Factors Associated with Serum 25-Hydroxyvitamin D Concentration in Two Cohorts of Pregnant Women in Southern Ontario, Canada

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Maternal Data Collection
2.3. Vitamin D Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographics and Physical Characteristics
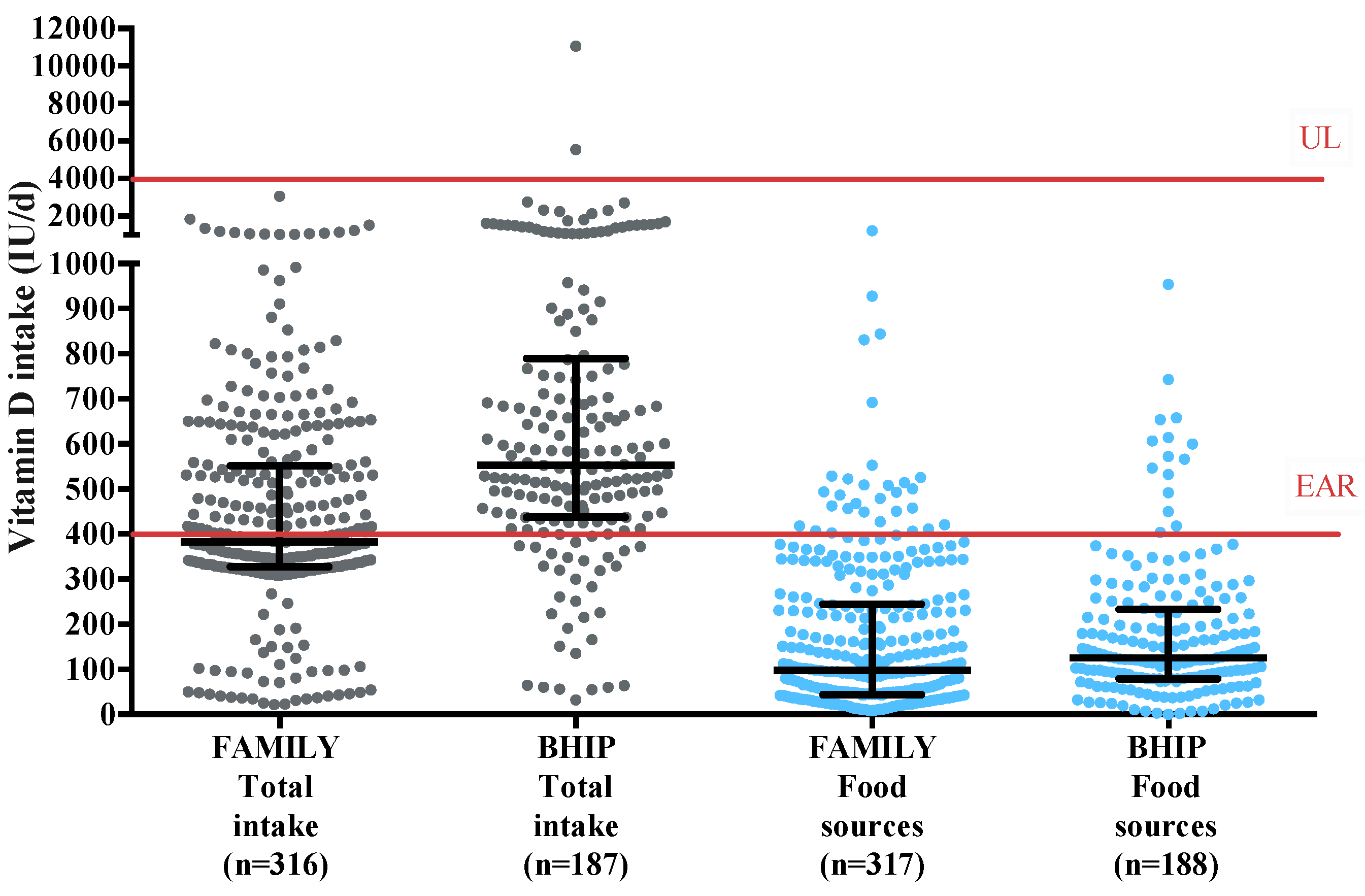
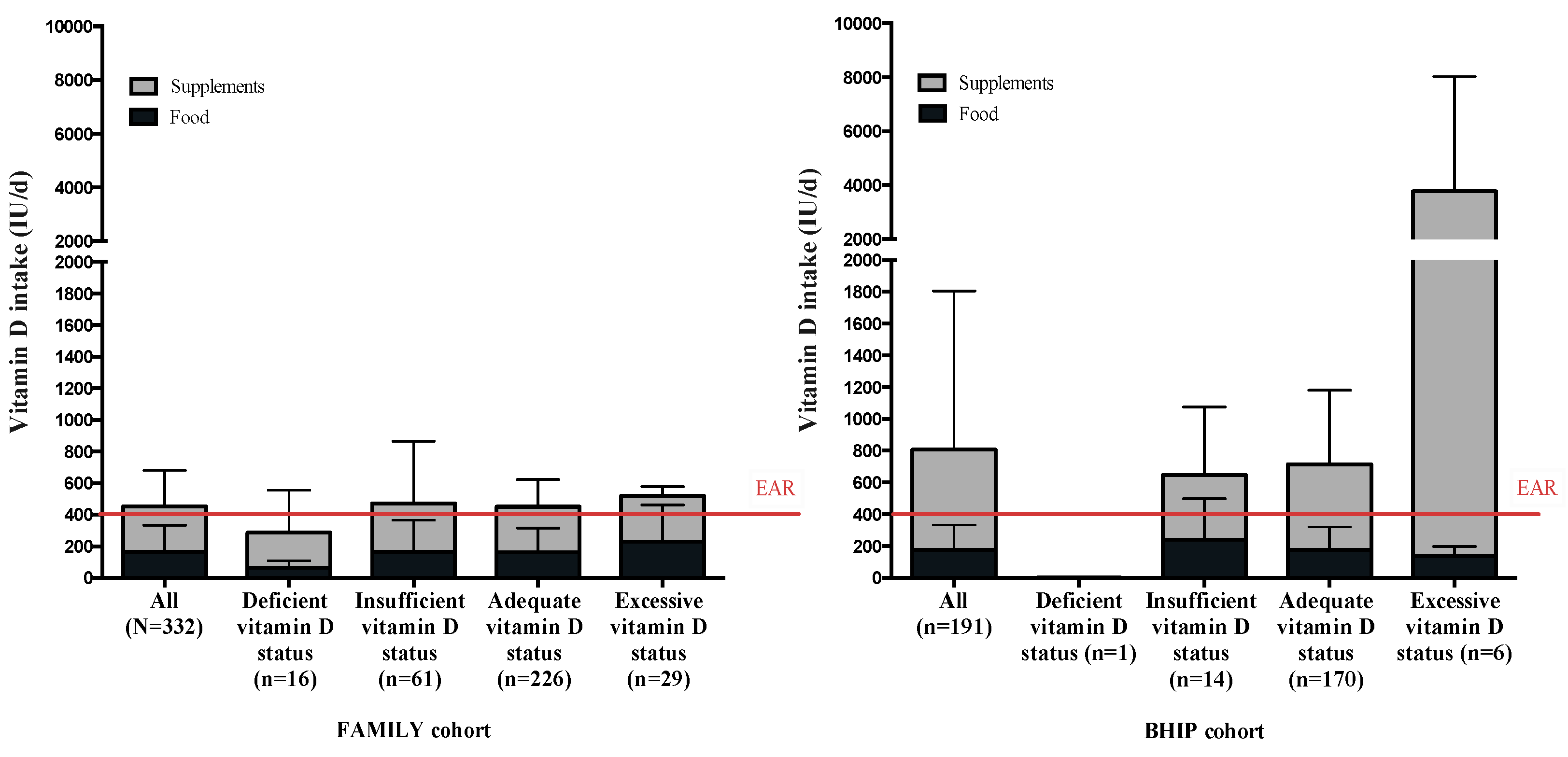
3.2. Intake of Vitamin D in Both Studies: Trend Over 10 Years
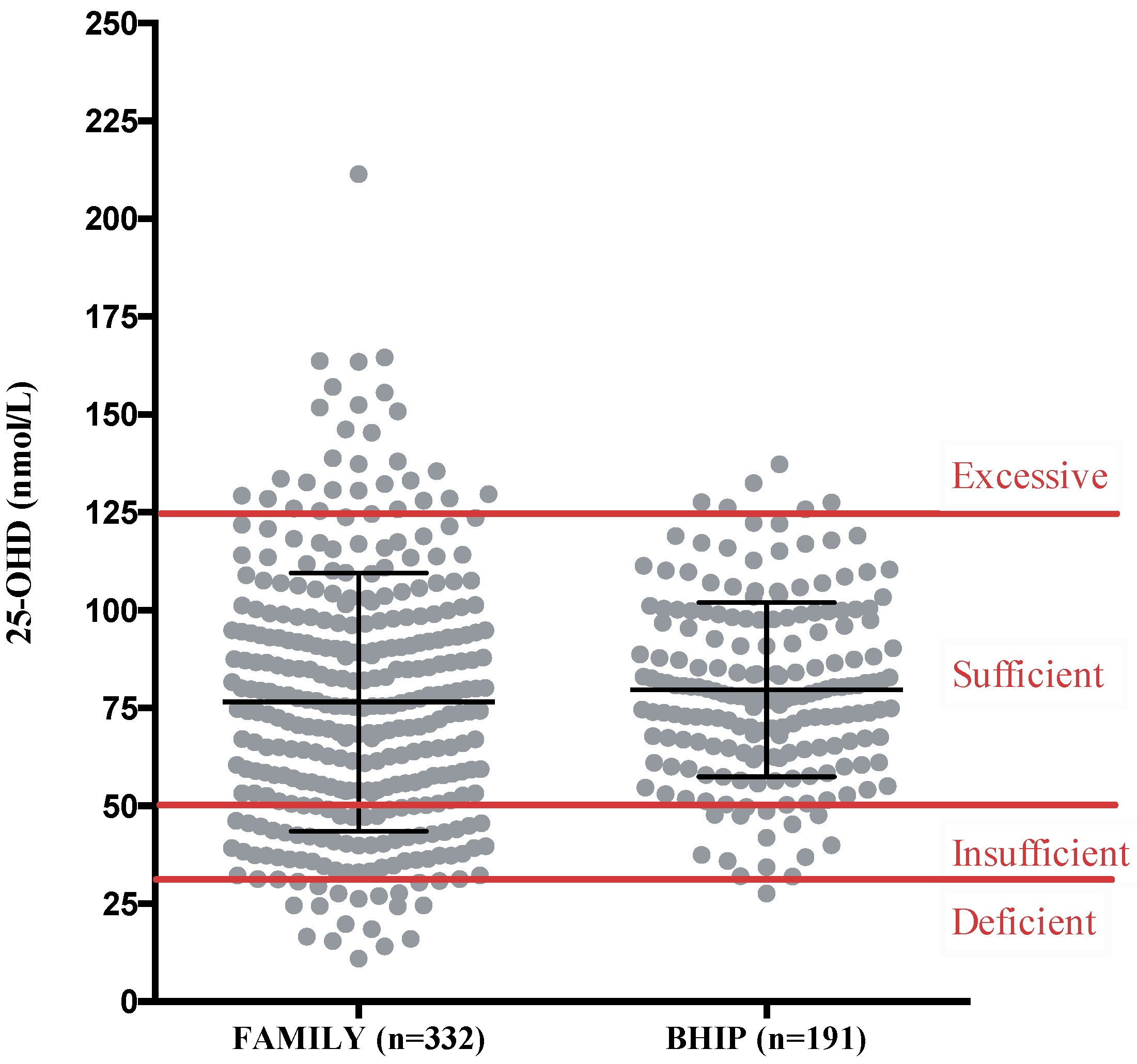
3.3. Maternal Serum 25-OHD Concentration during Pregnancy
3.4. Factors Associated with Maternal Serum 25-OHD Concentrations in Pregnancy
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heyden, E.L.; Wimalawansa, S.J. Vitamin D: Effects on human reproduction, pregnancy, and fetal well-being. J. Steroid Biochem. Mol. Biol. 2017, 180, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Larqué, E.; Morales, E.; Leis, R.; Blanco-Carnero, J.E. Maternal and foetal health implications of vitamin D status during pregnancy. Ann. Nutr. Metab. 2018, 72, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. Maternal vitamin D supplementation during pregnancy. Br. Med. Bull. 2018, 126, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Calcium, phosphorus, and bone metabolism in the fetus and newborn. Early Hum. Dev. 2015, 11, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Thorne-Lyman, A.; Fawzi, W.W. Vitamin D during pregnancy and maternal, neonatal and infant health outcomes: A systematic review and meta-analysis. Paediatr. Perinat. Epidemiol. 2012, 26, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.G.; Nuyt, A.M.; Weiler, H.; Leduc, L.; Santamaria, C.; Wei, S.Q. Association between vitamin D supplementation during pregnancy and offspring growth, morbidity, and mortality. JAMA Pediatr. 2018, 172, 635–645. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.; Palacios, C.; Lombardo, L.; Peña-Rosas, J. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Viljakainen, H.T.; Saarnio, E.; Hytinantti, T.; Miettinen, M.; Surcel, H.; Mäkitie, O.; Andersson, S.; Laitinen, K.; Lamberg-Allardt, C. Maternal vitamin D status determines bone variables in the newborn. J. Clin. Endocrinol. Metab. 2010, 95, 1749–1757. [Google Scholar] [CrossRef]
- Javaid, M.K.; Crozier, S.R.; Harvey, N.C.; Gale, C.R.; Dennison, E.M.; Boucher, B.J.; Arden, N.K.; Godfrey, K.M.; Cooper, C.; Princess Anne Hospital Study, G. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef]
- Viljakainen, H.T.; Korhonen, T.; Hytinantti, T.; Laitinen, E.K.A.; Andersson, S.; Mäkitie, O.; Lamberg-Allardt, C. Maternal vitamin D status affects bone growth in early childhood—A prospective cohort study. Osteoporos. Int. 2011, 22, 883–891. [Google Scholar] [CrossRef]
- Zhu, K.; Whitehouse, A.J.; Hart, P.H.; Kusel, M.; Mountain, J.; Lye, S.; Pennell, C.; Walsh, J.P. Maternal vitamin D status during pregnancy and bone mass in offspring at 20 years of age: A prospective cohort study. J. Bone Min. Res. 2014, 29, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Godel, J.C.; Canadian Paediatric Society; First Nations, Inuit and Métis Health Committee. Vitamin D supplementation: Recommendations for Canadian mothers and infants. Paediatr. Child Health 2007, 12, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Hollis, B.W. Vitamin D supplementation during pregnancy: Double-blind, randomized clinical trial of safety and effectiveness. J. Bone Miner. Res. 2011, 26, 2341–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.; Taylor, C.; Yaktine, A. Dietary Reference Intakes for Vitamin D and Calcium; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Scientific Advisory Committee on Nutrition. Vitamin D and Health; Assets Publishing Service: London, UK, 2016. [Google Scholar]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA) Dietary reference values for vitamin D. EFSA J. 2016, 14, e04547. [CrossRef]
- Morrison, K.M.; Atkinson, S.A.; Yusuf, S.; Bourgeois, J.; McDonald, S.; McQueen, M.J.; Persadie, R.; Hunter, B.; Pogue, J.; Teo, K. The Family Atherosclerosis Monitoring In earLY life (FAMILY) study. Rationale, design, and baseline data of a study examining the early determinants of atherosclerosis. Am. Heart J. 2009, 158, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Perreault, M.; Atkinson, S.A.; Mottola, M.F.; Phillips, S.M.; Bracken, K.; Hutton, E.K.; Xie, F.; Meyre, D.; Morassut, R.E.; Prapavessis, H.; et al. Structured diet and exercise guidance in pregnancy to improve health in women and their offspring: Study protocol for the Be Healthy in Pregnancy (BHIP) randomized controlled trial. Trials 2018, 19, 691. [Google Scholar] [CrossRef] [PubMed]
- Health Canada Prenatal Nutrition Guidelines for Health Professionals, Gestational Weight Gain. Available online: http://www.hc-sc.gc.ca/fn-an/alt_formats/pdf/nutrition/prenatal/ewba-mbsa-eng.pdf 2010 (accessed on 24 January 2013).
- Anand, S.S.; Yusuf, S.; Vuksan, V.; Devanesen, S.; Montague, P.; Kelemen, L.; Bosch, J.; Sigouin, C.; Teo, K.K.; Lonn, E.; et al. The Study of Health Assessment and Risk in Ethnic groups (SHARE): Rationale and design. The SHARE Investigators. Can. J. Cardiol. 1998, 14, 1349–1357. [Google Scholar]
- Kelemen, L.E.; Anand, S.S.; Vuksan, V.; Yi, Q.; Teo, K.K.; Devanesen, S.; Yusuf, S.; Investigators, S. Development and evaluation of cultural food frequency questionnaires for South Asians, Chinese, and Europeans in North America. J. Am. Diet. Assoc. 2003, 103, 1178–1184. [Google Scholar] [CrossRef]
- Merchant, A.T.; Kelemen, L.E.; De Koning, L.; Lonn, E.; Vuksan, V.; Jacobs, R.; Davis, B.; Teo, K.K.; Yusuf, S.; Anand, S.S. Interrelation of saturated fat, trans fat, alcohol intake, and subclinical atherosclerosis. Am. J. Clin. Nutr. 2008, 87, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Mottola, M.F.; Giroux, I.; Gratton, R.; Hammond, J.A.; Hanley, A.; Harris, S.; McManus, R.; Davenport, M.H.; Sopper, M.M. Nutrition and exercise prevent excess weight gain in overweight pregnant women. Med. Sci. Sport. Exerc. 2010, 42, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Held, C.; Iqbal, R.; Lear, S.A.; Rosengren, A.; Islam, S.; Mathew, J.; Yusuf, S. Physical activity levels, ownership of goods promoting sedentary behaviour and risk of myocardial infarction: Results of the INTERHEART study. Eur. Heart J. 2012, 33, 452–466. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.; Wolfe, L.; Mottola, M.; MacKinnon, C. Joint SOGC/CSEP clinical practice guideline: Exercise in pregnancy and the postpartum period. Can. J. Appl. Physiol. 2003, 28, 330–341. [Google Scholar] [CrossRef] [PubMed]
- The Analysis of 25-Hydroxyvitamin D in Serum Using UPLC/MS/MS. Available online: http://www.waters.com/webassets/cms/library/docs/720002748_vit_d_application_note.pdf (accessed on 7 January 2019).
- Hymøller, L.; Jensen, S.K. Vitamin D analysis in plasma by high performance liquid chromatography (HPLC) with C30 reversed phase column and UV detection—Easy and acetonitrile-free. J. Chromatogr. A 2011, 1218, 1835–1841. [Google Scholar] [CrossRef] [PubMed]
- Perichart-Perera, O.; Muñoz-Manrique, C.; Reyes-López, A.; Tolentino-Dolores, M.; Espino Y Sosa, S.; Ramírez-González, M.C. Metabolic markers during pregnancy and their association with maternal and newborn weight status. PLoS ONE 2017, 12, e0180874. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Langlois, K.; Greene-Finestone, L.; Little, J.; Hidiroglou, N.; Whiting, S. Vitamin D status of Canadians as measured in the 2007 to 2009 Canadian Health Measures Survey. Stat. Can. 2010, 21, 47–55. [Google Scholar]
- Moon, R.J.; Harvey, N.C.; Cooper, C.; D ’angelo, S.; Crozier, S.R.; Inskip, H.M.; Schoenmakers, I.; Prentice, A.; Arden, N.K.; Bishop, N.J.; et al. Determinants of the maternal 25-hydroxyvitamin D response to vitamin D supplementation during pregnancy. J. Clin. Endocrinol. Metab. 2016, 101, 5012–5020. [Google Scholar] [CrossRef]
- Morisset, A.-S.; Weiler, H.A.; Dubois, L.; Ashley-Martin, J.; Shapiro, G.D.; Dodds, L.; Massarelli, I.; Vigneault, M.; Arbuckle, T.E.; Fraser, W.D. Rankings of iron, vitamin D, and calcium intakes in relation to maternal characteristics of pregnant Canadian women. Appl. Physiol. Nutr. Metab. 2016, 41, 749–757. [Google Scholar] [CrossRef]
- Dubois, L.; Diasparra, M.; Bédard, B.; Colapinto, C.K.; Fontaine-Bisson, B.; Tremblay, R.E.; Fraser, W.D. Adequacy of nutritional intake during pregnancy in relation to prepregnancy BMI: Results from the 3D Cohort Study. Br. J. Nutr. 2018, 120, 335–344. [Google Scholar] [CrossRef]
- Li, W.; Green, T.J.; Innis, S.M.; Barr, S.I.; Whiting, S.J.; Shand, A.; von Dadelszen, P. Suboptimal vitamin D levels in pregnant women despite supplement use. Can. J. Public Health 2011, 102, 308–312. [Google Scholar]
- Gomez, M.F.; Field, C.J.; Olstad, D.L.; Loehr, S.; Ramage, S.; Mccargar, L.J.; Kaplan, B.J.; Dewey, D.; Bell, R.C.; Bernier, F.P.; et al. Use of micronutrient supplements among pregnant women in Alberta: Results from the Alberta Pregnancy Outcomes and Nutrition (APrON) cohort. Matern. Child Nutr. 2015, 11, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Aghajafari, F.; Field, C.J.; Kaplan, B.J.; Rabi, D.M.; Maggiore, J.A.; O’Beirne, M.; Hanley, D.A.; Eliasziw, M.; Dewey, D.; Weinberg, A.; et al. The current recommended vitamin D intake guideline for diet and supplements during pregnancy is not adequate to achieve vitamin D sufficiency for most pregnant women. PLoS ONE 2016, 11, e0157262. [Google Scholar] [CrossRef] [PubMed]
- Savard, C.; Lemieux, S.; Weisnagel, S.J.; Fontaine-Bisson, B.; Gagnon, C.; Robitaille, J.; Morisset, A.S. Trimester-specific dietary intakes in a sample of French-Canadian pregnant women in comparison with national nutritional guidelines. Nutrients 2018, 10, 768. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, C.G.; Giguère, Y.; Weiler, H.A.; Spencer, A.; Forest, J.C.; Armson, B.A.; Dodds, L. Determinants of vitamin D status in pregnant women and neonates. Can. J. Public Health 2016, 107, e410–e416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, D.E.; Leung, M.; Mesfin, E.; Qamar, H.; Watterworth, J.; Papp, E. Vitamin D supplementation during pregnancy: State of the evidence from a systematic review of randomised trials. BMJ 2017, 359, j5237. [Google Scholar] [CrossRef] [PubMed]
- Eggemoen, Å.R.; Jenum, A.K.; Mdala, I.; Knutsen, K.V.; Lagerlov, P.; Sletner, L. Vitamin D levels during pregnancy and associations with birth weight and body composition of the newborn: A longitudinal multiethnic population-based study. Br. J. Nutr. 2017, 117, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.C.; Holroyd, C.; Ntani, G.; Javaid, K.; Cooper, P.; Moon, R.; Cole, Z.; Tinati, T.; Godfrey, K.; Dennison, E.; et al. Vitamin D supplementation in pregnancy: A systematic review. Health Technol. Assess. 2014, 18, 1–190. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef]
- Wei, S.; Qi, H.; Luo, Z.; Fraser, W. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Boyle, V.T.; Thorstensen, E.B.; Mourath, D.; Jones, M.B.; McCowan, L.M.E.; Kenny, L.C.; Baker, P.N. The relationship between 25-hydroxyvitamin D concentration in early pregnancy and pregnancy outcomes in a large, prospective cohort. Br. J. Nutr. 2016, 116, 1409–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghajafari, F.; Field, C.J.; Kaplan, B.J.; Maggiore, J.A.; O’Beirne, M.; Hanley, D.A.; Eliasziw, M.; Dewey, D.; Ross, S.; Rabi, D. The high prevalence of vitamin D insufficiency in cord blood in Calgary, Alberta (APrON-D Study). J. Obstet. Gynaecol. Can. 2017, 39, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Hollis, B.W. The Implications of Vitamin D Status During Pregnancy on Mother and her Developing Child. Front. Endocrinol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Taylor, S.N.; Dawodu, A.; Johnson, D.D.; Hollis, B.W. Vitamin D and its role during pregnancy in attaining optimal health of mother and fetus. Nutrients 2012, 4, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Hauta-alus, H.H.; Kajantie, E.; Holmlund-Suila, E.M.; Rosendahl, J.; Valkama, S.M.; Enlund-Cerullo, M.; Helve, O.M.; Hytinantti, T.K.; Viljakainen, H.; Andersson, S.; et al. High pregnancy, cord blood and infant vitamin D concentrations may predict slower infant growth. J. Clin. Endocrinol. Metab. 2019, 104, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Makitie, O.; et al. Global consensus recommendations on prevention and management of nutritional rickets. Horm. Res. Paediatr. 2016, 85, 83–106. [Google Scholar] [CrossRef] [PubMed]
- Governement of Canada Summary of Proposed Amendments, Part I: Nutrition Symbols, Other Labelling Provisions, Partially Hydrogenated Oils and Vitamin D. Available online: https://www.canada.ca/en/health-canada/programs/consultation-front-of-package-nutrition-labelling-cgi/summary-of-proposed-amendments.html (accessed on 21 December 2018).
- Zerwekh, J.E. Blood biomarkers of vitamin D status. Am. J. Clin. Nutr. 2008, 87, 1087–1091. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| FAMILY Study N = 332 | BHIP Study N = 191 | |||
|---|---|---|---|---|
| Maternal Characteristics | N | (%) | N | (%) |
| Gestational age | 24–36 weeks | 12–17 weeks | ||
| Pre-pregnancy BMI (kg/m2) | ||||
| Underweight (<18.5) | 4 | 1 | 3 | 1 |
| Normal weight (18.5–24.9) | 144 | 45 | 91 | 48 |
| Overweight (25.0–29.9) | 103 | 32 | 61 | 32 |
| Obese (≥30) | 69 | 22 | 36 | 19 |
| Unknown | 12 | - | 0 | - |
| Ethnicity | ||||
| European descent | 285 | 86 | 171 | 90 |
| Other | 47 | 14 | 20 | 10 |
| Household income (CAD) | ||||
| <$50,000 | 68 | 21 | 15 | 8 |
| $50,000–$99,999 | 138 | 43 | 91 | 48 |
| ≥$100,000 | 111 | 35 | 79 | 41 |
| Unknown | 15 | 1 | 6 | 3 |
| Education (years) | ||||
| ≤13 | 46 | 14 | 0 | 0 |
| >13 | 286 | 86 | 191 | 100 |
| Smoking status | ||||
| Smoked during pregnancy | 10 | 3 | 0 | 0 |
| Former smoker; quit before pregnancy | 107 | 33 | n/a | n/a |
| Never smoked | 212 | 64 | n/a | n/a |
| Unknown | 3 | - | n/a | n/a |
| Exercise at study entry | ||||
| Not currently exercising | 49 | 15 | 42 | 22 |
| Currently exercising | 283 | 85 | 147 | 77 |
| Missing data | 0 | - | 2 | 1 |
| FAMILY Study | BHIP Study | |||||
|---|---|---|---|---|---|---|
| Category | Serum 25-OHD, nmol/L Mean (SD) (95% CI) | N (%) | p-value | Serum 25-OHD, nmol/L Mean (SD) (95% CI) | N (%) | p-value |
| All participants | 76.5 (32.9) (72.9, 80.1) | 332 | - | 79.7 (22.3) (76.5, 82.9) | 191 | - |
| Season of blood draw | 0.0001 | 0.0002 | ||||
| Summer (May–Oct.) | 83.47 (34.3) (78.3, 88.7) | 169 (51) | 84.9 (21.0) (80.9, 89.0) | 106 (55) | ||
| Winter (Nov–Apr.) | 68.5 (29.3) (63.9, 73.1) | 160 (48) | 73.2 (22.2) (68.4, 78.0) | 85 (45) | ||
| Missing data | - | 3 (1) | - | - | ||
| Pre-pregnancy BMI (kg/m2) | 0.11 | 0.10 | ||||
| Underweight (<18.5) | 72.2 (44.3) (1.6, 142.8) | 4 (1) | 90.3 (15.1) (52.6, 127.9) | 3 (1) | ||
| Normal (18.5–24.9) | 79.5 (33.4) (74.0, 85.0) | 144 (43) | 82.2 (21.2) (77.8, 86.5) | 93 (49) | ||
| Overweight (25.0–29.9) | 78.3 (33.7) (71.7, 84.9) | 103 (31) | 73.8 (20.5) (68.4, 79.2) | 58 (31) | ||
| Obese (≥30) | 68.1 (30.0) (60.9, 75.3) | 69 (21) | 81.8 (26.6) (90.7, 73,0) | 37 (19) | ||
| Missing data | - | 12 (4) | - | - | ||
| Variables | FAMILY Study | BHIP Study | ||||
|---|---|---|---|---|---|---|
| Estimated Coefficient | 95% CI | p-Value | Estimated Coefficient | 95% CI | p-Value | |
| Ethnicity (European descent as reference) | −5.85 | −10.97, −0.72 | 0.025 | −5.91 | −12.44, 0.61 | 0.075 |
| Season of blood draw for baseline blood (Winter as reference) | 7.73 | 4.27, 11.18 | <0.001 | 8.27 | 4.44, 12.09 | <0.001 |
| Exercising at enrollment | 0.53 | −5.73, 4.66 | 0.840 | 3.08 | −1.72, 7.88 | 0.206 |
| Pre-pregnancy BMI | −0.92 | −1.52, −0.31 | 0.003 | −0.37 | −1.19, 0.46 | 0.381 |
| Total vitamin D intake | −0.01 | −0.04, 0.02 | 0.469 | −0.01 | −0.04, 0.02 | 0.451 |
| Vitamin D intake from supplement | 0.01 | −0.02, 0.05 | 0.422 | 0.02 | −0.01, 0.05 | 0.174 |
| Vitamin D intake from milk | 1.03 | −3.97, 6.02 | 0.687 | 0.03 | −0.03, 0.10 | 0.272 |
| Vitamin D intake from low fat dairy products | 4.19 | −0.43, 8.82 | 0.076 | - | - | - |
| Vitamin D intake from regular fat dairy products (sour cream, cream, ice cream, cheese) | −2.11 | −5.99, 1.77 | 0.285 | 0.44 | 0.08, 0.81 | 0.017 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perreault, M.; Moore, C.J.; Fusch, G.; Teo, K.K.; Atkinson, S.A. Factors Associated with Serum 25-Hydroxyvitamin D Concentration in Two Cohorts of Pregnant Women in Southern Ontario, Canada. Nutrients 2019, 11, 123. https://doi.org/10.3390/nu11010123
Perreault M, Moore CJ, Fusch G, Teo KK, Atkinson SA. Factors Associated with Serum 25-Hydroxyvitamin D Concentration in Two Cohorts of Pregnant Women in Southern Ontario, Canada. Nutrients. 2019; 11(1):123. https://doi.org/10.3390/nu11010123
Chicago/Turabian StylePerreault, Maude, Caroline J. Moore, Gerhard Fusch, Koon K. Teo, and Stephanie A. Atkinson. 2019. "Factors Associated with Serum 25-Hydroxyvitamin D Concentration in Two Cohorts of Pregnant Women in Southern Ontario, Canada" Nutrients 11, no. 1: 123. https://doi.org/10.3390/nu11010123