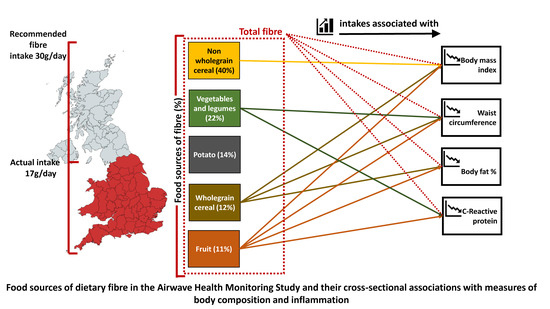
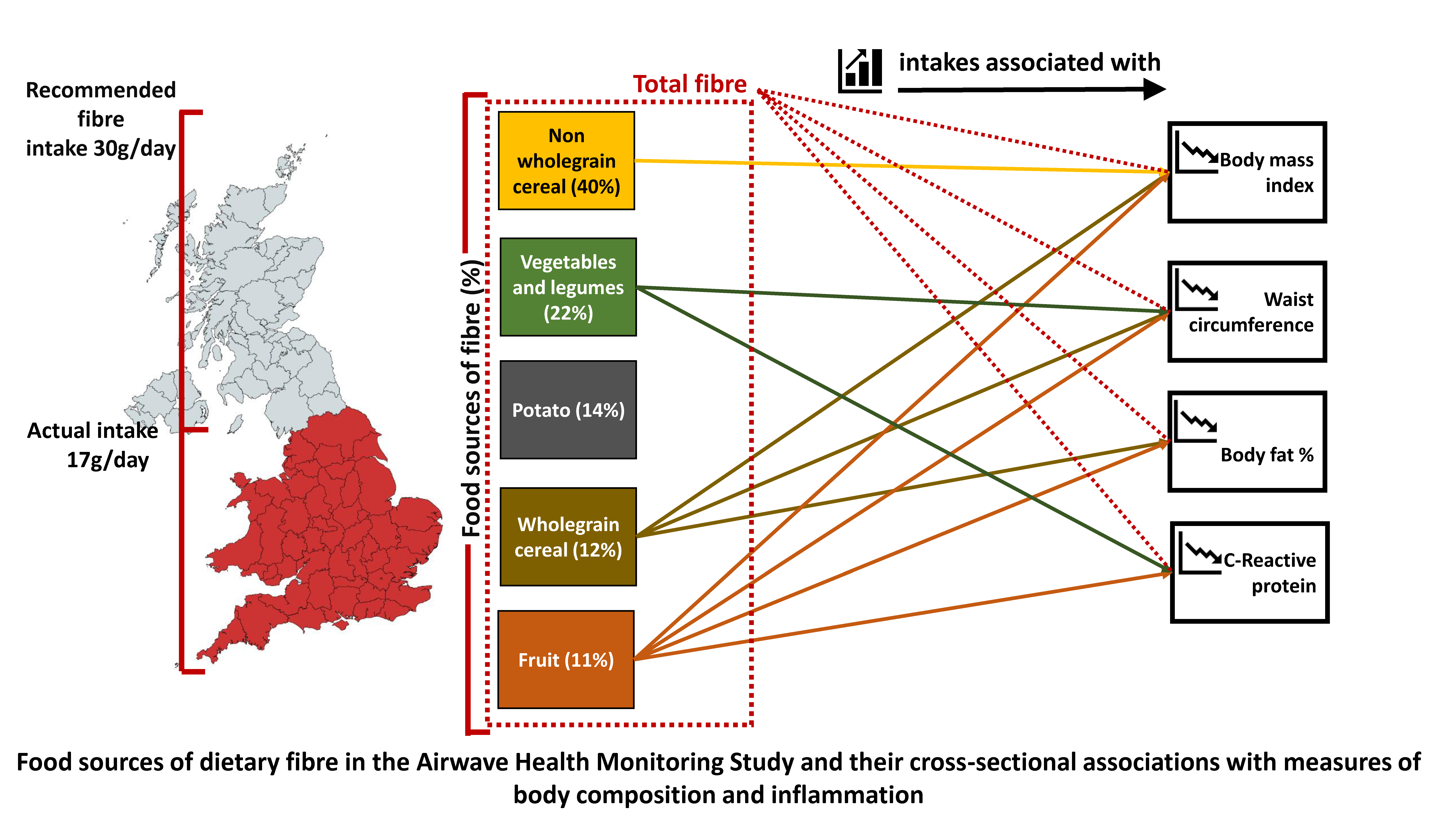
Intakes and Food Sources of Dietary Fibre and Their Associations with Measures of Body Composition and Inflammation in UK Adults: Cross-Sectional Analysis of the Airwave Health Monitoring Study

 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Fibre Intake and Other Dietary Variables
2.3. Measures of Body Composition
2.4. Measurement of Covariates
2.5. Statistical Analyses
2.6. Additional Analyses
3. Results
3.1. Cohort Characteristics
3.2. Fibre Intake and Body Composition
3.3. Additional Analyses
4. Discussion
4.1. Summary
4.2. Potential Mechanisms
4.3. Public Health Nutrition Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKinsey Global Institute. Overcoming Obesity: An Initial Economic Analysis. 2014. Available online: www.mckinsey.com/mgi (accessed on 27 December 2018).
- Hill, J.O.; Commerford, R. Physical activity, fat balance, and energy balance. Int. J. Sport Nutr. 1996, 6, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in Diet and Lifestyle and Long-Term Weight Gain in Women and Men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperling, L.S.; Mechanick, J.I.; Neeland, I.J.; Herrick, C.J.; Despres, J.P.; Ndumele, C.E.; Blum, Q.K. The CardioMetabolic Health Alliance: Working Toward a New Care Model for the Metabolic Syndrome. J. Am. Coll. Cardiol. 2015, 66, 1050–1067. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, M.A.H.; Pomerleau, J.; Grace, D.M.; Anderson, L. Fiber Intake of Normal Weight, Moderately Obese and Severely Obese Subjects. Obes. Res. 1995, 3, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Norat, T.; Ferrari, P.; Jenab, M.; Bueno-de-Mesquita, B.; Skeie, G.; Clavel-Chapelon, F. Dietary Fibre Intake and Risks of Cancers of the Colon and Rectum in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS ONE 2012, 7, e39361. [Google Scholar] [CrossRef] [PubMed]
- InterAct Consortium TI. Dietary fibre and incidence of type 2 diabetes in eight European countries: The EPIC-InterAct Study and a meta-analysis of prospective studies. Diabetologia 2015, 58, 1394–1408. [Google Scholar] [CrossRef] [PubMed]
- Van de Vijver, L.P.; van den Bosch, L.M.; van den Brandt, P.A.; Goldbohm, R.A. Whole-grain consumption, dietary fibre intake and body mass index in the Netherlands cohort study. Eur. J. Clin. Nutr. 2009, 63, 31–38. [Google Scholar] [CrossRef]
- Du, H.; van der, A.D.L.; Boshuizen, H.C.; Forouhi, N.G.; Wareham, N.J.; Halkjaer, J. Dietary fiber and subsequent changes in body weight and waist circumference in European men and women. Am. J. Clin. Nutr. 2010, 91, 329–336. [Google Scholar] [CrossRef]
- AlEssa, H.B.; Cohen, R.; Malik, V.S.; Adebamowo, S.N.; Rimm, E.B.; Manson, J.E. Carbohydrate quality and quantity and risk of coronary heart disease among US women and men. Am. J. Clin. Nutr. 2018, 107, 257–267. [Google Scholar] [CrossRef]
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Day, N.E. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar] [CrossRef] [PubMed]
- Lapice, E.; Maione, S.; Patti, L.; Cipriano, P.; Rivellese, A.A.; Riccardi, G.; Vaccaro, O. Abdominal adiposity is associated with elevated C-reactive protein independent of BMI in healthy nonobese people. Diabetes Care 2009, 32, 1734–1736. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Cornier, M.-A. Update on the NCEP ATP-III emerging cardiometabolic risk factors. BMC Med. 2014, 12, 115. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Inflammation in atherosclerosis: From pathophysiology to practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef]
- Elliott, P.; Vergnaud, A.C.; Singh, D.; Neasham, D.; Spear, J.; Heard, A. The Airwave Health Monitoring Study of police officers and staff in Great Britain: Rationale, design and methods. Environ. Res. 2014, 134, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R.; Eriksen, R.; Lamb, K.; McMeel, Y.; Vergnaud, A.C.; Spear, J.; Frost, G. Dietary assessment of British police force employees: A description of diet record coding procedures and cross-sectional evaluation of dietary energy intake reporting (The Airwave Health Monitoring Study). BMJ Open 2017, 7, e012927. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Howe, G.; Kushi, L. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.R.; Mann, K.D.; Kuznesof, S.A.; Richardson, D.P.; Seal, C.J. The whole grain content of foods consumed in the UK. Food Chem. 2017, 214, 453–459. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.Y.; Park, H.; Seo, J.C.; Kim, D.; Lim, Y.H.; Lim, S.; Hong, Y.C. Long working hours and cardiovascular disease: A meta-analysis of epidemiologic studies. J. Occup. Environ. Med. 2012, 54, 532–537. [Google Scholar] [CrossRef]
- Kivimäki, M.; Virtanen, M.; Kawachi, I.; Nyberg, S.T.; Alfredsson, L.; Batty, G.D.; Dragano, N. Long working hours, socioeconomic status, and the risk of incident type 2 diabetes: A meta-analysis of published and unpublished data from 222 120 individuals. Lancet Diabetes Endocrinol. 2014, 3, 27–34. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Scoring Protocol. 2005. Available online: http://www.ipaq.ki.se/scoring.htm (accessed on 20 October 2014).
- Coulombe, D. Orthogonal polynomial coefficients and trend analysis for unequal intervals and unequal Ns: A microcomputer application. Behav. Res. Methods 1985. Available online: https://link.springer.com/content/pdf/10.3758/BF03200967.pdf (accessed on 27 December 2018). [CrossRef]
- Muraki, I.; Rimm, E.B.; Willett, W.C.; Manson, J.E.; Hu, F.B.; Sun, Q. Potato Consumption and Risk of Type 2 Diabetes: Results from Three Prospective Cohort Studies. Diabetes Care 2016, 39, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Borch, D.; Juul-Hindsgaul, N.; Veller, M.; Astrup, A.; Jaskolowski, J.; Raben, A. Potatoes and risk of obesity, type 2 diabetes, and cardiovascular disease in apparently healthy adults: A systematic review of clinical intervention and observational studies. Am. J. Clin. Nutr. 2016, 104, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Freedman, L.S.; Carroll, R.J.; Midthune, D.; Kipnis, V. The impact of stratification by implausible energy reporting status on estimates of diet-health relationships. Biom. J. 2016, 58, 1538–1551. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek, E.J. Association between dietary fiber and serum C-reactive protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [CrossRef]
- Threapleton, D.; Greenwood, D.C.; Evans, C.E.L.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2013, 347, f6879. [Google Scholar] [CrossRef]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek III, E.J.; Ockene, I.S. Association In Proceedings of the and dietary food sources of fibre in Spain: Differences with regard to the prevalence of excess body weight and abdominal obesity in adults of the ANIBES study. Nutrients 2017, 9, 326. [Google Scholar]
- Borgi, L.; Rimm, E.B.; Willett, W.C.; Forman, J.P. Potato intake and incidence of hypertension: Results from three prospective US cohort studies. BMJ 2016, 353, i2351. [Google Scholar] [CrossRef]
- Birt, D.F.; Boylston, T.; Hendrich, S.; Jane, J.L.; Hollis, J.; Li, L.; Schalinske, K. Resistant starch: Promise for improving human health. Adv. Nutr. 2013, 4, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Reimer, R.A. Weight loss during oligofructose supplementation is associated with decreased ghrelin and increased peptide YY in overweight and obese adults. Am. J. Clin. Nutr. 2009, 89, 1751–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cani, P.D.; Joly, E.; Horsmans, Y.; Delzenne, N.M. Oligofructose promotes satiety in healthy human: A pilot study. Eur. J. Clin. Nutr. 2006, 60, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Friday, J.E.; Goldman, J.P.; Ahuja, J.K. Presence of inulin and oligofructose in the diets of Americans. J. Nutr. 1999, 129, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.A.; Havlik, J.; Cong, W.; Mullen, W.; Preston, T.; Morrison, D.J.; Combet, E. Polyphenols and health: Interactions between fibre, plant polyphenols and the gut microbiota. Nutr. Bull. 2017, 42, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Viardot, A.; Psichas, A.; Morrison, D.J.; Murphy, K.G.; Zac-Varghese, S.E.; Blundell, J.E. Effects of targeted delivery of propionate to the human colon on appetite regulation, body weight maintenance and adiposity in overweight adults. Gut 2015, 64, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Whitton, C.; Nicholson, S.K.; Roberts, C.; Prynne, C.J.; Pot, G.K.; Olson, A.; Henderson, H. NDNS Survey Results from Years 7 and 8 of the Rolling Programme. 2014. Available online: www.gov.uk/phe (accessed on 20 March 2018).
- Gibson, R.; Eriksen, R.; Singh, D.; Vergnaud, A.C.; Heard, A.; Chan, Q. A cross-sectional investigation into the occupational and socio-demographic characteristics of British police force employees reporting a dietary pattern associated with cardiometabolic risk: Findings from the Airwave Health Monitoring Study. Eur. J. Nutr. 2017, 57, 2913–2926. [Google Scholar] [CrossRef]
- Mann, K.D.; Pearce, M.S.; Seal, C.J. Providing evidence to support the development of whole grain dietary recommendations in the United Kingdom. Proc. Nutr. Soc. 2017, 76, 369–377. [Google Scholar] [CrossRef]
- Kromhout, D.; Spaaij, C.J.K.; de Goede, J.; Weggemans, R.M. The 2015 Dutch food-based dietary guidelines. Eur. J. Clin. Nutr. 2016, 70, 869–878. [Google Scholar] [CrossRef]
- Alinia, S.; Hels, O.; Tetens, I. The potential association between fruit intake and body weight—A review. Obes Rev. 2009, 10, 639–647. [Google Scholar] [CrossRef]
- Williamson, D.F.; Kahn, H.S.; Remington, P.L.; Anda, R.F. The 10-year incidence of overweight and major weight gain in US adults. Arch. Intern. Med. 1990, 150, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Cohort Strategic Review Subgroup. Medical Research Council. Maximising the Value of UK Population Cohorts. MRC Strategic Review of the Largest UK Population Cohort Studies. 2014. Available online: https://mrc.ukri.org/publications/browse/maximising-the-value-of-uk-population-cohorts/ (accessed on 28 March 2019).
- Lafay, L.; Mennen, L.; Basdevant, A.; Charles, M.A.; Borys, J.M.; Eschwege, E.; Romon, M. Does energy intake underreporting involve all kinds of food or only specific food items? Results from the Fleurbaix Laventie Ville Santé (FLVS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1500–1506. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Mean | SD |
|---|---|---|
| Age, years (SD) | 41.1 | 9.1 |
| N | % | |
| Men N (%) | 4220 | 61.2 |
| White | 6707 | 97.3 |
| Relationship status | ||
| Cohabiting | 1125 | 16.7 |
| Divorced/separated | 540 | 8.0 |
| Married | 4308 | 64.0 |
| Single | 763 | 11.3 |
| Missing | 162 | 2.3 |
| Education | ||
| Left school before taking GCSE | 259 | 3.8 |
| GCSE or equivalent | 2049 | 29.7 |
| Vocational qualifications | 498 | 7.2 |
| A-levels/Highers or equivalent | 2218 | 32.2 |
| Bachelor degree or equivalent | 1442 | 20.9 |
| Postgraduate qualifications | 431 | 6.3 |
| Employment force, country | ||
| England | 5175 | 75.2 |
| Scotland | 1093 | 15.9 |
| Wales | 614 | 8.9 |
| Missing | 16 | <0.01 |
| Rank | ||
| Police Constable/Sergeant | 433 | 7.7 |
| Inspector and above | 3295 | 58.6 |
| Police staff/Other | 1895 | 33.7 |
| Missing | 1275 | 18.4 |
| Hours worked per week | ||
| <35 | 596 | 8.6 |
| 35 < 40 | 2637 | 38.2 |
| 40 < 49 | 2260 | 32.8 |
| 49 < 55 | 726 | 10.5 |
| 55+ | 679 | 9.8 |
| Physical activity a | ||
| Low | 772 | 11.2 |
| Moderate | 3087 | 44.8 |
| High | 3039 | 44.1 |
| Smoking status | ||
| Never smoker | 4780 | 69.5 |
| Former smoker | 1542 | 22.4 |
| Current smoker | 554 | 8.1 |
| Missing | 22 | |
| Body Mass Index | ||
| <25 kg/m2 | 2303 | 33.4 |
| ≥25 kg/m2 and <30 kg/m2 | 3288 | 47.7 |
| >30 kg/m2 | 1307 | 18.9 |
| Waist circumference risk category * | ||
| Healthy measurement | 3513 | 51.0 |
| Elevated risk | 3385 | 49.0 |
| C-reactive protein | ||
| <1 mg/L | 3715 | 53.9 |
| ≥1 mg/L | 3183 | 46.1 |
| Achieving ≥30 g/day n (%) | 231 | 3.3 |
|---|---|---|
| Mean | SD | |
| Total fibre g/day AOAC | 17.3 | 6.0 |
| Source of fibre by food group | ||
| %non-whole grain cereal sources | 39.9 | 12.7 |
| % veg (exc. legume) | 16.2 | 8.5 |
| % potato (inc. crisps) | 13.6 | 8.6 |
| % whole grain | 12.4 | 9.8 |
| % fruit (exc. juice) | 11.2 | 9.2 |
| % legumes (inc. peanuts) | 6.0 | 5.7 |
| % nuts and seeds | 0.7 | 2.0 |
| Outcome Measure/Fiber Food Source | Model | Quintiles of Fibre Intake g/1000 kcal | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ptrend | |||||||
| Adjusted Means and 95% Confidence Interval (95%CI) | ||||||||||||
| Body Mass Index, kg/m2 | ||||||||||||
| Total fibre | Crude | 26.99 | 26.77, 27.21 | 26.73 | 26.53, 26.93 | 26.86 | 26.66, 27.06 | 26.52 | 26.32, 26.72 | 26.52 | 26.32, 26.72 | 0.0001 |
| Adjusted | 27.25 | 26.88, 27.62 | 26.94 | 26.57, 27.31 | 26.97 | 26.60, 27.34 | 26.54 | 26.17, 26.91 | 26.32 | 25.93, 26.71 | <0.0001 | |
| Whole grain fibre | Crude | 26.94 | 26.74, 27.14 | 26.82 | 26.62, 27.02 | 26.81 | 26.61, 27.01 | 26.63 | 26.43, 26.83 | 26.32 | 26.12, 26.52 | <0.0001 |
| Adjusted | 26.91 | 26.54, 27.28 | 26.90 | 26.53, 27.27 | 26.93 | 26.56, 27.30 | 26.78 | 26.41, 27.15 | 26.39 | 26.02, 26.76 | 0.0002 | |
| Cereal non-whole grain | Crude | 26.92 | 26.72, 27.12 | 26.76 | 26.56, 26.96 | 26.64 | 26.44, 26.84 | 26.78 | 26.58, 26.98 | 26.44 | 26.24, 26.64 | 0.0026 |
| Adjusted | 26.95 | 26.58, 27.32 | 26.82 | 26.45, 27.19 | 26.74 | 26.37, 27.11 | 26.86 | 26.49, 27.23 | 26.50 | 26.13, 26.87 | 0.0095 | |
| Fruit fibre | Crude | 27.36 | 27.16, 27.56 | 26.72 | 26.52, 26.92 | 26.68 | 26.48, 26.88 | 26.26 | 26.06, 26.46 | 26.55 | 26.35, 26.75 | <0.0001 |
| Adjusted | 27.30 | 26.93, 27.67 | 26.79 | 26.42, 27.16 | 26.80 | 26.43, 27.17 | 26.38 | 26.01, 26.75 | 26.59 | 26.20, 26.98 | <0.0001 | |
| Vegetable and legume fibre | Crude | 26.90 | 26.68, 27.12 | 26.81 | 26.61, 27.01 | 26.44 | 26.24, 26.64 | 26.63 | 26.43, 26.83 | 26.76 | 26.56, 26.96 | 0.36 |
| Adjusted | 27.02 | 26.65, 27.39 | 26.88 | 26.51, 27.25 | 26.54 | 26.17, 26.91 | 26.74 | 26.37, 27.11 | 26.70 | 26.33, 27.07 | 0.05 | |
| Potato fibre | Crude | 26.56 | 26.36, 26.76 | 26.59 | 26.39, 26.79 | 26.53 | 26.33, 26.73 | 26.66 | 26.46, 26.86 | 27.19 | 26.99, 27.39 | <0.0001 |
| Adjusted | 26.85 | 26.48, 27.22 | 26.81 | 26.44, 27.18 | 26.64 | 26.27, 27.01 | 26.58 | 26.21, 26.95 | 26.92 | 26.53, 27.31 | 0.93 | |
| Percentage body fat, % | ||||||||||||
| Total fibre | Crude | 28.13 | 27.80, 28.46 | 27.56 | 27.23, 27.89 | 27.49 | 27.16, 27.82 | 26.92 | 26.59, 27.25 | 26.80 | 26.47, 27.13 | <0.0001 |
| Adjusted | 28.10 | 27.51, 28.69 | 27.70 | 27.11, 28.29 | 27.57 | 26.98, 28.16 | 27.00 | 26.41, 27.59 | 26.77 | 26.16, 27.38 | <0.0001 | |
| Whole grain fibre | Crude | 28.06 | 27.73, 28.39 | 27.63 | 27.30, 27.96 | 27.43 | 27.1, 27.76 | 27.13 | 26.80, 27.46 | 26.58 | 26.25, 26.91 | <0.0001 |
| Adjusted | 27.59 | 27.00, 28.18 | 27.58 | 26.99, 28.17 | 27.50 | 26.91, 28.09 | 27.44 | 26.85, 28.03 | 26.81 | 26.22, 27.40 | 0.0007 | |
| Cereal non-whole grain | Crude | 27.81 | 27.48, 28.14 | 27.37 | 27.04, 27.70 | 27.48 | 27.15, 27.81 | 27.26 | 26.93, 27.59 | 26.91 | 26.58, 27.24 | 0.0002 |
| Adjusted | 27.58 | 26.99, 28.17 | 27.58 | 26.99, 28.17 | 27.56 | 26.97, 28.15 | 27.36 | 26.77, 27.95 | 27.36 | 26.77, 27.95 | 0.09 | |
| Fruit fibre | Crude | 28.66 | 28.33, 28.99 | 27.68 | 27.35, 28.01 | 27.42 | 27.09, 27.75 | 26.54 | 26.21, 26.87 | 26.62 | 26.29, 26.95 | <0.0001 |
| Adjusted | 28.09 | 27.50, 28.68 | 27.54 | 26.95, 28.13 | 27.55 | 26.96, 28.14 | 26.86 | 26.27, 27.45 | 26.86 | 26.25, 27.47 | <0.0001 | |
| Vegetable and legume fibre | Crude | 27.71 | 27.38, 28.04 | 27.56 | 27.23, 27.89 | 26.93 | 26.6, 27.260 | 27.24 | 26.91, 27.57 | 27.41 | 27.08, 27.74 | 0.22 |
| Adjusted | 27.66 | 27.07, 28.25 | 27.52 | 26.93, 28.11 | 27.03 | 26.44, 27.62 | 27.33 | 26.74, 27.92 | 27.33 | 26.74, 27.92 | 0.21 | |
| Potato fibre | Crude | 26.58 | 26.25, 26.91 | 27.18 | 26.85, 27.51 | 27.33 | 27.00, 27.66 | 27.32 | 26.99, 27.65 | 28.40 | 28.07, 28.73 | <0.0001 |
| Adjusted | 27.18 | 26.59, 27.77 | 27.49 | 26.90, 28.08 | 27.40 | 26.81, 27.99 | 27.01 | 26.42, 27.60 | 27.65 | 27.04, 28.26 | 0.28 | |
| Waist circumference, cm | ||||||||||||
| Total fibre | Crude | 88.75 | 88.24, 89.26 | 87.86 | 87.35, 88.37 | 87.94 | 87.43, 88.45 | 87.02 | 86.51, 87.53 | 86.55 | 86.04, 87.06 | <0.0001 |
| Adjusted | 89.04 | 88.10, 89.98 | 88.21 | 87.27, 89.15 | 88.16 | 87.22, 89.10 | 87.24 | 86.30, 88.18 | 86.57 | 85.59, 87.55 | <0.0001 | |
| Whole grain fibre | Crude | 88.43 | 87.92, 88.94 | 87.98 | 87.47, 88.49 | 87.80 | 87.29, 88.31 | 87.52 | 87.01, 88.03 | 86.25 | 85.74, 86.76 | <0.0001 |
| Adjusted | 88.08 | 87.16, 89.00 | 88.05 | 87.11, 88.99 | 88.02 | 87.10, 88.94 | 88.01 | 87.07, 88.95 | 86.73 | 85.79, 87.67 | 0.0004 | |
| Cereal non-whole grain | Crude | 88.21 | 87.70, 88.72 | 87.66 | 87.15, 88.17 | 87.47 | 86.96, 87.98 | 87.84 | 87.33, 88.35 | 86.81 | 86.30, 87.32 | 0.0007 |
| Adjusted | 88.09 | 87.15, 89.03 | 87.70 | 86.78, 88.62 | 87.69 | 86.75, 88.63 | 88.06 | 87.12, 89.00 | 87.21 | 86.25, 88.17 | 0.07 | |
| Fruit fibre | Crude | 89.36 | 88.85, 89.87 | 88.16 | 87.65, 88.67 | 87.69 | 87.18, 88.20 | 86.43 | 85.92, 86.94 | 86.48 | 85.97, 86.99 | <0.0001 |
| Adjusted | 88.94 | 88.02, 89.86 | 88.16 | 87.24, 89.08 | 87.98 | 87.06, 88.90 | 86.84 | 85.90, 87.78 | 86.95 | 85.99, 87.91 | <0.0001 | |
| Vegetable and legume fibre | Crude | 88.34 | 87.81, 88.87 | 87.99 | 87.48, 88.50 | 87.10 | 86.59, 87.61 | 87.23 | 86.72, 87.74 | 87.41 | 86.90, 87.92 | 0.0083 |
| Adjusted | 88.42 | 87.50, 89.34 | 88.01 | 87.09, 88.93 | 87.31 | 86.37, 88.25 | 87.53 | 86.59, 88.47 | 87.47 | 86.53, 88.41 | 0.0156 | |
| Potato fibre | Crude | 86.69 | 86.18, 87.20 | 87.52 | 87.01, 88.03 | 87.21 | 86.70, 87.72 | 87.52 | 87.01, 88.03 | 89.01 | 88.50, 89.52 | <0.0001 |
| Adjusted | 87.56 | 86.62, 88.50 | 88.02 | 87.08, 88.96 | 87.44 | 86.50, 88.38 | 87.24 | 86.30, 88.18 | 88.40 | 87.44, 89.36 | 0.18 | |
| C-reactive protein, mg/L | ||||||||||||
| Total fibre | Crude | 1.08 | 1.02, 1.14 | 1.01 | 0.96, 1.06 | 0.99 | 0.94, 1.04 | 0.90 | 0.85, 0.94 | 0.82 | 0.78, 0.86 | <0.0001 |
| Adjusted | 1.12 | 1.02, 1.23 | 1.08 | 0.98, 1.18 | 1.07 | 0.97, 1.17 | 0.97 | 0.88, 1.07 | 0.90 | 0.81, 0.99 | <0.0001 | |
| Whole grain fibre | Crude | 1.05 | 1.00, 1.11 | 0.98 | 0.93, 1.04 | 0.94 | 0.89, 0.99 | 0.91 | 0.87, 0.96 | 0.87 | 0.83, 0.92 | <0.0001 |
| Adjusted | 1.05 | 0.95, 1.15 | 1.03 | 0.94, 1.14 | 1.01 | 0.92, 1.11 | 1.01 | 0.92, 1.11 | 0.98 | 0.89, 1.08 | 0.10 | |
| Cereal non-whole grain | Crude | 0.92 | 0.93, 1.03 | 0.97 | 0.92, 1.02 | 0.96 | 0.92, 1.01 | 0.94 | 0.89, 0.98 | 0.90 | 0.86, 0.95 | 0.0120 |
| Adjusted | 1.02 | 0.92, 1.12 | 1.02 | 0.93, 1.12 | 1.04 | 0.95, 1.15 | 1.01 | 0.92, 1.11 | 1.00 | 0.91, 1.10 | 0.64 | |
| Fruit fibre | Crude | 1.12 | 1.06, 1.18 | 1.03 | 0.98, 1.09 | 0.97 | 0.92, 1.02 | 0.84 | 0.80, 0.89 | 0.83 | 0.79, 0.88 | <0.0001 |
| Adjusted | 1.11 | 1.01, 1.22 | 1.07 | 0.98, 1.18 | 1.05 | 0.95, 1.15 | 0.93 | 0.85, 1.02 | 0.95 | 0.86, 1.05 | <0.0001 | |
| Vegetable and legume fibre | Crude | 1.03 | 0.97, 1.08 | 1.05 | 1.00, 1.10 | 0.91 | 0.87, 0.96 | 0.90 | 0.86, 0.95 | 0.89 | 0.85, 0.94 | <0.0001 |
| Adjusted | 1.07 | 0.97, 1.17 | 1.11 | 1.01, 1.22 | 0.98 | 0.89, 1.08 | 0.97 | 0.88, 1.07 | 0.97 | 0.88, 1.06 | 0.0005 | |
| Potato fibre | Crude | 0.86 | 0.82, 0.91 | 0.92 | 0.88, 0.97 | 0.96 | 0.91, 1.01 | 0.95 | 0.90, 1.00 | 1.07 | 1.02, 1.13 | <0.0001 |
| Adjusted | 0.98 | 0.89, 1.08 | 1.02 | 0.93, 1.12 | 1.02 | 0.93, 1.13 | 0.98 | 0.89, 1.08 | 1.06 | 0.96, 1.17 | 0.15 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, R.; Eriksen, R.; Chambers, E.; Gao, H.; Aresu, M.; Heard, A.; Chan, Q.; Elliott, P.; Frost, G. Intakes and Food Sources of Dietary Fibre and Their Associations with Measures of Body Composition and Inflammation in UK Adults: Cross-Sectional Analysis of the Airwave Health Monitoring Study. Nutrients 2019, 11, 1839. https://doi.org/10.3390/nu11081839
Gibson R, Eriksen R, Chambers E, Gao H, Aresu M, Heard A, Chan Q, Elliott P, Frost G. Intakes and Food Sources of Dietary Fibre and Their Associations with Measures of Body Composition and Inflammation in UK Adults: Cross-Sectional Analysis of the Airwave Health Monitoring Study. Nutrients. 2019; 11(8):1839. https://doi.org/10.3390/nu11081839
Chicago/Turabian StyleGibson, Rachel, Rebeca Eriksen, Edward Chambers, He Gao, Maria Aresu, Andrew Heard, Queenie Chan, Paul Elliott, and Gary Frost. 2019. "Intakes and Food Sources of Dietary Fibre and Their Associations with Measures of Body Composition and Inflammation in UK Adults: Cross-Sectional Analysis of the Airwave Health Monitoring Study" Nutrients 11, no. 8: 1839. https://doi.org/10.3390/nu11081839