Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Eligibility
2.3. Recruitment
2.4. Study Design and Data Collection
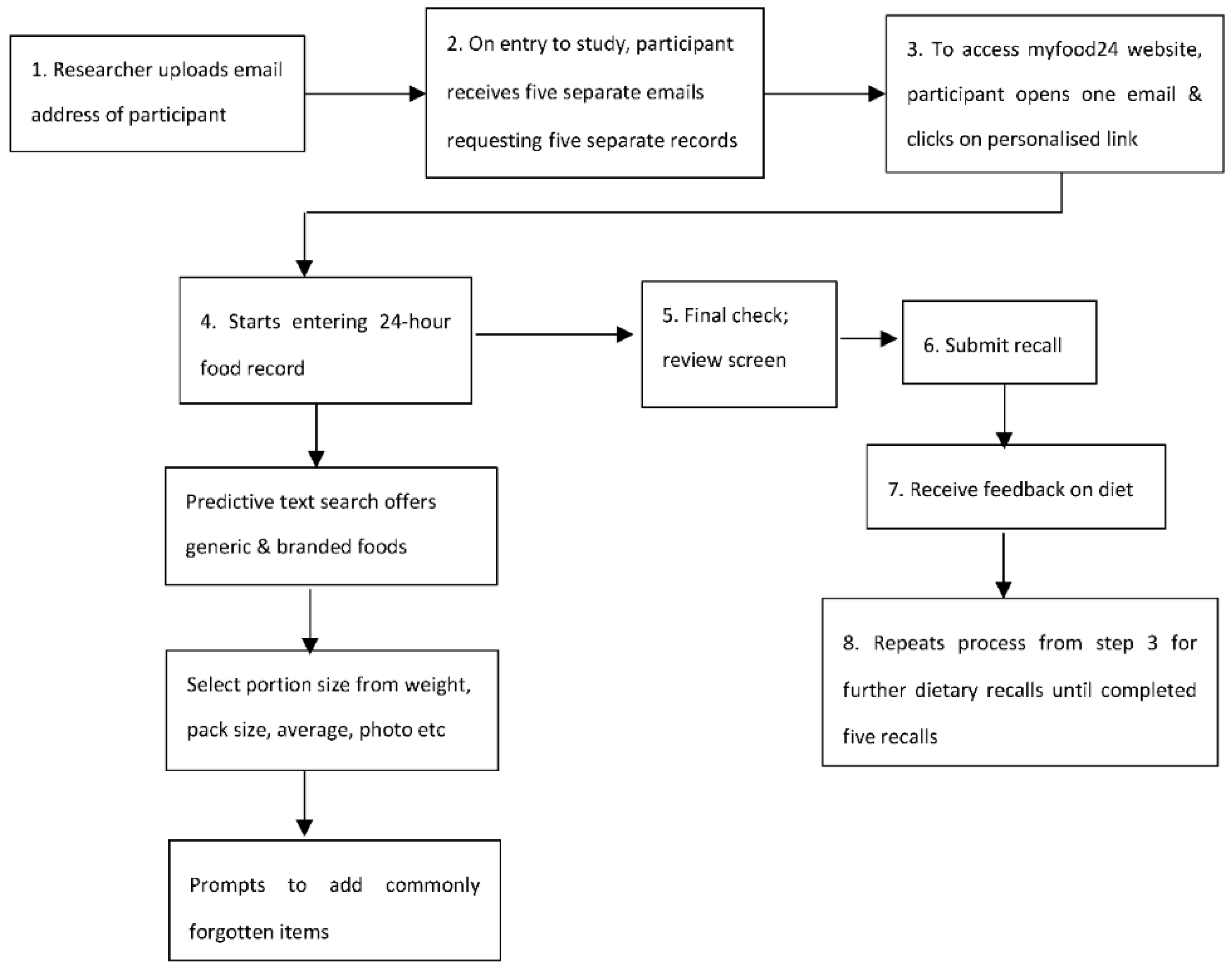
2.4.1. Completing a Food Record Using myfood24
2.4.2. User Questionnaire
2.4.3. Interviews
2.5. Data Analysis
2.5.1. Statistical Analyses
2.5.2. Analysis of Interviews
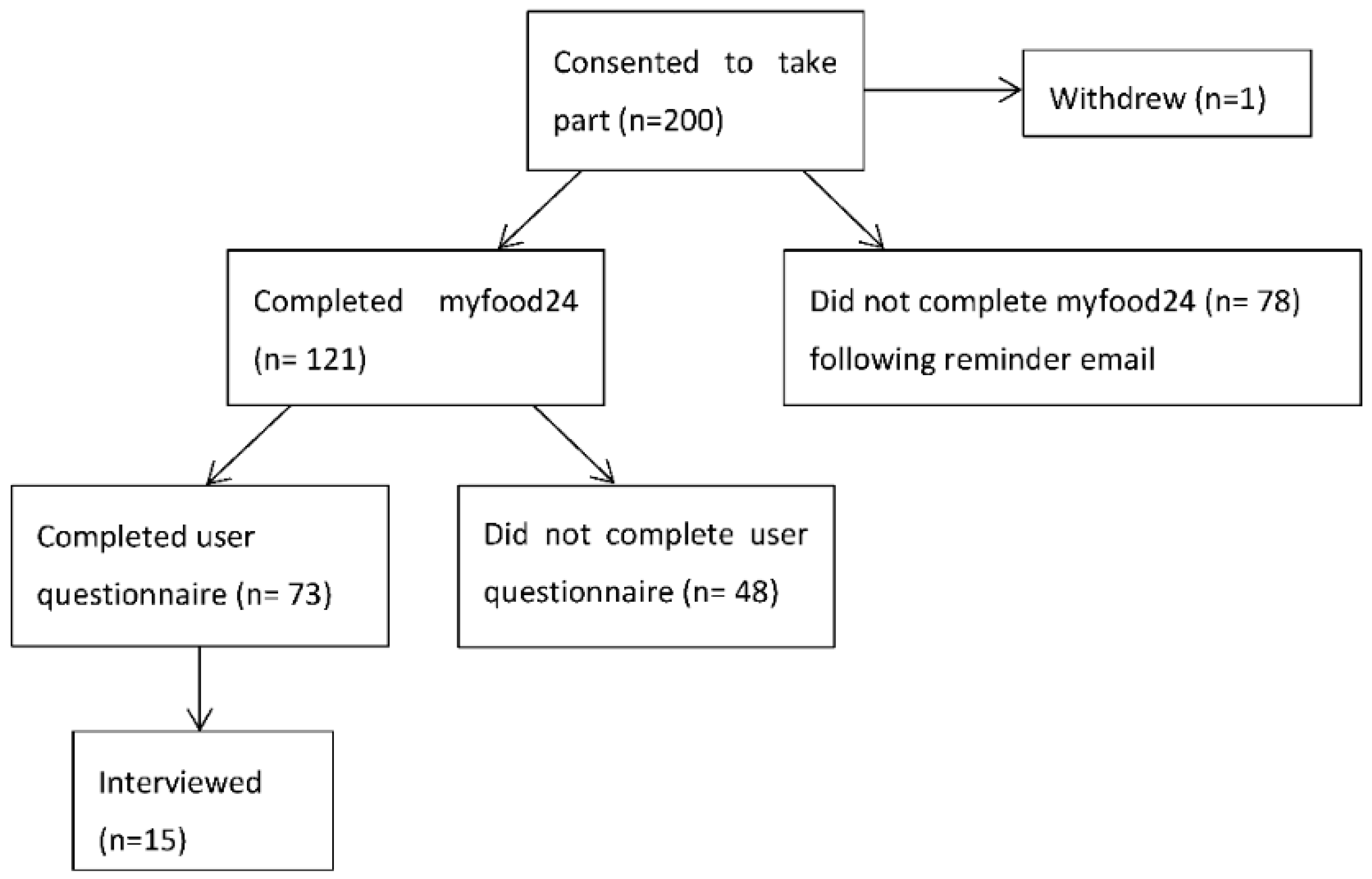
3. Results
3.1. Characteristics of Participants
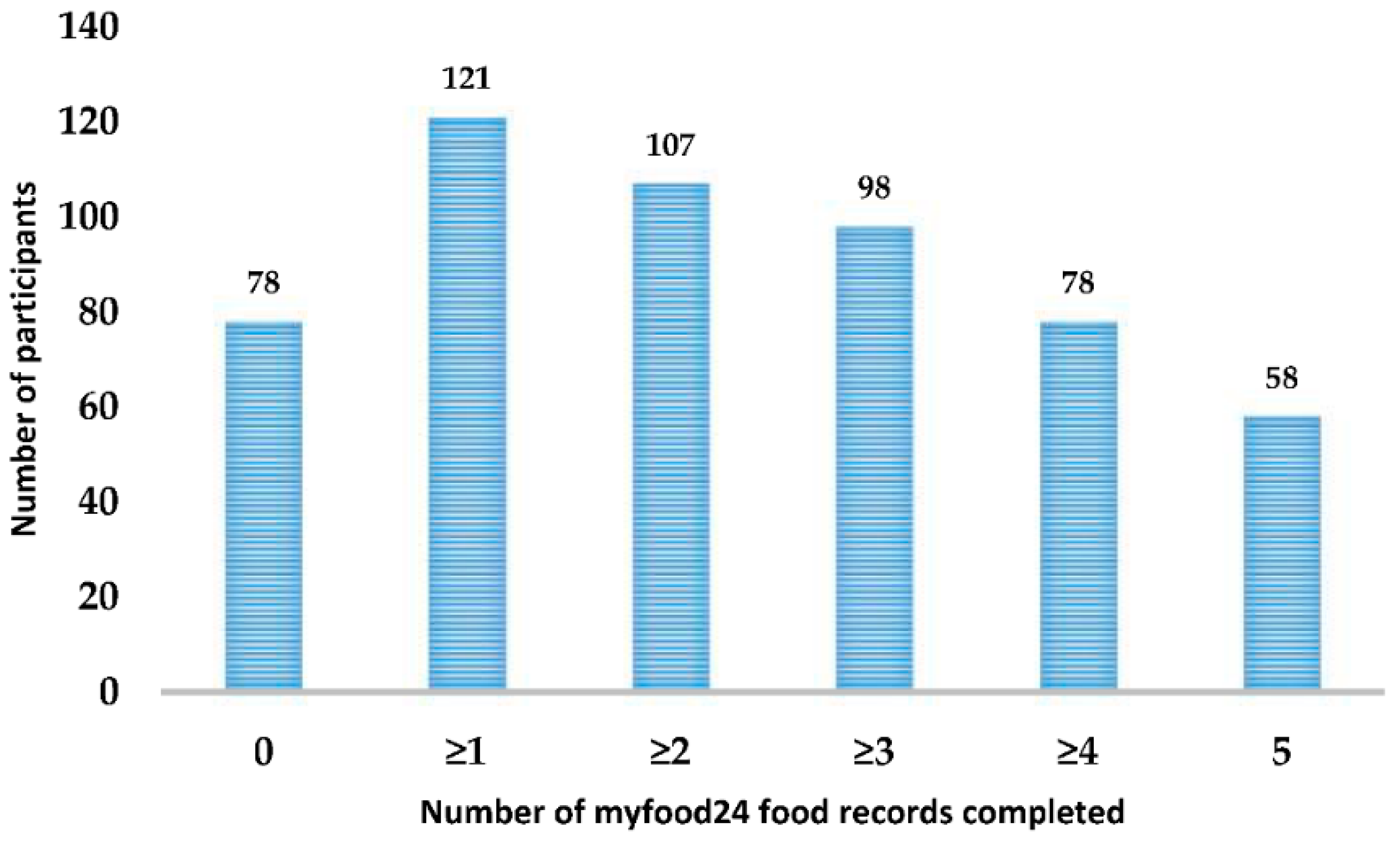
3.2. Completion of myfood24 Recalls
3.3. User Questionnaire
3.4. Interviews
3.4.1. Characteristics of Interviewees
3.4.2. Themes
‘I found it quite easy… I mean, you just typed in a word and it would bring what you wanted up and then you chose from the list’.(Interview 3)
‘Obviously you don’t weigh your food… it was nice to see actually a portion size’(interview 6)
‘I didn’t have to go back and correct anything really because it reminded me’(interview 3)
‘For something that was quite simple, it would take actually a long time to find it’(interview 4)
‘It was quite time consuming having to kind of search for things and put everything in in its own, you know, like all the different components that made up a meal’.(interview 11)
‘I did find it frustrating, to be honest, in terms of just trying to find what matched what I was eating, I don’t know how accurate it was for me’(Interview 4)
‘a week’s worth of days in front of you it does make you think about what you’re eating and how much’(Interview 3)
‘I was like ooh I shouldn’t have eaten that or oh, I’ve had a really good day today.’(Interview 12)
‘Once you can see it in numbers and can see the picture of it, it’s harder just to shrug off and think I’m fine...I couldn’t just go on with it’ (interview 11).
‘I thought that [myfood24] made me remember things. It was more specific. I think it was easy to forget when you’re writing it down. You know because it reminded you—have you remembered to put a drink down here, have you remembered to put a snack down there.’(Interview 9)
‘I think a phone app would be a lot easier…you’d just keep updating it as the day went along… it’d make it more helpful like that’(Interview 12)
‘I don’t know if there was an option where you could save that information, and maybe it was something that I missed, but I would have found that useful as an ongoing thing, if you could save it…’(Interview 7)
‘I thought what might be quite useful would be more like a graph … that shows like you’re here and this is what you really should be getting, aiming for.’(Interview 2)
4. Discussion
4.1. Feasibility of Using myfood24 as An Electronic Food Record
4.2. Usability
4.3. Improving Uptake of Use of the Tool and Usability of Software in the Future
4.4. Opportunities for Use of myfood24 in a Clinical Setting
4.5. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- NICE. Diabetes in Pregnancy: Management from Preconception to the Postnatal Period; NICE Guidelines [NG3]; NICE: London, UK, 2015. [Google Scholar]
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Lawlor, D.A. Treatments for gestational diabetes: A systematic review and meta-analysis. BMJ Open 2017, 7, e015557. [Google Scholar] [CrossRef] [PubMed]
- Noctor, E.; Dunne, F. A practical guide to pregnancy complicated by diabetes. Diabetes Prim. Care 2014, 16, 146–153. [Google Scholar]
- Bingham, S.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.; Roe, L.; Day, N.E. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1997, 72, 619–643. [Google Scholar] [CrossRef]
- Illner, A.-K.; Freisling, H.; Boeing, H.; Huybrechts, I.; Crispim, S.P.; Slimani, N. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int. J. Epidemiol. 2012, 41, 1187–1203. [Google Scholar] [CrossRef] [PubMed]
- Timon, C.M.; van den Barg, R.; Blain, R.J.; Kehoe, L.; Evans, K.; Walton, J.; Flynn, A.; Gibney, E.R. A review of the design and validation of web- and computer-based 24-h dietary recall tools. Nutr. Res. Rev. 2016, 29, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Sharp, D.B.; Allman-Farinelli, M. Feasibility and validity of mobile phones to assess dietary intake. Nutrition 2014, 30, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Rusin, M.; Arsand, E.; Hartvigsen, G. Functionalities and input methods for recording food intake: A systematic review. Int. J. Med. Inform. 2013, 82, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Long, J.D.; Littlefield, L.A.; Estep, G.; Martin, H.; Rogers, T.J.; Boswell, C.; Shriver, B.J.; Roman-Shriver, C.R. Evidence Review of Technology and Dietary Assessment. Worldviews Evid. Based Nurs. 2010, 7, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.; Hawkins, A.; Delve, J.; Adamson, A.J. Reducing the cost of dietary assessment: Self-completed recall and analysis of nutrtion for use with children (SCRAN24). J. Hum. Nutr. Diet. 2014, 27 (Suppl. 1), 26–35. [Google Scholar] [CrossRef]
- Thompson, F.E.; Subar, A.F.; Loria, C.M.; Reedy, J.L.; Baranowski, T. Need for technological innovation in dietary assessment. J. Am. Diet. Assoc. 2010, 110, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Probst, Y.C.; Faraji, S.; Batterham, M.; Steel, D.G.; Tapsell, L.C. Computerized dietary assessments compare well with interviewer administered diet histories for patients with type 2 diabetes mellitus in the primary healthcare setting. Patient Educ. Couns. 2008, 72, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Touvier, M.; Kesse-Guyot, E.; Mejean, C.; Pollet, C.; Malon, A.; Castetbon, K. Comparison between an interactive web-based self-administered 24 h dietary record and an interview by a dietitian for large-scale epidemiological studies. Br. J. Nutr. 2011, 105, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Ngo, J.; Engelen, A.; Molag, M.; Roesle, J.; García-Segovia, P.; Serra-Majem, L. A review of the use of information and communication technologies for dietary assessment. Br. J. Nutr. 2009, 101 (Suppl. 2), S102–S112. [Google Scholar] [CrossRef]
- Porter, J.; Huggins, C.E.; Truby, H.; Collins, J. The Effect of Using Mobile Technology-Based Methods That Record Food or Nutrient Intake on Diabetes Control and Nutrition Outcomes: A Systematic Review. Nutrients 2016, 8, 815. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.; Porter, J. Dietary mobile apps and their effect on nutritional indicators in chronic renal disease: A systematic review. Nephrology 2015, 20, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, C.; Brauer, P.; Royall, D.; Keller, H.; Hanning, R.M.; Dicenso, A. Use of electronic dietary assessment tools in primary care: An interdisciplinary perspective. BMC Med. Inform. Decis. Mak. 2015, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- Ashman, A.M.; Collins, C.E.; Brown, L.J.; Rae, K.M.; Rollo, M.E. Validation of a Smartphone Image-Based Dietary Assessment Method for Pregnant Women. Nutrients 2017, 9, E73. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Albar, S.A.; Morris, M.A.; Mulla, U.Z.; Hancock, N.; Evans, C.E.; Alwan, N.A.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S.; et al. Development of a UK Online 24-h Dietary Assessment Tool: Myfood24. Nutrients 2015, 7, 4016–4032. [Google Scholar] [CrossRef] [PubMed]
- Albar, S.A.; Carter, M.C.; Alwan, N.A.; Evans, C.E.L.; Cade, J.E. Formative evaluation of the usability and acceptability of myfood24 among adolescents: A UK online dietary assessments tool. BMC Nutr. 2015, 1, 29. [Google Scholar] [CrossRef]
- Albar, S.; Alwan, N.; Evans, C.; Greenwood, D.; Cade, J. Agreement between an online dietary assessment tool (myfood24) and an interview-administered 24-h dietary recall in British adolescents aged 11–18 years. Br. J. Nutr. 2016, 115, 1678–1686. [Google Scholar] [CrossRef] [PubMed]
- Wark, P.; Hardie, L.; Frost, G.; Alwan, N.; Carter, M.; Elliott, P.; Ford, H.E.; Hancock, N.; Morris, M.A.; Mulla, U.Z.; et al. Validity of an online 24-hour recall tool (myfood24) for dietary assessment in population studies: Comparison with biomarkers and standard interviews. BMC Med. 2018, 16, 136. [Google Scholar] [CrossRef] [PubMed]
- Virzi, R.A. Streamlining the Design Process: Running Fewer Subjects. Available online: http://journals.sagepub.com/doi/abs/10.1177/154193129003400411 (accessed on 22 August 2018).
- Guest, G.; Bunce, A.; Johnson, J. How Many Interviews Are Enough?: An Experiment with Data Saturation and Variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Bristol Online Survey. Available online: https://www.onlinesurveys.ac.uk/ (accessed on 22 August 2018).
- Brooke, J. SUS—A Quick and Dirty Usability Scale. Available online: https://hell.meiert.org/core/pdf/sus.pdf (accessed on 22 August 2018).
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Petrie, H.; Bevan, N. The Evaluation of Acceptability, Usability and User Experience; The Universal Access Handbook; CRC Press: Boca Raton, FL, USA, 2009; pp. 10–20. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- NICE. Health App: GDm-Health for People with Gestational Diabetes. Available online: https://www.nice.org.uk/advice/mib131/chapter/The-technology#current-care-pathway (accessed on 22 April 2018).
- Rollo, M.E.; Ash, S.; Lyons-Wall, P.; Russell, A.W. Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes. Nutrients 2015, 7, 4897–4910. [Google Scholar] [CrossRef] [PubMed]
- Lieffers, J.R.; Hanning, R.M. Dietary Assessment and Self-monitoring: With Nutrition Applications for Mobile Devices. Can.J. Diet. Pract. Res. 2012, 73, e253–e260. [Google Scholar] [CrossRef] [PubMed]
- Probst, Y.C.; Tapsell, L.C. Computerised dietary assessment interviews: Health professionals and patients’ opinions about web communications. Nutr. Diet. 2012, 69, 56–63. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.; Nykjaer, C.; Cade, J. “My Meal Mate” (MMM): Validation of the diet measures captured on a smartphone application to facilitate weight loss. Br. J. Nutr. 2013, 109, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Darwin, Z.; Smith, D.; Haddrill, R.; Scott, E.; McGowan, L.; Cade, J. Women’s experiences of pregnancy and the management of gestational diabetes: A qualitative interview study. BMC Pregnancy Childbirth 2018. submitted. [Google Scholar]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Sturt, J.; Dennick, K.; Hessler, D.; Hunter, B.M.; Oliver, J.; Fisher, L. Effective interventions for reducing diabetes distress; systematic review and metaanlysis. Int. Diabetes Nurs. 2015, 12, 40–55. [Google Scholar] [CrossRef]
- Fisher, L.; Hessler, D.; Glasgow, R.E.; Arean, P.A.; Masharani, U.; Naranjo, D.; Strycker, L.A. REDEEM: A pragmatic trial to reduce diabetes distress. Diabetes Care 2013, 36, 2551–2558. [Google Scholar] [CrossRef] [PubMed]
- Jenum, A.K.; Mørkrid, K.; Sletner, L.; Vangen, S.; Vange, S.; Torper, J.L.; Nakstad, B.; Voldner, N.; Rognerud-Jensen, O.H.; Berntsen, S.; et al. Impact of ethnicity on gestational diabetes identified with the WHO and the modified International Association of Diabetes and Pregnancy Study Groups criteria: A population-based cohort study. Eur. J. Endocrinol. 2012, 166, 317–324. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Completed myfood24 (n = 121) | Not Completed myfood24 (n = 78) | p Value | |||
|---|---|---|---|---|---|
| n | Mean | n | Mean | ||
| Maternal Age, years (SD) | 121 | 33.5 (4.6) | 78 | 33.2 (5.6) | 0.7 |
| Booking body mass index (BMI), kg/m² (SD) | 119 | 29.5 (6.2) | 77 | 30.0 (7.0) | 0.7 |
| Fasting Blood Glucose, mmol/l (SD) | 115 | 4.9 (0.6) | 61 | 5.2 (0.8) | 0.008 |
| Ethnicity | 0.001 | ||||
| White (%) | 79 | 65.3 | 35 | 44.9 | |
| Asian (%) | 31 | 25.6 | 23 | 29.5 | |
| * Other (%) | 11 | 9.1 | 20 | 25.6 | |
| Parity | 0.02 | ||||
| Primiparous (%) | 52 | 43 | 21 | 26.9 | |
| Multiparous (%) | 69 | 57 | 57 | 73.1 | |
| Completed User Q | Did Not Return User Q | p Value | |||
|---|---|---|---|---|---|
| n | Mean | n | Mean | ||
| Age, Years (SD) | 73 | 34.3 (4.3) | 48 | 32.2 (4.7) | 0.01 |
| Pre-Pregnancy BMI, kg/m2 (SD) | 72 | 28.3 (5.0) | 47 | 31.4 (7.5) | 0.008 |
| Fasting Blood Glucose, mmol/L (SD) | 72 | 4.9 (0.7) | 43 | 5.0 (0.5) | 0.5 |
| Ethnicity | |||||
| White (%) | 52 | 71.2 | 27 | 56.3 | 0.4 |
| Asian (%) | 15 | 20.6 | 16 | 33.3 | |
| Other (%) | 6 | 8.2 | 5 | 10.4 | |
| Parity | 0.9 | ||||
| Primiparous (%) | 31 | 42.5 | 21 | 43.8 | |
| Multiparous (%) | 42 | 57.5 | 27 | 56.2 | |
| Number of days completed myfood24 (SD) | 73 | 4.2 (1.1) | 48 | 3.2 (1.6) | <0.001 |
| System Usability Scale (SUS) score (95% CI) | 73 | 70.9 (67.1, 74.6) | - | - | - |
| Occupation | 68 | - | - | - | |
| Managerial & professionals (%) | 32 | 47 | |||
| Intermediate & lower supervisory | 17 | 25 | |||
| Semi routine & routine (%) | 4 | 6 | |||
| Not employed (%) | 15 | 22 | |||
| Education level | 70 | - | - | - | |
| Degree or above (%) | 42 | 58.3 | |||
| No degree (%) | 30 | 41.7 | |||
| Had previously filled in food diary (%) | 26 | 35.6 | - | - | - |
| Previously used technology to record food (%) | 33 | 45.2 | - | - | - |
| Internet ability good to excellent (%) | 71 | 97.3 | - | - | - |
| Access to internet (%) | 72 | 98.6 | - | - | - |
| Use internet daily (%) | 69 | 94.5 | - | - | - |
| Confident in using technology (%) | 66 | 90.4 | - | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianfrancesco, C.; Darwin, Z.; McGowan, L.; Smith, D.M.; Haddrill, R.; Carter, M.; Scott, E.M.; Alwan, N.A.; Morris, M.A.; Albar, S.A.; et al. Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients 2018, 10, 1147. https://doi.org/10.3390/nu10091147
Gianfrancesco C, Darwin Z, McGowan L, Smith DM, Haddrill R, Carter M, Scott EM, Alwan NA, Morris MA, Albar SA, et al. Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients. 2018; 10(9):1147. https://doi.org/10.3390/nu10091147
Chicago/Turabian StyleGianfrancesco, Carla, Zoe Darwin, Linda McGowan, Debbie M. Smith, Roz Haddrill, Michelle Carter, Eleanor M. Scott, Nisreen A. Alwan, Michelle A. Morris, Salwa A. Albar, and et al. 2018. "Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes" Nutrients 10, no. 9: 1147. https://doi.org/10.3390/nu10091147
APA StyleGianfrancesco, C., Darwin, Z., McGowan, L., Smith, D. M., Haddrill, R., Carter, M., Scott, E. M., Alwan, N. A., Morris, M. A., Albar, S. A., & Cade, J. E. (2018). Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients, 10(9), 1147. https://doi.org/10.3390/nu10091147