol. 1996, 63, 662–671. [Google Scholar] [CrossRef]
- Koduru, M.R.; Ramesh, A.; Adapa, S.; Shetty, J. Salivary albumin as a biomarker for oral squamous cell carcinoma and chronic periodontitis. Ann. Med. Health Sci. Res. 2017, 7, 337–340. [Google Scholar]
- Abramczyk, H.; Brozek-Pluska, B. Raman Imaging in Biochemical and Biomedical Applications. Diagnosis and Treatment of Breast Cancer. Chem. Rev. 2013, 8, 5766–5781. [Google Scholar] [CrossRef]
- Allred, D.C.; Clark, G.M.; Elledge, R.; Fuqua, S.A.; Brown, R.W.; Chamness, G.C.; Osborne, C.K.; McGuire, W.L. Association of p53 Protein Expression With Tumor Cell Proliferation Rate and Clinical Outcome in Node-Negative Breast Cancer. JNCI 1993, 3, 200–206. [Google Scholar] [CrossRef]
- Kerr, L.T.; Byrne, H.J.; Hennelly, B.M. Optimal choice of sample substrate and laser wavelength for Raman spectroscopic analysis of biological specimen. Anal. Methods 2015, 7, 5041–5052. [Google Scholar] [CrossRef] [Green Version]
- Mikoliunaite, L.; Rodriguez, R.D.; Sheremet, E.; Kolchuzhin, V.; Mehner, J.; Ramanavicius, A.; Zahn, D.R. The substrate matters in the Raman spectroscopy analysis of cells. Sci. Rep. 2015, 5, 13150. [Google Scholar] [CrossRef]
Sample Availability: Samples of the compounds are available from the authors. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
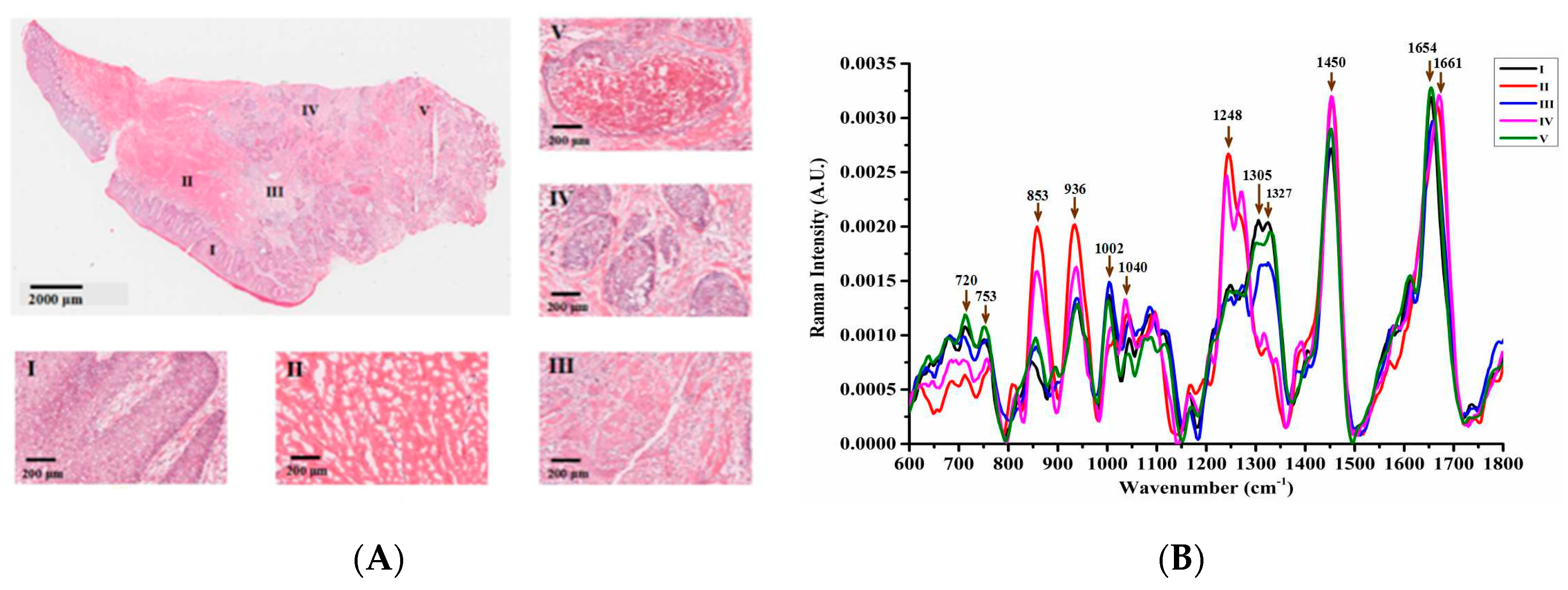
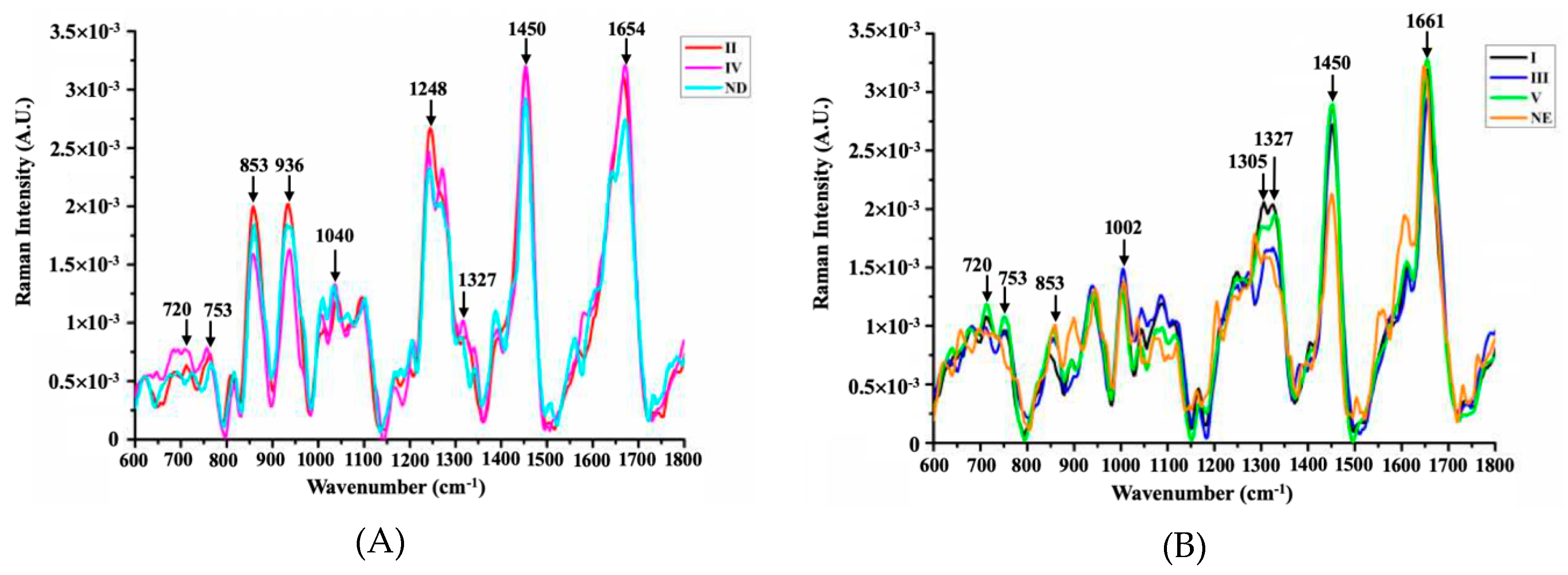
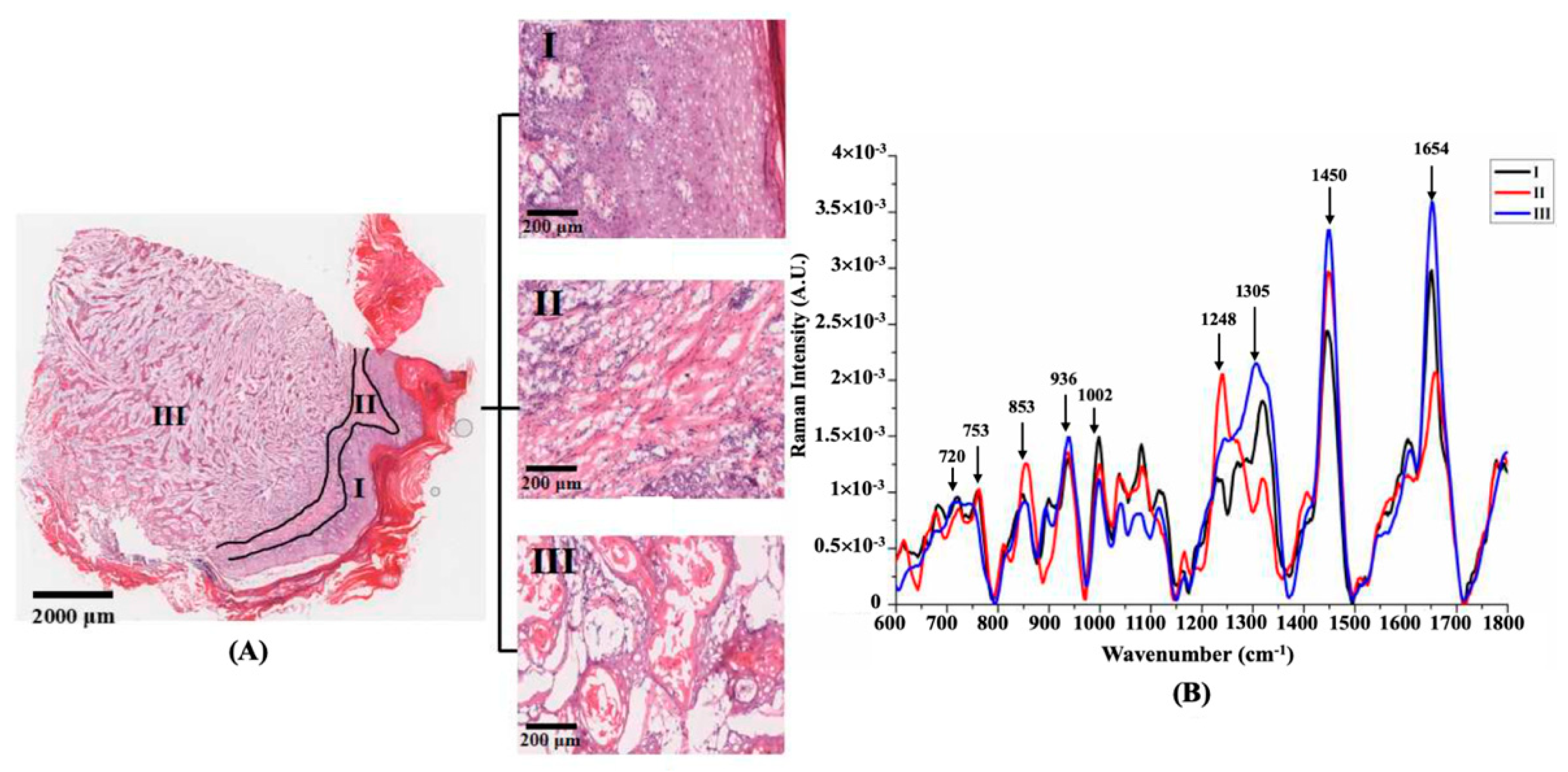
| Wavenumber (cm−1) | Tentative Peak Assignment | Refs. |
|---|---|---|
| 720 | υ (C-N) nucleotide peak or lipid/DNA | [18,19] |
| 753 | Symmetric breathing of tryptophan | [18,19] |
| 853 | υ (C-C) collagen proline ring | [10,20,21] |
| 936 | υ (C-C) collagen backbone/proline ring | [10,20,21] |
| 1002 | υ (C-C) aromatic symmetric ring breathing of phenylalanine | [22,23] |
| 1032 | C-N in-plane bending of phenylalanine | [24,25] |
| 1040 | υ (S-O) cysteic acid | [26,27] |
| 1248 | υ (CN) and δ (NH) amide III of collagen: proline rich | [11,28] |
| 1305 | δ (CH2) lipids/ceramide, | [22,29] |
| 1327 | CH3/CH2 wagging of nucleic acids | [19,30] |
| 1450 | δ (CH2) scissoring of proteins and lipids | [20,21,30] |
| 1654 | υ (C=C) Amide I (protein/lipid) | [28,29] |
| 1661 | υ (C=O) Amide I (collagen) | [21] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Yu, F.; Li, J.; Song, D.; Li, H.; Wang, K.; He, Q.; Wang, S. Investigation on the Cancer Invasion and Metastasis of Skin Squamous Cell Carcinoma by Raman Spectroscopy. Molecules 2019, 24, 2059. https://doi.org/10.3390/molecules24112059
Zhang X, Yu F, Li J, Song D, Li H, Wang K, He Q, Wang S. Investigation on the Cancer Invasion and Metastasis of Skin Squamous Cell Carcinoma by Raman Spectroscopy. Molecules. 2019; 24(11):2059. https://doi.org/10.3390/molecules24112059
Chicago/Turabian StyleZhang, Xu, Fan Yu, Jie Li, Dongliang Song, Heping Li, Kaige Wang, Qingli He, and Shuang Wang. 2019. "Investigation on the Cancer Invasion and Metastasis of Skin Squamous Cell Carcinoma by Raman Spectroscopy" Molecules 24, no. 11: 2059. https://doi.org/10.3390/molecules24112059