A Compositive Strategy to Study the Pharmacokinetics of TCMs: Taking Coptidis Rhizoma, and Coptidis Rhizoma-Glycyrrhizae Radix et Rhizoma as Examples

 and
and
Abstract
:
1. Introduction
2. Results
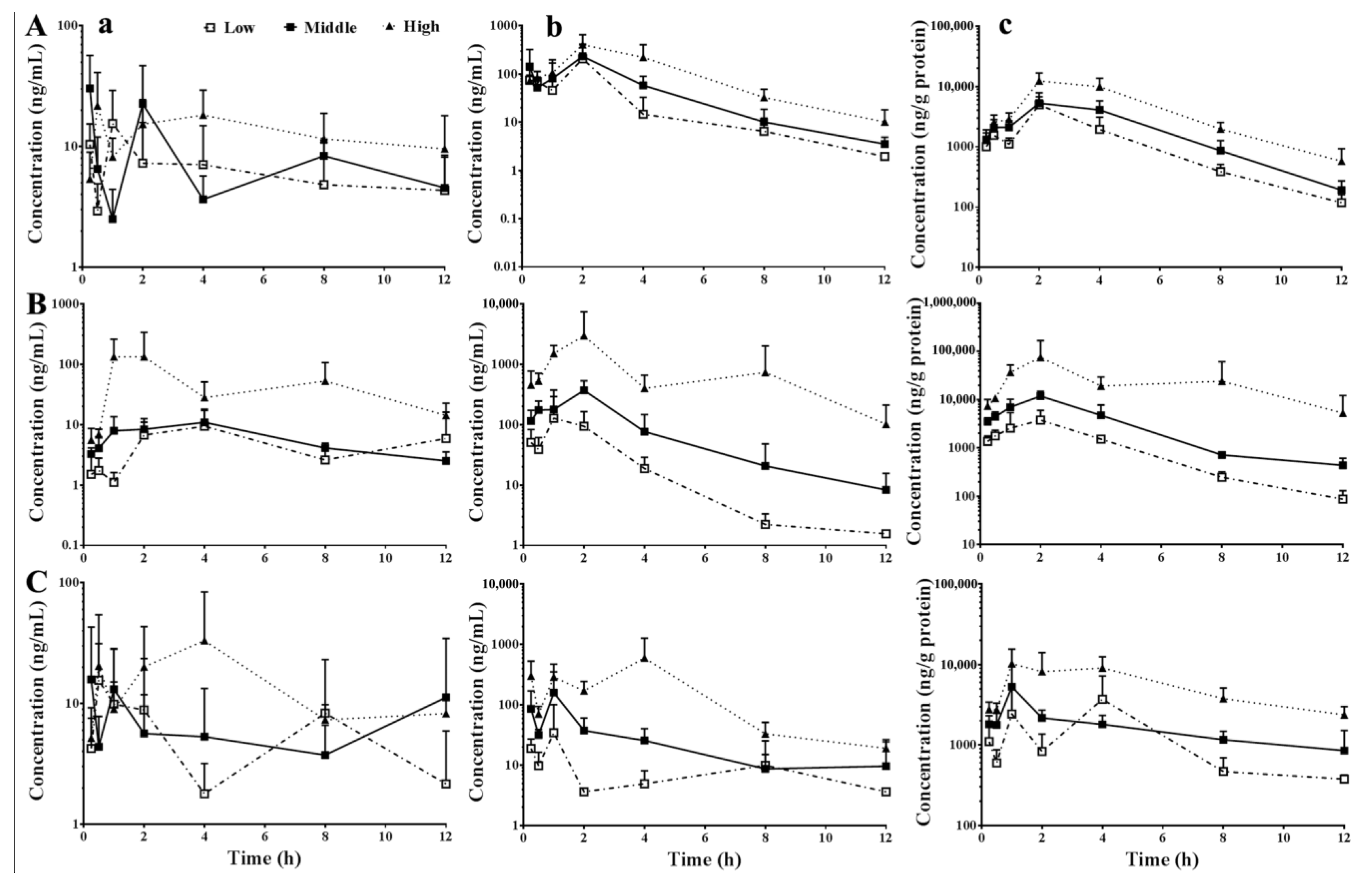
2.1. Dose-Exposure Relationships of Orally Administered Pure Berberine, CRE, and CR-GRE
2.2. Hepatic Accumulation of Berberine
2.3. Roles of Intestinal Absorption and Hepatic Disposition in the Dose-Exposure Relationships of Oral Pure Berberine, CRE, and CR-GRE
2.4. Roles of Intestinal Absorption and Hepatic Disposition in Differentiating the Pharmacokinetic Properties of Oral Pure Berberine, CRE, and CR-GRE
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Materials
5.2. Animals
5.3. Preparation and Quality Control of Coptidis Rhizoma and Coptidis Rhizoma-Glycyrrhizae Radix et Rhizoma Extracts
5.4. Liquid Chromatography Tandem Mass Spectrometry (LC-MS/MS)
5.5. Pharmacokinetics of Berberine in Mice
5.6. Pharmacokinetic Data Processing
5.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Corson, T.W.; Crews, C.M. Molecular understanding and modern application of traditional medicines: Triumphs and trials. Cell 2007, 130, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Hu, Y.; Tan, W.; Wu, X.; Chen, R.; Cao, J.; Chen, M.; Wang, Y. Compatibility art of traditional Chinese medicine: From the perspective of herb pairs. J. Ethnopharmacol. 2012, 143, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Elfawal, M.A.; Towler, M.J.; Reich, N.G.; Weathers, P.J.; Rich, S.M. Dried whole-plant Artemisia annua slows evolution of malaria drug resistance and overcomes resistance to artemisinin. Proc. Natl. Acad. Sci. USA 2015, 112, 821–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, B.L.; Yin, C.; Zhang, B.K.; Dai, Y.; Jia, Y.Q.; Yang, Y.; Li, Q.; Shi, R.; Wang, T.M.; Wu, J.S.; et al. Naturally occurring proteinaceous nanoparticles in Coptidis Rhizoma extract act as concentration-dependent carriers that facilitate berberine absorption. Sci. Rep. 2016, 6, 20110. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.M.; Ribnicky, D.M.; Lipsky, P.E.; Raskin, I. Revisiting the ancient concept of botanical therapeutics. Nat. Chem. Biol. 2007, 3, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, Z.; Li, S.; Ye, X.; Li, X.; He, K. Synergy effects of herb extracts: Pharmacokinetics and pharmacodynamic basis. Fitoterapia 2014, 92, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Eisenblaetter, T.; Teichert, L. Dose Linearity and Proportionality. In Drug Discovery and Evaluation: Methods in Clinical Pharmacology; Vogel, H.G., Maas, J., Gebauer, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Ma, B.L.; Ma, Y.M. Pharmacokinetic herb-drug interactions with traditional Chinese medicine: Progress, causes of conflicting results and suggestions for future research. Drug Metab. Rev. 2016, 48, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Keung, W.M.; Lazo, O.; Kunze, L.; Vallee, B.L. Potentiation of the bioavailability of daidzin by an extract of Radix puerariae. Proc. Natl. Acad. Sci. USA 1996, 93, 4284–4288. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, H.; Kopp, B.; Krenn, L.; Guo, D.; Sendker, J. Traditional Chinese herbal medicine preparation: Invoking the butterfly effect. Science 2015, 350, S64–S66. [Google Scholar]
- Kosinska, A.; Andlauer, W. Modulation of tight junction integrity by food components. Food Res. Int. 2013, 54, 951–960. [Google Scholar] [CrossRef]
- Duan, D.; Doak, A.K.; Nedyalkova, L.; Shoichet, B.K. Colloidal aggregation and the in vitro activity of traditional Chinese medicines. ACS Chem. Biol. 2015, 10, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Ke, L.J.; Gao, G.Z.; Shen, Y.; Zhou, J.W.; Rao, P.F. Encapsulation of Aconitine in Self-Assembled Licorice Protein Nanoparticles Reduces the Toxicity In Vivo. Nanoscale Res. Lett. 2015, 10, 449. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Feng, Y.B.; Tsao, S.; Wang, N.; Curtain, R.; Wang, Y.W. Berberine and Coptidis Rhizoma as novel antineoplastic agents: A review of traditional use and biomedical investigations. J. Ethnopharmacol. 2009, 126, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, B.L.; Ma, Y.M.; Shi, R.; Wang, T.M.; Zhang, N.; Wang, C.H.; Yang, Y. Identification of the toxic constituents in Rhizoma Coptidis. J. Ethnopharmacol. 2010, 128, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.M.; Shang, E.X.; Zhao, J.L.; Fan, X.S.; Duan, J.A.; Qian, D.W.; Tao, W.W.; Tang, Y.P. Data mining and frequency analysis for licorice as a “Two-Face” herb in Chinese Formulae based on Chinese Formulae Database. Phytomedicine 2014, 21, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Ludden, T.M. Nonlinear pharmacokinetics: Clinical Implications. Clin. Pharmacokinet. 1991, 20, 429–446. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.S.; Zheng, Y.R.; Zhang, Y.F.; Long, X.Y. Research progress on berberine with a special focus on its oral bioavailability. Fitoterapia 2016, 109, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.P.; Mahajan, S. Berberine and its derivatives: A patent review (2009–2012). Expert Opin. Ther. Pat. 2013, 23, 215–231. [Google Scholar] [CrossRef] [PubMed]
- Kheir, M.M.; Wang, Y.; Hua, L.; Hu, J.; Li, L.; Lei, F.; Du, L. Acute toxicity of berberine and its correlation with the blood concentration in mice. Food Chem. Toxicol. 2010, 48, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.L.; Yang, Y.; Dai, Y.; Li, Q.; Lin, G.; Ma, Y.M. Polyethylene glycol 400 (PEG400) affects the systemic exposure of oral drugs based on multiple mechanisms: Taking berberine as an example. RSC Adv. 2017, 7, 2435–2442. [Google Scholar] [CrossRef]
- Allijn, I.E.; Czarny, B.M.; Wang, X.; Chong, S.Y.; Weiler, M.; da Silva, A.E.; Metselaar, J.M.; Lam, C.S.; Pastorin, G.; de Kleijn, D.P.; et al. Liposome encapsulated berberine treatment attenuates cardiac dysfunction after myocardial infarction. J. Control Release 2017, 247, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Sut, S.; Faggian, M.; Baldan, V.; Poloniato, G.; Castagliuolo, I.; Grabnar, I.; Perissutti, B.; Brun, P.; Maggi, F.; Voinovich, D.; et al. Natural Deep Eutectic Solvents (NADES) to Enhance Berberine Absorption: An In Vivo Pharmacokinetic Study. Molecules 2017, 22, 1921. [Google Scholar] [CrossRef] [PubMed]
- Amidon, G.L.; Lennernas, H.; Shah, V.P.; Crison, J.R. A Theoretical Basis for a Biopharmaceutic Drug Classification—The Correlation of in-Vitro Drug Product Dissolution and in-Vivo Bioavailability. Pharm. Res. 1995, 12, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.D.; Trevaskis, N.L.; Charman, S.A.; Shanker, R.M.; Charman, W.N.; Pouton, C.W.; Porter, C.J. Strategies to address low drug solubility in discovery and development. Pharmacol. Rev. 2013, 65, 315–499. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.T.; Hao, H.P.; Xie, H.G.; Lai, L.; Wang, Q.; Liu, C.X.; Wang, G.J. Extensive intestinal first-pass elimination and predominant hepatic distribution of berberine explain its low plasma levels in rats. Drug Metab. Dispos. 2010, 38, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.L.; Tsai, T.H. Hepatobiliary excretion of berberine. Drug Metab. Dispos. 2004, 32, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Xue, Y.; Zhang, C.; Wang, L.; Lin, Y.; Pan, G. The involvement of multidrug and toxin extrusion protein 1 in the distribution and excretion of berberine. Xenobiotica 2018, 48, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wu, Z.T.; Ma, L.L.; Ni, X.; Lin, Y.F.; Wang, L.; Chen, K.P.; Huang, C.G.; Pan, G. Organic anion-transporting polypeptides contribute to the hepatic uptake of berberine. Xenobiotica 2015, 45, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.C.; Branco, A.F.; Matos, J.A.; Pereira, S.L.; Parke, D.; Perkins, E.L.; Serafim, T.L.; Sardao, V.A.; Santos, M.S.; Moreno, A.J.; et al. Mitochondrially targeted effects of berberine [Natural Yellow 18, 5,6-dihydro-9,10-dimethoxybenzo(g)-1,3-benzodioxolo(5,6-a) quinolizinium] on K1735-M2 mouse melanoma cells: Comparison with direct effects on isolated mitochondrial fractions. J. Pharmacol. Exp. Ther. 2007, 323, 636–649. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.C.; Ding, L.Q.; Qiu, F. Potential drug interactions associated with glycyrrhizin and glycyrrhetinic acid. Drug Metab. Rev. 2015, 47, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.L.; Yao, M.K.; Zhong, J.; Ma, Y.M.; Gao, C.L.; Wu, J.S.; Qiu, F.R.; Wang, C.H.; Wang, X.H. Increased Systemic Exposure to Rhizoma Coptidis Alkaloids in Lipopolysaccharide-Pretreated Rats Attributable to Enhanced Intestinal Absorption. Drug Metab. Dispos. 2012, 40, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Xing, H.; Ye, H. Efficacy of berberine in patients with type 2 diabetes mellitus. Metab. Clin. Exp. 2008, 57, 712–717. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the extracts (CRE, CR-GRE) are available from the authors. |



{kind=link}
{kind=link}
{kind=link}
| TCMs | Locations | AUC0–12h (ng·h/mL) | Proportionality (γβ-1) | |||
|---|---|---|---|---|---|---|
| Low | Middle | High | Low–High | Middle–High | ||
| Ber | S. circulation | 75.4 | 99.2 | 158.7 | 0.23 | 0.28 |
| P. vein | 462.1 | 685.9 | 1549.7 | 0.37 | 0.57 | |
| Liver | 16,673.0 | 26,711.9 | 60,648.4 | 0.40 | 0.57 | |
| CRE | S. circulation | 62.6 | 75.3 | 629.8 | 1.10 | 7.76 |
| P. vein | 333.6 | 1117.5 | 10,295.2 | 3.37 | 9.43 | |
| Liver | 14,359.6 | 43,657.3 | 311,370.2 | 2.37 | 5.65 | |
| CR-GRE | S. circulation | 70.6 | 77.3 | 191.2 | 0.30 | 0.68 |
| P. vein | 101.4 | 340.0 | 2537.0 | 2.78 | 6.19 | |
| Liver | 17,328.1 | 20,135.8 | 68,701.5 | 0.44 | 1.29 | |
| TCMs | Dosages | AHP | AHC |
|---|---|---|---|
| Ber | Low | 36.1 | 221.1 |
| Middle | 38.9 | 269.3 | |
| High | 39.1 | 382.2 | |
| CRE | Low | 43.0 | 229.4 |
| Middle | 39.1 | 579.8 | |
| High | 30.2 | 494.4 | |
| CR-GRE | Low | 170.8 | 245.6 |
| Middle | 59.2 | 260.6 | |
| High | 27.1 | 359.3 |
| TCMs | Dosages | FL | FL-high/FL-low | FL-ber/FL-CRE or FL-CR-GRE/FL-CRE | FI | FI-high/FI-low | FI-ber/FI-CRE or FI-CR-GRE/FI-CRE |
|---|---|---|---|---|---|---|---|
| Ber | Low | 0.16 | / | 0.87 | 462.1 | / | 1.39 |
| Middle | 0.14 | / | 2.15 | 228.6 | / | 0.61 | |
| High | 0.10 | 0.63 | 1.67 | 172.2 | 0.37 | 0.15 | |
| CRE | Low | 0.19 | / | / | 333.6 | / | / |
| Middle | 0.07 | / | / | 372.5 | / | / | |
| High | 0.06 | 0.33 | / | 1143.9 | 3.43 | / | |
| CR-GRE | Low | 0.70 | / | 3.71 | 101.4 | / | 0.30 |
| Middle | 0.23 | / | 3.37 | 113.3 | / | 0.30 | |
| High | 0.08 | 0.11 | 1.23 | 281.9 | 2.78 | 0.25 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Q.; Yang, Y.; Zhou, T.; Wang, R.; Li, N.; Zheng, M.; Li, Y.-Y.; Zhang, J.-Q.; Wu, F.; Yang, B.-C.; et al. A Compositive Strategy to Study the Pharmacokinetics of TCMs: Taking Coptidis Rhizoma, and Coptidis Rhizoma-Glycyrrhizae Radix et Rhizoma as Examples. Molecules 2018, 23, 2042. https://doi.org/10.3390/molecules23082042
Li Q, Yang Y, Zhou T, Wang R, Li N, Zheng M, Li Y-Y, Zhang J-Q, Wu F, Yang B-C, et al. A Compositive Strategy to Study the Pharmacokinetics of TCMs: Taking Coptidis Rhizoma, and Coptidis Rhizoma-Glycyrrhizae Radix et Rhizoma as Examples. Molecules. 2018; 23(8):2042. https://doi.org/10.3390/molecules23082042
Chicago/Turabian StyleLi, Qiao, Yan Yang, Ting Zhou, Rui Wang, Na Li, Min Zheng, Yuan-Yuan Li, Ji-Quan Zhang, Fei Wu, Bai-Can Yang, and et al. 2018. "A Compositive Strategy to Study the Pharmacokinetics of TCMs: Taking Coptidis Rhizoma, and Coptidis Rhizoma-Glycyrrhizae Radix et Rhizoma as Examples" Molecules 23, no. 8: 2042. https://doi.org/10.3390/molecules23082042