The Impact of Maternal Eating Disorders on Dietary Intake and Eating Patterns during Pregnancy: A Systematic Review

 ,
, 
Abstract
:1. Introduction
- Do pregnant women with a history of EDs show different dietary intakes and patterns as compared to healthy pregnant women?
- Do pregnant women with a history of EDs deviate from international dietary recommendations guidelines for pregnancy?
- Do pregnant women with a history of EDs differ from healthy pregnant women with regard to nutritional biomarkers and dietary supplement intake?
- Do pregnant women with a history of EDs show dysfunctional eating behaviors, i.e., restrictive eating, dieting, binge eating? Here, we will focus exclusively on behavioral eating aspects (which also represent ED symptoms), but not solely on ED symptoms with no direct connection to food intake (e.g., self-induced vomiting).
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Participants
2.2.2. Interventions
2.2.3. Comparators
2.2.4. Outcome
2.2.5. Study design
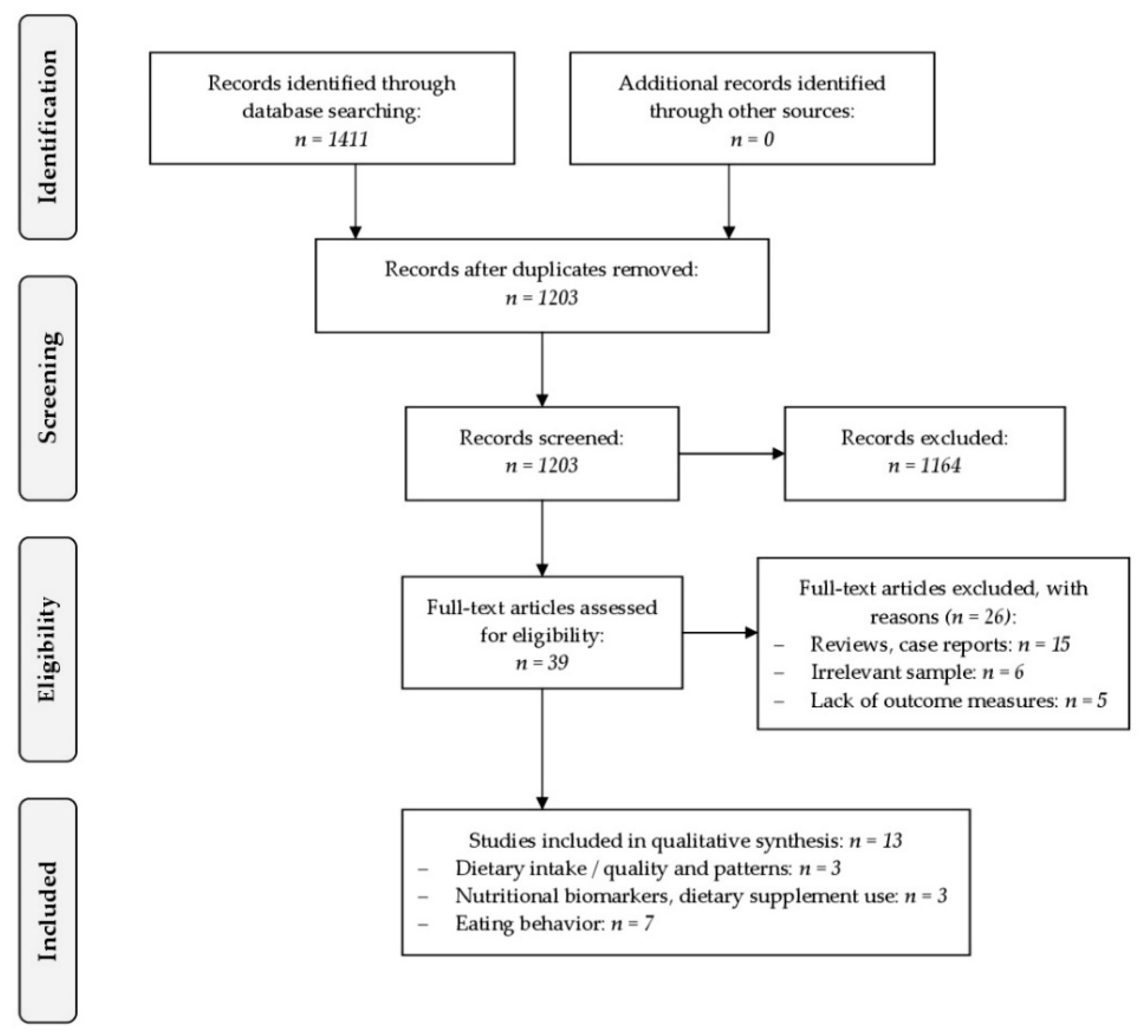
3. Results
- Dietary intake/quality and patterns (n = 3)
- Nutritional biomarkers and dietary supplement use (n = 3)
- Eating behavior (n = 7)
3.1. Studies Investigating Dietary Intake and Patterns in Pregnant Women with Eating Disorders
3.2. Studies Investigating Maternal Biomarkers of Nutrition and Dietary Supplement Use in Pregnant Women with Eating Disorders
3.3. Studies Investigating Eating Behavior in Pregnant Women with EDs
4. Discussion
4.1. Dietary Intake and Patterns in Pregnant Women with Eating Disorders
4.2. Maternal Biomarkers of Nutrition and Dietary Supplement Use in Pregnant Women with Eating Disorders
4.3. Dysfunctional Eating Behavior in Pregnant Women with EDs
4.4. Strengths and Limitations
5. Conclusions and Future Directions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Koletzko, B.; Cremer, M.; Flothkötter, M.; Graf, C.; Hauner, H.; Hellmers, C.; Kersting, M.; Krawinkel, M.; Przyrembel, H.; Röbl-Mathieu, M.; et al. Diet and lifestyle before and during pregnancy—Practical recommendations of the germany-wide healthy start—Young family network. Geburtshilfe Frauenheilkd. 2018, 78, 1262–1282. [Google Scholar] [CrossRef]
- Berti, C.; Biesalski, H.K.; Gärtner, R.; Lapillonne, A.; Pietrzik, K.; Poston, L.; Redman, C.; Koletzko, B.; Cetin, I. Micronutrients in pregnancy: Current knowledge and unresolved questions. Clin. Nutr. 2011, 30, 689–701. [Google Scholar] [CrossRef] [Green Version]
- Lucas, A. Long-term programming effects of early nutrition—Implications for the preterm infant. J. Perinatol. 2005, 25, S2. [Google Scholar] [CrossRef]
- Barker, D.J. The fetal and infant origins of adult disease. BMJ (Clin. Res. Ed.) 1990, 301, 1111. [Google Scholar] [CrossRef]
- Hoffman, D.J.; Reynolds, R.M.; Hardy, D.B. Developmental origins of health and disease: Current knowledge and potential mechanisms. Nutr. Rev. 2017, 75, 951–970. [Google Scholar] [CrossRef]
- Barker, D.J.P. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. New Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef]
- Easter, A.; Bye, A.; Taborelli, E.; Corfield, F.; Schmidt, U.; Treasure, J.; Micali, N. Recognising the symptoms: How common are eating disorders in pregnancy? Eur. Eat. Disord. Rev. 2013, 21, 340–344. [Google Scholar] [CrossRef] [PubMed]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013. [Google Scholar]
- Eagles, J.M.; Lee, A.J.; Raja, E.A.; Millar, H.R.; Bhattacharya, S. Pregnancy outcomes of women with and without a history of anorexia nervosa. Psychol. Med. 2012, 42, 2651–2660. [Google Scholar] [CrossRef]
- Koubaa, S.; Hallstrom, T.; Lindholm, C.; Hirschberg, A.L. Pregnancy and neonatal outcomes in women with eating disorders. Obstet. Gynecol. 2005, 105, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Micali, N.; Simonoff, E.; Treasure, J. Risk of major adverse perinatal outcomes in women with eating disorders. Br. J. Psychiatry 2007, 190, 255–259. [Google Scholar] [CrossRef] [Green Version]
- Franko, D.L.; Blais, M.A.; Becker, A.E.; Delinsky, S.S.; Greenwood, D.N.; Flores, A.T.; Ekeblad, E.R.; Eddy, K.T.; Herzog, D.B. Pregnancy complications and neonatal outcomes in women with eating disorders. Am. J. Psychiatry 2001, 158, 1461–1466. [Google Scholar] [CrossRef]
- Solmi, F.; Sallis, H.; Stahl, D.; Treasure, J.; Micali, N. Low birth weight in the offspring of women with anorexia nervosa. Epidemiol. Rev. 2014, 36, 49–56. [Google Scholar] [CrossRef]
- Linna, M.S.; Raevuori, A.; Haukka, J.; Suvisaari, J.M.; Suokas, J.T.; Gissler, M. Pregnancy, obstetric, and perinatal health outcomes in eating disorders. Am. J. Obstet. Gynecol. 2014, 211, e391–e398. [Google Scholar] [CrossRef]
- Bulik, C.M.; Von Holle, A.; Siega-Riz, A.M.; Torgersen, L.; Lie, K.K.; Hamer, R.M.; Berg, C.K.; Sullivan, P.; Reichborn-Kjennerud, T. Birth outcomes in women with eating disorders in the norwegian mother and child cohort study (moba). Int. J. Eat. Disord. 2009, 42, 9–18. [Google Scholar] [CrossRef]
- Koubaa, S.; Hallstrom, T.; Hagenas, L.; Hirschberg, A.L. Retarded head growth and neurocognitive development in infants of mothers with a history of eating disorders: Longitudinal cohort study. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 1413–1422. [Google Scholar] [CrossRef]
- Barona, M.; Taborelli, E.; Corfield, F.; Pawlby, S.; Easter, A.; Schmidt, U.; Treasure, J.; Micali, N. Neurobehavioural and cognitive development in infants born to mothers with eating disorders. J. Child Psychol. Psychiatry 2017, 58, 931–938. [Google Scholar] [CrossRef] [Green Version]
- HO, A.S.L.; SOH, N.L.; WALTER, G.; TOUYZ, S. Comparison of nutrition knowledge among health professionals, patients with eating disorders and the general population. Nutr. Diet. 2011, 68, 267–272. [Google Scholar] [CrossRef]
- Blais, M.A.; Becker, A.E.; Burwell, R.A.; Flores, A.T.; Nussbaum, K.M.; Greenwood, D.N.; Ekeblad, E.R.; Herzog, D.B. Pregnancy: Outcome and impact on symptomatology in a cohort of eating-disordered women. Int. J. Eat. Disord. 2000, 27, 140–149. [Google Scholar] [CrossRef]
- Micali, N.; Treasure, J. Biological effects of a maternal ed on pregnancy and foetal development: A review. Eur. Eat. Disord. Rev. 2009, 17, 448–454. [Google Scholar] [CrossRef]
- Bulik, C.M.; Von Holle, A.; Hamer, R.; Knoph Berg, C.; Torgersen, L.; Magnus, P.; Stoltenberg, C.; Siega-Riz, A.M.; Sullivan, P.; Reichborn-Kjennerud, T. Patterns of remission, continuation and incidence of broadly defined eating disorders during early pregnancy in the norwegian mother and child cohort study (moba). Psychol. Med. 2007, 37, 1109–1118. [Google Scholar] [CrossRef]
- Crow, S.J.; Agras, W.S.; Crosby, R.; Halmi, K.; Mitchell, J.E. Eating disorder symptoms in pregnancy: A prospective study. Int. J. Eat. Disord. 2008, 41, 277–279. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; et al. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65–W-94. [Google Scholar] [CrossRef]
- NEDA. PICA. Available online: https://www.nationaleatingdisorders.org/learn/by-eating-disorder/other/pica (accessed on 8 January 2019).
- Procter, S.B.; Campbell, C.G. Position of the academy of nutrition and dietetics: Nutrition and lifestyle for a healthy pregnancy outcome. J. Acad. Nutr. Diet. 2014, 114, 1099–1103. [Google Scholar] [CrossRef]
- Maternal and Child Nutrition. Public Health Guideline [ph11]. Available online: https://www.nice.org.uk/guidance/qs98/resources/maternal-and-child-nutrition-pdf-2098975759045 (accessed on 8 January 2019).
- Micali, N.; Northstone, K.; Emmett, P.; Naumann, U.; Treasure, J.L. Nutritional intake and dietary patterns in pregnancy: A longitudinal study of women with lifetime eating disorders. Br. J. Nutr. 2012, 108, 2093–2099. [Google Scholar] [CrossRef]
- Siega-Riz, A.M.; Haugen, M.; Meltzer, H.M.; Von Holle, A.; Hamer, R.; Torgersen, L.; Knopf-Berg, C.; Reichborn-Kjennerud, T.; Bulik, C.M. Nutrient and food group intakes of women with and without bulimia nervosa and binge eating disorder during pregnancy. Am. J. Clin. Nutr. 2008, 87, 1346–1355. [Google Scholar] [CrossRef]
- Nguyen, A.N.; de Barse, L.M.; Tiemeier, H.; Jaddoe, V.W.V.; Franco, O.H.; Jansen, P.W.; Voortman, T. Maternal history of eating disorders: Diet quality during pregnancy and infant feeding. Appetite 2017, 109, 108–114. [Google Scholar] [CrossRef]
- Koubaa, S.; Hallstrom, T.; Brismar, K.; Hellstrom, P.M.; Hirschberg, A.L. Biomarkers of nutrition and stress in pregnant women with a history of eating disorders in relation to head circumference and neurocognitive function of the offspring. BMC Pregnancy Childbirth 2015, 15, 318. [Google Scholar] [CrossRef]
- Dellava, J.E.; Von Holle, A.; Torgersen, L.; Reichborn-Kjennerud, T.; Haugen, M.; Meltzer, H.M.; Bulik, C.M. Dietary supplement use immediately before and during pregnancy in norwegian women with eating disorders. Int. J. Eat. Disord. 2011, 44, 325–332. [Google Scholar] [CrossRef]
- Micali, N.; Treasure, J.; Simonoff, E. Eating disorders symptoms in pregnancy: A longitudinal study of women with recent and past eating disorders and obesity. J. Psychosom. Res. 2007, 63, 297–303. [Google Scholar] [CrossRef]
- Crow, S.J.; Keel, P.K.; Thuras, P.; Mitchell, J.E. Bulimia symptoms and other risk behaviors during pregnancy in women with bulimia nervosa. Int. J. Eat. Disord. 2004, 36, 220–223. [Google Scholar] [CrossRef]
- Lacey, J.H.; Smith, G. Bulimia nervosa: The impact of pregnancy on mother and baby. Br. J. Psychiatry 1987, 150, 777–781. [Google Scholar] [CrossRef]
- Morgan, J.F.; Lacey, J.H.; Sedgwick, P.M. Impact of pregnancy on bulimia nervosa. Br. J. Psychiatry 1999, 174, 135–140. [Google Scholar] [CrossRef]
- Lemberg, R.; Phillips, J. The impact of pregnancy on anorexia nervosa and bulimia. Int. J. Eat. Disord. 1989, 8, 285–295. [Google Scholar] [CrossRef]
- Rodrigo, C.P.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food frequency questionnaires. Nutr. Hosp. 2015, 31, 49–56. [Google Scholar]
- Pinto, E.; Severo, M.; Correia, S.; Dos Santos Silva, I.; Lopes, C.; Barros, H. Validity and reproducibility of a semi-quantitative food frequency questionnaire for use among portuguese pregnant women. Matern. Child Nutr. 2010, 6, 105–119. [Google Scholar] [CrossRef]
- Brantsæter, A.L.; Haugen, M.; Alexander, J.; Meltzer, H.M. Validity of a new food frequency questionnaire for pregnant women in the norwegian mother and child cohort study (moba). Matern. Child Nutr. 2008, 4, 28–43. [Google Scholar] [CrossRef]
- McGowan, C.A.; Curran, S.; McAuliffe, F.M. Relative validity of a food frequency questionnaire to assess nutrient intake in pregnant women. J. Hum. Nutr. Diet. 2014, 27, 167–174. [Google Scholar] [CrossRef]
- Bernardo, W.; Simões, R.; Buzzini, R.; Nunes, V.; Glina, F. Adverse effects of the consumption of artificial sweeteners—Systematic review. Rev. Da Assoc. Médica Bras. 2016, 62, 120–122. [Google Scholar] [CrossRef]
- Li, J.; Zhao, H.; Song, J.-M.; Zhang, J.; Tang, Y.-L.; Xin, C.-M. A meta-analysis of risk of pregnancy loss and caffeine and coffee consumption during pregnancy. Int. J. Gynecol. Obstet. 2015, 130, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Wu, Y.; Neelakantan, N.; Chong, M.F.-F.; Pan, A.; van Dam, R.M. Maternal caffeine intake during pregnancy and risk of pregnancy loss: A categorical and dose–response meta-analysis of prospective studies. Public Health Nutr. 2016, 19, 1233–1244. [Google Scholar] [CrossRef]
- Jahanfar, S.; Jaafar, S.H. Effects of restricted caffeine intake by mother on fetal, neonatal and pregnancy outcomes. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [Green Version]
- Hart, S.; Abraham, S.; Franklin, R.C.; Russell, J. The reasons why eating disorder patients drink. Eur. Eat. Disord. Rev. 2011, 19, 121–128. [Google Scholar] [CrossRef]
- Cano-Marquina, A.; Tarín, J.J.; Cano, A. The impact of coffee on health. Maturitas 2013, 75, 7–21. [Google Scholar] [CrossRef] [PubMed]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on the safety of caffeine. EFSA J. 2015, 13, 4102. [Google Scholar]
- ACOG. Committee opinion no. 462: Moderate caffeine consumption during pregnancy. Obstet. Gynecol. 2010, 116, 467–468. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O. Maternal iron status: Relation to fetal growth, length of gestation, and iron endowment of the neonate. Nutr. Rev. 2011, 69, S23–S29. [Google Scholar] [CrossRef]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; de Benoist, B. Worldwide prevalence of anaemia, who vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef]
- Milman, N. Oral iron prophylaxis in pregnancy: Not too little and not too much! J. Pregnancy 2012, 2012, 8. [Google Scholar] [CrossRef]
- Menon, K.C.; Ferguson, E.L.; Thomson, C.D.; Gray, A.R.; Zodpey, S.; Saraf, A.; Das, P.K.; Skeaff, S.A. Effects of anemia at different stages of gestation on infant outcomes. Nutrition 2016, 32, 61–65. [Google Scholar] [CrossRef]
- Scholl, T.O.; Hediger, M.L.; Fischer, R.L.; Shearer, J.W. Anemia vs iron deficiency: Increased risk of preterm delivery in a prospective study. Am. J. Clin. Nutr. 1992, 55, 985–988. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 12, 1–254. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force. Folic acid supplementation for the prevention of neural tube defects: Us preventive services task force recommendation statement. JAMA 2017, 317, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Henson, M.C.; Castracane, V.D. Leptin in pregnancy: An update1. Biol. Reprod. 2006, 74, 218–229. [Google Scholar] [CrossRef]
- Easter, A.; Taborelli, E.; Bye, A.; Zunszain, P.A.; Pariante, C.M.; Treasure, J.; Schmidt, U.; Micali, N. Perinatal hypothalamic-pituitary-adrenal axis regulation among women with eating disorders and their infants. Psychoneuroendocrinology 2017, 76, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleger, F.; Linder, K.; Walter, L.; Heni, M.; Brändle, J.; Brucker, S.; Pauluschke-Fröhlich, J.; Weiss, M.; Häring, H.-U.; Preissl, H.; et al. Family history of diabetes is associated with delayed fetal postprandial brain activity. Front. Endocrinol. 2018, 9, 673. [Google Scholar] [CrossRef]
- Fehlert, E.; Willmann, K.; Fritsche, L.; Linder, K.; Mat-Husin, H.; Schleger, F.; Weiss, M.; Kiefer-Schmidt, I.; Brucker, S.; Häring, H.-U.; et al. Gestational diabetes alters the fetal heart rate variability during an oral glucose tolerance test: A fetal magnetocardiography study. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1891–1898. [Google Scholar] [CrossRef]
- Paslakis, G.; de Zwaan, M. Clinical management of females seeking fertility treatment and of pregnant females with eating disorders. Eur. Eat. Disord. Rev. 2019, 1–9. [Google Scholar] [CrossRef]


{kind=link}
| Source | Study Design | Country | Sample | ED Diagnosis | n | Prevalence of EDs | Outcome | Dietary Information |
|---|---|---|---|---|---|---|---|---|
| Nguyen et al., 2017 [31] | Cross-sectional analysis of the Generation R study | Netherlands | Pregnant women with and without a history of any ED | Self-reported questionnaire and clinical diagnoses (subsample; n = 928) during pregnancy | 6196 | 9.5% (n = 591) | Diet quality score, including 15 components and cut-offs (e.g., vegetables (≥200 g/day), dairy (≥300 g/day), red meat (≤375 g/week)) | Semi-quantitative modified 293-item FFQ at 13.6 weeks of gestation (12.4–16.2) |
| Main findings | Women with a history of EDs had a higher diet quality score than women without EDs | |||||||
| Micali et al., 2012 [29] | Cross-sectional analysis of the ALSPAC study | United Kingdom | Pregnant women with and without a lifetime AN, BN, and AN + BN (exclusion: non-singleton pregnancies, miscarriage) | Self-reported questionnaire at 12 weeks of gestation | 10,137 | 4.1% (n = 414); AN (n = 151); BN (n = 186); AN + BN (n = 77) | Frequency of consumption of various food groups, daily nutrient intakes (macronutrients), and dietary patterns | FFQ at 32 weeks of gestation; 14 food groups, 5 dietary patterns |
| Main findings (compared to control women) | 1. Women with lifetime ED:
| 2. Women with a lifetime AN:
| ||||||
| Siega-Riz et al., 2008 [30] | Cross-sectional analysis of the MoBA study | Norway | Pregnant women with and without lifetime BN and BED | Self-reported questionnaire 6 month before and during pregnancy (18.1 week of gestation) | 30,040 | 6.1% lifetime ED (n = 1840); 4.6% active ED (n = 1393); BN/BN (n = 59); BN/BED (n = 60); BED/BED (n = 650); none/BED (n = 624) | Nutrient and food group intakes | Semi-quantitative FFQ at gestational weeks 15–22; 255 questions, 20 food groups |
| Main findings (compared to control women) | 1. Women with BED before + during pregnancy:
| 2. Women with incident BED during pregnancy:
| ||||||
| Source | Study Design | Country | Sample | ED Diagnosis | n | Prevalence of EDs | Outcome | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Koubaa et al., 2015 [32] | Longitudinal cohort study (follow-up period: 1 year) | Sweden | Pregnant, nulliparous non-smoking women with and without a history of AN and BN | Interview according to DSM-IV diagnostic criteria; medical records | 96 | 38.5% (n = 37); AN (active AN: n = 8; past AN: n = 12); BN (active BN: n = 1; past BN: n = 16) | Maternal serum biomarkers of nutrition and stress at 10 weeks of gestation within a routine blood sample (ferritin, cortisol, TSH, T4, insulin, IGF-I and IGFBP1) | Women with previous AN:
|
| Linna et al., 2014 [15] | Register search study | Finland | Female ED patients and unexposed controls | Attending physicians at the clinic with ICD-10 (AN, BN, atypical AN/BN) and DSM-IV (BED) criteria | 4299 | 15.3% (n = 657); AN (n = 182); BN (n = 436); BED (n = 39) | Pregnancy complications (obtained from Medical Birth Register): gestational diabetes mellitus, initiation of insulin treatment, anemia, antenatal corticosteroid treatment, pregnancy-related ICD-10 diagnoses | Anemia was more frequent among women with AN (3.97%) compared with unexposed women (1.54%) |
| Dellava et al., 2013 [33] | Cross-sectional analysis of the MoBA study | Norway | Pregnant women across eating disorder subtypes compared with a referent group | Self-reported questionnaire at GW 19 | 37,307 | 6.3% (n = 2348); AN (n = 34); BN (n = 326); BED (n = 1944); EDNOS-P (n = 44) | Use of dietary supplements (checklist including 22 specific nutrients, at three time points prior to pregnancy (≥9 weeks, 8–5 weeks and 4–1 week before conception) and eight time periods during pregnancy (GW 1–4, 5–8, 9–12 13–16, 17–20, 21–24, 25–28, and 29+) | Dietary supplement use during pregnancy was as follows (between group differences were not statistically significant):
|
| Source | Study Design | Country | Sample | ED Diagnosis | n | Prevalence of EDs | Outcome | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Crow et al., 2008 [23] | Cross-sectional analysis of the McKnight Longitudinal Study of Eating Disorders | United States of America | Pregnant women with full/subthreshold AN, BN or BED | EDE | 42 | AN (n = 5; 11.9%); BN (n = 15; 35.7%); BED (n = 4; 9.5%); partial AN (n = 5; 11.9%); partial BN (n = 10; 23.8%); partial BED (n = 3; 7.1%) | Eating behaviors and disordered eating cognitions over the course of pregnancy | Frequency of objective binge eating episodes per 28 days intrapartum: 2.9 (vs. 8.7 prepartum) |
| Micali et al., 2007 [34] | Cross-sectional analysis of the ALSPAC study | United Kingdom | Pregnant women with and without recent/past AN, BN, AN + BN | Self-reported questionnaire at 12 weeks of gestation | 12,252 | 0.5% recent ED (n = 57; 6 AN, 51 BN); 3.2% past ED (n = 395; 167 AN, 158 BN, 70 AN + BN) | 18 GW: Self-induced vomiting, laxative use, exercise behavior, shape and weight concern; 32 GW: appraisals about weight gain during pregnancy, dieting, LOC | Dieting in pregnancy:
|
| Crow et al., 2004 [35] | Cross-sectional analysis of a longitudinal study (follow-up period: 10 – 15 years) | United States of America | Pregnant women with BN | EDI; SCID; Eating Disorders Questionnaire; self-report of BN symptoms | 129 | all BN | Bulimic symptoms, alcohol, drug, and tobacco use during pregnancy | Frequency of binge eating during pregnancy was rated as:
|
| Blais et al., 2000 [20] | Longitudinal Study | United States of America | Pregnant women with AN and BN | LIFE-EAT II every 6 month | 82 | 31,7% AN (AN-R: n = 7; AN-BP: n = 19); 68.3% BN (n = 56) | Pregnancy outcome (live birth, therapeutic/spontaneous abortion), ED symptomatology (restrictive eating, binging, etc.) | BN subjects: ↓ frequency of binging from prepregnancy to post-pregnancy AN subjects: No significant differences were seen for binging frequency and restrictive eating |
| Morgan et al., 1999 [37] | Retrospective analysis | United Kingdom | Pregnant women actively suffering from BN | EDE, SCID | 94 | all BN | Symptoms of bulimia nervosa and associated psychopathology at conception, each trimester and postnatally | Objective binge episodes improved with each passing trimester of pregnancy |
| Lemberg et al., 1989 [38] | Longitudinal study | United States of America | Pregnant women with an active AN, BN or mixed symptoms | Retrospective, 55-item questionnaire on ED symptoms and course of pregnancy | 43 | 57% AN-R; 77% BN; 16% combination of both | Eating behaviors both antenatal and postnatal | Women who restricted their intake (n = 36):
|
| Lacey et al., 1987 [36] | Longitudinal study | United Kingdom | Pregnant untreated BN women | St George’s Hospital eating disorder unit; DSM-III | 20 | all BN | Impact of pregnancy on dietary difficulties of the bulimic woman | 19 of the 20 subjects reduced frequency of binge eating over the course of pregnancy; only 5 patients were binge eating during the 3rd trimester; 75% having a complete cessation of binging by the 3rd trimester |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dörsam, A.F.; Preißl, H.; Micali, N.; Lörcher, S.B.; Zipfel, S.; Giel, K.E. The Impact of Maternal Eating Disorders on Dietary Intake and Eating Patterns during Pregnancy: A Systematic Review. Nutrients 2019, 11, 840. https://doi.org/10.3390/nu11040840
Dörsam AF, Preißl H, Micali N, Lörcher SB, Zipfel S, Giel KE. The Impact of Maternal Eating Disorders on Dietary Intake and Eating Patterns during Pregnancy: A Systematic Review. Nutrients. 2019; 11(4):840. https://doi.org/10.3390/nu11040840
Chicago/Turabian StyleDörsam, Annica F., Hubert Preißl, Nadia Micali, Sophia B. Lörcher, Stephan Zipfel, and Katrin E. Giel. 2019. "The Impact of Maternal Eating Disorders on Dietary Intake and Eating Patterns during Pregnancy: A Systematic Review" Nutrients 11, no. 4: 840. https://doi.org/10.3390/nu11040840