Socioeconomic Disparities in Diet Vary According to Migration Status among Adolescents in Belgium

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
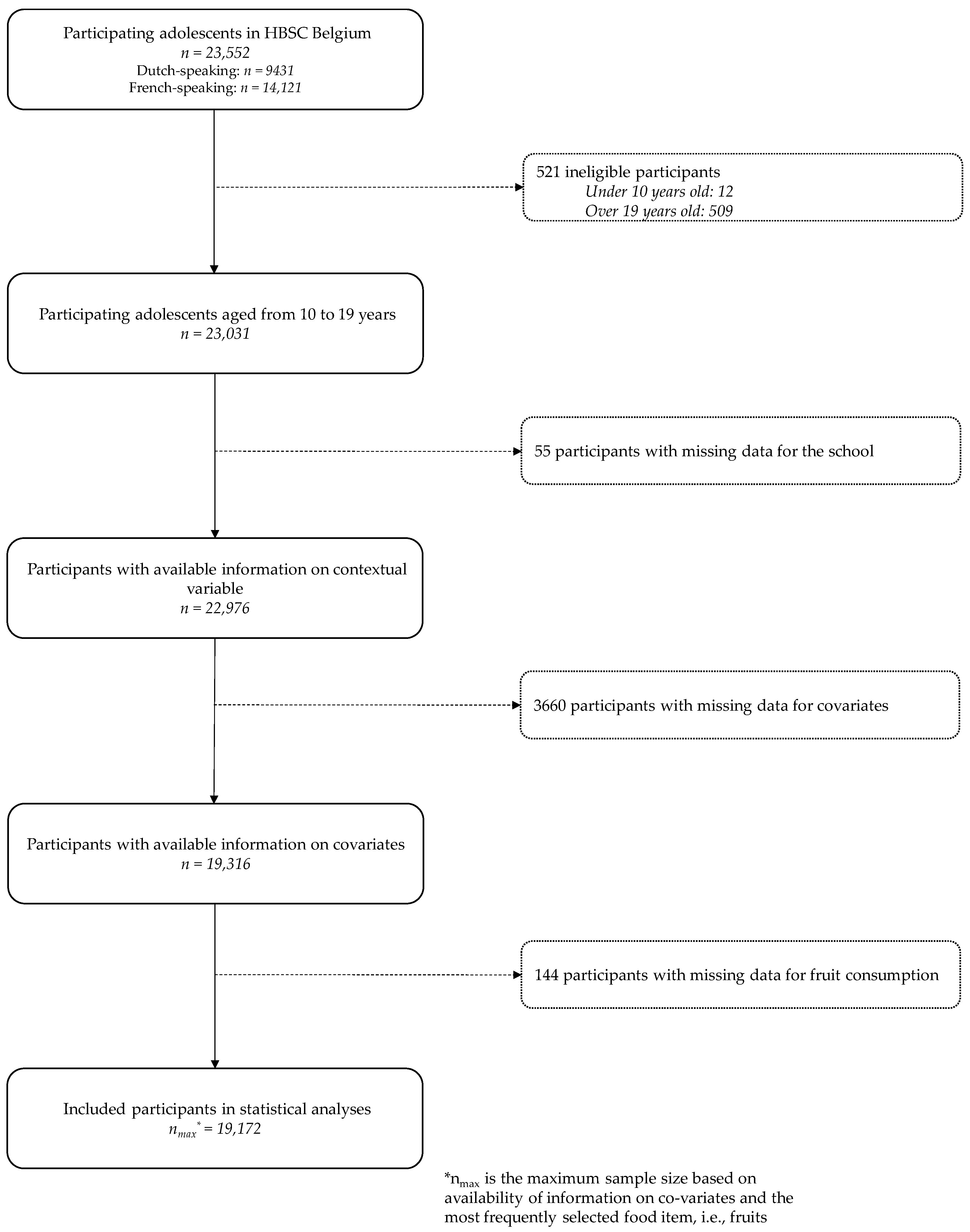
2.1. Sampling
2.2. Measures
2.3. Statistical Analyses
2.3.1. Reprocessing Data
2.3.2. Modeling
3. Results
3.1. Fruit Consumption (Reference Category: >Once a Day)
3.2. Vegetable Consumption (Reference Category: >Once a Day)
3.3. Fish Consumption (Reference Category: ≥Two Days a Week)
3.4. Dairy Product Consumption (Reference Category: >Once a Day)
3.5. Chips and Fries Consumption (Reference Category: <Once a Day)
3.6. Sugar-Sweetened Beverages (Reference Category: ≤Once a Week)
4. Discussion
4.1. Dietary Acculturation
4.2. Socioeconomic Disparities in Dietary Habits
4.3. Sociodemographic Disparities in Dietary Habits
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grootveld, M.; Percival, B.C.; Grootveld, K. Chronic Non-Communicable Disease Risks Presented by Lipid Oxidation Products in Fried Foods. HepatoBiliary Surg. Nutr. 2018, 7, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.-M.; Knuppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Fardet, A.; Rock, E. In vitro and in vivo antioxidant potential of milks, yoghurts, fermented milks and cheeses: A narrative review of evidence. Nutr. Res. Rev. 2018, 31, 52–70. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Dugravot, A.; Shipley, M.; Goldberg, M.; Zins, M.; Kivimäki, M.; Marmot, M.; Sabia, S.; Singh-Manoux, A. Health behaviours, socioeconomic status, and mortality: Further analyses of the British Whitehall II and the French GAZEL prospective cohorts. PLoS Med. 2011, 8, e1000419. [Google Scholar] [CrossRef]
- Méjean, C.; Droomers, M.; Van Der Schouw, Y.T.; Sluijs, I.; Czernichow, S.; Grobbee, D.E.; Bueno-de-Mesquita, H.B.; Beulens, J.W.J. The contribution of diet and lifestyle to socioeconomic inequalities in cardiovascular morbidity and mortality. Int. J. Cardiol. 2013, 168, 5190–5195. [Google Scholar] [CrossRef]
- Lien, N.; Jacobs, D.R.; Klepp, K.-I. Exploring predictors of eating behaviour among adolescents by gender and socio-economic status. Public Health Nutr. 2002, 5, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Kelder, S.H.; Perry, C.L.; Klepp, K.I.; Lytle, L.L. Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. Am. J. Public Health 1994, 84, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Mathers, J.C.; Rugg-Gunn, A.J.; Adamson, A.J. Longitudinal change in food habits between adolescence (11–12 years) and adulthood (32–33 years): The ASH30 Study. J. Public Health 2006, 28, 10–16. [Google Scholar] [CrossRef]
- Drouillet-Pinard, P.; Dubuisson, C.; Bordes, I.; Margaritis, I.; Lioret, S.; Volatier, J.-L. Socio-economic disparities in the diet of French children and adolescents: A multidimensional issue. Public Health Nutr. 2017, 20, 870–882. [Google Scholar] [CrossRef]
- Béghin, L.; Dauchet, L.; de Vriendt, T.; Cuenca-García, M.; Manios, Y.; Toti, E.; Plada, M.; Widhalm, K.; Repasy, J.; Huybrechts, I.; et al. Influence of parental socio-economic status on diet quality of European adolescents: Results from the HELENA study. Br. J. Nutr. 2014, 111, 1303–1312. [Google Scholar] [CrossRef]
- Allen, M.L.; Elliott, M.N.; Morales, L.S.; Diamant, A.L.; Hambarsoomian, K.; Schuster, M.A. Adolescent participation in preventive health behaviors, physical activity, and nutrition: Differences across immigrant generations for Asians and Latinos compared with Whites. Am. J. Public Health 2007, 97, 337–343. [Google Scholar] [CrossRef]
- Brown, A.G.M.; Houser, R.F.; Mattei, J.; Rehm, C.D.; Mozaffarian, D.; Lichtenstein, A.H.; Folta, S.C. Diet quality among US-born and foreign-born non-Hispanic blacks: NHANES 2003-2012 data. Am. J. Clin. Nutr. 2018, 107, 695–706. [Google Scholar] [CrossRef]
- Deboosere, P.; Gadeyne, S. Adult Migrant Mortality Advantage in Belgium: Evidence Using Census and Register Data. Population 2005, 655–698. [Google Scholar] [CrossRef]
- Neuman, S. Are immigrants healthier than native residents? IZA World Labor 2014. [Google Scholar] [CrossRef] [Green Version]
- Vandenheede, H.; Willaert, D.; de Grande, H.; Simoens, S.; Vanroelen, C. Mortality in adult immigrants in the 2000s in Belgium: A test of the ‘healthy-migrant’ and the ‘migration-as-rapid-health-transition’ hypotheses. Trop. Med. Int. Health 2015, 20, 1832–1845. [Google Scholar] [CrossRef]
- Barker, G.G. Choosing the best of both worlds: The acculturation process revisited. Int. J. Intercult. Relat. 2015, 45, 56–69. [Google Scholar] [CrossRef]
- Méjean, C.; Traissac, P.; Eymard-Duvernay, S.; Delpeuch, F.; Maire, B. Influence of acculturation among Tunisian migrants in France and their past/present exposure to the home country on diet and physical activity. Public Health Nutr. 2009, 12, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Llull, R.; Bibiloni, M.; Pons, A.; Tur, J.A. Food consumption patterns of Balearic Islands’ adolescents depending on their origin. J. Immigr. Minor Health 2015, 17, 358–366. [Google Scholar] [CrossRef]
- Te Velde, S.J.; Wind, M.; van Lenthe, F.J.; Klepp, K.-I.; Brug, J. Differences in fruit and vegetable intake and determinants of intakes between children of Dutch origin and non-Western ethnic minority children in the Netherlands—A cross sectional study. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 31. [Google Scholar] [CrossRef]
- Malmusi, D.; Borrell, C.; Benach, J. Migration-related health inequalities: Showing the complex interactions between gender, social class and place of origin. Soc. Sci. Med. 2010, 71, 1610–1619. [Google Scholar] [CrossRef]
- Pantzer, K.; Rajmil, L.; Tebé, C.; Codina, F.; Serra-Sutton, V.; Ferrer, M.; Ravens-Sieberer, U.; Simeoni, M.-C.; Alonso, J. Health related quality of life in immigrants and native school aged adolescents in Spain. J. Epidemiol. Community Health 2006, 60, 694–698. [Google Scholar] [CrossRef] [Green Version]
- Currie, C.; Griebler, R.; Inchley, J.; Theunissen, A.; Molcho, M.; Samdal, O.; Dür, W. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2009/10 Survey; CAHRU: St Andrews, Hong Kong, China, 2010. [Google Scholar]
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef]
- Vereecken, C.A.; Rossi, S.; Giacchi, M.V.; Maes, L. Comparison of a short food-frequency questionnaire and derived indices with a seven-day diet record in Belgian and Italian children. Int. J. Public Health 2008, 53, 297–305. [Google Scholar] [CrossRef]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C. Psychometric Validation of the Revised Family Affluence Scale: A Latent Variable Approach. Child. Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef]
- Conseil Supérieur de la Santé. Recommandations Nutritionnelles pour la Belgique 2016. Avis n°9285; Conseil Supérieur de la Santé: Bruxelles, Belgium, 2016. [Google Scholar]
- Hartwell, H.J.; Edwards, J.S.A.; Brown, L. Acculturation and food habits: Lessons to be learned. Br. Food J. 2011, 113, 1393–1405. [Google Scholar] [CrossRef]
- Raynor, H.A.; Vadiveloo, M. Understanding the Relationship Between Food Variety, Food Intake, and Energy Balance. Curr. Obes. Rep. 2018, 7, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, S.; Mavrikaki, E. Greek adolescents and the Mediterranean diet: Factors affecting quality and adherence. Nutrition 2015, 31, 345–349. [Google Scholar] [CrossRef]
- Skårdal, M.; Western, I.M.; Ask, A.M.S.; Øverby, N.C. Socioeconomic differences in selected dietary habits among Norwegian 13–14 year-olds: A cross-sectional study. Food Nutr. Res. 2014, 58. [Google Scholar] [CrossRef]
- Morris, M.A.; Hulme, C.; Clarke, G.P.; Edwards, K.L.; Cade, J.E. What is the cost of a healthy diet? Using diet data from the UK Women’s Cohort Study. J. Epidemiol. Community Health 2014, 68, 1043–1049. [Google Scholar] [CrossRef]
- Stewart, S.D.; Menning, C.L. Family structure, nonresident father involvement, and adolescent eating patterns. J. Adolesc. Health 2009, 45, 193–201. [Google Scholar] [CrossRef]
- Baek, Y.J.; Paik, H.Y.; Shim, J.E. Association between family structure and food group intake in children. Nutr. Res. Pract. 2014, 8, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Reicks, M.; Banna, J.; Cluskey, M.; Gunther, C.; Hongu, N.; Richards, R.; Topham, G.; Wong, S.S. Influence of Parenting Practices on Eating Behaviors of Early Adolescents during Independent Eating Occasions: Implications for Obesity Prevention. Nutrients 2015, 7, 8783–8801. [Google Scholar] [CrossRef] [Green Version]
- Bauer, K.W.; Hearst, M.O.; Escoto, K.; Berge, J.M.; Neumark-Sztainer, D. Parental employment and work-family stress: Associations with family food environments. Soc. Sci. Med. 2012, 75, 496–504. [Google Scholar] [CrossRef] [Green Version]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.M.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major Differences in Diet across Three Linguistic Regions of Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2017, 9, 1163. [Google Scholar] [CrossRef]
- Census/Statbel. Population par Lieu de Résidence (Province), Sexe, Position dans le Ménage (C), État Civil, Situation sur le Marché de L’emploi (A) et Lieu de Naissance (A). Available online: http://census2011.fgov.be/censusselection/selectionFR.html (accessed on 16 July 2018).
- Bere, E.; Brug, J.; Klepp, K.-I. Why do boys eat less fruit and vegetables than girls? Public Health Nutr. 2008, 11, 321–325. [Google Scholar] [CrossRef] [Green Version]
- Caine-Bish, N.L.; Scheule, B. Gender differences in food preferences of school-aged children and adolescents. J. Sch. Health 2009, 79, 532–540. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef]
- Salvy, S.-J.; Vartanian, L.R.; Coelho, J.S.; Jarrin, D.; Pliner, P.P. The role of familiarity on modeling of eating and food consumption in children. Appetite 2008, 50, 514–518. [Google Scholar] [CrossRef]
- McHale, S.M.; Updegraff, K.A.; Whiteman, S.D. Sibling Relationships and Influences in Childhood and Adolescence. J. Marriage Fam. 2012, 74, 913–930. [Google Scholar] [CrossRef] [Green Version]
- Berge, J.M.; Meyer, C.; Maclehose, R.F.; Crichlow, R.; Neumark-Sztainer, D. All in the Family: Correlations between Parents’ and Adolescent Siblings’ Weight and Weight-related Behaviors. Obesity 2015, 23, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Senguttuvan, U.; Whiteman, S.D.; Jensen, A.C. Family Relationships and Adolescents’ Health Attitudes and Weight: The Understudied Role of Sibling Relationships. Fam. Relat. 2014, 63, 384–396. [Google Scholar] [CrossRef] [Green Version]
- De Ridder, K.; Bel, S.; Brocatus, L.; Cuypers, K.; Lebacq, T.; Moyersoen, I.; Ost, C.; Teppers, E. Enquête de Consommation Alimentaire 2014-2015: Rapport 4: La Consommation Alimentaire. Available online: https://fcs.wiv-isp.be/nl/Gedeelde%20%20documenten/FRANS/Rapport%204/Resume_rapport_4_finaal_finaal.pdf (accessed on 13 August 2018).
- Moore, G.F.; Tapper, K.; Moore, L.; Murphy, S. Cognitive, behavioral, and social factors are associated with bias in dietary questionnaire self-reports by schoolchildren aged 9 to 11 years. J. Am. Diet. Assoc. 2008, 108, 1865–1873. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Sample | Natives | 2nd-Generation Immigrants | 1st-Generation Immigrants | p value |
|---|---|---|---|---|---|
| (n = 19,172) % | (n = 13,353) % | (n = 4214) % | (n = 1605) % | ||
| Gender | <0.001 † | ||||
| Boys | 50.6 | 51.5 | 47.5 | 51.7 | |
| Girls | 49.4 | 48.5 | 52.5 | 48.3 | |
| Age | <0.001 ¥ | ||||
| 10–12 years | 28.8 | 29.6 | 28.7 | 22.5 | |
| 13–16 years | 50.2 | 49.9 | 50.6 | 51.4 | |
| 17–19 years | 21.0 | 20.5 | 20.7 | 26.1 | |
| Family structure a | <0.001 | ||||
| Two parents | 66.4 | 66.1 | 67.9 | 65.0 | |
| Blended family | 14.1 | 15.8 | 9.9 | 12.0 | |
| Single-parent family | 19.5 | 18.1 | 22.2 | 23.0 | |
| Family Affluence Scale a | <0.001 | ||||
| High | 19.4 | 20.6 | 17.0 | 16.4 | |
| Medium | 63.7 | 66.1 | 59.8 | 53.6 | |
| Low | 16.9 | 13.3 | 23.2 | 30.0 | |
| Parental working status a | <0.001 | ||||
| Both parents working | 68.4 | 76.1 | 51.9 | 47.0 | |
| One working, the other at home | 17.4 | 13.4 | 27.8 | 23.7 | |
| One working, the other not at home | 8.1 | 7.2 | 8.5 | 14.0 | |
| None working | 6.1 | 3.3 | 11.8 | 15.3 | |
| Siblings | <0.001 † | ||||
| Single child | 9.3 | 9.8 | 7.5 | 10.5 | |
| Siblings | 90.7 | 90.2 | 92.5 | 89.5 | |
| School Region | <0.001 | ||||
| Brussels-Capital | 11.4 | 3.4 | 29.2 | 31.7 | |
| Wallonia | 46.6 | 48.7 | 43.0 | 38.2 | |
| Flanders | 42.0 | 47.9 | 27.8 | 30.1 | |
| Geographical area of origin | <0.001 * | ||||
| Europe | 43.7 | 59.8 | |||
| America | 3.0 | 6.7 | |||
| Asia | 7.3 | 7.7 | |||
| Middle East and South Africa | 36.0 | 13.1 | |||
| Sub-Saharan Africa | 10.0 | 12.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouche, M.; de Clercq, B.; Lebacq, T.; Dierckens, M.; Moreau, N.; Desbouys, L.; Godin, I.; Castetbon, K. Socioeconomic Disparities in Diet Vary According to Migration Status among Adolescents in Belgium. Nutrients 2019, 11, 812. https://doi.org/10.3390/nu11040812
Rouche M, de Clercq B, Lebacq T, Dierckens M, Moreau N, Desbouys L, Godin I, Castetbon K. Socioeconomic Disparities in Diet Vary According to Migration Status among Adolescents in Belgium. Nutrients. 2019; 11(4):812. https://doi.org/10.3390/nu11040812
Chicago/Turabian StyleRouche, Manon, Bart de Clercq, Thérésa Lebacq, Maxim Dierckens, Nathalie Moreau, Lucille Desbouys, Isabelle Godin, and Katia Castetbon. 2019. "Socioeconomic Disparities in Diet Vary According to Migration Status among Adolescents in Belgium" Nutrients 11, no. 4: 812. https://doi.org/10.3390/nu11040812