Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness

 ,
,  , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
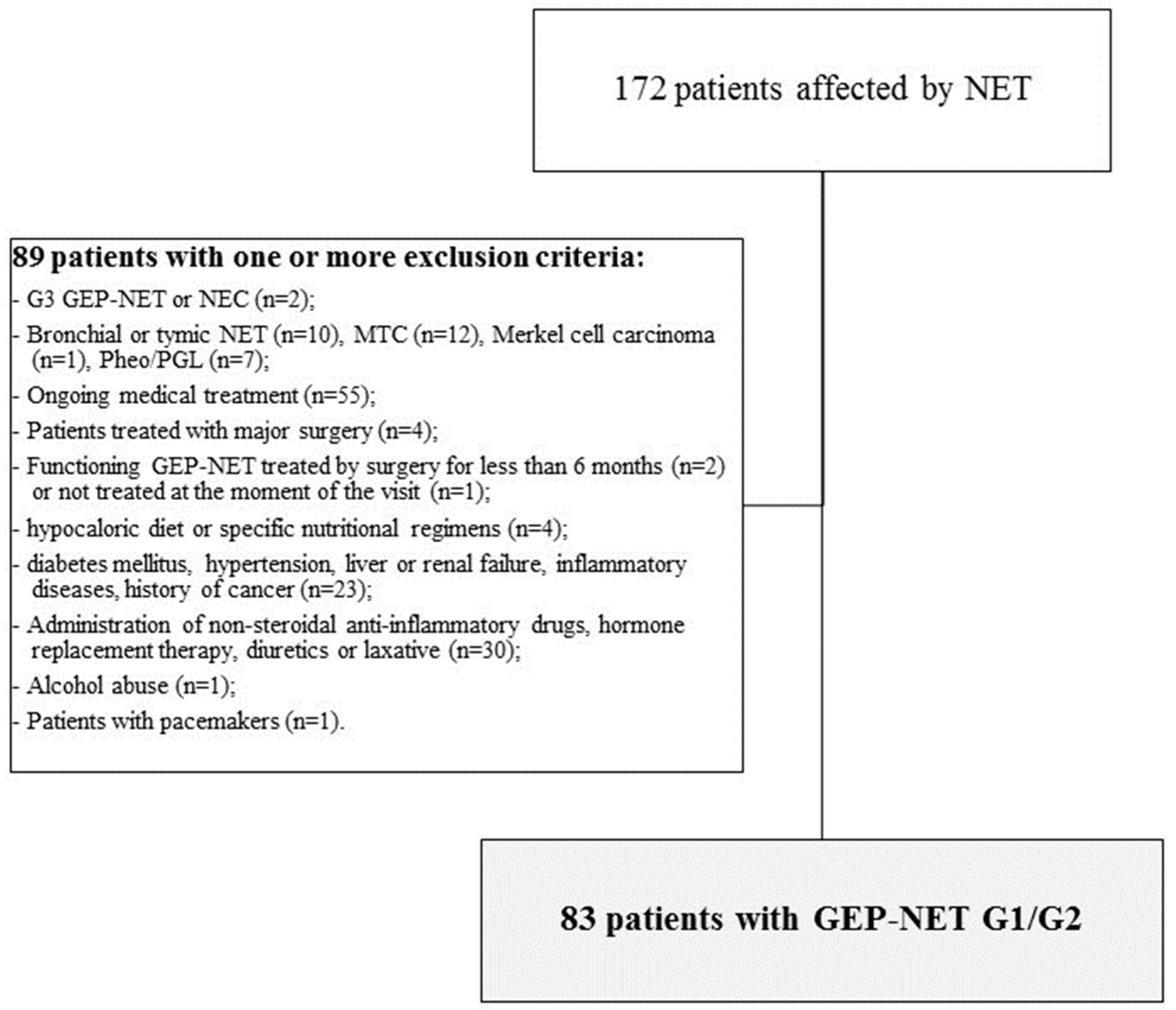
2.2. Population Study
- Histological diagnosis of well-differentiated, low grade (G)1 and G2 GEP-NET, including sporadic tumors or patients with multiple endocrine neoplasia type 1 (MEN1) syndrome, according to classification of by the World Health Organization (WHO) [18];
- Non-functioning GEP-NET patients that were treatment-naïve (evaluated at the moment of the diagnosis or before starting any medical treatment), or that discontinued Somatostatin Analogues (SSAs) for more than 6 months or after endoscopic surgery performed more than 6 months before the visit;
- Functioning GEP-NET patients who underwent endoscopic tumor resection and who were biochemically free of disease for more than 6 months and who had not resumed medical treatment;
- Diagnosis of bronchial or thymic NET, medullary thyroid cancer, Merkel cell carcinoma, pheochromocytoma/paraganglioma;
- Ongoing medical treatment, including SSAs or targeted therapy, at the moment of the visit, since they could affect the gastrointestinal secretory, motor, and absorptive functions or cause anorexia and liver toxicity [5];
- Patients who had undergone major surgery, since it could change the anatomy of the gastrointestinal tract;
- Patients with functioning GEP-NET that had been treated with curative surgery for less than 6 months before the visit;
- Patients with functioning GEP-NET that had not been treated at the moment of the visit, since the secretion of hormones, peptides and amines could cause malabsorption, diarrhea, steatorrhea and altered motility of the gastrointestinal tract [5];
- Patients on a hypocaloric diet in the last three months or specific nutritional regimens, including vegan or vegetarian diets and vitamin/mineral or antioxidant supplementation;
- Presence of clinical conditions that could influence fluid balance and metabolism, including diabetes mellitus, hypertension, liver or renal failure, acute or chronic inflammatory diseases, history of cancer, based on a complete medical examination and laboratory investigations;
- Current administration of medicaments that could influence the fluid balance, including non-steroidal anti-inflammatory drugs, hormone replacement therapy, diuretics or laxative;
- Abuse of alcohol defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM)-V criteria [19];
2.3. Clinicopathological Characteristics of the Tumor
2.4. Lifestyle Habits
2.5. Dietary Assessment
2.6. Adherence to the Mediterranean Diet
2.7. Anthropometric Measurements and Blood Pressure
2.8. Assay Methods
2.9. Bioelectrical Impedance Analysis
2.10. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Nutritional Status in GEP-NET Patients and Control Group
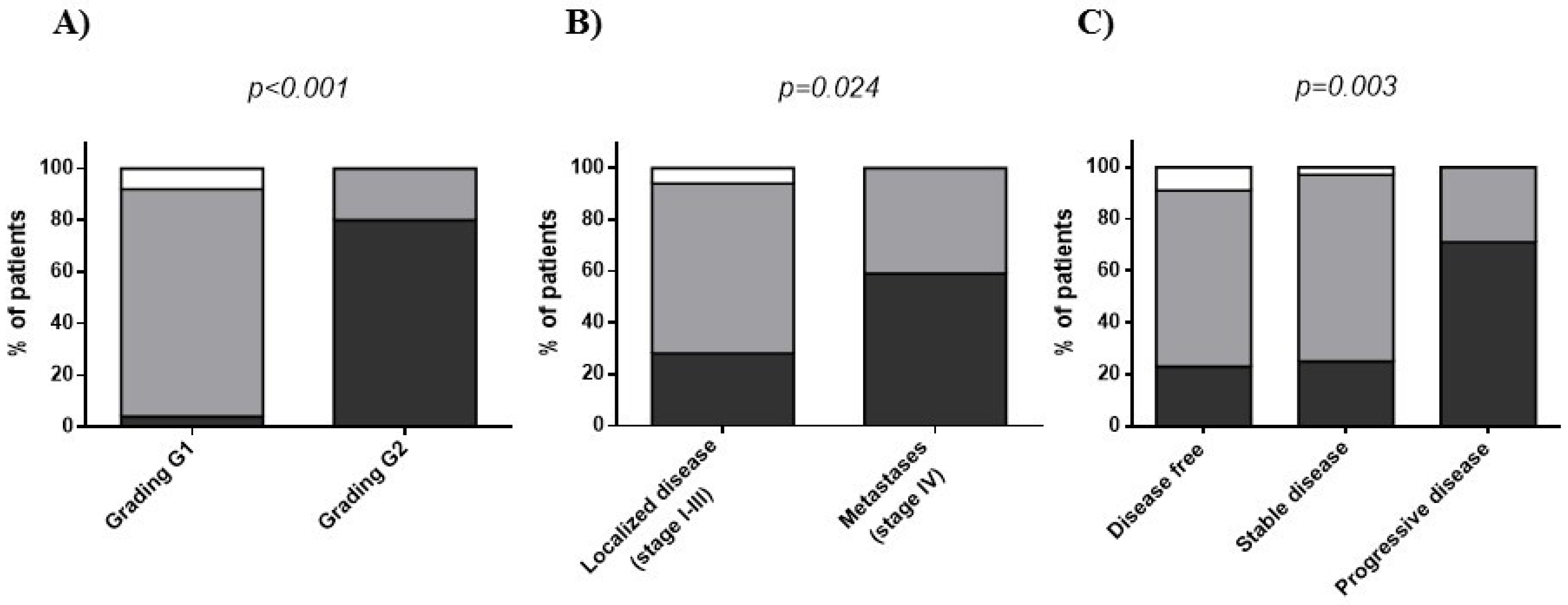
3.3. Nutritional Status in GEP-NET Patients According to Tumor Grading, Stage and Disease Status
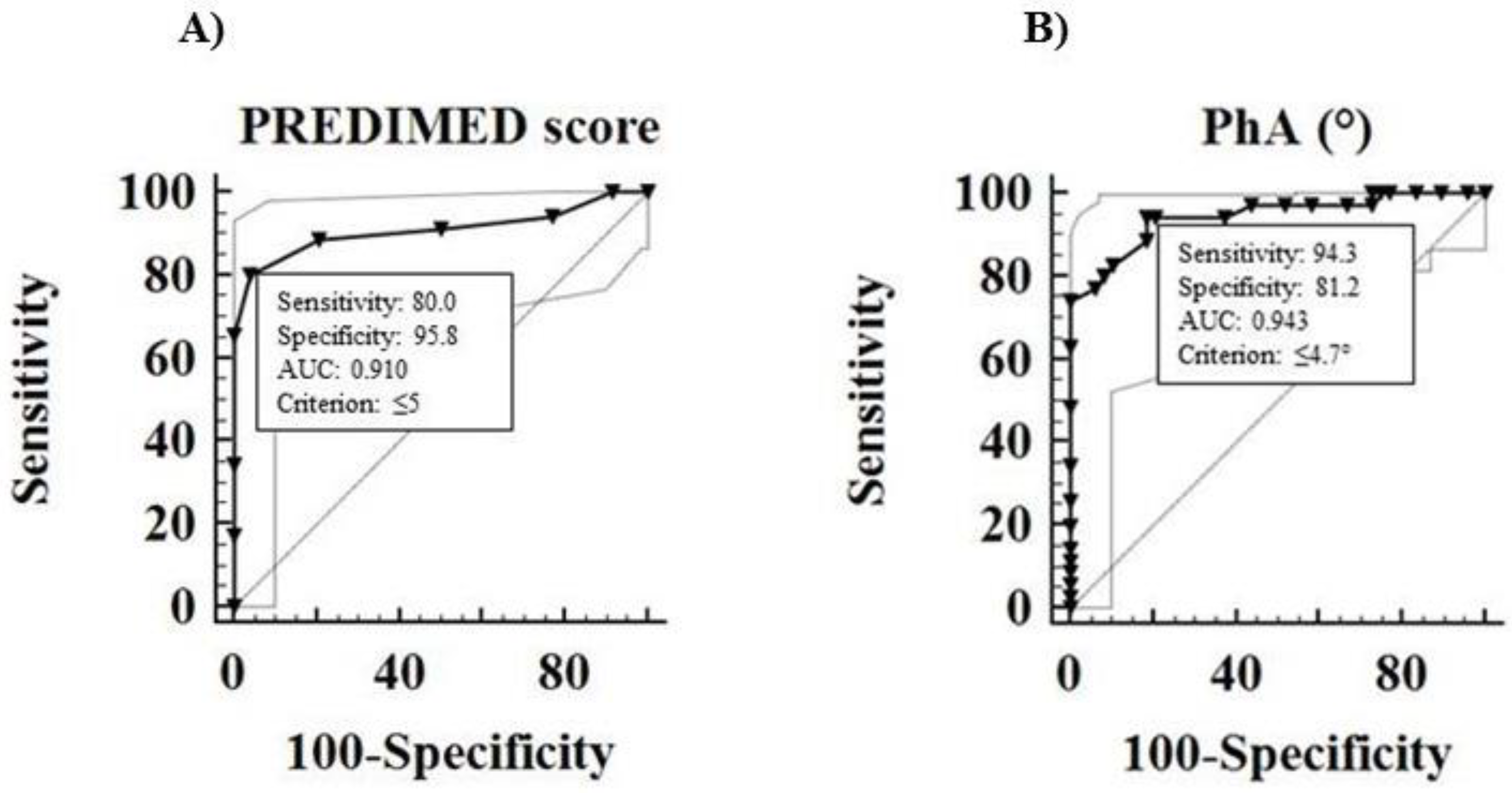
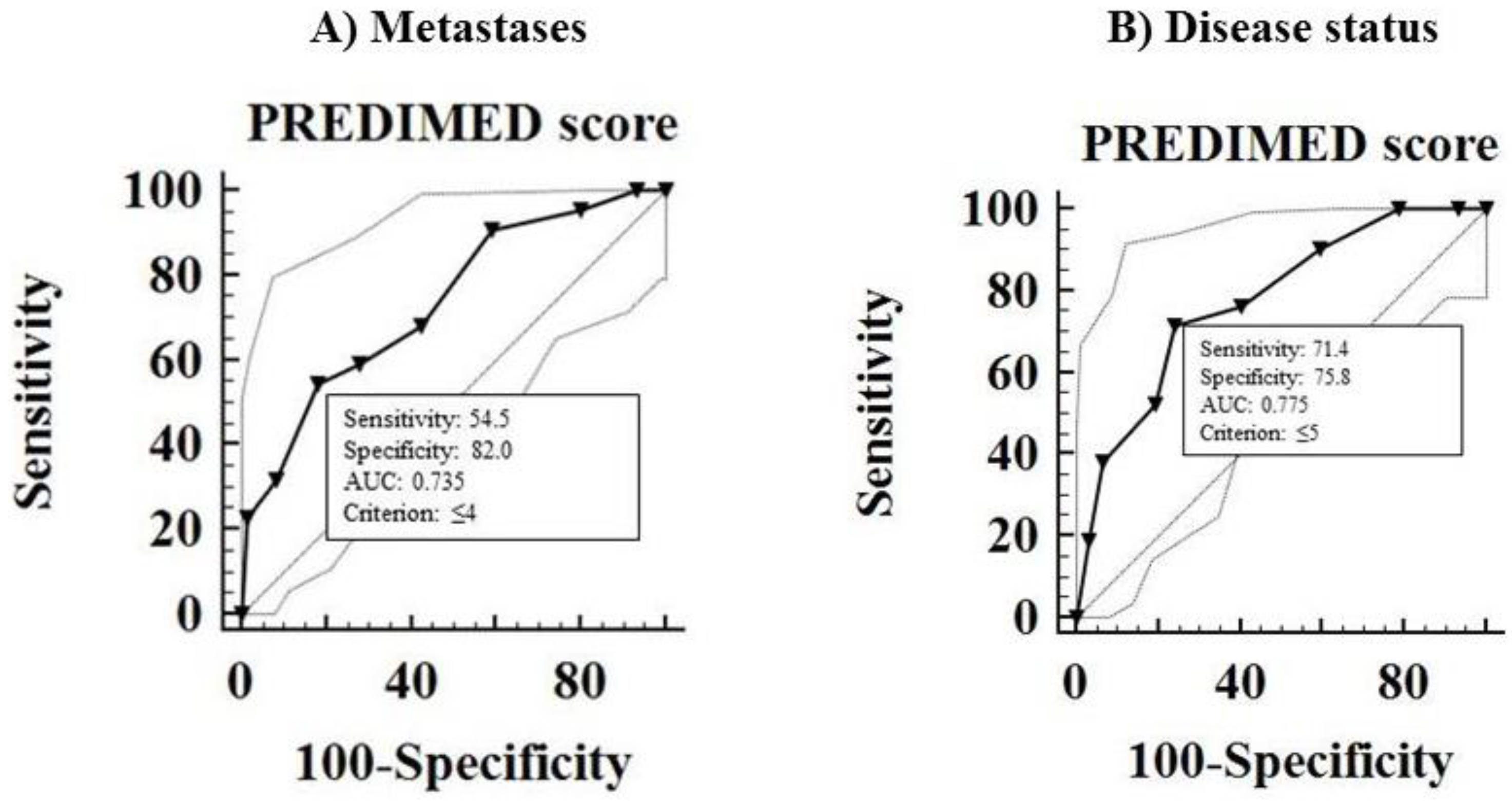
3.4. Correlation between Tumor Aggressiveness and Nutritional Status in GEP-NET Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, A.; Ferolla, P.; Grimaldi, F.; Campana, D.; Manzoni, M.; Davi, M.V.; Bianchi, A.; Valcavi, R.; Papini, E.; Giuffrida, D.; et al. Natural history of gastro-entero-pancreatic and thoracic neuroendocrine tumors. Data from a large prospective and retrospective Italian epidemiological study: The NET management study. J. Endocrinol. Invest. 2012, 35, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Kloppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Go, V.L.; Srihari, P.; Kamerman Burns, L.A. Nutrition and gastroenteropancreatic neuroendocrine tumors. Endocrinol. Metab. Clin. N. Am. 2010, 39, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Gallo, M.; Muscogiuri, G.; Pizza, G.; Ruggeri, R.M.; Barrea, L.; Faggiano, A.; Colao, A.; Group, N. The management of neuroendocrine tumours: A nutritional viewpoint. Crit. Rev. Food Sci. Nutr. 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Glazer, E.; Stanko, K.; Ong, E.; Guerrero, M. Decreased Inpatient Mortality in Obese Patients with Abdominal Nets. Endocr. Pract. 2014, 20, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Ekeblad, S.; Skogseid, B.; Dunder, K.; Oberg, K.; Eriksson, B. Prognostic factors and survival in 324 patients with pancreatic endocrine tumor treated at a single institution. Clin. Cancer Res. 2008, 14, 7798–7803. [Google Scholar] [CrossRef] [PubMed]
- Maasberg, S.; Knappe-Drzikova, B.; Vonderbeck, D.; Jann, H.; Weylandt, K.H.; Grieser, C.; Pascher, A.; Schefold, J.C.; Pavel, M.; Wiedenmann, B.; et al. Malnutrition Predicts Clinical Outcome in Patients with Neuroendocrine Neoplasia. Neuroendocrinology 2017, 104, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrache, F.; Vullierme, M.P.; Roy, C.; El Assoued, Y.; Couvelard, A.; O’Toole, D.; Mitry, E.; Hentic, O.; Hammel, P.; Levy, P.; et al. Arterial phase enhancement and body mass index are predictors of response to chemoembolisation for liver metastases of endocrine tumours. Br. J. Cancer 2007, 96, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.; Barros, A.J.; Wang, J.; Heymsfield, S.B.; Pierson, R.N., Jr. Bioelectrical impedance analysis: Population reference values for phase angle by age and sex. Am. J. Clin. Nutr. 2005, 82, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobaus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis-clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Geler, M.; Urquiza-Salvat, N.; Cozar, J.M.; Robles-Fernandez, I.; Rivas, A.; Martinez-Gonzalez, L.J.; Ocana-Peinado, F.M.; Lorente, J.A.; Alvarez-Cubero, M.J. The influence of nutritional factors on prostate cancer incidence and aggressiveness. Aging Male 2018, 21, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Ros, M.M.; Roswall, N.; Bueno-de-Mesquita, H.B.; Travier, N.; Tjonneland, A.; Kiemeney, L.A.; Sacerdote, C.; Tumino, R.; Ljungberg, B.; et al. Adherence to the Mediterranean diet and risk of bladder cancer in the EPIC cohort study. Int. J. Cancer 2014, 134, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Escrich, E.; Moral, R.; Solanas, M. Olive oil, an essential component of the Mediterranean diet, and breast cancer. Public Health Nutr. 2011, 14, 2323–2332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Macchia, P.E.; Di Somma, C.; Falco, A.; Savanelli, M.C.; Colao, A.; Savastano, S. Mediterranean Diet and Phase Angle in a Sample of Adult Population: Results of a Pilot Study. Nutrients 2017, 9, 151. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Arnold, R.; Capella, C.; Klimstra, D.S.; Klöppel, G.; Komminoth, P.; Solcia, E. Nomenclature and classification of digestive neuroendocrine tumours. In World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Digestive System; Bosman, F., Lyon, F.C.I., Eds.; IARC: Lyons, France, 2010. [Google Scholar]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Rindi, G.; Kloppel, G.; Alhman, H.; Caplin, M.; Couvelard, A.; de Herder, W.W.; Erikssson, B.; Falchetti, A.; Falconi, M.; Komminoth, P.; et al. TNM staging of foregut (neuro)endocrine tumors: A consensus proposal including a grading system. Virchows Arch. 2006, 449, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Inzani, F.; Petrone, G.; Fadda, G.; Rindi, G. Cyto-histology in NET: What is necessary today and what is the future? Rev. Endocr. Metab. Disord. 2017, 18, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Circelli, L.; Sciammarella, C.; Guadagno, E.; Tafuto, S.; del Basso de Caro, M.; Botti, G.; Pezzullo, L.; Aria, M.; Ramundo, V.; Tatangelo, F.; et al. CXCR4/CXCL12/CXCR7 axis is functional in neuroendocrine tumors and signals on mTOR. Oncotarget 2016, 7, 18865–18875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Di Somma, C.; Macchia, P.E.; Falco, A.; Savanelli, M.C.; Orio, F.; Colao, A.; Savastano, S. Influence of nutrition on somatotropic axis: Milk consumption in adult individuals with moderate-severe obesity. Clin. Nutr. 2017, 36, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Tarantino, G.; Somma, C.D.; Muscogiuri, G.; Macchia, P.E.; Falco, A.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet and Circulating Levels of Sirtuin 4 in Obese Patients: A Novel Association. Oxid. Med. Cell. Longev. 2017, 2017, 6101254. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Macchia, P.E.; Tarantino, G.; Di Somma, C.; Pane, E.; Balato, N.; Napolitano, M.; Colao, A.; Savastano, S. Nutrition: A key environmental dietary factor in clinical severity and cardio-metabolic risk in psoriatic male patients evaluated by 7-day food-frequency questionnaire. J. Transl. Med. 2015, 13, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Annunziata, G.; Megna, M.; Falco, A.; Balato, A.; Colao, A.; Savastano, S. Coffee consumption, metabolic syndrome and clinical severity of psoriasis: Good or bad stuff? Arch. Toxicol. 2018, 92, 1831–1845. [Google Scholar] [CrossRef] [PubMed]
- Turconi, G.; Guarcello, M.; Berzolari, F.G.; Carolei, A.; Bazzano, R.; Roggi, C. An evaluation of a colour food photography atlas as a tool for quantifying food portion size in epidemiological dietary surveys. Eur. J. Clin. Nutr. 2005, 59, 923–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Balato, N.; Di Somma, C.; Macchia, P.E.; Napolitano, M.; Savanelli, M.C.; Esposito, K.; Colao, A.; Savastano, S. Nutrition and psoriasis: Is there any association between the severity of the disease and adherence to the Mediterranean diet? J. Transl. Med. 2015, 13, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Tramontano, G.; De Luca, V.; Illario, M.; Colao, A.; Savastano, S. Association between Mediterranean diet and hand grip strength in older adult women. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Savanelli, M.C.; Barrea, L.; Macchia, P.E.; Savastano, S.; Falco, A.; Renzullo, A.; Scarano, E.; Nettore, I.C.; Colao, A.; Di Somma, C. Preliminary results demonstrating the impact of Mediterranean diet on bone health. J. Transl. Med. 2017, 15, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuolo, L.; Barrea, L.; Savanelli, M.C.; Savastano, S.; Rubino, M.; Scarano, E.; Soprano, M.; Illario, M.; Colao, A.; Di Somma, C. Nutrition and Osteoporosis: Preliminary data of Campania Region of European PERsonalised ICT Supported Service for Independent Living and Active Ageing. Transl. Med. UniSa. 2015, 13, 13–18. [Google Scholar] [PubMed]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Aros, F.; Gomez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Waist Circumference and Waist–Hip Ratio. Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Nishida, C.; Ko, G.T.; Kumanyika, S. Body fat distribution and noncommunicable diseases in populations: Overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur. J. Clin. Nutr. 2010, 64, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Yanovski, J.A.; Yanovski, S.Z.; Filmer, K.M.; Hubbard, V.S.; Avila, N.; Lewis, B.; Reynolds, J.C.; Flood, M. Differences in body composition of black and white girls. Am. J. Clin. Nutr. 1996, 64, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Macchia, P.E.; Di Somma, C.; Napolitano, M.; Balato, A.; Falco, A.; Savanelli, M.C.; Balato, N.; Colao, A.; Savastano, S. Bioelectrical phase angle and psoriasis: A novel association with psoriasis severity, quality of life and metabolic syndrome. J. Transl. Med. 2016, 14, 130–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gomez, J.; Lilienthal Heitmann, B.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F. Bioelectrical impedance analysis: A review of principles and applications. J. Am. Coll. Nutr. 1992, 11, 199–209. [Google Scholar] [PubMed]
- Altieri, B.; Barrea, L.; Modica, R.; Muscogiuri, G.; Savastano, S.; Colao, A.; Faggiano, A. Nutrition and neuroendocrine tumors: An update of the literature. Rev. Endocr. Metab. Disord. 2018, 19, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Milner, J.A. Molecular targets for bioactive food components. J. Nutr. 2004, 134, S2492–S2498. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lis, C.G.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Lammersfeld, C.A. Bioelectrical impedance phase angle as a prognostic indicator in advanced pancreatic cancer. Br. J. Nutr. 2004, 92, 957–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, D.; Lammersfeld, C.A.; Vashi, P.G.; King, J.; Dahlk, S.L.; Grutsch, J.F.; Lis, C.G. Bioelectrical impedance phase angle as a prognostic indicator in breast cancer. BMC Cancer 2008, 8, 249. [Google Scholar] [CrossRef] [PubMed]
- Toso, S.; Piccoli, A.; Gusella, M.; Menon, D.; Bononi, A.; Crepaldi, G.; Ferrazzi, E. Altered tissue electric properties in lung cancer patients as detected by bioelectric impedance vector analysis. Nutrition 2000, 16, 120–124. [Google Scholar] [CrossRef]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical impedance phase angle in clinical practice: Implications for prognosis in advanced colorectal cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hoidrup, S.; Andreasen, A.H.; Osler, M.; Pedersen, A.N.; Jorgensen, L.M.; Jorgensen, T.; Schroll, M.; Heitmann, B.L. Assessment of habitual energy and macronutrient intake in adults: Comparison of a seven day food record with a dietary history interview. Eur. J. Clin. Nutr. 2002, 56, 105–113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | GEP-NET Patients n. 83 | Control Group n. 83 | p-Value |
|---|---|---|---|
| Clinical characteristics Gender-male Age-mean (range) | 40 (48.2%) 56 (18–80) | 40 (48.2%) 57 (23–82) | 0.877 (χ2 = 0.02) 0.307 |
| Lifestyle Habits Smoking-yes Physical activity-yes | 32 (38.6%) 41 (49.4%) | 51 (61.4%) 45 (54.2%) | 0.005 (χ2 = 7.81) 0.986 (χ2 = 0.00) |
| Anthropometric measurement BMI (kg/m2) WC (cm) | 27.79 ± 5.57 92.76 ± 15.38 | 27.54 ± 2.84 87.92 ± 10.66 | 0.859 0.050 |
| Blood pressure SBP (mmHg) DBP (mmHg) | 123.79 ± 12.16 76.99 ± 7.99 | 118.49 ± 11.93 73.86 ± 6.87 | 0.010 0.007 |
| Metabolic profile | |||
| Fasting Glucose (mg/dL) | 109.52 ± 16.51 | 89.29 ± 11.72 | <0.001 |
| Total cholesterol (mg/dL) | 194.83 ± 41.19 | 149.08 ± 22.41 | <0.001 |
| HDL cholesterol (mg/dL) | 44.43 ± 14.35 | 50.45 ± 8.67 | <0.001 |
| LDL cholesterol (mg/dL) | 123.35 ± 40.85 | 77.20 ± 25.00 | <0.001 |
| Triglycerides (mg/dL) | 135.23 ± 47.81 | 107.22 ± 26.57 | <0.001 |
| Bioelectrical variables | |||
| R (Ω) | 514.23 ± 80.21 | 523.54 ± 59.99 | 0.279 |
| Xc (Ω) | 42.31 ± 9.50 | 52.19 ± 8.13 | <0.001 |
| PhA (°) | 4.73 ± 0.88 | 5.70 ± 0.55 | <0.001 |
| PhA (°) males | 4.69 ± 0.86 | 5.76 ± 0.60 | <0.001 |
| PhA (°) females | 4.76 ± 0.91 | 5.65 ± 0.52 | <0.001 |
| Questions of PREDIMED Questionnaire | GEP-NET Patients n. 83 | Control Group n. 83 | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | χ2 | p-Values | |
| Use of extra virgin olive oil as main culinary lipid | 78 | 94.0 | 79 | 95.2 | 0.00 | 1.000 |
| Extra virgin olive oil >4 tablespoons | 49 | 59.0 | 52 | 62.7 | 0.10 | 0.751 |
| Vegetables ≥2 servings/day | 30 | 36.1 | 49 | 59.0 | 7.83 | 0.005 |
| Fruits ≥3 servings/day | 27 | 32.5 | 50 | 60.2 | 11.72 | 0.001 |
| Red/processed meats <1/day | 25 | 30.1 | 41 | 49.4 | 5.66 | 0.017 |
| Butter, cream, margarine <1/day | 63 | 75.9 | 40 | 48.2 | 12.38 | 0.001 |
| Soda drinks <1/day | 34 | 41.0 | 54 | 65.1 | 8.73 | 0.003 |
| Wine glasses ≥7/week | 14 | 16.9 | 29 | 34.9 | 6.15 | 0.013 |
| Legumes ≥3/week | 38 | 45.8 | 37 | 44.6 | 0.00 | 1.000 |
| Fish/seafood ≥3/week | 18 | 21.7 | 36 | 43.4 | 7.93 | 0.005 |
| Commercial sweets and confectionery ≤2/week | 43 | 51.8 | 39 | 47.0 | 0.22 | 0.641 |
| Tree nuts ≥3/week | 20 | 24.1 | 33 | 39.8 | 21.14 | <0.001 |
| Poultry more than red meats | 41 | 49.4 | 43 | 51.8 | 0.02 | 0.876 |
| Use of sofrito sauce ≥2/week | 33 | 39.8 | 31 | 37.3 | 0.03 | 0.873 |
| PREDIMED categories | ||||||
| Low adherence to the MD | 30 | 36.1 | 28 | 33.7 | 0.03 | 0.870 |
| Average adherence to the MD | 49 | 59.0 | 33 | 39.8 | 5.42 | 0.019 |
| High adherence to the MD | 4 | 4.8 | 22 | 26.5 | 13.18 | 0.001 |
| Parameters | G1 n. 48 | G2 n. 35 | p-Value | Stage I-III (Localized Disease) n. 61 | Stage IV (Metastases) n. 22 | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | 54.85 ± 17.31 | 59.14 ± 12.64 | 0.103 | 55.72 ± 16.82 | 59.27 ± 11.37 | 0.123 |
| Anthropometric measurement | ||||||
| BMI (kg/m2) | 27.09 ± 5.89 | 28.74 ± 5.01 | 0.141 | 27.23 ± 5.77 | 29.31 ± 4.75 | 0.081 |
| WC (cm) | 90.29 ± 14.99 | 96.15 ± 15.46 | 0.092 | 90.72 ± 15.42 | 98.41 ± 14.05 | 0.032 |
| Blood pressure | ||||||
| SBP (mmHg) | 121.04 ± 11.39 | 127.57 ± 12.32 | 0.017 | 121.89 ± 12.08 | 129.09 ± 10.98 | 0.014 |
| DBP (mmHg) | 75.83 ± 7.88 | 78.57 ± 8.00 | 0.130 | 76.15 ± 7.27 | 79.32 ± 9.54 | 0.213 |
| Metabolic profile | ||||||
| Fasting Glucose (mg/dL) | 104.38 ± 15.61 | 116.57 ± 15.23 | 0.001 | 106.26 ± 16.32 | 118.54 ± 13.64 | 0.001 |
| Total cholesterol (mg/dL) | 177.54 ± 28.14 | 218.54 ± 44.67 | <0.001 | 186.74 ± 37.16 | 217.27 ± 44.26 | 0.009 |
| HDL cholesterol (mg/dL) | 46.97 ± 11.77 | 40.94 ± 16.83 | 0.007 | 47.00 ± 13.94 | 37.31 ± 13.27 | 0.002 |
| LDL cholesterol (mg/dL) | 106.02 ± 27.74 | 147.13 ± 44.21 | <0.001 | 114.99 ± 35.51 | 146.55 ± 46.31 | 0.013 |
| Triglycerides (mg/dL) | 122.73 ± 37.34 | 152.37 ± 55.33 | 0.050 | 123.75 ± 41.61 | 167.05 ± 50.36 | 0.003 |
| Bioelectrical variables | ||||||
| R (Ω) | 502.08 ± 75.14 | 530.89 ± 84.95 | 0.125 | 511.97 ± 79.39 | 520.50 ± 84.01 | 0.693 |
| Xc (Ω) | 45.89 ± 7.56 | 37.40 ± 9.78 | <0.001 | 43.70 ± 8.09 | 38.45 ± 12.02 | 0.008 |
| PhA (°) | 5.26 ± 0.62 | 4.00 ± 0.65 | <0.001 | 4.93 ± 0.80 | 4.16 ± 0.86 | <0.001 |
| Nutritional assessment | ||||||
| PREDIMED score | 7.56 ± 1.28 | 4.29 ± 1.87 | <0.001 | 6.69 ± 2.05 | 4.77 ± 2.22 | <0.001 |
| Total energy (kcal) | 2223.29 ± 235.67 | 2307.88 ± 235.47 | 0.107 | 2256.96 ± 231.39 | 2264.49 ± 260.66 | 0.943 |
| Protein (g of total kcal) | 94.59 ± 12.21 | 101.77 ± 16.08 | 0.026 | 96.21 ± 12.29 | 101.55 ± 18.66 | 0.191 |
| Animal (g of total kcal) | 70.31 ± 11.54 | 73.77 ± 10.25 | 0.129 | 71.68 ± 11.11 | 71.99 ± 11.26 | 0.903 |
| Plant (g of total kcal) | 24.29 ± 10.01 | 28.01 ± 14.32 | 0.236 | 24.52 ± 10.42 | 29.54 ± 15.51 | 0.178 |
| Carbohydrate (g of total kcal) | 300.19 ± 36.57 | 308.89 ± 34.06 | 0.246 | 304.80 ± 36.50 | 301.25 ± 33.58 | 0.706 |
| Complex (g of total kcal) | 188.41 ± 23.05 | 190.63 ± 22.83 | 0.633 | 190.53 ± 23.27 | 186.06 ± 21.80 | 0.431 |
| Simple (g of total kcal) | 111.78 ± 15.77 | 118.27 ± 14.01 | 0.040 | 114.27 ± 15.53 | 115.19 ± 15.02 | 0.785 |
| Fat (gr of total kcal) | 71.57 ± 7.60 | 73.91 ± 9.57 | 0.275 | 72.55 ± 7.66 | 72.59 ± 10.73 | 0.879 |
| SFA (g of total kcal) | 25.79 ± 5.16 | 26.80 ± 10.30 | 0.664 | 26.03 ± 6.55 | 26.72 ± 10.46 | 0.829 |
| MUFA (g of total kcal) | 30.94 ± 3.65 | 31.34 ± 3.50 | 0.587 | 31.12 ± 3.36 | 31.07 ± 4.19 | 0.877 |
| PUFA (g of total kcal) | 14.84 ± 3.94 | 15.77 ± 5.80 | 0.566 | 15.39 ± 5.34 | 14.79 ± 2.90 | 0.791 |
| n-6 PUFA (g/day) | 7.64 ± 3.58 | 8.83 ± 4.86 | 0.173 | 8.21 ± 4.65 | 7.96 ± 2.57 | 0.500 |
| n-3 PUFA (g/day) | 7.20 ± 1.59 | 6.94 ± 1.98 | 0.415 | 7.18 ± 1.67 | 6.83 ± 1.99 | 0.299 |
| Parameters | Disease Status | |||
|---|---|---|---|---|
| Free of the Disease n. 34 | Stable Disease n. 28 | Progressive Disease n. 21 | p-Value | |
| Age (years) | 55.61 ± 17.33 | 57.71 ± 15.23 | 56.95 ± 13.51 | 0.720 |
| Anthropometric measurement | ||||
| BMI (kg/m2) | 27.21 ± 4.94 | 27.54 ± 6.72 | 29.06 ± 4.83 | 0.411 |
| WC (cm) | 90.93 ± 16.20 | 92.36 ± 14.44 | 96.26 ± 15.36 | 0.458 |
| Blood pressure | ||||
| SBP (mmHg) | 123.08 ± 12.55 | 121.79 ± 11.07 | 127.62 ± 12.16 | 0.256 |
| DBP (mmHg) | 76.02 ± 7.66 | 77.14 ± 7.75 | 78.33 ± 8.99 | 0.631 |
| Metabolic profile | ||||
| Fasting Glucose (mg/dL) | 105.38 ± 12.99 | 106.82 ± 16.87 | 119.81 ± 17.42 | 0.005 |
| Total cholesterol (mg/dL) | 195.67 ± 41.66 | 178.64 ± 32.72 | 215.05 ± 42.99 | 0.017 |
| HDL cholesterol (mg/dL) | 42.15 ± 13.94 | 49.18 ± 12.43 | 41.81 ± 14.35 | 0.035 |
| LDL cholesterol (mg/dL) | 126.23 ± 38.67 | 105.35 ± 33.54 | 142.70 ± 44.65 | 0.012 |
| Triglycerides (mg/dL) | 136.50 ± 41.33 | 120.57 ± 38.41 | 152.71 ± 62.74 | 0.327 |
| Bioelectrical variables | ||||
| R (Ω) | 512.71 ± 83.84 | 507.61 ± 73.76 | 525.52 ± 85.06 | 0.767 |
| Xc (Ω) | 41.65 ± 9.88 | 45.79 ± 7.76 | 38.76 ± 9.84 | 0.025 |
| PhA (°) | 4.66 ± 0.82 | 5.19 ± 0.71 | 4.22 ± 0.91 | <0.001 |
| Nutritional assessment | ||||
| PREDIMED score | 6.91 ± 2.25 | 6.54 ± 1.79 | 4.52 ± 2.02 | <0.001 |
| Total energy (kcal) | 2256.94 ± 257.14 | 2254.24 ± 204.66 | 2268.51 ± 257.36 | 0.983 |
| Protein (g of total kcal) | 96.82 ± 13.50 | 97.39 ± 14.13 | 99.22 ± 16.36 | 0.855 |
| Animal (g of total kcal) | 71.87 ± 10.06 | 71.94 ± 10.98 | 71.37 ± 13.18 | 0.948 |
| Plant (g of total kcal) | 24.96 ± 10.62 | 25.44 ± 10.98 | 27.85 ± 15.63 | 0.752 |
| Carbohydrate (g of total kcal) | 302.62 ± 37.01 | 303.83 ± 30.79 | 305.91 ± 40.54 | 0.954 |
| Complex (g of total kcal) | 188.00 ± 23.11 | 189.85 ± 19.44 | 190.84 ± 27.26 | 0.902 |
| Simple (g of total kcal) | 114.61 ± 15.60 | 113.98 ± 14.46 | 115.07 ± 16.62 | 0.979 |
| Fat (g of total kcal) | 73.24 ± 9.49 | 72.15 ± 6.69 | 72.00 ± 9.31 | 0.868 |
| SFA (g of total kcal) | 27.26 ± 7.87 | 25.67 ± 5.12 | 25.24 ± 10.17 | 0.380 |
| MUFA (g of total kcal) | 30.88 ± 3.76 | 31.40 ± 3.22 | 31.10 ± 3.86 | 0.824 |
| PUFA (g of total kcal) | 15.10 ± 6.12 | 15.08 ± 2.96 | 15.65 ± 4.53 | 0.653 |
| n-6 PUFA (gr/day) | 7.99 ± 5.08 | 7.71 ± 2.77 | 8.97 ± 4.21 | 0.385 |
| n-3 PUFA (gr/day) | 7.11 ± 1.99 | 7.38 ± 1.03 | 6.68 ± 2.10 | 0.280 |
| Parameters | Grading G2 | Stage IV (Metastases) | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | p-Value | 95% CI | R2 | OR | p-Value | 95% CI | R2 | |
| Age (years) | 1.02 | 0.217 | 0.99–1.05 | 0.019 | 1.02 | 0.359 | 0.98–1.05 | 0.010 |
| Anthropometric measurement | ||||||||
| BMI (kg/m2) | 1.06 | 0.191 | 0.97–1.15 | 0.021 | 1.07 | 0.145 | 0.98–1.17 | 0.026 |
| WC (cm) | 0.07 | 0.049 | 0.99–1.06 | 0.036 | 1.03 | 0.049 | 1.00– 1.07 | 0.048 |
| Blood pressure | ||||||||
| SBP (mmHg) | 1.05 | 0.018 | 1.01–1.09 | 0.071 | 1.05 | 0.020 | 1.00–1.10 | 0.069 |
| DBP (mmHg) | 1.04 | 0.125 | 0.99–1.11 | 0.029 | 1.05 | 0.114 | 0.99–1.12 | 0.031 |
| Metabolic profile | ||||||||
| Fasting Glucose (mg/dL) | 1.06 | 0.002 | 1.02–1.09 | 0.136 | 1.05 | 0.005 | 1.01–1.09 | 0.108 |
| Total cholesterol (mg/dL) | 1.03 | <0.001 | 1.02–1.05 | 0.241 | 1.02 | 0.004 | 1.00–1.04 | 0.108 |
| HDL cholesterol (mg/dL) | 0.97 | 0.044 | 0.94–1.00 | 0.045 | 0.93 | 0.011 | 0.88–0.98 | 0.105 |
| LDL cholesterol (mg/dL) | 1.03 | <0.001 | 1.02–1.05 | 0.242 | 1.02 | 0.003 | 1.00–1.04 | 0.114 |
| Triglycerides (mg/dL) | 1.01 | 0.007 | 1.00–1.03 | 0.094 | 1.02 | 0.001 | 1.00–1.04 | 0.157 |
| Bioelectical variables | ||||||||
| R (Ω) | 1.00 | 0.109 | 0.99–1.01 | 0.032 | 1.00 | 0.667 | 0.99–1.00 | 0.002 |
| Xc (Ω) | 0.88 | <0.001 | 0.83–0.95 | 0.200 | 0.94 | 0.031 | 0.89–0.99 | 0.060 |
| PhA (°) | 0.01 | <0.001 | 0.01–0.08 | 0.529 | 0.31 | 0.001 | 0.15–0.64 | 0.149 |
| Nutritional assessment | ||||||||
| PREDIMED score | 0.31 | <0.001 | 0.19–0.50 | 0.486 | 0.66 | 0.001 | 0.51–0.85 | 0.137 |
| Total energy (kcal) | 1.00 | 0.113 | 1.00–1.01 | 0.031 | 1.00 | 0.898 | 0.99–1.00 | 0.000 |
| Protein (g of total kcal) | 1.01 | 0.029 | 1.00–1.07 | 0.061 | 1.02 | 0.042 | 0.99–1.06 | 0.026 |
| Animal (g of total kcal) | 1.03 | 0.164 | 0.98–1.07 | 0.024 | 1.00 | 0.909 | 0.96–1.05 | 0.000 |
| Plant (g of total kcal) | 1.03 | 0.171 | 0.99–1.07 | 0.023 | 1.03 | 0.002 | 0.99–1.08 | 0.033 |
| Carbohydrate (g of total kcal) | 1.00 | 0.272 | 0.99–1.02 | 0.015 | 0.99 | 0.686 | 0.98–1.01 | 0.002 |
| Complex (g of total kcal) | 1.00 | 0.661 | 0.98–1.02 | 0.002 | 0.99 | 0.430 | 0.97–1.01 | 0.008 |
| Simple (g of total kcal) | 1.03 | 0.042 | 0.99–1.06 | 0.044 | 1.00 | 0.808 | 0.97–1.04 | 0.001 |
| Fat (gr of total kcal) | 1.03 | 0.218 | 0.98–1.09 | 0.019 | 1.00 | 0.983 | 0.95–1.06 | 0.000 |
| SFA (g of total kcal) | 1.02 | 0.555 | 0.96–1.08 | 0.004 | 1.01 | 0.136 | 0.95–1.08 | 0.002 |
| MUFA (g of total kcal) | 1.03 | 0.610 | 0.91–1.17 | 0.003 | 0.99 | 0.954 | 0.87–1.14 | 0.000 |
| PUFA (g of total kcal) | 1.04 | 0.391 | 0.95–1.14 | 0.009 | 0.97 | 0.614 | 0.87–1.09 | 0.003 |
| n-6 PUFA (g/day) | 1.07 | 0.081 | 0.96–1.20 | 0.020 | 0.99 | 0.807 | 0.87–1.11 | 0.001 |
| n-3 PUFA (g/day) | 0.92 | 0.502 | 0.71–1.18 | 0.005 | 0.89 | 0.428 | 0.68–1.18 | 0.008 |
| Progressive Disease | |||
|---|---|---|---|
| Parameters | χ2 | p Value | AIC |
| Age (years) | 107.35 | 0.054 | 201.30 |
| Anthropometric measurement | |||
| BMI (kg/m2) | 176.49 | 0.125 | 317.39 |
| WC (cm) | 156.71 | 0.033 | 266.41 |
| Blood pressure | |||
| SBD (mmHg) | 28.64 | 0.050 | 75.82 |
| DBD (mmHg) | 23.06 | 0.027 | 56.61 |
| Metabolic profile | |||
| Fasting Glucose (mg/dL) | 116.57 | 0.043 | 215.48 |
| Total cholesterol (mg/dL) | 140.08 | 0.220 | 277.92 |
| HDL cholesterol (mg/dL) | 109.25 | 0.011 | 187.09 |
| LDL cholesterol (mg/dL) | 168.17 | 0.147 | 309.55 |
| Triglycerides (mg/dL) | 159.85 | 0.030 | 269.70 |
| Bioelectical variables | |||
| R (Ω) | 156.03 | 0.233 | 303.33 |
| Xc (Ω) | 82.00 | 0.088 | 173.49 |
| PhA (°) | 85.71 | 0.010 | 154.83 |
| Nutritional assessment | |||
| PREDIMED score | 32.24 | 0.005 | 70.80 |
| Total energy (kcal) | 173.72 | 0.217 | 326.77 |
| Protein (g of total kcal) | 179.26 | 0.196 | 332.00 |
| Animal (g of total kcal) | 179.23 | 0.195 | 332.01 |
| Plant (g of total kcal) | 179.25 | 0.197 | 331.09 |
| Carbohydrate (g of total kcal) | 178.25 | 0.196 | 332.08 |
| Complex (g of total kcal) | 179.26 | 0.199 | 332.00 |
| Simple (g of total kcal) | 176.26 | 0.191 | 331.00 |
| Fat (g of total kcal) | 173.72 | 0.217 | 326.77 |
| SFA (g of total kcal) | 176.48 | 0.206 | 329.38 |
| MUFA (g of total kcal) | 173.72 | 0.217 | 326.77 |
| PUFA (g of total kcal) | 176.49 | 0.176 | 325.39 |
| n-6 PUFA (gr/day) | 176.50 | 0.206 | 329.39 |
| n-3 PUFA (gr/day) | 176.48 | 0.085 | 309.38 |
| Parameters | Multiple Regression Analysis | |||
|---|---|---|---|---|
| Model 1–Tumor Grading- | R2 | β | t | p value |
| PREDIMED score | 0.591 | −0.724 | −9.45 | <0.001 |
| PhA (°) | 0.595 | −0.394 | −4.04 | <0.001 |
| Simple carbohydrate (g of total kcal) | 0.629 | 0.194 | 2.88 | 0.005 |
| LDL cholesterol (mg/dL) | 0.646 | 0.171 | 2.19 | 0.031 |
| Variable excluded: WC, SBP, fasting Glucose, total cholesterol, HDL cholesterol, triglycerides, Xc, protein (g of total kcal). | ||||
| Model 2–Tumor Stage- | R2 | β | t | p value |
| Triglycerides (mg/dL) | 0.151 | 0.402 | 3.95 | <0.001 |
| PREDIMED score | 0.232 | −0.306 | −3.08 | 0.003 |
| Variable excluded: WC, SBP, DBP, fasting Glucose, HDL cholesterol, PhA. | ||||
| Model 3–Disease Status- | R2 | β | t | p value |
| PREDIMED score | 0.152 | −0.403 | −3.96 | <0.001 |
| Variable excluded: WC, SBP, DBP, fasting Glucose, HDL cholesterol, triglycerides, PhA. | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrea, L.; Altieri, B.; Muscogiuri, G.; Laudisio, D.; Annunziata, G.; Colao, A.; Faggiano, A.; Savastano, S. Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness. Nutrients 2018, 10, 1854. https://doi.org/10.3390/nu10121854
Barrea L, Altieri B, Muscogiuri G, Laudisio D, Annunziata G, Colao A, Faggiano A, Savastano S. Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness. Nutrients. 2018; 10(12):1854. https://doi.org/10.3390/nu10121854
Chicago/Turabian StyleBarrea, Luigi, Barbara Altieri, Giovanna Muscogiuri, Daniela Laudisio, Giuseppe Annunziata, Annamaria Colao, Antongiulio Faggiano, and Silvia Savastano. 2018. "Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness" Nutrients 10, no. 12: 1854. https://doi.org/10.3390/nu10121854