Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to the 10-Valent Pneumococcal Conjugate Vaccine (PCV10) in Italy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
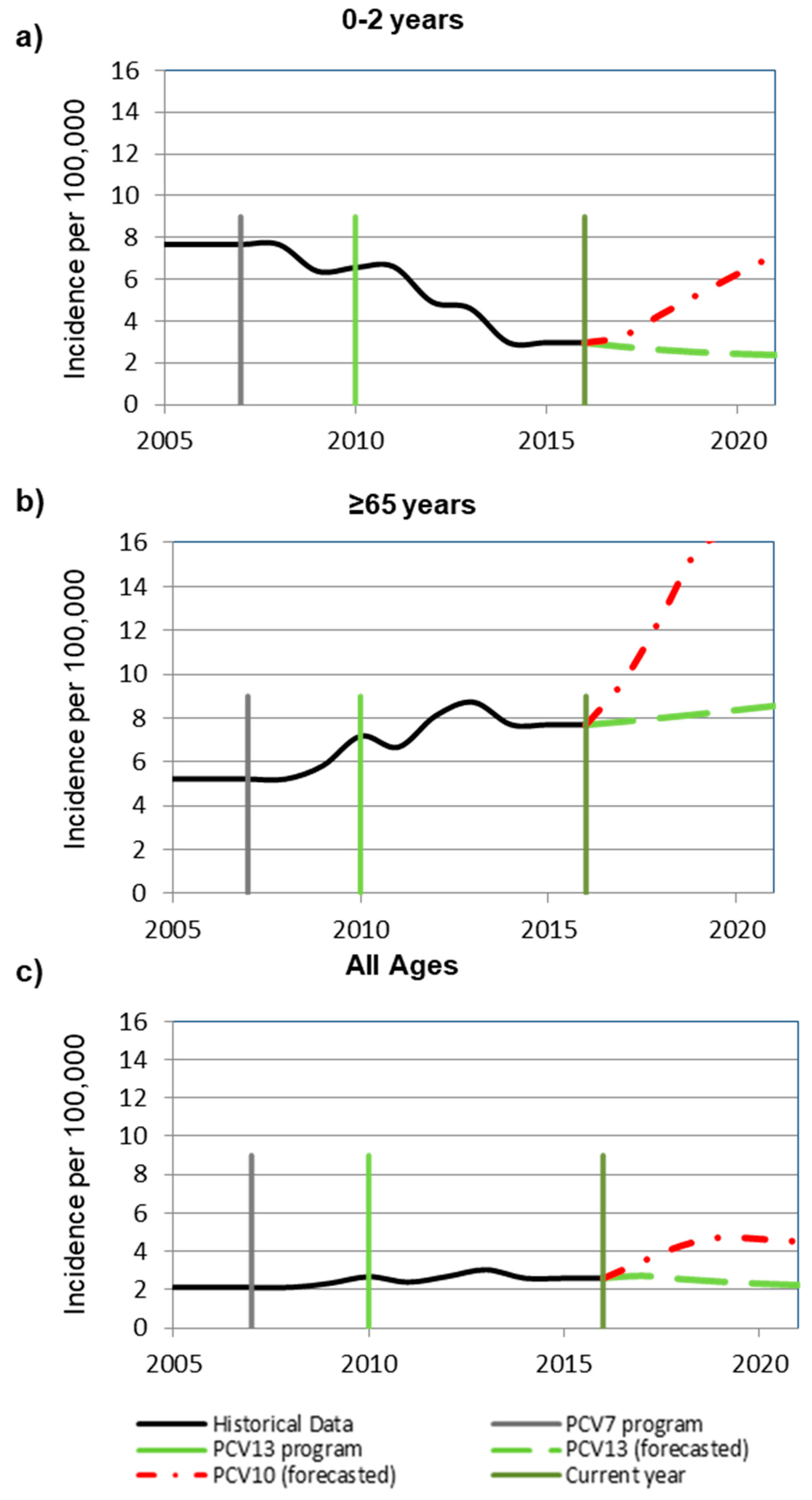
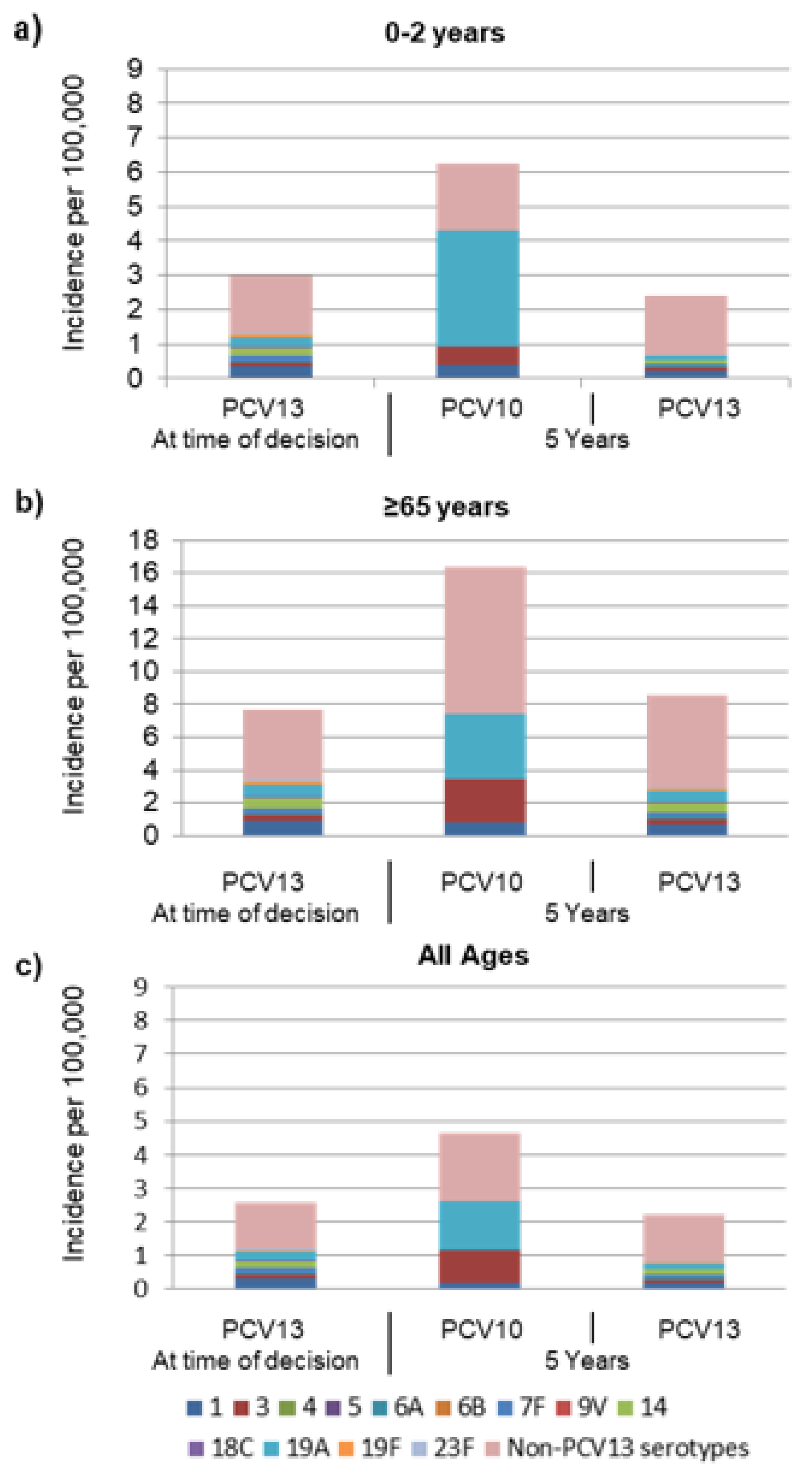
2.1. Epidemiological Results
2.2. Base Case Cost-Effectiveness Analysis Results
2.3. Sensitivity Results
3. Discussion
4. Materials and Methods
4.1. Model Design
4.2. Model Assumptions
4.3. Epidemiologic Setting and Inputs
4.4. Economic Input
4.5. Utilities
4.6. Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Pneumococcal vaccines WHO position paper—2012. Wkly. Epidemiol. Rec. 2012, 87, 129–144. [Google Scholar]
- Hausdorff, W.P.; Feikin, D.R.; Klugman, K.P. Epidemiological differences among pneumococcal serotypes. Lancet Infect. Dis. 2005, 5, 83–93. [Google Scholar] [CrossRef]
- Tsai, Y.H.; Hsieh, M.J.; Chang, C.J.; Wen, Y.W.; Hu, H.C.; Chao, Y.N.; Huang, Y.C.; Yang, C.T.; Huang, C.C. The 23-valent pneumococcal polysaccharide vaccine is effective in elderly adults over 75 years old-Taiwan’s PPV vaccination program. Vaccine 2015, 3, 2897–2902. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.J.; Waight, P.A.; George, R.C.; Slack, M.P.; Miller, E. Impact and effectiveness of 23-valent pneumococcal polysaccharide vaccine against invasive pneumococcal disease in the elderly in England and Wales. Vaccine 2012, 30, 6802–6808. [Google Scholar] [CrossRef]
- Wang, Y.; Li, J.; Wang, Y.; Gu, W.; Zhu, F. Effectiveness and practical uses of 23-valent pneumococcal polysaccharide vaccine in healthy and special populations. Hum. Vaccines Immunother. 2018, 14, 1003–1012. [Google Scholar] [CrossRef] [Green Version]
- Htar, M.T.T.; Stuurman, A.L.; Ferreira, G.; Alicino, C.; Bollaerts, K.; Paganino, C.; Reinert, R.R.; Schmitt, H.J.; Trucchi, C.; Vestraeten, T.; et al. Effectiveness of pneumococcal vaccines in preventing pneumonia in adults, a systematic review and meta-analyses of observational studies. PLoS ONE 2017, 12, e0177985. [Google Scholar]
- Ministero della Salute. DGPRV 0024720-P-27/05/2010. Indicazioni in merito alla somministrazione del vaccino antipneumococcico Prevenar 13 in età pediatrica. Prot n. 111432/72AF. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwjJy_qyrtjnAhXizIsBHaumC8UQFjAAegQIBhAB&url=https%3A%2F%2Fwww.fimpcalabria.org%2Fpublic%2Fvaccinazioni%2Findicazioni%2520in%2520merito%2520alla%2520somministrazione%2520del%2520vaccino%2520antipneumococcico%2520prevenar%252013%2520in%2520et%25C3%25A0%2520pediatrica%2520(2).pdf&usg=AOvVaw3c-X61f4k77BZQmseiR3VL (accessed on 3 June 2010).
- Centro Nazionale di Epidemiologia. Dati e Evidenze Disponibili per L’utilizzo dei Vaccini Anti-Pneumococcici nei Soggetti a Rischio di Qualsiasi età e per L’eventuale Ampliamento Dell’offerta ai Soggetti Anziani. Available online: http://www.epicentro.iss.it/vaccini/pdf/Dati%20e%20evidenze%20vaccini%20antipneumococcici.pdf (accessed on 20 March 2019).
- Epicentro: Il Portale Dell’epidemiologia per la Sanità Pubblica. Le Vaccinazioni in Italia. Copertura Vaccinale. Available online: http://www.epicentro.iss.it/vaccini/dati_ita (accessed on 1 April 2019).
- Italian Minister of Health. National Prevention Immunization Plan. Available online: www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 1 April 2019).
- Castiglia, P. Recommendations for pneumococcal immunization outside routine childhood immunization programs in Western Europe. Adv. Ther. 2014, 31, 1011–1044. [Google Scholar] [CrossRef] [Green Version]
- Orsi, A.; Ansaldi, F.; Trucchi, C.; Rosselli, R.; Icardi, G. Pneumococcus and the elderly in Italy: A summary of available evidence regarding carriage, clinical burden of lower respiratory tract infections and on-field effectiveness of PCV13 vaccination. Int. J. Mol. Sci. 2016, 17, 1140. [Google Scholar] [CrossRef] [Green Version]
- Desmet, S.; Verhaegen, J.; Van Ranst, M.; Peetermans, W.; Lagrou, K. Switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10: A defendable approach? Lancet Infect. Dis. 2018, 18, 830–831. [Google Scholar] [CrossRef] [Green Version]
- Izurieta, P.; Breuer, T. Interpretation of the switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10 in Belgium. Lancet Infect. Dis. 2018, 18, 831–832. [Google Scholar] [CrossRef] [Green Version]
- Camilli, R.; D’Ambrosio, F.; Del Grosso, M.; Pimentel de Araujo, F.; Caporali, M.G.; Del Manso, M.; Gherardi, G.; D’Ancona, F.; Pantosti, A.; Pneumococcal Surveillance Group. Impact of pneumococcal conjugate vaccine (PCV7 and PCV13) on pneumococcal invasive diseases in Italian children and insight into evolution of pneumococcal population structure. Vaccine 2017, 35, 4587–4593. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.; Wasserman, M.; Jadavi, T.; Postma, M.; Breton, M.C.; Peloquin, F.; Earnshaw, S.; McDade, C.; Sings, H.; Farkouh, R. Clinical and economic impact of a potential switch from 13-valent to 10-valent pneumococcal conjugate infant vaccination in Canada. Infect. Dis. Ther. 2018, 7, 353–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, M.; Palacios, M.G.; Grajales, A.G.; Baez-Revueltas, F.B.; Wilson, M.; McDade, C.; Farkouh, R. Modeling the sustained use of the 13-valent pneumococcal conjugate vaccine compared to switching to the 10-valent vaccine in Mexico. Hum. Vaccines Immunother. 2019, 15, 560–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castañeda-Orjuela, C.; De la Hoz-Restrepo, F. How cost effective is switching universal vaccination from PCV10 to PCV13? A case study from a developing country. Vaccine 2018, 36, 5766–5773. [Google Scholar] [CrossRef] [PubMed]
- Song, J.H. Advanvces in pneumococcal antibiotic resistence. Exp. Rev. Respir. Med. 2013, 7, 491–498. [Google Scholar] [CrossRef]
- Matanock, A.; Lee, G.; Gierke, R.; Kobayashi, M.; Leidner, A.; Pilishvili, T. Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 Years: Updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1069–1075. [Google Scholar] [CrossRef] [Green Version]
- Castiglia, P.; Pradelli, L.; Castagna, S.; Freguglia, V.; Palù, G.; Esposito, S. Overall effectiveness of pneumococcal conjugate vaccines: An economic analysis of PHiD-CV and PCV-13 in the immunization of infants in Italy. Hum. Vaccines Immunother. 2017, 13, 2307–2315. [Google Scholar] [CrossRef]
- Pastor, L.; Sings, H.; Hilton, B.; Kohli, M.; Kruse, M.; Wasserman, M. (Eds.) A systematic review of pneumococcal conjugate vaccine (PCV) impact on acute otitis media (OM) and nasopharyngeal carriage (NP) due to nontypeable haemophilus influenza (NTHi). In Proceedings of the 35th Annual Meeting of the European Society for Paediatric Infectious Diseases, Madrid, Spain, 23–27 May 2017. [Google Scholar]
- Wasserman, M.; Sings, H.L.; Jones, D.; Pugh, S.; Moffatt, M.; Farkouh, R. Review of vaccine effectiveness assumptions used in economic evaluations of infant pneumococcal conjugate vaccine. Expert Rev. Vaccines 2018, 17, 71–78. [Google Scholar] [CrossRef]
- Ansaldi, F.; de Florentiis, D.; Canepa, P.; Ceravolo, A.; Rappazzo, E.; Iudici, R.; Icardi, G.; Durando, P. Carriage of Streptoccoccus pneumoniae in healthy adults aged 60 years or over in a population with very high and long-lasting pneumococcal conjugate vaccine coverage in children: Rationale and perspectives for PCV13 implementation. Hum. Vaccines Immunother. 2013, 9, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Ansaldi, F.; de Florentiis, D.; Canepa, P.; Zancolli, M.; Martini, M.; Orsi, A.; Durando, P.; Icardi, G. Carriage of Streptoccoccus pneumoniae 7 years after implementation of vaccination program in a population with very high and long-lasting coverage, Italy. Vaccine 2012, 30, 2288–2294. [Google Scholar] [CrossRef]
- Bloom, D.E.; Black, S.; Salisbury, D.; Rappuoli, R. Antimicrobial resistance and the role of vaccines. Proc. Natl. Acad. Sci. USA 2018, 115, 12868–12871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, D.E.; Fan, V.Y.; Sevilla, J.P. The broad socioeconomic benefits of vaccination. Sci. Transl. Med. 2018, 10, eaaj2345. [Google Scholar] [CrossRef] [PubMed]
- Rinta-Kokko, H.; Palmu, A.A.; Auranen, K.; Nuorti, J.P.; Toropainen, M.; Siira, L.; Virtanen, M.J.; Nohynek, H.; Jokinen, J. Long-term impact of 10-valent pneumococcal conjugate vaccination on invasive pneumococcal disease among children in Finland. Vaccine 2018, 36, 1934–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epicentro. Vaccinazioni Dell’età Pediatrica e Dell’adolescente—Coperture Vaccinali. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 1 June 2019).
- Boccalini, S.; Azzari, C.; Resti, M.; Valleriani, C.; Cortimiglia, M.; Tiscione, E.; Bechini, A.; Bonanni, P. Economic and clinical evaluation of a catch-up dose of 13-valent pneumococcal conjugate vaccine in children already immunized with three doses of the 7-valent vaccine in Italy. Vaccine 2011, 29, 9521–9528. [Google Scholar] [CrossRef]
- D’Ancona, F.; Caporali, M.G.; Del Manso, M.; Giambi, C.; Camilli, R.; D’Ambrosio, F.; Del Grosso, M.; Iannazzo, S.; Rizzuto, E.; Pantosti, A. Invasive pneumococcal disease in children and adults in seven Italian regions after the introduction of the conjugate vaccine, 2008–2014. Epidemiol. Prev. 2015, 39, 134–138. [Google Scholar]
- Melegaro, A.; Edmunds, W.J. Cost-effectiveness analysis of pneumococcal conjugate vaccination in England and Wales. Vaccine 2004, 22, 4203–4214. [Google Scholar] [CrossRef]
- Liese, J.G.; Silfverdal, S.A.; Giaquinto, C.; Carmona, A.; Larcombe, J.H.; Garcia-Sicilia, J.; Fuat, A.; Garces-Sanchez, M.; Basanta, M.L.; Hiraldo, E.M.; et al. Incidence and clinical presentation of acute otitis media in children aged <6 years in European medical practices. Epidemiol. Infect. 2014, 142, 1778–1788. [Google Scholar] [CrossRef] [Green Version]
- Ansaldi, F.; Sticchi, L.; Durando, P.; Carloni, R.; Oreste, P.; Vercelli, M.; Crovari, P.; Icardi, G. Decline in pneumonia and acute otitis media after the introduction of childhood pneumococcal vaccination in Liguria, Italy. J. Int. Med. Res. 2008, 6, 1255–1260. [Google Scholar] [CrossRef]
- Baldo, V.; Cocchio, S.; Baldovin, T.; Buja, A.; Furlan, P.; Bertoncello, C.; Russo, F.; Saia, M. A population-based study on the impact of hospitalization for pneumonia in different age groups. BMC Infect. Dis. 2014, 14, 485. [Google Scholar] [CrossRef] [Green Version]
- Ansaldi, F.; Orsi, A.; Altomonte, F.; Bertone, G.; Parodi, V.; Carloni, R.; Moscatelli, P.; Pasero, E.; Oreste, P.; Icardi, G. Emergency department syndromic surveillance system for early detection of 5 syndromes: A pilot project in a reference teaching hospital in Genoa, Italy. J. Prev. Med. Hyg. 2008, 49, 131–135. [Google Scholar]
- Koskela, H. Keuhkokuumeen aiheuttama sairaalahoidon tarve nyt ja tulevaisuudessa. Suomen Lääkärilehti 2013, 68, 1349–1355. [Google Scholar]
- Epicentro. Malattie Batteriche Invasive (Sepsi e Meningiti). Available online: https://www.epicentro.iss.it/meningite/aggiornamenti (accessed on 6 April 2019).
- WHO Commission on Macroeconomics and Health. Macroeconomics and Health: Investing in Health for Economic Development. Report of the Commission on Macroeconomics and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Cost Effectiveness and Strategic Planning (WHO-CHOICE). Available online: https://www.who.int/choice/costs/en/ (accessed on 6 April 2019).
- Tariffe Dell’assistenza Ospedaliera per Acuti, Published on Official Gazette No 23 dated 28 January 2013. Available online: https://www.gazzettaufficiale.it/eli/id/2013/01/28/13A00528/sg (accessed on 6 April 2019).
- Mantovani, L.G.; de Portu, S.; Cortesi, P.A.; Belisari, A. Valutazione economica del vaccino coniugato 13-valente. JPH 2010, 7, S36–S45. [Google Scholar]
- Boccalini, S.; Bechini, A.; Levi, M.; Tiscione, E.; Gasparini, R.; Bonanni, P. Cost-effectiveness of new adult pneumococcal vaccination strategies in Italy. Hum. Vaccines Immunother. 2013, 9, 699–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Census. 2017. Available online: www.istat.it (accessed on 2 April 2019).
- Paulden, M. Recent amendments to NICE’s value-based assessment of health technologies: Implicitly inequitable? Expert Rev. Pharmacoecon. Outcomes Res. 2017, 17, 239–242. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Guide for Standardization of Economic Evaluations of Immunization Programmes; World Health Organization: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/handle/10665/69981 (accessed on 16 May 2019).
- Attema, A.E.; Brouwer, W.B.F.; Claxton, K. Discounting in Economic Evaluations. Pharmacoeconomics 2018, 3, 745–758. [Google Scholar] [CrossRef] [Green Version]
- Chuck, A.W.; Jacobs, P.; Tyrrell, G.; Kellner, J.D. Pharmacoeconomic evaluation of 10- and 13-valent pneumococcal conjugate vaccines. Vaccine 2010, 28, 5485–5490. [Google Scholar] [CrossRef]
- Bennett, J.E.; Sumner, W.; Downs, S.M., 2nd; Jaffe, D.M. Parents’ utilities for outcomes of occult bacteremia. Arch. Pediatr. Adolesc. Med. 2000, 154, 43–48. [Google Scholar]
- Cheng, A.K.; Niparko, J.K. Cost-utility of the cochlear implant in adults: A meta-analysis. Arch. Otolaryngol. Head Neck Surg. 1999, 125, 1214–1218. [Google Scholar] [CrossRef] [Green Version]
- Oostenbrink, R.; Moll, H.A.; Essink-Bot, M.L. The EQ-5D and the Health Utilities Index for permanent sequelae after meningitis: A head-to-head comparison. J. Clin. Epidemiol. 2002, 55, 791–799. [Google Scholar] [CrossRef]
- Morrow, A.; De Wals, P.; Petit, G.; Guay, M.; Erickson, L.J. The burden of pneumococcal disease in the Canadian population before routine use of the seven-valent pneumococcal conjugate vaccine. Can. J. Infect. Dis. Med. Microbiol. 2007, 18, 121–127. [Google Scholar] [CrossRef] [Green Version]
- The National Immunization Programme in the Netherlands: RIVM. LCI Guideline. 2017. Available online: https://lci.rivm.nl/richtlijnen/pneumokokkenziekte-invasief (accessed on 16 May 2019).
- Dagan, R.; Pelton, S.; Bakaletz, L.; Cohen, R. Prevention of early episodes of otitis media by pneumococcal vaccines might reduce progression to complex disease. Lancet Infect. Dis. 2016, 16, 480–492. [Google Scholar] [CrossRef]
- Tregnaghi, M.W.; Saez-Llorens, X.; López, P.; Abate, H.; Smith, E.; Pósleman, A.; Calvo, A.; Wong, D.; Cortes-Barbosa, C.; Ceballos, A.; et al. Efficacy of Pneumococcal Nontypable Haemophilus influenzae Protein D Conjugate Vaccine (PHiD-CV) in Young Latin American Children: A Double-Blind Randomized Controlled Trial. PLoS Med. 2014, 11, e1001657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Shimol, S.; Givon-Lavi, N.; Leibovitz, E.; Raiz, S.; Greenberg, D.; Dagan, R. Impact of widespread introduction of pneumococcal conjugate vaccines on pneumococcal and nonpneumococcal otitis media. Clin. Infect. Dis. 2016, 6, 611–618. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Italy | ||
|---|---|---|---|
| PCV13 | PCV10 | Incremental | |
| Morbidity | |||
| IPD cases | 7168 | 12,659 | −5491 |
| Acute otitis media cases | 555,730 | 949,633 | −393,902 |
| Pneumonia cases | 427,623 | 453,855 | −26,233 |
| Total cases | 990,520 | 1,416,147 | −425,627 |
| Mortality | |||
| IPD cases | 1061 | 1875 | −814 |
| Outcomes | |||
| QALYs gained | 211,218,952 | 211,215,677 | 3275 |
| Direct medical cost | |||
| Vaccination program cost | €461,385,903 | €280,093,471 | €181,292,432 |
| IPD | €35,894,686 | €63,247,183 | −€27,352,496 |
| AOM | €44,396,639 | €72,265,426 | −€27,868,787 |
| Pneumonia | €723,483,604 | €754,708,583 | −€27,868,787 |
| Total cost | €1,265,160,833 | €1,170,314,663 | €94,846,170 |
| Incremental cost-effectiveness | |||
| Cost per QALY gained | €28,963 PCV13 cost-effective | ||
| PCV13 | PCV10 | Incremental | ||||
|---|---|---|---|---|---|---|
| Scenario | Cost | QALYs | Cost | QALYs | Cost | QALYs |
| Base case | €1,265,160,833 | 211,218,952 | €1,170,314,663 | 211,215,677 | €94,846,170 | 3275 |
| Including NTHi and Moraxella catarrhalis for both vaccines | €1,337,750,244 | 211,216,821 | €1,253,389,766 | 211,213,238 | €84,360,478 | 3583 |
| Excluding NTHi and M. catarrhalis for PCV10 | €1,337,750,244 | 211,216,821 | €1,323,200,530 | 211,211,189 | €14,549,714 | 5632 |
| Ten-year time horizon | €2,180,992,438 | 364,913,596 | €2,034,702,338 | 364,904,743 | €146,290,100 | 8853 |
| Netherlands PCV10 trend line | €1,266,772,485 | 211,218,959 | €1,105,206,477 | 211,218,306 | €161,566,008 | 653 |
| Including indirect effects on hospitalized pneumonia | €1,216,099,224 | 211,219,055 | €1,164,320,376 | 211,219,055 | €51,778,848 | 3360 |
| Input | Age Range (years) | Source | ||||||
|---|---|---|---|---|---|---|---|---|
| <2 | 2–4 | 5–17 | 18–34 | 35–49 | 50–64 | ≥65 | ||
| Population | 1,492,050 | 1,080,898 | 7,433,899 | 11,252,659 | 14,290,635 | 12,066,427 | 13,014,942 | [44] |
| Disease rates in 2016 (per 100,000 person-years) | ||||||||
| Invasive pneumococcal disease (IPD) | 2.98 | 2.98 | 0.99 | 0.36 | 1.46 | 1.43 | 7.7 | [21,23] |
| Case fatality rate (CFR) | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | [15] |
| Pneumococcal meningitis | ||||||||
| Incidence | 0.61 | 0.15 | 0.18 | 0.03 | 0.15 | 0.12 | 0.18 | [15] |
| Case fatality rate (CFR) | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | 0.15 | [15] |
| Hearing loss, probability of (%) | 0.2 | [40] | ||||||
| Neurological sequelae, probability of (%) | 0.25 | [40] | ||||||
| Inpatient pneumonia | ||||||||
| Incidence (per 100,000 person-years) | 2190.9 | 2190.9 | 191.4 | 51 | 51 | 51 | 1,280 | [26,27,29] |
| Outpatient pneumonia | ||||||||
| Incidence (per 100,000 person-years) | 1079.1 | 1079.1 | 95.7 | 34 | 34 | 34 | 853 | |
| Simple AOM | ||||||||
| Incidence (per 100,000 person-years) | 19300 | 19700 | [25] | |||||
| Direct medical costs (local currency) | ||||||||
| Pneumococcal bacteremia | 3176 | 3176 | 3176 | 5493 | 5493 | 5493 | 5493 | [32,33,34] |
| Pneumococcal meningitis | 8067 | 8067 | 8067 | 8067 | 8067 | 8067 | 8067 | [32,33,34] |
| Pneumonia inpatient | 2190 | 2190 | 191.4 | 51 | 51 | 51 | 1280 | [32,33,34] |
| Pneumonia outpatient | 1079 | 1079 | 95.7 | 34 | 34 | 34 | 853.3 | [32,33,34] |
| Simple AOM | 76 | 76 | 76 | [32,33,34] | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansaldi, F.; Pugh, S.; Amicizia, D.; Di Virgilio, R.; Trucchi, C.; Orsi, A.; Zollo, A.; Icardi, G. Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to the 10-Valent Pneumococcal Conjugate Vaccine (PCV10) in Italy. Pathogens 2020, 9, 76. https://doi.org/10.3390/pathogens9020076
Ansaldi F, Pugh S, Amicizia D, Di Virgilio R, Trucchi C, Orsi A, Zollo A, Icardi G. Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to the 10-Valent Pneumococcal Conjugate Vaccine (PCV10) in Italy. Pathogens. 2020; 9(2):76. https://doi.org/10.3390/pathogens9020076
Chicago/Turabian StyleAnsaldi, Filippo, Sarah Pugh, Daniela Amicizia, Roberto Di Virgilio, Cecilia Trucchi, Andrea Orsi, Alessandro Zollo, and Giancarlo Icardi. 2020. "Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to the 10-Valent Pneumococcal Conjugate Vaccine (PCV10) in Italy" Pathogens 9, no. 2: 76. https://doi.org/10.3390/pathogens9020076