Biodistribution and Tumor Uptake of 67Ga-Nimotuzumab in a Malignant Pleural Mesothelioma Xenograft

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Radiolabeling
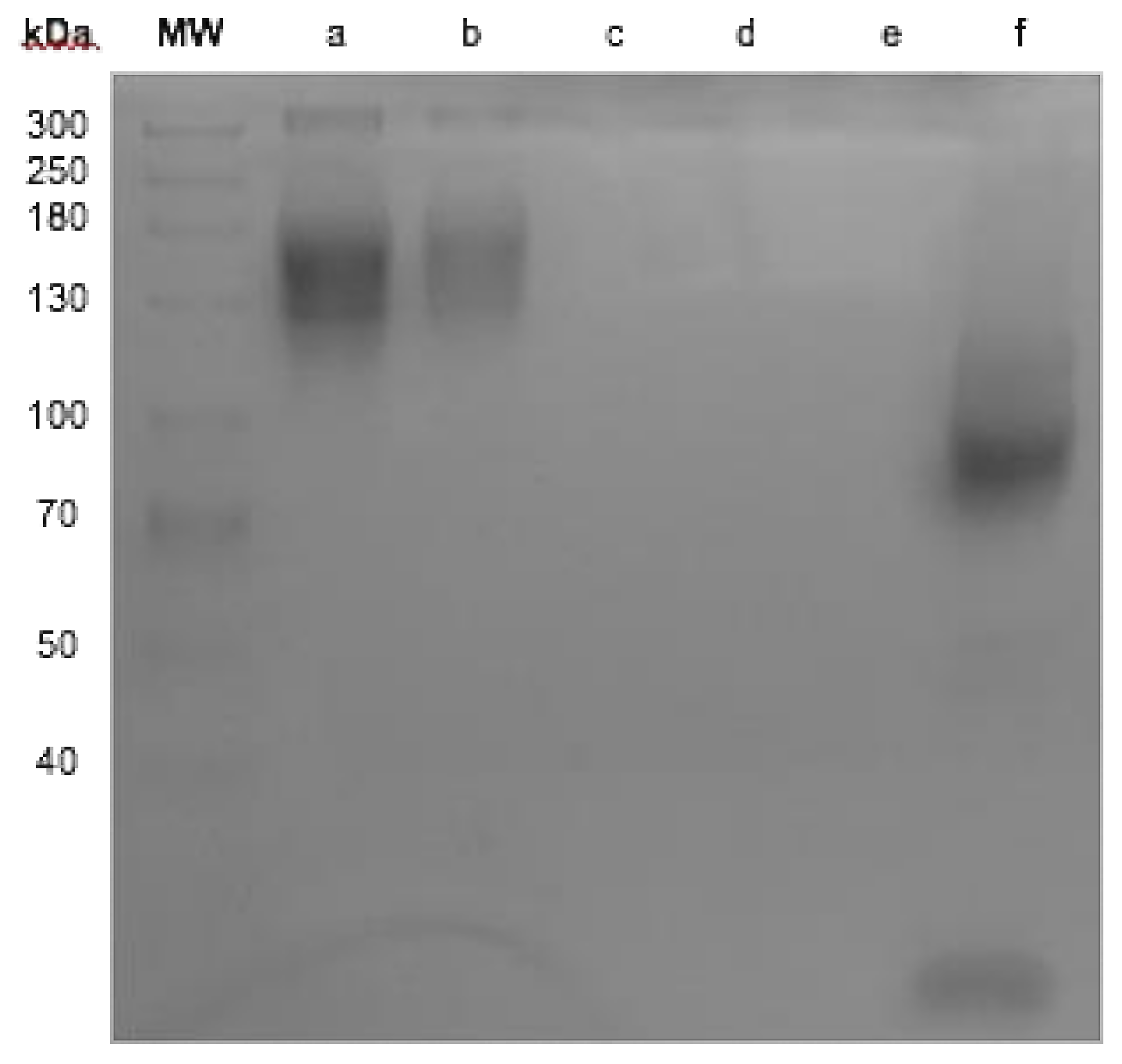
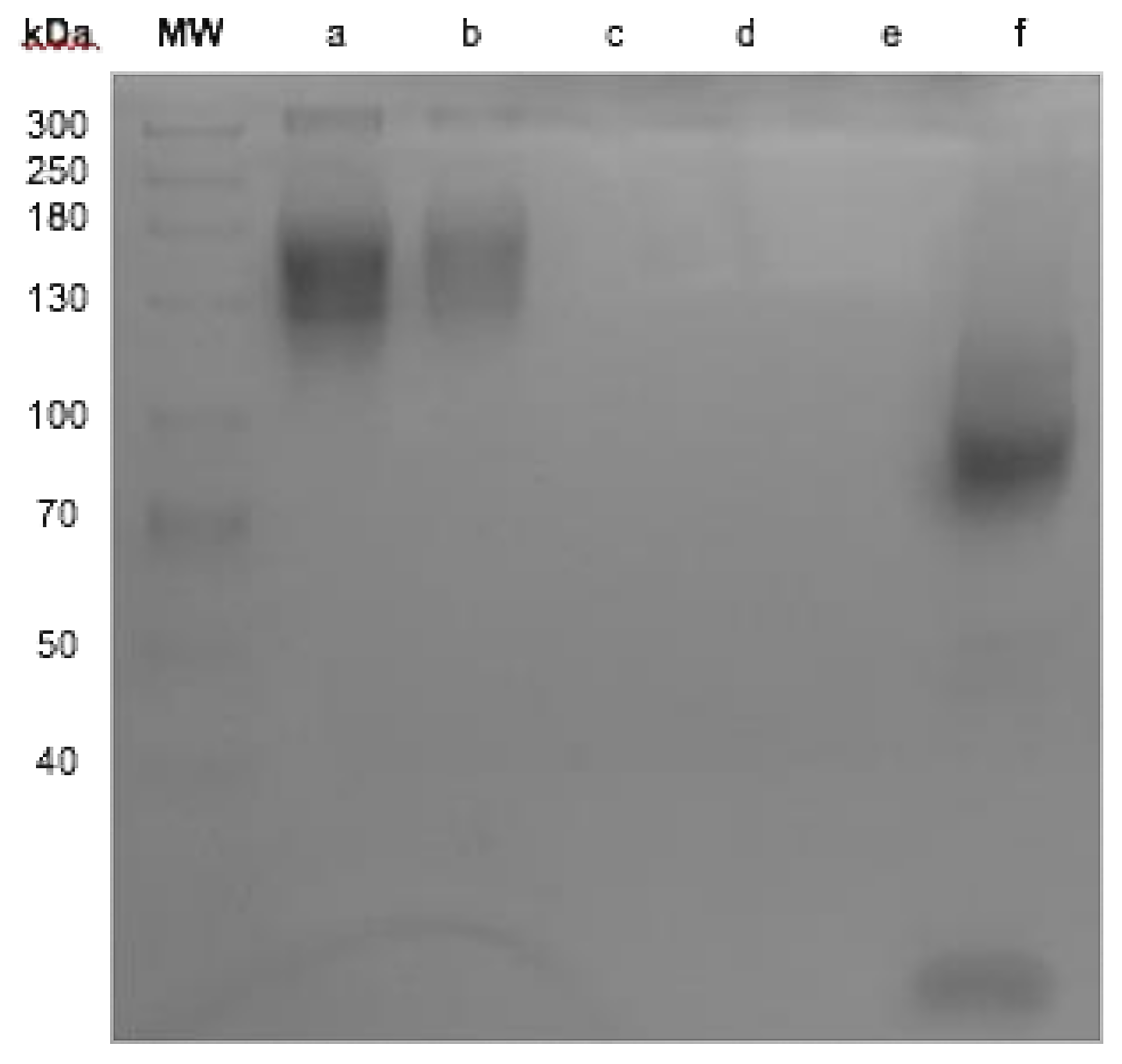
2.2. Antibody Integrity
2.3. Cell Binding Assay
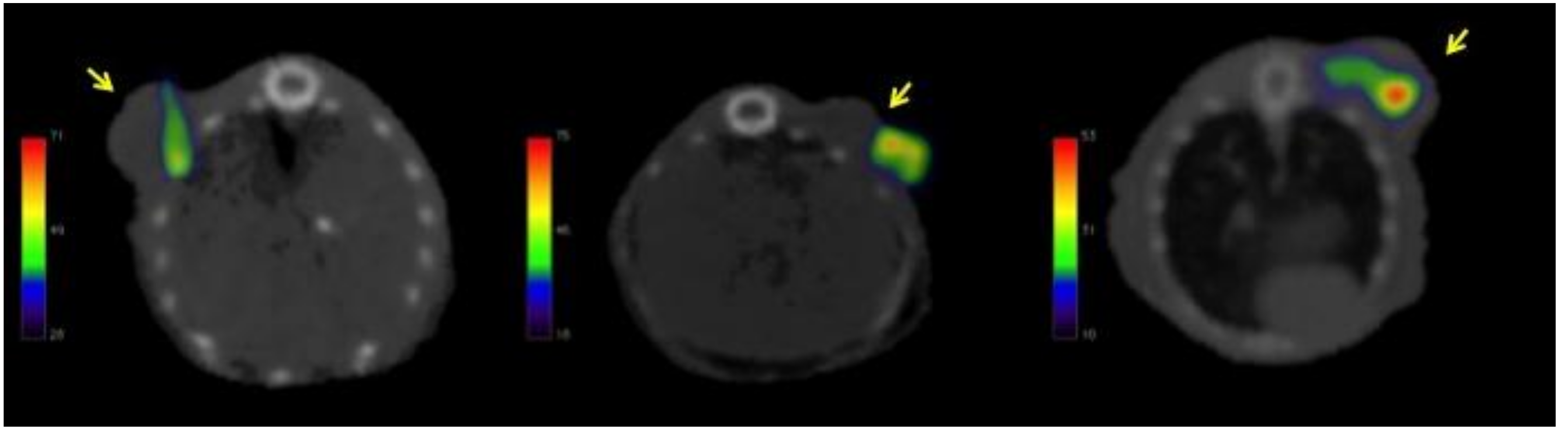
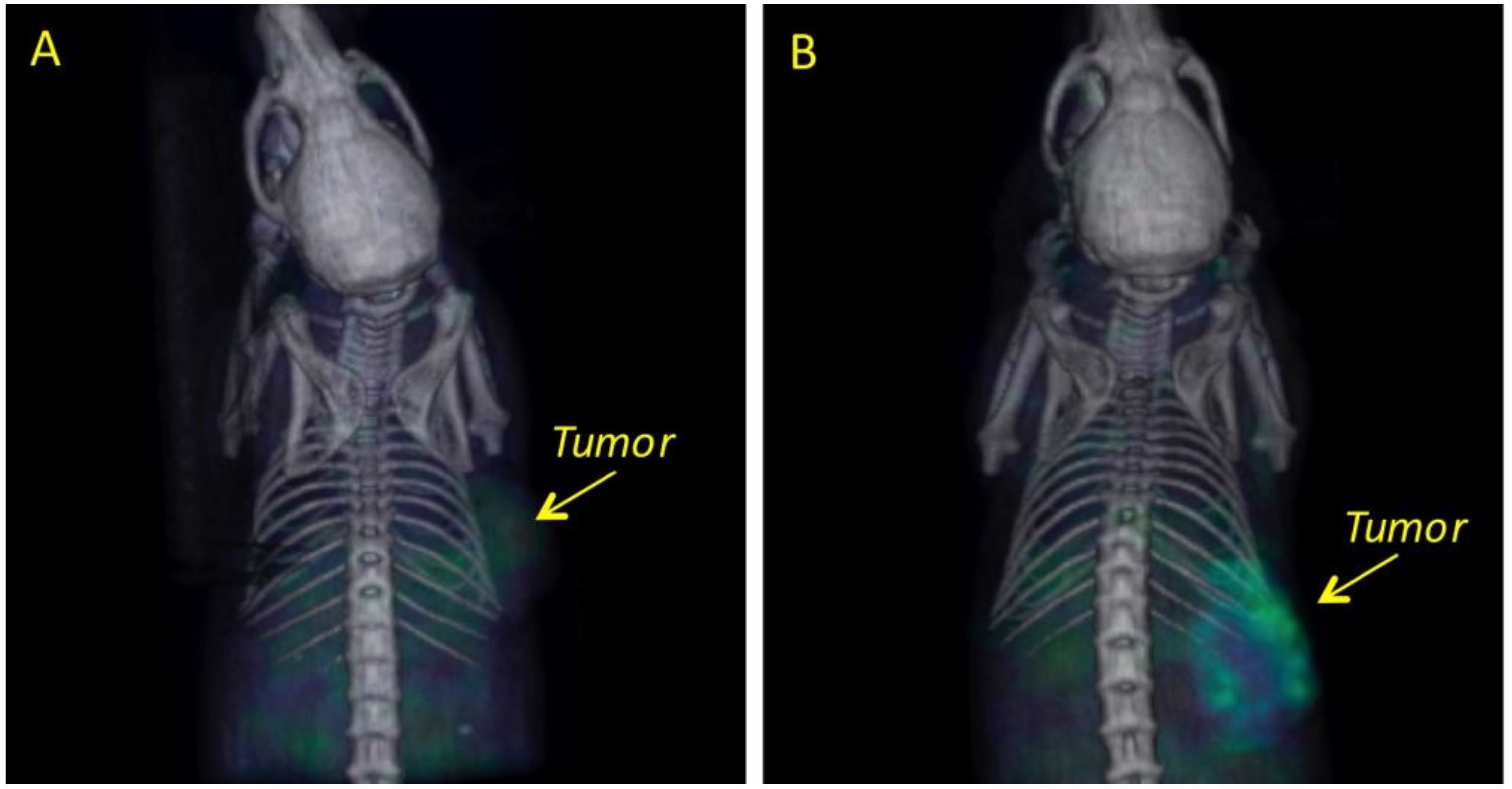
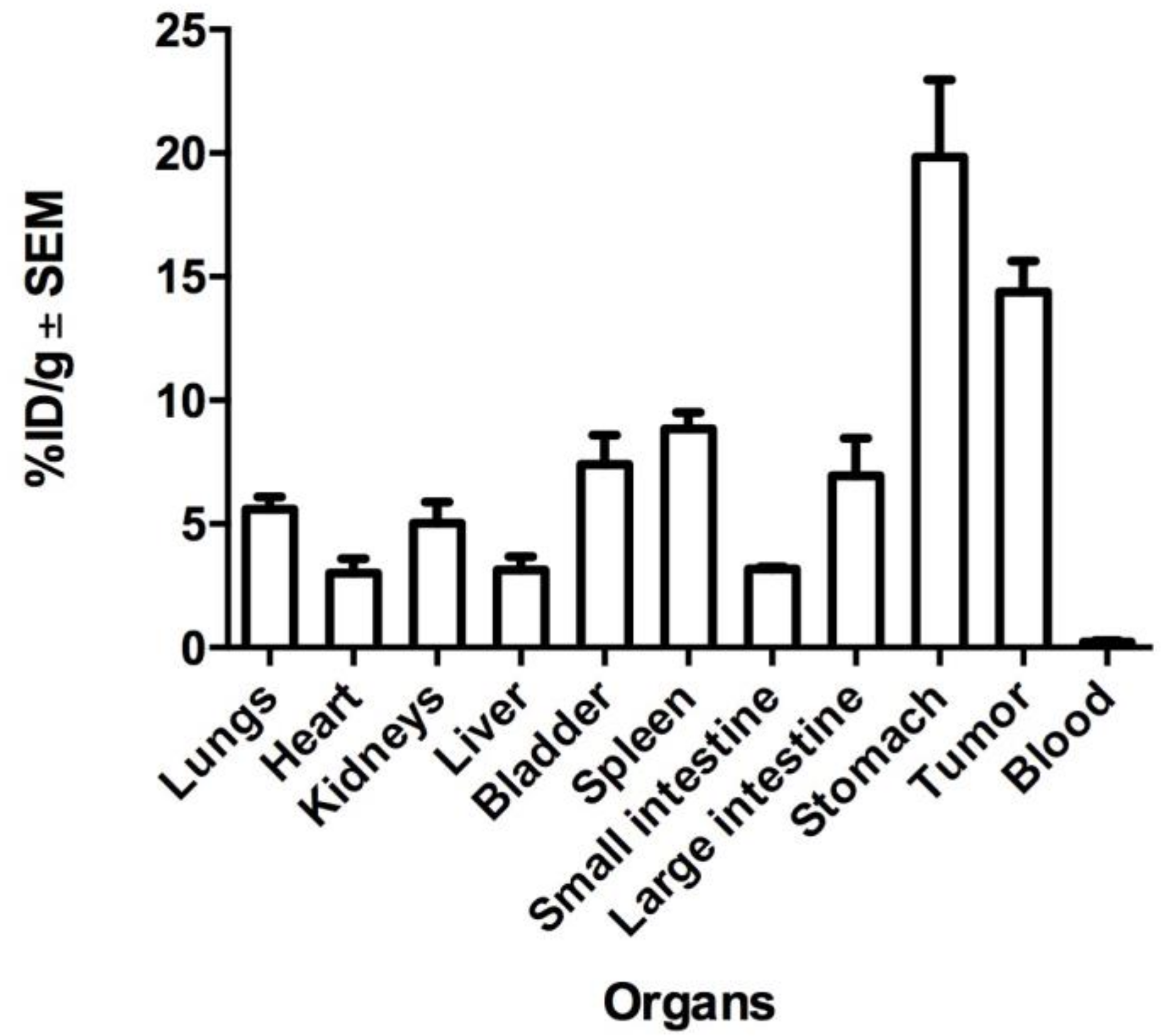
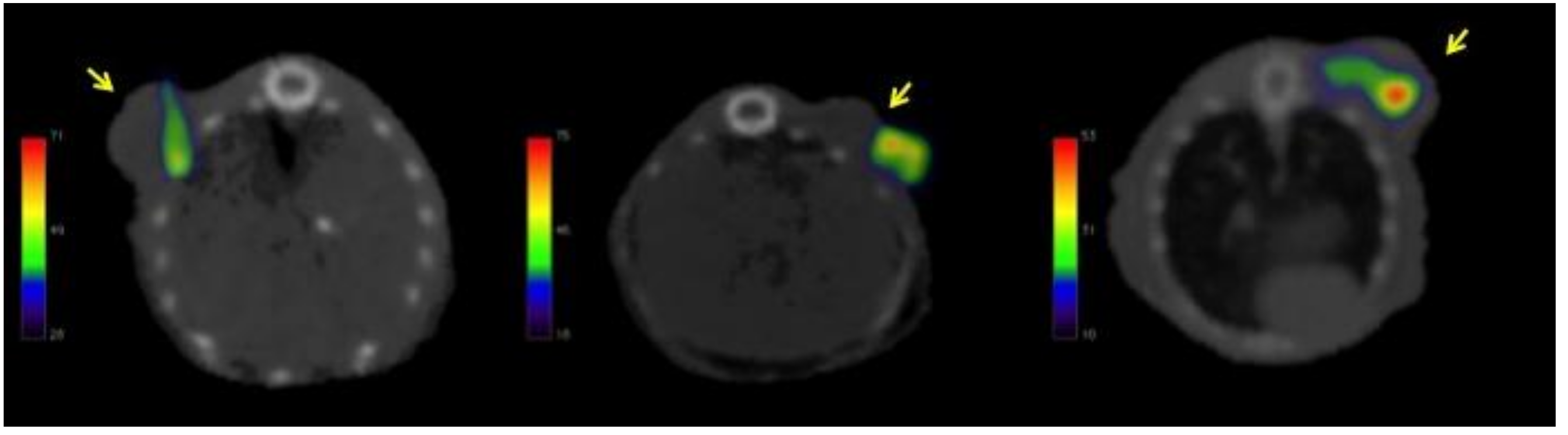
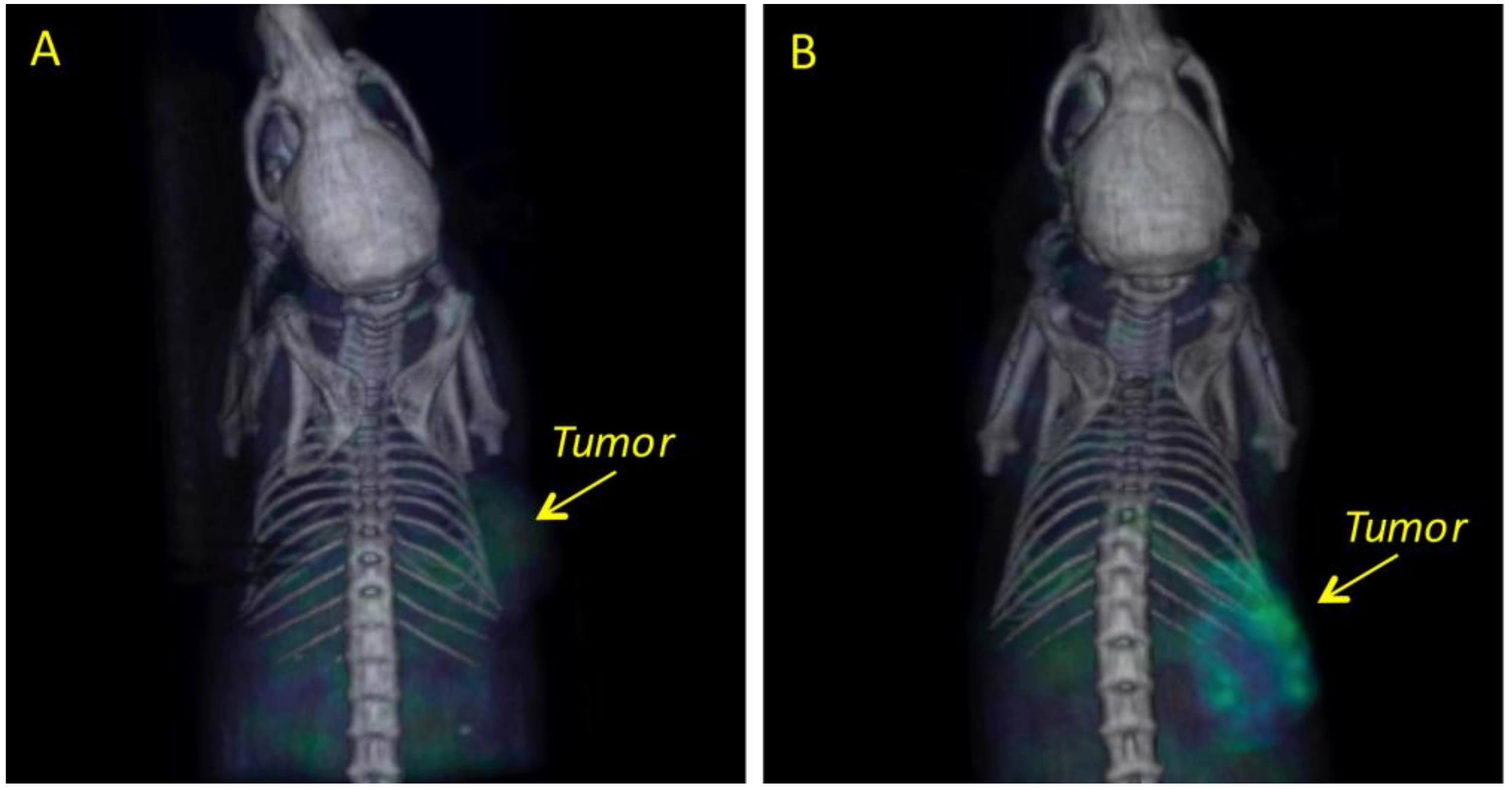
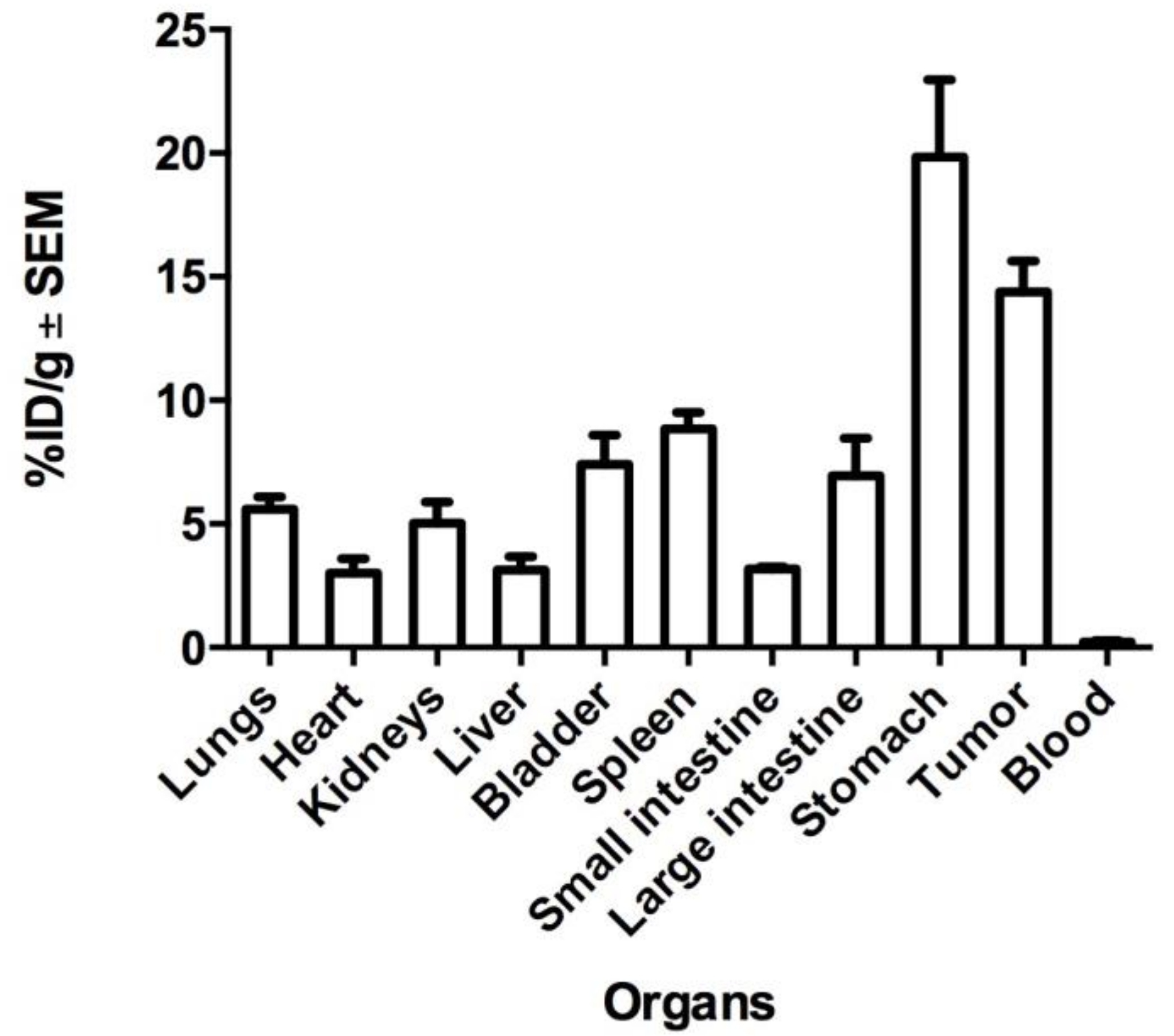
2.4. Biodistribution and Tumor Uptake in Mesothelioma Xenografts
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. Animals
4.3. Antibody Conjugation with DTPA
4.4. Nimotuzumab Integrity Test
4.5. Radiolabeling
4.6. In Vitro Binding Nimotuzumab Assay
4.7. Mesothelioma Xenografts
4.8. Biodistribution and Molecular Imaging Studies
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Astoul, P.; Roca, E.; Galateau-Salle, F.; Scherpereel, A. Malignant Pleural Mesothelioma: From the Bench to the Bedside. Respiration 2012, 83, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Escribano-Dueñas, A.M.; Vaquero-Barrios, J.M. Mesotelioma pleural maligno. An. Sist. Sanit. Navar. 2005, 28, 29–35. [Google Scholar] [Green Version]
- Yang, H.; Testa, J.R.; Carbone, M. Mesothelioma Epidemiology, Carcinogenesis and Pathogenesis. Curr. Treat. Options Oncol. 2009, 9, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Zucali, P.A.; Giaccone, G. Biology and management of malignant pleural mesothelioma. Eur. J. Cancer 2006, 42, 2706–2714. [Google Scholar] [CrossRef] [PubMed]
- Federico, R.; Adolfo, F.; Giuseppe, M.; Lorenzo, S.; Martino, D.T.; Anna, C.; Adriano, P.; Gino, C.; Francesca, R.; Matteo, C.; et al. Phase II trial of neoadjuvant pemetrexed plus cisplatin followed by surgery and radiation in the treatment of pleural mesothelioma. BMC Cancer 2013. [Google Scholar] [CrossRef] [PubMed]
- Goudar, R.K. Review of pemetrexed in combination with cisplatin for the treatment of malignant pleural mesothelioma. Ther. Clin. Risk Manag. 2008, 4, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Neumann, V.; Löseke, S.; Nowak, D.; Herth, F.J.F.; Tannapfel, A. Malignant pleural mesothelioma: Incidence, etiology, diagnosis, treatment, and occupational health. Dtsch. Arztebl. Int. 2013, 110, 319–326. [Google Scholar] [PubMed]
- Reck, M.; Stahel, R.A.; von Pawel, J.; Karthaus, M.; Korfee, S.; Serke, M.; Schuette, W.H.; Eschbach, C.; Fink, T.H.; Leschinger, M.I.; et al. Pemetrexed in the treatment of malignant mesothelioma: Results from an expanded access program in Germany. Respir. Med. 2010, 104, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pistolesi, M.; Rusthoven, J. Malignant Pleral Mesothelioma, Update, Current Management, and Newer Therapeutic Strategies. Chest 2004, 126, 1318–1329. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef] [PubMed]
- Kreitman, R.J.; Hassan, R.; Fitzgerald, D.J.; Pastan, I. Phase I Trial of Continuous Infusion Anti-Mesothelin Recombinant Immunotoxin SS1P. Clin Cancer Res. 2010, 15, 5274–5279. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; Medina, L.A.; Estrada-Lobato, E.; Ramírez-Tirado, L.A.; Mendoza-García, V.O.; de la Garza-Salazar, J. High liposomal doxorubicin tumour tissue distribution, as determined by radiopharmaceutical labelling with (99 m)Tc-LD, is associated with the response and survival of patients with unresectable pleural mesothelioma treated with a combination of liposomal. Cancer Chemother. Pharmacol. 2014, 74, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; López-Macías, D.; Mendoza-García, V.O.; Bacon-Fonseca, L.; Muñoz-Montaño, W.; Macedo-Pérez, E.O.; Muñiz-Hernández, S.; Blake-Cerda, M.; Corona-Cruz, J.F. A phase II trial of prolonged, continuous infusion of low-dose gemcitabine plus cisplatin in patients with advanced malignant pleural mesothelioma. Cancer Chemother. Pharmacol. 2014, 73, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Kotova, S.; Wong, R.M.; Cameron, R.B. New and emerging therapeutic options for malignant pleural mesothelioma: Review of early clinical trials. Cancer Manag. Res. 2015, 7, 51–63. [Google Scholar] [PubMed]
- Rea, F.; Favaretto, A.; Marulli, G.; Spaggiari, L.; Martino, D.T.; Ceribelli, A.; Paccagnella, A.; Crivellari, G.; Russo, F.; Ceccarelli, M.; et al. Phase II trial of neoadjuvant pemetrexed plus cisplatin followed by surgery and radiation in the treatment of pleural mesothelioma. J. Clin. Oncol. 2011. [Google Scholar] [CrossRef]
- Mendelsohn, J.; Baselga, J. Epidermal growth factor receptor targeting in cancer. Semin. Oncol. 2006, 33, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Shin, D.M. Monoclonal antibodies to target epidermal growth factor receptor-positive tumors. Cancer 2002, 94, 1593–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, D.P.; Raja, S.; Murthy, S.C. Malignant Pleural Mesothelioma. Curr. Oncol. Rep. 2011, 13, 259–264. [Google Scholar]
- Lee, A.Y.; Ras, D.J.; He, B.; Jablons, D.M. Update on the molecular biology of malignant mesothelioma. Cancer 2007, 109, 1454–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taffaro, M.L.; Salgia, R.; Johnson, B.E. Inhibition of Epidermal Growth Factor Receptor Signaling in Malignant Pleural Mesothelioma. Cancer Res. 2002, 62, 5242–5247. [Google Scholar]
- Ohta, Y.; Shridhar, V.; Bright, R.K.; Kalemkerian, G.P.; Du, W.; Carbone, M.; Watanabe, Y.; Pass, H.I. VEGF and VEGF type C play an important role in angiogenesis and lymphangiogenesis in human malignant mesothelioma tumours. Br. J. Cancer 1999, 81, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yewale, C.; Baradia, D.; Vhora, I.; Patil, S.; Misra, A. Epidermal growth factor receptor targeting in cancer: A review of trends and strategies. Biomaterials 2013, 34, 8690–8707. [Google Scholar] [CrossRef] [PubMed]
- Belli, C.; Anand, S.; Tassi, G.; Fennel, D.; Mutti, L. Translational therapies for malignant pleural mesothelioma. Expert Rev. Resp. Med. 2010, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Torres, L.A.; Perera, A.; Batista, J.F.; Hernández, A.; Crombet, T.; Ramos, M.; Eliac, N.; Marilyna, P.; Elvia, S.; Susanaa, R.; et al. Phase I/II clinical trial of the humanized anti-EGF-r monoclonal antibody h-R3 labelled with 99mTc in patients with tumour of epithelial origin. Nucl. Med. Commun. 2005, 26, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Ramos, T.C.; Figueredo, J.; Catala, M.; González, S.; Selva, J.C.; Cruz, T.M.; Toledo, C.; Silva, S.; Pestano, Y.; Ramos, M.; et al. Treatment of High-Grade Glioma Patients with the Humanized Anti-epidermal Growth Factor Receptor (EGFR) antibody h-R3. Cancer Biol. Ther. 2006, 5, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.; Crombet, T.; Leon, J.; Moreno, E. A view on EGFR-targeted therapies from the oncogene-addiction perspective. Front. Pharmacol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, W.; Yoshino, T.; Takahashi, T.; Okamoto, I.; Ueda, S.; Tsuya, A.; Bole, N.; Nishio, K.; Fukuoka, M.; Yamamoto, N.; et al. A phase I, pharmacokinetic and pharmacodynamic study of nimotuzumab in Japanese patients with advanced solid tumors. Cancer Chemother. Pharmacol. 2013, 72, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Shuptrine, C.W.; Surana, R.; Weiner, L.M. Monoclonal antibodies for the treatment of cancer. Semin. Cancer Biol. 2012, 22, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalsky, R.J.; Falen, S.W. Radiopharmaceuticals in Nuclear Pharmacy and Nuclear Medicine, 2nd ed.; American Pharmacists Association: Washington, DC, USA, 2004. [Google Scholar]
- Vera, D.R.B.; Eigner, S.; Beran, M.; Henke, K.E.; Laznickova, A.; Laznicek, M.; Melichar, F.; Chinol, M. Preclinical Evaluation of Lu-177-Nimotuzumab: A Potential Tool for Radioimmunotherapy of Epidermal Growth Factor Receptor-Overexpressing Tumors. Cancer Biother. Radiopharm. 2011, 26, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Fasih, A.; Fonge, H.; Cai, Z.; Leyton, J.V.; Tikhomirov, I.; Done, S.J.; Reilly, R.M. 111In-Bn-DTPA-nimotuzumab with/without modification with nuclear translocation sequence (NLS) peptides: An Auger electron-emitting radioimmunotherapeutic agent for EGFR-positive and trastuzumab (Herceptin)—resistant breast cancer. Breast Cancer Res. Treat. 2012, 135, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.; Velikyan, I.; Blom, E.; Ulin, J.; Monazzam, A.; Pahlman, L.; Micke, P.; Wanders, A.; Mcbride, W.; Goldenberg, D.M.; et al. In vitro autoradiography of carcinoembryonic antigen in tissue from patients with colorectal cancer using multifunctional antibody TF2 and (67/68Ga)-labeled haptens by pretargeting. Am. J. Nucl. Med. Mol. Imaging 2012, 2, 141–150. [Google Scholar] [PubMed]
- Agarwal, V.; Lind, M.J.; Cawkwell, L. Targeted epidermal growth factor receptor therapy in malignant pleural mesothelioma: Where do we stand? Cancer Treat. Rev. 2011, 37, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Motta, A.B.; Pinheiro, G.; Antonángelo, L.; Parra, E.R.; Monteiro, M.M.; Pereira, J.C.d.N.; Takagaki, T.; Filho, M.T.; Martins, S.; Capelozzi, V. Morphological aspects as prognostic factors in malignant mesothelioma: A study of 58 cases. J. Bras. Pneumol. 2006, 32, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Gaafar, R.; Bahnassy, A.; Abdelsalam, I.; Kamel, M.M.; Helal, A.; Abdel-Hamid, A.; Eldin, N.A.; Mokhtar, N. Tissue and serum EGFR as prognostic factors in malignant pleural mesothelioma. Lung Cancer. 2010, 70, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Hnatowich, D.J.; Childs, R.L.; Lanteigne, D.; Najafi, A. The preparation of DTPA-coupled antibodies radiolabeled with metallic radionuclides: An improved method. J. Immunol. Methods 1983, 65, 147–157. [Google Scholar] [CrossRef]
- Vergara, I.; Castillo, E.Y.; Romero-piña, M.E.; Torres-viquez, I.; Paniagua, D.; Boyer, L.V.; Alagón, A.; Medina, L.A. Biodistribution and Lymphatic Tracking of the Main Neurotoxin of Micrurus fulvius Venom by Molecular Imaging. Toxins 2016, 8, 85. [Google Scholar] [CrossRef] [PubMed]
- Mateo, C.; Moreno, E.; Amour, K.; Lombardero, J.; Harris, W.; Perez, R. Humanization of a mouse monoclonal antibody that blocks the epidermal growth factor receptor: Recovery of antagonistic activity. Immunotechnology 1997, 3, 71–81. [Google Scholar] [CrossRef]
- Sandana, G.; John, M.; Rose, C.; Takeuchi, S.; John, G.S.M.; Rose, C.; Takeuchi, S. Understanding Tools and Techniques in Protein Structure Prediction. Syst. Comput. Biol. Bioinform. Comput. Model. 2011. [Google Scholar] [CrossRef] [Green Version]
- Marjolijn, N.; Hooge, L.; Kosterink, M.G.W.; Perik, P.J.; Nijnuis, H.; Tran, L.; Bart, M.; Suurmeijer, A.J.H.; de Jong, S.; Jager, P.L.; et al. Preclinical characterisation of 111 In-DTPA-trastuzumab. Br. J. Pharmacol. 2004, 143, 99–106. [Google Scholar]
- Barta, P.; Laznickova, A.; Laznicek, M.; Vera, D.R.B.; Beran, M. Preclinical evaluation of radiolabelled nimotuzumab, a promising monoclonal antibody targeting the epidermal growth factor receptor. J. Label. Compd. Radiopharm. 2013, 56, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Haigler, H.; Ash, J.F.; Singer, S.J.; Cohen, S. Visualization by fluorescence of the binding and internalization of epidermal growth factor in human carcinoma cells A-431. Proc. Natl. Acad. Sci. USA 1978, 75, 3317–3321. [Google Scholar] [CrossRef] [PubMed]
- Kameswaran, M.; Samuel, G.; Dev Sarma, H.; Shinde, S.N.; Dash, A.; Venkatesh, M. 131I-Nimotuzumab—A potential radioimmunotherapeutic agent in treatment of tumors expressing EGFR. Appl. Radiat. Isot. 2015, 102, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Berrozpe, J.D.; Lanao, J.M.; Delfina, J.M.P. Biofarmacia y Farmacocinética Vol: II; Editorial Sintesis: Madrid, Spain, 2001. [Google Scholar]
- Iznaga Escobar, N.; Morales, A.M.; Ducongé, J.; Torres, I.C.; Fernández, E.; Gómez, J.A. Pharmacokinetics, biodistribution and dosimetry of 99mTc-labeled anti-human epidermal growth factor receptor humanized monoclonal antibody R3 in rats. Nucl. Med. Biol. 1998, 25, 17–23. [Google Scholar] [CrossRef]
- Chopra, A. 177Lu-Labeled h-R3 (nimotuzumab), a humanized monoclonal antibody targeting the external domain of the epidermal growth factor receptor. Mol. Imaging Contrast Agent Database 2012. [Google Scholar] [CrossRef]
- Levêque, D.; Wisniewski, S.; Jehl, F. Pharmacokinetics of therapeutic monoclonal antibodies used in oncology. Anticancer Res. 2005, 25, 2327–2343. [Google Scholar] [PubMed]
- Keizer, R.J. Pharmacometrics in Early Clinical Drug Development. Ph.D Thesis, Utrecht University, Amsterdam, The Netherlands, 1980. [Google Scholar]
- Konikowski, T.; Glenn, H.J.; Haynie, T.P. Kinetics of 67Ga compunds in brain sarcomas and kidneys of mice. J. Nucl. Med. 1972, 14, 164–171. [Google Scholar]
- Calvo, E.; Walko, C.; Dees, E.C. Pharmacogenomics, Pharmacokinetics, and Pharmacodynamics in the Era of Targeted Therapies. Am. Soc. Clin. Oncol. Educ. 2016. [Google Scholar] [CrossRef] [PubMed]
- Meibohm, B.; Derendorf, H. Pharmacokinetics and Pharmacodynamics of Biotech Drugs. Rev. Cell Biol. Mol. 2006. [Google Scholar] [CrossRef]
- Ramos-Suzarte, M.; Pintado, A.P.; Mesa, N.R.; Oliva, J.P.; Iznaga-Escobar, N.; Aroche, L.T.; Pimentel, G.; Gonzalez, M.; Rodriguez, O.T.; Crombet, R.T.; et al. Diagnostic Efficacy and Safety of 99m Tc-Labeled Monoclonal Antibody Ior c5 in Patients with Colorectal and Anal Carcinomas ES SC RIB. Cancer Biol. Ther. 2007, 6, 1–8. [Google Scholar] [CrossRef]
Sample Availability: Samples of the compounds are not available from the authors. |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time (h) | % Tumor | Tumor/Liver |
|---|---|---|
| 1 | 1.52 ± 0.15 | 6.61 ± 0.42 |
| 12 | 1.44 ± 0.23 | 6.21 ± 2.26 |
| 24 | 1.82 ± 0.18 | 8.46 ± 2.48 |
| 48 | 1.47 ± 0.31 | 5.71 ± 1.95 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izquierdo-Sánchez, V.; Muñiz-Hernández, S.; Vázquez-Becerra, H.; Pacheco-Yepez, J.; Romero-Piña, M.E.; Arrieta, O.; Medina, L.A. Biodistribution and Tumor Uptake of 67Ga-Nimotuzumab in a Malignant Pleural Mesothelioma Xenograft. Molecules 2018, 23, 3138. https://doi.org/10.3390/molecules23123138
Izquierdo-Sánchez V, Muñiz-Hernández S, Vázquez-Becerra H, Pacheco-Yepez J, Romero-Piña ME, Arrieta O, Medina LA. Biodistribution and Tumor Uptake of 67Ga-Nimotuzumab in a Malignant Pleural Mesothelioma Xenograft. Molecules. 2018; 23(12):3138. https://doi.org/10.3390/molecules23123138
Chicago/Turabian StyleIzquierdo-Sánchez, Vanessa, Saé Muñiz-Hernández, Héctor Vázquez-Becerra, Judith Pacheco-Yepez, Mario E. Romero-Piña, Oscar Arrieta, and Luis Alberto Medina. 2018. "Biodistribution and Tumor Uptake of 67Ga-Nimotuzumab in a Malignant Pleural Mesothelioma Xenograft" Molecules 23, no. 12: 3138. https://doi.org/10.3390/molecules23123138