Effects of Blackcurrant Anthocyanin on Endothelial Function and Peripheral Temperature in Young Smokers

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
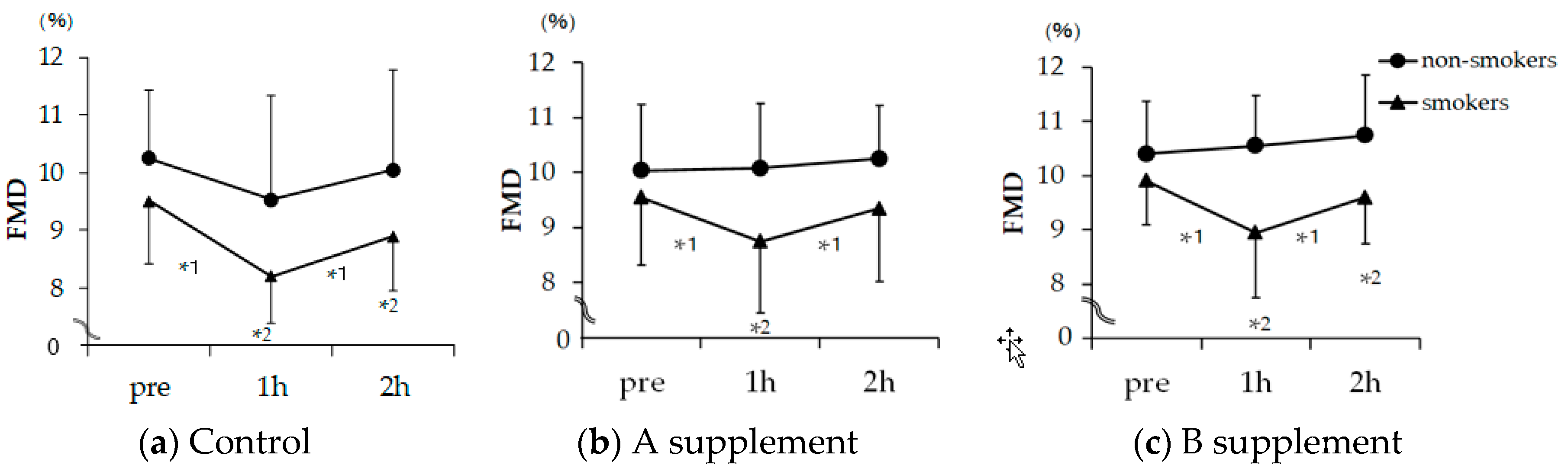
2.1. FMD
2.2. Skin Temperature
3. Discussion
3.1. Effect of Smoking on Endothelial Function
3.2. Antioxidants in Blackcurrant
3.3. Effect of Blackcurrant on Smoking-Induced Endothelial Dysfunction
4. Materials and Methods
4.1. Subjects
4.2. Study Design
4.3. Measurement of FMD
4.4. Temperature of the Skin
4.5. Statistical Analysis
4.6. Ethical Issues
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Laurent, S.; Boutouyrie, P. Arterial Stiffness and Stroke in Hypertension Therapeutic Implications for Stroke Prevention. CNS Drugs 2005, 19, 1–11. [Google Scholar] [CrossRef]
- Suzuki, J.; Kurosu, T.; Kon, T.; Tomaru, T. Impact of cardiovascular risk factors on progression of arteriosclerosis in younger patients: Evaluation by carotid duplex ultrasonography and cardio-ankle vascular index(CAVI). J. Atheroscler. Thromb. 2014, 21, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Teo, K.K.; Ounpuu, S.; Hawken, S.; Pandey, M.R.; Valentin, V.; Hunt, D.; Diaz, R.; Rashed, W.; Freeman, R.; Jiang, L.; et al. Interheart. Study Investigators. Tobacco Use and Risk of Myocardial in Farction in 52 Countries in the INTERHEART Study: A Case-Control Study. Lancet 2006, 368, 647–658. [Google Scholar] [CrossRef]
- Godo, S.; Shimokawa, H. Endothelial Functions. Arterioscler. Thromb. Vasc. Biol. 2017, 37, e108–e114. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, C.; Kamiloglu, S.; Capanoglu, E.; Van Camp, J. Cell Systems to Investigate the Impact of Polyphenols on Cardiovascular Health. Nutrients 2015, 7, 9229–9255. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A.; García-Cardeña, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Chun, O.K.; Chung, S.J.; Song, W.O. Estimated dietary flavonoid intake and major food sources of U.S. adults. J. Nutr. 2007, 137, 1244–1252. [Google Scholar] [CrossRef]
- Kim, K.; Vance, T.M.; Chun, O.K. Estimated intake and major food sources of flavonoids among US adults: Changes between 1999–2002 and 2007–2010 in NHANES. Eur. J. Nutr. 2016, 55, 833–843. [Google Scholar] [CrossRef]
- Manach, C.; Donovan, J.L. Pharmacokinetics and metabolism of dietary flavonoids in humans. Free Radic. Res. 2004, 38, 771–785. [Google Scholar] [CrossRef]
- Heiss, C.; Jahn, S.; Taylor, M.; Real, W.M.; Angeli, F.S.; Wong, M.L.; Amabile, N.; Prasad, M.; Rassaf, T.; Ottaviani, J.I.; et al. Improvement of endothelial function with dietary flavanols is associated with mobilization of circulating angiogenic cells in patients with coronary artery disease. J. Am. Coll. Cardiol. 2010, 56, 218–224. [Google Scholar] [CrossRef]
- Mink, P.J.; Scrafford, C.G.; Barraj, L.M.; Harnack, L.; Hong, C.P.; Nettleton, J.A.; Jacobs, D.R., Jr. Flavonoid intake and cardiovascular disease mortality: A prospective study in postmenopausal women. Am. J. Clin. Nutr. 2007, 85, 895–909. [Google Scholar] [CrossRef] [PubMed]
- Arts, I.C.W.; Hollman, P.C.H. Polyphenols and disease risk in epidemiologic studies. Am. J. Clin. Nutr. 2005, 81, 317S–325S. [Google Scholar] [CrossRef] [PubMed]
- Thoppil, R.J.; Bhatia, D.; Barnes, K.F.; Haznagy-Radnai, E.; Hohmann, J.; Darvesh, A.S.; Bishayee, A. Black currant anthocyanins abrogate oxidative stress through Nrf2-mediated antioxidant mechanisms in a rat model of hepatocellular carcinoma. Curr. Cancer Drug Targets 2012, 12, 1244–1257. [Google Scholar] [PubMed]
- Bishayee, A.; Mbimba, T.; Thoppil, R.J.; Háznagy-Radnai, E.; Sipos, P.; Darvesh, A.S.; Folkesson, H.G.; Hohmann, J. Anthocyanin-rich black currant (Ribes nigrum L.) extract affords chemoprevention against diethylnitrosamine-induced hepatocellular carcinogenesis in rats. J. Nutr. Biochem. 2011, 22, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Bishayee, A.; Háznagy-Radnai, E.; Mbimba, T.; Sipos, P.; Morazzoni, P.; Darvesh, A.S.; Bhatia, D.; Hohmann, J. Anthocyanin-rich black currant extract suppresses the growth of human hepatocellular carcinoma cells. Nat. Prod. Commun. 2010, 5, 1613–1618. [Google Scholar] [CrossRef]
- Al-Awwadi, N.A.; Araiz, C.; Bornet, A.; Delbosc, S.; Cristol, J.P.; Linck, N.; Azay, J.; Teissedre, P.L.; Cros, G. Extracts enriched in different polyphenolic families normalize increased cardiac NADPH oxidase expression while having differential effects on insulin resistance, hypertension, and cardiac hypertrophy in high-fructose-fed rats. J. Agric. Food Chem. 2005, 53, 151–157. [Google Scholar] [CrossRef]
- Sasaki, R.; Nishimura, N.; Hoshino, H.; Isa, Y.; Kadowaki, M.; Ichi, T.; Tanaka, A.; Nishiumi, S.; Fukuda, I.; Ashida, H.; et al. Cyanidin 3-glucoside ameliorates hyperglycemia and insulin sensitivity due to downregulation of retinol binding protein 4 expression in diabetic mice. Biochem. Pharmacol. 2007, 74, 1619–1627. [Google Scholar] [CrossRef]
- Parkar, S.G.; Redgate, E.L.; McGhie, T.K.; Hurst, R.D. In vitro studies of modulation of pathogenic and probiotic bacterial proliferation and adhesion to intestinal cells by blackcurrant juices. J. Funct. Foods 2014, 8, 35–44. [Google Scholar] [CrossRef]
- Cisowska, A.; Wojnicz, D.; Hendrich, A.B. Anthocyanins as antimicrobial agents of natural plant origin. Nat. Prod. Commun. 2011, 6, 149–156. [Google Scholar] [CrossRef]
- Ohguro, H.; Ohguro, I.; Yagi, S. Effects of black currant anthocyanins on intraocular pressure in healthy volunteers and patients with glaucoma. J. Ocul. Pharmacol. Ther. 2013, 29, 61–67. [Google Scholar] [CrossRef]
- Ohguro, H.; Ohguro, I.; Katai, M.; Tanaka, S. Two-year randomized, placebo-controlled study of black currant anthocyanins on visual field in glaucoma. Ophthalmologica 2012, 228, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Nakaishi, H.; Matsumoto, H.; Tominaga, S.; Hirayama, M. Effects of black current anthocyanoside intake on dark adaptation and VDT work-induced transient refractive alteration in healthy humans. Altern. Med. Rev. 2000, 5, 553–562. [Google Scholar] [PubMed]
- Matsumoto, H.; Takenami, E.; Iwasaki-Kurashige, K.; Osada, T.; Katsumura, T.; Hamaoka, T. Effects of blackcurrant anthocyanin intake on peripheral muscle circulation during typing work in humans. Eur. J. Appl. Physiol. 2005, 94, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Xia, M.; Ma, J.; Hao, Y.; Liu, J.; Mou, H.; Cao, L.; Ling, W. Anthocyanin supplementation improves serum LDL- and HDL-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Lyall, K.A.; Hurst, S.M.; Cooney, J.; Jensen, D.; Lo, K.; Hurst, R.D.; Stevenson, L.M. Short-term blackcurrant extract consumption modulates exercise-induced oxidative stress and lipopolysaccharide-stimulated inflammatory responses. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R70–R81. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xia, M.; Yang, Y.; Liu, F.; Li, Z.; Hao, Y.; Mi, M.; Jin, T.; Ling, W. Purified anthocyanin supplementation improves endothelial function via NO-cGMP activation in hypercholesterolemic individuals. Clin. Chem. 2011, 57, 1524–1533. [Google Scholar] [CrossRef]
- Wolfe, K.; Wu, X.; Liu, R.H. Antioxidant activity of apple peels. J. Agric. Food Chem. 2003, 51, 9–14. [Google Scholar] [CrossRef]
- Dohadwala, M.M.; Holbrook, M.; Hamburg, N.M.; Shenouda, S.M.; Chung, W.B.; Titas, M.; Kluge, M.A.; Wang, N.; Palmisano, J.; Milbury, P.E.; et al. Effects of cranberry juice consumption on vascular function in patients with coronary artery disease. Am. J. Clin. Nutr. 2011, 93, 934–940. [Google Scholar] [CrossRef]
- Elhadd, T.A.; Khan, F.; Kirk, G.; McLaren, M.; Newton, R.W.; Greene, S.A.; Belch, J.J. Influence of puberty on endothelial dysfunction and oxidative stress in young patients with type 1 diabetes. Diabetes Care 1998, 21, 1990–1996. [Google Scholar] [CrossRef]
- Neunteufl, T.; Priglinger, U.; Heher, S.; Zehetgruber, M.; Söregi, G.; Lehr, S.; Huber, K.; Maurer, G.; Weidinger, F.; Kostner, K. Effects of vitamin E on chronic and acute endothelial dysfunction in smokers. J. Am. Coll. Cardiol. 2000, 35, 277–283. [Google Scholar] [CrossRef]
- Endemann, D.H.; Schiffrin, E.L. Endothelial dysfunction. J. Am. Soc. Nephrol. 2004, 15, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.S.; Singel, D.J.; Loscalzo, J. Biochemistry of nitric oxide and its redox-activated forms. Science 1992, 258, 1898–1902. [Google Scholar] [CrossRef] [PubMed]
- Fairlie-Jones, L.; Davison, K.; Fromentin, E.; Hill, A.M. The Effect of Anthocyanin-Rich Foods or Extracts on Vascular Function in Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2017, 9, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallance, P.; Leiper, J. Blocking NO synthesis: How, where and why? Nat. Rev. Drug Discov. 2002, 1, 939–950. [Google Scholar] [CrossRef] [PubMed]
- Yoshizak, A.; Tomisawa, T.; Osanai, T.; Nanashima, N.; Kitajima, M.; Mikami, K.; Fujita, T.; Maeda, H.; Kato, Y. Single Oral Administration of Anthocyanin Rescues Smoking-Induced Dysfunction in Young Smokers but Facilitates Oxidative Stress in Non-Smokers. Food Nutr. Sci. 2018, 9, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Ovaskainen, M.L.; Törrönen, R.; Koponen, J.M.; Sinkko, H.; Hellström, J.; Reinivuo, H.; Mattila, P. Dietary intake and major food sources of polyphenols in Finnish adults. J. Nutr. 2008, 138, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Slimestad, R.; Solheim, H. Anthocyanins from black currants (Ribes nigrum L.). J. Agric. Food Chem. 2002, 50, 3228–3231. [Google Scholar] [CrossRef]
- Ghosh, D.; Konishi, T. Anthocyanins and anthocyanin-rich extracts: Role in diabetes and eye function. Asia Pac. J. Clin. Nutr. 2007, 16, 200–208. [Google Scholar]
- Gopalan, A.; Reuben, S.C.; Ahmed, S.; Darvesh, A.S.; Hohmann, J.; Bishayee, A. The health benefits of blackcurrants. Food Funct. 2012, 3, 795–809. [Google Scholar] [CrossRef]
- Ziberna, L.; Tramer, F.; Moze, S.; Vrhovsek, U.; Mattivi, F.; Passamonti, S. Transport and bioactivity of cyanidin 3-glucoside into the vascular endothelium. Free Radic. Biol. Med. 2012, 52, 1750–1759. [Google Scholar] [CrossRef]
- Shih, P.H.; Chan, Y.C.; Liao, J.W.; Wang, M.F.; Yen, G.C. Antioxidant and cognitive promotion effects of anthocyanin-rich mulberry (Morus atropurpurea L.) on senescence-accelerated mice and prevention of Alzheimer’s disease. J. Nutr. Biochem. 2010, 21, 598–605. [Google Scholar] [CrossRef]
- Ossola, B.; Kaariainen, T.M.; Mannisto, P.T. The multiple faces of quercetin in neuroprotection. Expert Opin. Drug Saf. 2009, 8, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Herman, M.G.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, H.; Kohro, T.; Higashi, Y.; Takase, B.; Suzuki, T.; Ishizu, T.; Ueda, S.; Yamazaki, T.; Furumoto, T.; Kario, K.; et al. A multicenter study design to assess the clinical usefulness of semi-automatic measurement of flow-mediated vasodilatation of the brachial artery. Int. Heart J. 2012, 53, 170–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| N Group (n = 11) | S Group (n = 13) | 2-Way Repeated Measure ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|
| pre | post1 | post2 | pre | post1 | post2 | |||
| Lt | Control | 29.2 | 29.5 | 28.6 | 29.7 | 28.8 | 27.7 | n.s. |
| A | 29.4 | 28.9 | 28.3 | 28.4 | 28.7 | 30.0 | p < 0.05 | |
| B | 27.6 | 26.5 | 26.2 | 28.6 | 27.6 | 28.4 | n.s. | |
| Rt | Control | 29.1 | 29.3 | 28.6 | 29.8 | 28.8 | 26.9 | n.s. |
| A | 29.1 | 28.8 | 28.0 | 28.2 | 28.8 | 29.5 | n.s. | |
| B | 27.5 | 26.6 | 26.4 | 28.5 | 27.3 | 28.1 | n.s. | |
| Ld | Control | 30.5 | 30.6 | 30.5 | 31.2 | 30.1 | 29.9 | n.s. |
| A | 31.2 | 30.7 | 29.3 | 30.1 | 30.3 | 31.2 | p < 0.01 | |
| B | 30.1 | 29.6 | 29.0 | 30.2 | 29.5 | 30.2 | p < 0.05 | |
| Rd | Control | 30.3 | 30.6 | 30.7 | 31.4 | 30.3 | 29.5 | p < 0.05 |
| A | 31.0 | 30.4 | 30.1 | 30.1 | 30.4 | 30.8 | p < 0.05 | |
| B | 30.3 | 29.5 | 29.2 | 30.1 | 29.6 | 30.2 | p < 0.05 | |
| Non-Smoking Group (n = 13) | Smoking Group (n = 11) | ||
|---|---|---|---|
| age (year) | 22 ± 2.1 | 21 ± 0.9 | |
| BMI (kg/m2) | 20.9 ± 1.4 | 21.3 ± 2.1 | |
| a number of cigarette (number) | 0 | 14 ± 5 | |
| nicotine (mg/a cigarette) | 0 | 1.5 ± 2.0 | |
| tar (mg/a cigarette) | 0 | 10.9 ± 3.9 | |
| Food Habit | 1 meal | 0 | 1 |
| 2 meals | 4 | 2 | |
| 3 meals | 5 | 7 | |
| much difference | 2 | 3 | |
| caffeine intake | every day | 2 | 5 |
| sometimes | 3 | 6 | |
| no intake | 6 | 2 | |
| Sleeping time | less than 3 h | 1 | 0 |
| 4–6 h | 4 | 2 | |
| 6–8 h | 5 | 6 | |
| A capsule | B capsule | |
|---|---|---|
| weight (g) | 1.02 | 1.47 |
| calorie (kcal) | 5.7 | 7.9 |
| protein (g) | 0.32 | 0.47 |
| lipid (g) | 0.36 | 0.49 |
| carbohydrate (g) | 0.3 | 0.4 |
| Na (mg) | <5 | 9.5 |
| βcarotene (μg) | 1800 | 2250 |
| Vitamine C (mg) | 50 | |
| Vitamine E (mg) | 27 | |
| Cu (mg) | 0.6 | |
| Zn (mg) | 9 | |
| BCA (mg) | 50 | 50 |
| lutein (mg) | 0.5 | 12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomisawa, T.; Nanashima, N.; Kitajima, M.; Mikami, K.; Takamagi, S.; Maeda, H.; Horie, K.; Lai, F.-c.; Osanai, T. Effects of Blackcurrant Anthocyanin on Endothelial Function and Peripheral Temperature in Young Smokers. Molecules 2019, 24, 4295. https://doi.org/10.3390/molecules24234295
Tomisawa T, Nanashima N, Kitajima M, Mikami K, Takamagi S, Maeda H, Horie K, Lai F-c, Osanai T. Effects of Blackcurrant Anthocyanin on Endothelial Function and Peripheral Temperature in Young Smokers. Molecules. 2019; 24(23):4295. https://doi.org/10.3390/molecules24234295
Chicago/Turabian StyleTomisawa, Toshiko, Naoki Nanashima, Maiko Kitajima, Kasumi Mikami, Shizuka Takamagi, Hayato Maeda, Kayo Horie, Fu-chih Lai, and Tomohiro Osanai. 2019. "Effects of Blackcurrant Anthocyanin on Endothelial Function and Peripheral Temperature in Young Smokers" Molecules 24, no. 23: 4295. https://doi.org/10.3390/molecules24234295