Caustic Ingestion in the Elderly: Influence of Age on Clinical Outcome

 and
and
Abstract
:1. Introduction
2. Results
2.1. Demographic and Caustic Injury Description
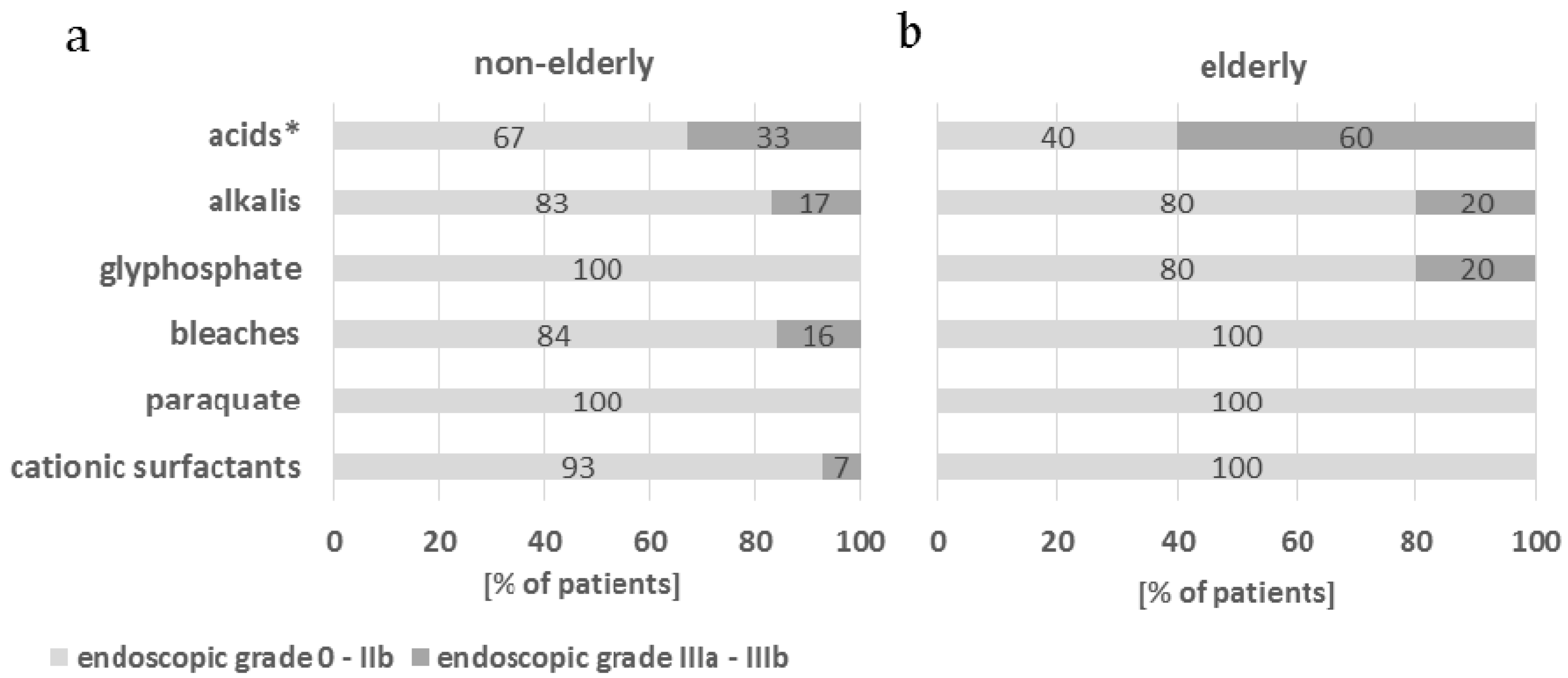
2.2. Chemical Origin of the Caustic Substances and Their Corrosive Potential
2.3. Complications and Clinical Outcome
3. Discussion
4. Materials and Methods
4.1. Main Characteristics of Chemical Substances Involved
4.2. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mrazova, K.; Navratil, T.; Pelclova, D. Consequences of ingestions of potentially corrosive cleaning products, one-year follow-up. Int. J. Electrochem. Sci. 2012, 7, 1734–1748. [Google Scholar]
- Plackova, S.; Placha, K.; Caganova, B.; Bibza, J. A retrospective analysis of caustic ingestions in Slovakia. Clin. Toxicol. 2013, 51, 313–314. [Google Scholar]
- Cheng, H.T.; Cheng, C.L.; Lin, C.H.; Tang, J.H.; Chu, Y.Y.; Liu, N.J.; Chen, P.C. Caustic ingestion in adults: The role of endoscopic classification in predicting outcome. BMC Gastroenterol. 2008, 8, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Contini, S.; Scarpignato, C. Caustic injury of the upper gastrointestinal tract: A comprehensive review. World J. Gastroenterol. 2013, 19, 3918–3930. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.S.; Tai, W.C.; Hu, M.L.; Wu, K.L.; Chiu, Y.C. Predicting the progress of caustic injury to complicated gastric outlet obstruction and esophageal stricture using modified endoscopic mucosal injury grading scale. Biomed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Koschny, R.; Herceg, M.; Stremmel, W.; Eisenbach, C. Fatal course of a suicidal intoxication with hydrochloric acid. Case Rep. Gastroenterol. 2013, 7, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Caganova, B.; Foltanova, T.; Plackova, S.; Placha, K.; Bibza, J.; Puchon, E.; Ondriasova, E.; Batora, I. Caustic effects of chemicals: Risk factors for complications and mortality in acute poisoning. Monatsh. Chem. 2017, 148, 497–503. [Google Scholar] [CrossRef]
- Chibishev, A.; Simonovska, N.; Bozinovska, C.; Pereska, Z.; Smokovski, I.; Glasnovic, M. Respiratory complication from acute corrosive poisonings in adults. Mater. Sociomed. 2014, 26, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Kluger, Y.; Ishay, O.B.; Sartelli, M.; Katz, A.; Ansaloni, L.; Gomez, C.A.; Biffl, W.; Catena, F.; Fraga, G.P.; Di Saverio, S.; et al. Caustic ingestion management: World society of emergency surgery preliminary survey of expert opinion. World J. Emerg. Surg. 2015, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Cabral, C.; Chirica, M.; de Chaisemartin, C.; Gornet, J.M.; Munoz-Bongrand, N.; Halimi, B.; Cattan, P.; Sarfati, E. Caustic injuries of the upper digestive tract: A population observational study. Surg. Endosc. 2012, 26, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, H.; Ozokutan, B.H.; Gündüz, F.; Gözen, A. Gastric perforation after corrosive ingestion. Pediatr. Surg. Int. 2011, 27, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Chibishev, A.; Simonovska, N.; Shikole, A. Post-corrosive injuries of upper gastrointestinal tract. Prilozi 2010, 31, 297–316. [Google Scholar] [PubMed]
- European Network for Safety among Elderly (EUNESE). 2012. Available online: www.injuryobservatory.net/wp-content/uploads/2012/08/SelfOlder-Guide-Prevention-of-accidental-poison.pdf (accessed on 18 August 2017).
- Afzali, S.; Seifrabiei, M.A.; Taheri, S.K.; Pourabdollah, J. Acute poisoning in elderly; a five-year study (2008–2013) in Hamadan. Iran. Asia Pac. J. Med. Toxicol. 2015, 4, 143–146. [Google Scholar]
- World Health Organization. Health statistics and information systems: Definition of an older or elderly person. 2015. Available online: http://www.who.int/healthinfo/survey/ageingdefnolder/en/ (accessed on 3 August 2015).
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2013. Available online: http://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2013.pdf (accessed on 18 August 2017).
- Zargar, S.A.; Kochhar, R.; Mehta, S.; Mehta, S.K. The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest. Endosc. 1991, 37, 165–169. [Google Scholar] [CrossRef]
- Klein-Schwartz, W.; Oderda, G.M. Poisoning in the elderly. Epidemiological, clinical and management considerations. Drugs Aging 1991, 1, 67–89. [Google Scholar] [CrossRef] [PubMed]
- Ferraris, V.A. Treatment of caustic esophageal injury: The source of knowledge is experience. J. Thorac. Cardiovasc. Surg. 2016, 152, 1386–1387. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.M.; Liu, N.J.; Pai, B.C.; Liu, Y.H.; Tsai, M.H.; Lee, C.S.; Chu, Y.Y.; Lin, C.C.; Chiu, C.T.; Cheng, H.T. The role of age in predicting the outcome of caustic ingestion in adults: A retrospective analysis. BMC Gastroenterol. 2011, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Cowan, T.; Foster, R.; Isbister, G.K. Acute and chronic oesophageal injury following caustic ingestions in a 25-year cohort. Clin. Toxicol. 2016, 54, 344–359. [Google Scholar] [CrossRef]
- Rollin, M.; Jaulim, A.; Vaz, F.; Sandhu, G.; Wood, S.; Birchall, M.; Dawas, K. Caustic ingestion injury of the upper aerodigestive tract in adults. Ann. R. Coll. Surg. Engl. 2015, 97, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Peroni, G.; Miccono, A.; Guerriero, F.; Guido, D.; Perna, S. Nutritional management in an elderly man with esophageal and gastric necrosis after caustic soda ingestion: A case report. Ther. Clin. Risk Manag. 2016, 12, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Chirica, M.; Munoz-Bongrand, N.; Sarfati, E.; Cattan, P. Emergency Management of Caustic Injuries. In Acute Care Surgery Handbook, 1st ed.; Di Saverio, S., Catena, F., Ansaloni, L., Coccolini, F., Velmahos, G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; Volume 1, pp. 471–483. ISBN 978-3-319-15340-7. [Google Scholar]
- Bicakci, U.; Tander, B.; Deveci, G.; Rizalar, R.; Ariturk, E.; Bernay, F. Minimally invasive management of children with caustic ingestion: Less pain for patients. Pediatr. Surg. Int. 2010, 26, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Lin, J.L.; Huang, W.H.; Weng, C.H.; Lee, S.Y.; Hsu, C.W.; Chen, K.H.; Wang, I.K.; Liang, C.C.; Chang, C.T.; et al. Spectrum of corrosive esophageal injury after intentional paraquat or glyphosate-surfactant herbicide ingestion. Int. J. Gen. Med. 2013, 6, 677–683. [Google Scholar] [CrossRef] [PubMed]
- TOXBASE—National Poisons Information Service, Edinburgh, UK, 2017. Available online: www.toxbase.org (accessed on 13 October 2017).
- Yen, T.H.; Lin, J.L.; Lin-Tan, D.T.; Hsu, C.W.; Weng, C.H.; Chen, Y.H. Spectrum of corrosive esophageal injury after intentional paraquat ingestion. Am. J. Emerg. Med. 2010, 28, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Olson, K.R. Poisoning and Drug Overdose, 6th ed.; The McGraw-Hill Companies, Inc.: San Francisco, CA, USA, 2012; p. 815. ISBN 976-0-07-166833-0. [Google Scholar]
- Poisindex, Micromedex Healthcare Series, Greenwood Village, CO, USA, 2017; Volume 174.
- Lupa, M.; Magne, J.; Guarisco, J.L.; Amedee, R. Update on the diagnosis and treatment of caustic ingestion. Ochsner. J. 2009, 9, 54–59. [Google Scholar] [PubMed]
- Poley, J.W.; Steyerberg, E.W.; Kuipers, E.J.; Dees, J.; Hartmans, R.; Tilanus, H.W.; Siersema, P.D. Ingestion of acid and alkaline agents: outcome and prognostic value of early upper endoscopy. Gastrointest. Endosc. 2004, 60, 372–377. [Google Scholar] [CrossRef]
- Rodrigues, G.; Prabhu, R. Harpic (hydrochloric acid) ingestion causing ‘isolated’ gastric fundus perforation. Span. J. Surg. Res. 2014, 17, 19–21. [Google Scholar]
- Smędra-Kaźmirska, A.; Kędzierski, M.; Barzdo, M.; Jurczyk, A.; Szram, S.; Berent, J. Accidental intoxication with hydrochloric acid and hydrofluoric acid mixture. Arch. Med. Sadowej. Kryminol. 2014, 64, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Sanchez, A.; Carrion, G.; Barreiro, A.; Ortiz, C.; De Fuenmayor, M.L.; Gimeno, M.; Ponferrada, A.; Martin, S.; Aldeguer, M. Massive gastric necrosis from hydrochloric acid ingestion. Rev. Esp. Enferm. Dig. 2009, 101, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Jurisic, D.; Samardzic, J.; Hreckovski, B.; Bano, V.; Jakovina, T.; Held, R. Massive necrosis of the upper gastrointestinal tract with acute gastric perforation and metabolic acidosis after hydrochloric acid (HCl) ingestion. Zentralbl. Chir. 2011, 136, 289–290. [Google Scholar] [CrossRef] [PubMed]
- Sari, I.; Zengin, S.; Pehlivan, Y.; Davutoglu, V.; Yildirim, C. Fatal myocardial infarction after hydrochloric acid ingestion in a suicide attempt. Am. J. Emerg. Med. 2008, 26, 634.e5–634.e7. [Google Scholar] [CrossRef] [PubMed]
- European Chemical Agency (ECHA). 2017. Available online: https://echa.europa.eu/regulations/reach/registration (accessed on 18 August 2017).
- Caganova, B.; Plackova, S. Vital role for the National Toxicological Information Centre. Eur. J. Hosp. Pharm. 2009, 15, 45. [Google Scholar]
- Tovar, R.; Leikin, J.B. Irritants and corrosives. Emerg. Med. Clin. N. Am. 2015, 33, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Giampreti, A.; Chiara, F.; Lonati, D.; Petrolini, V.M.; Vecchio, S.; Aloise, M.; Flachi, D.; Rognoni, C.; Manzo, L.; Locatelli, C.A. Caustic effects due to sodium hypochlorite ingestion: Toxicological properties, clinical manifestations and esophago-gastro-duodenoscopy. Clin. Toxicol. 2013, 51, 310–311. [Google Scholar]
Sample Availability: Samples of the compounds are not available from the authors. |

{kind=link}
| Variables | Total (n = 176) | Non-Elderly (<60 years, n = 115) | Elderly (≥60 years, n = 61) |
|---|---|---|---|
| Mean age (years) | 51.8 (19–87) | 43.0 (19–59) | 68.8 (60–87) |
| Gender | |||
| Male (%) | 124 (70.5) | 82 (71.3) | 42 (68.9) |
| Female (%) | 52 (29.5) | 33 (28.7) | 19 (31.1) |
| Circumstance | |||
| Accident (%) | 108 (61.4) | 77 (67.0) | 31 (50.8) |
| Intention (%) | 63 (35.8) | 36 (31.3) | 27 (44.3) |
| Missing (%) | 5 (2.8) | 2 (1.7) | 3 (4.9) |
| Endoscopic grade | |||
| 0 (%) | 6 (3.4) | 4 (3.5) | 2 (3.3) |
| I (%) | 51 (29.0) | 34 (29.6) | 17 (27.9) |
| IIa (%) | 65 (36.9) | 47 (40.9) | 18 (29.5) |
| IIb (%) | 9 (5.1) | 6 (5.2) | 3 (4.9) |
| IIIa (%) | 19 (10.8) | 10 (8.7) | 9 (14.8) |
| IIIb (%) | 20 (11.4) | 11 (9.6) | 9 (14.8) |
| Missing (%) 1 | 6 (3.4) | 3 (2.6) | 3 (4.9) |
| Location of caustic injury | |||
| Oropharyng (%) | 103 (58.5) | 70 (60.9) | 33 (54.1) |
| Oesophagus (%) | 98 (55.7) | 59 (51.3) | 39 (63.9) |
| Stomach (%) | 98 (55.7) | 63 (54.8) | 35 (57.4) |
| Duodenum (%) | 33 (18.8) | 20 (17.4) | 13 (21.3) |
| Caustic Substance | Total (%) n = 176 | Non-Elderly (<60 years, n = 115) | Elderly (≥ 60 years, n = 61) | p |
|---|---|---|---|---|
| Acids (%) | 58 (33.0) | 32 (27.8) | 26 (42.6) | 0.047 |
| HCl (%) | 24 (13.6) | 10 (8.7) | 14 (23.0) | 0.009 |
| H2SO4 (%) | 13 (7.4) | 6 (5.2) | 7 (11.5) | 0.131 |
| H3PO4 (%) | 6 (3.4) | 4 (3.5) | 2 (3.3) | 1.000 |
| HNO3 (%) | 2 (1.1) | 2 (1.7) | 0 (0.0) | 0.544 |
| Alkalis (%) | 46 (26.1) | 36 (31.3) | 10 (16.4) | 0.032 |
| NaOH (%) | 25 (14.2) | 20 (17.4) | 5 (8.2) | 0.096 |
| Na2SiO3 (%) | 9 (5.1) | 6 (5.2) | 3 (4.9) | 1.000 |
| KOH (%) | 4 (2.3) | 3 (2.6) | 1 (1.6) | 1.000 |
| Bleaches (%) | 28 (15.9) | 19 (16.5) | 9 (14.8) | 0.760 |
| Chlorine-based bleaches (%) | 20 (11.4) | 14 (12.2) | 6 (9.8) | 0.642 |
| Oxygen-based bleaches (%) | 8 (4.5) | 5 (4.3) | 3 (4.9) | 1.000 |
| Cationic surfactants (%) | 20 (11.4) | 15 (13.0) | 5 (8.2) | 0.335 |
| Glyphosate 1 (%) | 9 (5.1) | 4 (3.5) | 5 (8.2) | 0.279 |
| Paraquat 2, Diquat 3 (%) | 8 (4.5) | 5 (4.3) | 3 (4.9) | 1.000 |
| Others (%) | 7 (4.0) | 4 (3.5) | 3 (4.9) | 0.695 |
| Parameter | Total (n = 176) | Non-Elderly (≤60 years, n = 115) | Elderly (>60 years, n = 61) | p |
|---|---|---|---|---|
| Respiratory complications (%) | 39 (22.2) | 20 (17.4) | 19 (31.1) | 0.037 |
| Pneumonia (%) | 14 (8.0) | 7 (6.1) | 7 (11.5) | 0.209 |
| RF 1 (%) | 35 (19.9) | 18 (15.7) | 17 (27.9) | 0.050 |
| GI 2 complications (%) | 38 (21.6) | 25 (21.7) | 13 (21.3) | 0.948 |
| Bleeding (%) | 24 (13.6) | 18 (15.7) | 6 (9.8) | 0.285 |
| Perforation (%) | 15 (8.5) | 9 (7.8) | 6 (9.8) | 0.649 |
| Peritonitis/Mediastinitis (%) | 14 (8.0) | 6 (5.2) | 8 (13.1) | 0.065 |
| Fistula (%) | 2 (1.1) | 0 (0.0) | 2 (3.3) | 0.119 |
| Stricture (%) | 2 (1.1) | 2 (1.7) | 0 (0.0) | 0.300 |
| Leukocytosis (%) | 32 (18.2) | 11 (9.6) | 21 (34.4) | 0.001 |
| Antibiotic usage (%) | 95 (54.0) | 56 (48.7) | 39 (63.9) | 0.050 |
| Mean length of hospital stay (%) | 6.0 (1–45) (n = 149) | 4.8 (1–22) (n = 97) | 8.2 (1–45) (n = 52) | 0.003 |
| Mortality (%) | 27 (15.3) | 13 (11.3) | 14 (23.0) | 0.041 |
| Caustic Substance | OR | 95% CI | p |
|---|---|---|---|
| Acids (%) | 9.130 | 2.766–30.128 | 0.001 |
| HCl (%) | 10.694 | 2.546–44.919 | 0.001 |
| Alkalis (%) | 0.664 | 0.154–2.874 | 0.729 |
| NaOH (%) | 1.111 | 0.171–7.203 | 1.000 |
| Glyphosate (%) | 1.111 | 0.171–7.203 | 1.000 |
| Paraquat (%) | 0.818 | 0.070–9.561 | 1.000 |
| Caustic Substance | Fatal Outcome (n = 176) | Non-Elderly (≤60 years, n = 115) | Elderly (>60 years, n = 61) |
|---|---|---|---|
| Acids (%) | 22 (12.5) | 11 (9.6) | 11 (18.0) |
| HCl (%) | 14 (8.0) | 7 (6.1) | 7 (11.5) |
| H2SO4 (%) | 4 (2.3) | 0 (0.0) | 4 (6.6) |
| HNO3 (%) | 2 (1.1) | 2 (1.7) | 0 (0.0) |
| Unidentified acid (%) | 2 (1.1) | 2 (1.7) | 0 (0.0) |
| Glyphosate (%) | 2 (1.1) | 0 (0.0) | 2 (3.3) |
| Paraquat (%) | 3 (1.7) | 2 (1.7) | 1 (1.6) |
| Total (%) | 27 (15.3) | 13 (11.3) | 14 (23.0) |
| Caustic Substance | OR | 95% CI | p |
|---|---|---|---|
| Acid (%) | 7.822 | 1.898–32.241 | 0.002 |
| HCl (%) | 5.714 | 1.527–21.391 | 0.006 |
| Glyphosate (%) | 2.444 | 0.366–16.337 | 0.322 |
| Paraquat (%) | 1.731 | 0.145–20.637 | 0.549 |
| Grade 0 | Normal examination |
| Grade I | Edema and hyperemia of the mucosa |
| Grade IIa | Superficial ulceration, erosions, friability, blisters, exudates, hemorrhages, whitish membranes |
| Grade IIb | Grade IIa plus deep discrete or circumferential ulcerations |
| Grade IIIa | Small scattered areas of multiple ulceration and areas of necrosis with brown-black or greyish discoloration |
| Grade IIIb | Extensive necrosis |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caganova, B.; Foltanova, T.; Puchon, E.; Ondriasova, E.; Plackova, S.; Fazekas, T.; Kuzelova, M. Caustic Ingestion in the Elderly: Influence of Age on Clinical Outcome. Molecules 2017, 22, 1726. https://doi.org/10.3390/molecules22101726
Caganova B, Foltanova T, Puchon E, Ondriasova E, Plackova S, Fazekas T, Kuzelova M. Caustic Ingestion in the Elderly: Influence of Age on Clinical Outcome. Molecules. 2017; 22(10):1726. https://doi.org/10.3390/molecules22101726
Chicago/Turabian StyleCaganova, Blazena, Tatiana Foltanova, Erik Puchon, Elena Ondriasova, Silvia Plackova, Tomas Fazekas, and Magdalena Kuzelova. 2017. "Caustic Ingestion in the Elderly: Influence of Age on Clinical Outcome" Molecules 22, no. 10: 1726. https://doi.org/10.3390/molecules22101726