Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
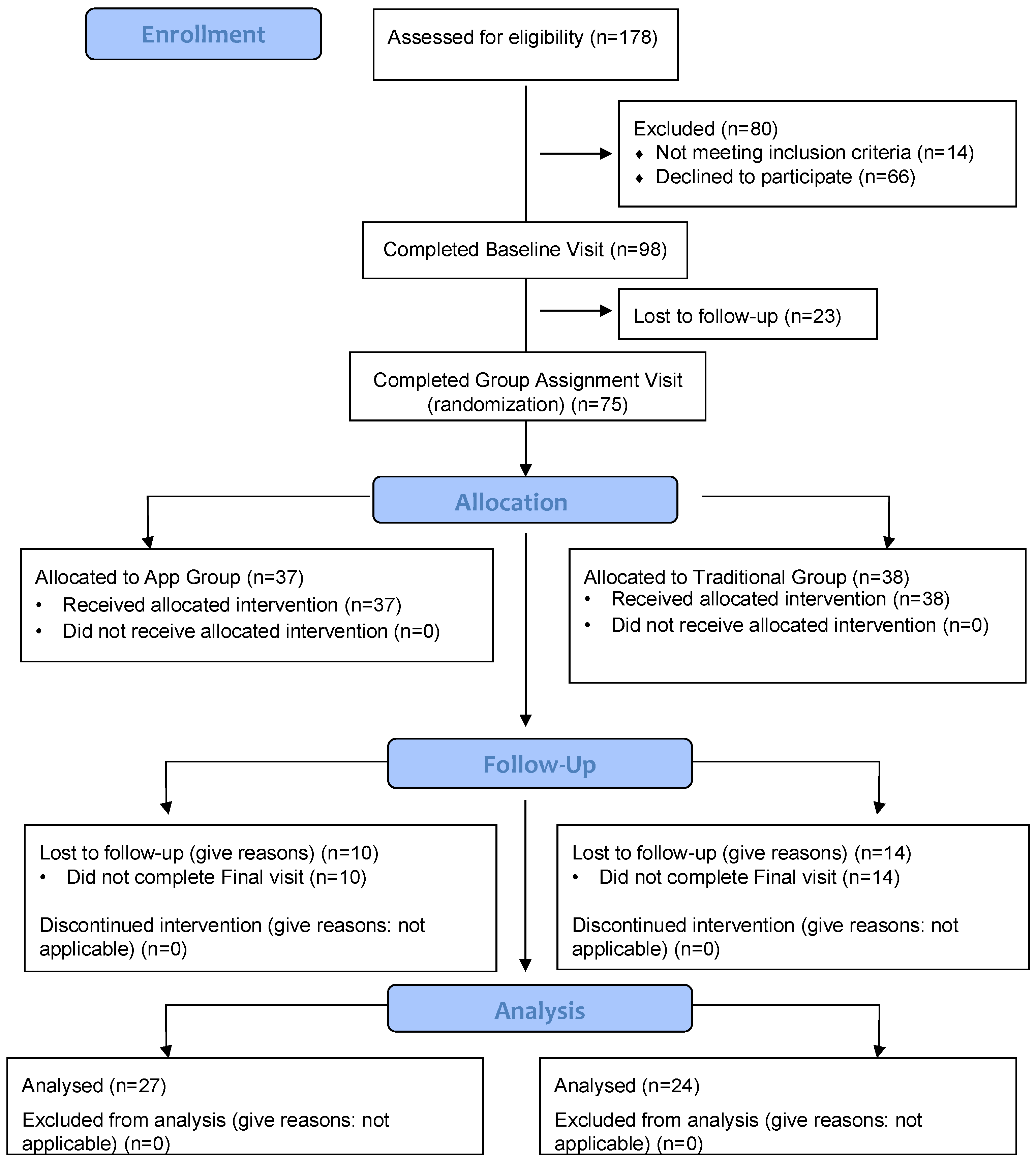
2.1. Study Design
2.2. Participants, Eligibility, and Recruitment
2.3. Intervention Groups
2.3.1. “MyNutriCart” (App Group)
- Estimation of energy requirements for each family member based on age, sex, and physical activity using the equations from the Dietary Reference Intakes [14]. The app automatically subtracted 500 kcals from the total calculated energy requirement for study participants only (not family members) to allow for a weight loss of about 1 pound/week [15];
- General food recommendations from the DGA [2], such as consumption of half of the grains as whole grains and low-fat dairy products, in addition to a variety of protein foods (beans, eggs, poultry, fish, and seashells);
- Number of servings per food group, based on the caloric level of each member, as recommended by the DGA [2]. Servings of each food group from each member were added to get a total of each food group per day;
- Intended number of days of the shopping event to multiply the servings per food group to get a total of foods to purchase;
- Participant’s pre-specified budget and weekly discounts offered by the largest local supermarkets (which was retrieved from an independent and free website service) to maximize the budget;
- Sample menus for each caloric level of the household based on local preferences, which were previously designed by a registered dietitian (RD).
2.3.2. Traditional Nutritional Counseling (Traditional Group)
2.4. Instruments and Measures
- Food frequency questionnaire (FFQ). We used a short version of the Tucker’s semi-quantitative FFQ, which was validated in Puerto Rican adults [18]. The questionnaire was interview-administered, and respondents were asked to estimate the frequency of food consumption from 10 categories (daily, weekly, monthly), using the preceding eight weeks as the reference period. Summary questions for the frequency of consumption of the following food groups: fruits, vegetables, starchy vegetables, refined and whole grains, legumes, healthy proteins, red meats, cold cuts and cured meats, whole-fat and low-fat dairy products, 100% fruit juices, and SSB were conducted.
- Intake of foods using three 24-h dietary recalls. These were conducted during 2 non-consecutive weekdays and one weekend day using the Nutrition Data System for Research multi-pass method (5 steps) (Version 25, 2014) [19]. The baseline 24-h recalls were done before participants were informed about their group assignment; one was done in person at the baseline visit and the other 2 recalls were done by phone in the following 2–3 days. For the post-intervention recalls, we completed the first 2 by phone and the last one when they came to the post-intervention visit. For the first recall, we used a portion size booklet displaying standardized food servings as a visual aid for participants to estimate their usual portion sizes. A copy of this booklet was provided to each participant to take home to help in estimating portion sizes when we called them to complete the other recalls by phone. Intake (in servings) from the following food groups were averaged for the 3 days for both baseline and post-intervention recalls: fruits, vegetables, starchy vegetables, refined and whole grains, legumes, healthy proteins, red meats, cold cuts and cured meats, whole-fat and low-fat dairy products, 100% fruit juices, SSB, and snacks and sweets.
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ward, B.W.; Schiller, J.S.; Goodman, R.A. Multiple Chronic Conditions Among US Adults: A 2012 Update. Prev. Chronic Dis. 2014, 11, 130389. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture Dietary Guidelines for Americans. 2015. Available online: Health.gov (accessed on 2 June 2017).
- Guenther, P.M.; Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef]
- Rowe, S.; Alexander, N.; Almeida, N.G.; Black, R.; Burns, R.; Bush, L.; Crawford, P.; Keim, N.; Kris-Etherton, P.; Weaver, C. Translating the Dietary Guidelines for Americans 2010 to Bring about Real Behavior Change. J. Am. Diet. Assoc. 2011, 111, 28–39. [Google Scholar] [CrossRef]
- Ivens, B.J.; Smith Edge, M. Food and Nutrition Science Solutions Joint Task Force Translating the Dietary Guidelines to Promote Behavior Change: Perspectives from the Food and Nutrition Science Solutions Joint Task Force. J. Acad. Nutr. Diet. 2016, 116, 1697–1702. [Google Scholar] [CrossRef]
- Lewis, K.D.; Burton-Freeman, B.M. The role of innovation and technology in meeting individual nutritional needs. J. Nutr. 2010, 140, 426S–436S. [Google Scholar] [CrossRef] [PubMed]
- Escaron, A.L.; Meinen, A.M.; Nitzke, S.A.; Martinez-Donate, A.P. Supermarket and Grocery Store–Based Interventions to Promote Healthful Food Choices and Eating Practices: A Systematic Review. Prev. Chronic Dis. 2013, 10, 120156. [Google Scholar] [CrossRef] [PubMed]
- Kalnikaitė, V.; Bird, J.; Rogers, Y. Decision-making in the aisles: Informing, overwhelming or nudging supermarket shoppers? Pers. Ubiquitous Comput. 2013, 17, 1247–1259. [Google Scholar] [CrossRef]
- Hollywood, L.E.; Cuskelly, G.J.; O’Brien, M.; McConnon, A.; Barnett, J.; Raats, M.M.; Dean, M. Healthful grocery shopping. Perceptions and barriers. Appetite 2013, 70, 119–126. [Google Scholar] [CrossRef]
- Kelley, P.G.; Consolvo, S.; Cranor, L.F.; Jung, J.; Sadeh, N.; Wetherall, D. A Conundrum of Permissions: Installing Applications on an Android Smartphone. In Financial Cryptography and Data Security, FC2012; Blyth, J., Dietrich, S., Camp, L.J., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2012; Volume 7398, pp. 68–79. [Google Scholar]
- Gilliland, J.; Sadler, R.; Clark, A.; O’Connor, C.; Milczarek, M.; Doherty, S.; Gilliland, J.; Sadler, R.; Clark, A.; O’Connor, C.; et al. Using a Smartphone Application to Promote Healthy Dietary Behaviours and Local Food Consumption. BioMed Res. Int. 2015, 2015, 841368. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Lopez, D.; Torres, M.; Velez, J.; Grullon, J.; Negron, E.; Perez, C.; Palacios, C. Development and Evaluation of a Nutritional Smartphone Application for Making Smart and Healthy Choices in Grocery Shopping. Healthc. Inform. Res. 2017, 23, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Academy of Nutrition and Dietetics Adult Weight Management (AWM) Guideline. Available online: http://www.andeal.org/topic.cfm?cat=2798 (accessed on 20 February 2017).
- US Department of Agriculture (USDA) Choose MyPlate. Available online: https://www.choosemyplate.gov/MyPlate (accessed on 21 February 2017).
- French, S.A.; Wall, M.; Mitchell, N.R.; Shimotsu, S.T.; Welsh, E. Annotated receipts capture household food purchases from a broad range of sources. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, C.; Trak, M.A.; Betancourt, J.; Joshipura, K.; Tucker, K.L. Validation and reproducibility of a semi-quantitative FFQ as a measure of dietary intake in adults from Puerto Rico. Public Health Nutr. 2015, 18, 2550–2558. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Sielaff, B.H.; Chong, K.; Buzzard, I.M. Computerized collection and analysis of dietary intake information. Comput. Methods Programs Biomed. 1989, 30, 47–57. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988; Volume 2. [Google Scholar]
- Levine, T.R.; Hullett, C.R. Eta Squared, Partial Eta Squared, and Misreporting of Effect Size in Communication Research. Hum. Commun. Res. 2002, 28, 612–625. [Google Scholar] [CrossRef]
- Petrogianni, M.; Kanellakis, S.; Kallianioti, K.; Argyropoulou, D.; Pitsavos, C.; Manios, Y. A multicomponent lifestyle intervention produces favourable changes in diet quality and cardiometabolic risk indices in hypercholesterolaemic adults. J. Hum. Nutr. Diet. 2013, 26, 596–605. [Google Scholar] [CrossRef]
- Torres, R.; Santos, E.; Orraca, L.; Elias, A.; Palacios, C. Diet quality, social determinants, and weight status in Puerto Rican children aged 12 years. J. Acad. Nutr. Diet. 2014, 114, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.; Torres, R.; Perez, C.M.; Palacios, C. Social environment factors, diet quality, and body weight in 12-year-old children from four public schools in Puerto Rico. P. R. Health Sci. J. 2014, 33, 80–87. [Google Scholar]
- Torres, R.; Serrano, M.; Perez, C.M.; Palacios, C. Physical environment, diet quality, and body weight in a group of 12-year-old children from four public schools in Puerto Rico. P. R. Health Sci. J. 2014, 33, 14–21. [Google Scholar]
- Guilloty, N.I.; Soto, R.; Anzalota, L.; Rosario, Z.; Cordero, J.F.; Palacios, C. Diet, Pre-pregnancy BMI, and Gestational Weight Gain in Puerto Rican Women. Matern. Child Health J. 2015, 19, 2453–2461. [Google Scholar] [CrossRef] [Green Version]
- Neville, C.E.; McKinley, M.C.; Draffin, C.R.; Gallagher, N.E.; Appleton, K.M.; Young, I.S.; Edgar, J.D.; Woodside, J.V. Participating in a fruit and vegetable intervention trial improves longer term fruit and vegetable consumption and barriers to fruit and vegetable consumption: A follow-up of the ADIT study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 158. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Atkin, A.J.; Biddle, S.J.H.; Gorely, T. A family-based intervention to increase fruit and vegetable consumption in adolescents: A pilot study. Public Health Nutr. 2010, 13, 876–885. [Google Scholar] [CrossRef]
- Erinosho, T.O.; Pinard, C.A.; Nebeling, L.C.; Moser, R.P.; Shaikh, A.R.; Resnicow, K.; Oh, A.Y.; Yaroch, A.L. Development and implementation of the National Cancer Institute’s Food Attitudes and Behaviors Survey to assess correlates of fruit and vegetable intake in adults. PLoS ONE 2015, 10, e0115017. [Google Scholar] [CrossRef]
- McLaughlin, C.; Tarasuk, V.; Kreiger, N. An examination of at-home food preparation activity among low-income, food-insecure women. J. Am. Diet. Assoc. 2003, 103, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Mummah, S.; Robinson, T.N.; Mathur, M.; Farzinkhou, S.; Sutton, S.; Gardner, C.D. Effect of a mobile app intervention on vegetable consumption in overweight adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- Eyles, H.; McLean, R.; Neal, B.; Jiang, Y.; Doughty, R.N.; McLean, R.; Ni Mhurchu, C. A salt-reduction smartphone app supports lower-salt food purchases for people with cardiovascular disease: Findings from the SaltSwitch randomised controlled trial. Eur. J. Prev. Cardiol. 2017, 24, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Laing, B.Y.; Mangione, C.M.; Tseng, C.-H.; Leng, M.; Vaisberg, E.; Mahida, M.; Bholat, M.; Glazier, E.; Morisky, D.E.; Bell, D.S. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: A randomized, controlled trial. Ann. Intern. Med. 2014, 161, S5–S12. [Google Scholar] [CrossRef]
- Scholtz, C. A Novel ‘Food Lists’ App to Promote Weight Loss, Improve Diet Quality, and Strengthen Diet Adherence: The Foodmindr Study; Arizona State University: Tempe, AZ, USA, 2016. [Google Scholar]
- Wharton, C.M.; Johnston, C.S.; Cunningham, B.K.; Sterner, D. Dietary Self-Monitoring, But Not Dietary Quality, Improves With Use of Smartphone App Technology in an 8-Week Weight Loss Trial. J. Nutr. Educ. Behav. 2014, 46, 440–444. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Traditional group (n = 24) | App group (n = 27) | p Value * |
|---|---|---|---|
| Mean (SD) or % | |||
| Age, years | 36.8 (5.86) | 33.8 (7.30) | 0.12 |
| Female sex, % | 91.7 | 88.9 | 0.56 |
| More than high school education, % | 83.3 | 81.5 | 0.58 |
| Number of family members in household | 3.17 (1.24) | 3.11 (1.34) | 0.88 |
| Weight (kg) | 83.3 (14.9) | 93.3 (20.4) | 0.09 |
| Height (m) | 1.58 (0.06) | 1.62 (0.08) | 0.12 |
| BMI, kg/m2 | 33.3 (5.81) | 35.6 (7.50) | 0.29 |
| Overweight, % | 31.6 | 30.0 | 0.92 |
| Obese, % | 68.4 | 70.0 | |
| Variable | Baseline | Post-Intervention | Difference between Groups at Baseline | Difference between Baseline and Post-Intervention | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Traditional Group (n = 18) | App Group (n = 13) | Traditional Group (n = 18) | App Group (n = 13) | Traditional Group | App Group | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p Value * | p Value * | ||
| Fruits | 1.03 | 1.02 | 1.27 | 1.05 | 1.78 | 1.63 | 2.34 | 2.31 | 0.53 | 0.05 | 0.08 |
| Vegetables | 1.75 | 1.76 | 1.31 | 1.03 | 3.42 | 4.07 | 3.71 | 3.68 | 0.43 | 0.07 | 0.02 |
| Whole grains | 0.31 | 0.55 | 0.23 | 0.39 | 0.61 | 0.49 | 0.98 | 1.37 | 0.68 | 0.06 | 0.04 |
| 100% fruit juices | 0.14 | 0.33 | 0.08 | 0.19 | 0.13 | 0.28 | 0.49 | 0.94 | 0.55 | 0.45 | 0.07 |
| SSB †† | 1.14 | 1.19 | 0.65 | 0.85 | 1.10 | 1.25 | 2.13 | 3.46 | 0.22 | 0.46 | 0.10 |
| Variable | Baseline | Post-Intervention | Difference between Groups at Baseline | Difference between Baseline and Post-Intervention | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Traditional Group (n = 18) | App Group (n = 13) | Traditional Group (n = 18) | App Group (n = 13) | Traditional Group | App Group | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p Value * | |||
| Fruits | 0.87 | 0.96 | 1.13 | 1.16 | 1.09 | 0.99 | 1.37 | 1.06 | 0.49 | 0.19 | 0.18 |
| Vegetables | 0.65 | 0.69 | 0.76 | 0.69 | 0.69 | 0.69 | 1.45 | 1.55 | 0.66 | 0.43 | 0.06 |
| Starchy vegetables | 1.18 | 0.94 | 1.10 | 0.65 | 1.10 | 0.93 | 1.60 | 1.28 | 0.78 | 0.39 | 0.10 |
| Refined grains | 3.59 | 2.06 | 3.36 | 1.38 | 2.64 | 1.65 | 2.18 | 1.51 | 0.71 | 0.02 | 0.01 |
| Whole grains | 1.12 | 0.73 | 1.32 | 1.03 | 1.41 | 0.79 | 1.78 | 1.17 | 0.52 | 0.06 | 0.09 |
| Legumes | 0.13 | 0.16 | 0.23 | 0.24 | 0.18 | 0.18 | 0.07 | 0.12 | 0.14 | 0.16 | 0.02 |
| Healthy proteins | 1.26 | 1.20 | 0.82 | 0.84 | 0.77 | 1.04 | 0.42 | 0.59 | 0.24 | 0.05 | 0.10 |
| Red meats | 3.90 | 1.94 | 4.25 | 1.98 | 3.49 | 1.92 | 4.22 | 1.76 | 0.62 | 0.23 | 0.48 |
| Cold cuts & cured meats | 0.40 | 0.47 | 0.38 | 0.51 | 0.50 | 0.47 | 0.40 | 0.44 | 0.91 | 0.22 | 0.46 |
| Whole-fat dairies | 1.01 | 0.58 | 0.42 | 0.31 | 0.63 | 0.35 | 0.38 | 0.28 | 0.00 | 0.00 | 0.34 |
| Low-fat dairies | 0.36 | 0.25 | 0.75 | 0.75 | 0.43 | 0.60 | 0.75 | 0.87 | 0.06 | 0.33 | 0.49 |
| 100% fruit juices | 0.23 | 0.41 | 0.35 | 0.47 | 0.09 | 0.16 | 0.11 | 0.28 | 0.47 | 0.11 | 0.01 |
| SSB †† | 0.45 | 1.29 | 0.07 | 0.15 | 0.24 | 0.46 | 0.08 | 0.19 | 0.27 | 0.28 | 0.41 |
| Sweets and snacks | 1.32 | 1.57 | 1.36 | 1.05 | 0.98 | 1.16 | 0.58 | 0.74 | 0.94 | 0.21 | 0.03 |
| Variable | Adjusted Mean Difference | 95% CI | p Value * | Partial Eta-Squared |
|---|---|---|---|---|
| Fruits | 0.13 | −0.50, 0.77 | 0.67 | 0.006 |
| Vegetables | 0.74 | −0.12, 1.60 | 0.09 | 0.10 |
| Starchy vegetables | 0.52 | −0.29, 1.32 | 0.20 | 0.06 |
| Refined grains | −0.35 | −1.34, 0.64 | 0.47 | 0.02 |
| Whole grains | 0.27 | −0.38, 0.93 | 0.40 | 0.02 |
| Legumes | −0.11 | −0.23, 0.004 | 0.06 | 0.12 |
| Healthy proteins | −0.25 | −0.88, 0.37 | 0.41 | 0.02 |
| Red meats | 0.68 | −0.67, 2.04 | 0.31 | 0.04 |
| Cold cuts and cured meats | −0.10 | −0.42, 0.23 | 0.55 | 0.01 |
| Regular dairies | −0.09 | −0.34, 0.17 | 0.49 | 0.02 |
| Low-fat dairies | 0.35 | −0.23, 0.93 | 0.22 | 0.05 |
| 100% fruit juices | −0.005 | −0.16, 0.15 | 0.94 | 0.0002 |
| SSB † | −0.17 | −0.44, 0.10 | 0.21 | 0.05 |
| Snacks and sweets | −0.40 | −1.13, 0.32 | 0.26 | 0.04 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palacios, C.; Torres, M.; López, D.; Trak-Fellermeier, M.A.; Coccia, C.; Pérez, C.M. Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial. Nutrients 2018, 10, 1967. https://doi.org/10.3390/nu10121967
Palacios C, Torres M, López D, Trak-Fellermeier MA, Coccia C, Pérez CM. Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial. Nutrients. 2018; 10(12):1967. https://doi.org/10.3390/nu10121967
Chicago/Turabian StylePalacios, Cristina, Michelle Torres, Desiree López, Maria A. Trak-Fellermeier, Catherine Coccia, and Cynthia M. Pérez. 2018. "Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial" Nutrients 10, no. 12: 1967. https://doi.org/10.3390/nu10121967
APA StylePalacios, C., Torres, M., López, D., Trak-Fellermeier, M. A., Coccia, C., & Pérez, C. M. (2018). Effectiveness of the Nutritional App “MyNutriCart” on Food Choices Related to Purchase and Dietary Behavior: A Pilot Randomized Controlled Trial. Nutrients, 10(12), 1967. https://doi.org/10.3390/nu10121967