Insomnia and Information and Communication Technologies (ICT) in Elderly People: A Systematic Review


 , , and
, , and
Abstract
1. Introduction
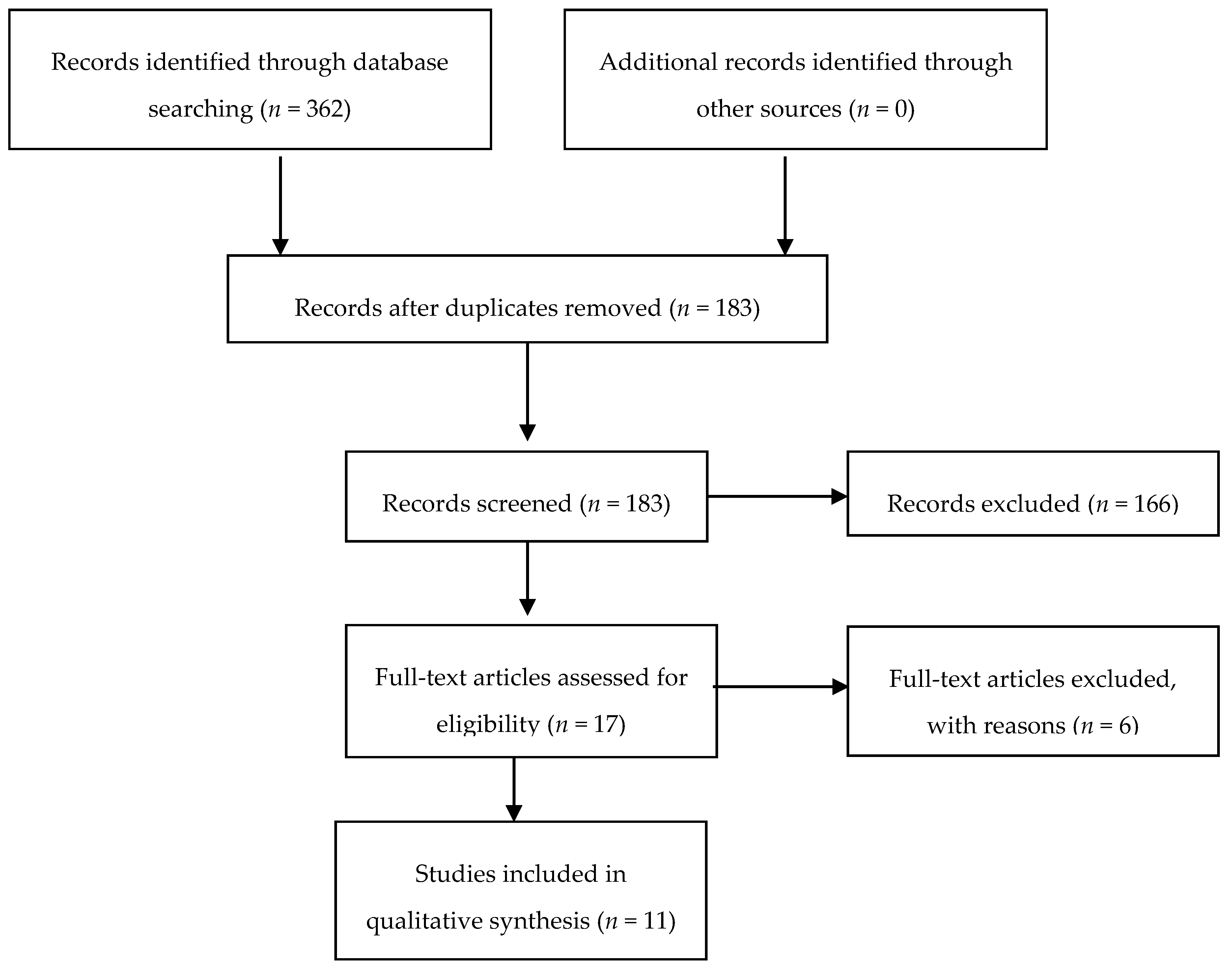
2. Material and Methods
- Internet delivered – CBTi;
- Virtual coaches; and
- Sleep technologies.
3. Results
3.1. Internet-Delivered CBTi
3.2. Virtual Coaches
3.3. Sleep Technologies
4. Conclusions
- (1)
- Focusing on demonstrating the effect of technological approach on sleep quality is important for future studies in this field.
- (2)
- Research efforts are needed to develop new technological tools with greater benefits to reduce insomnia and abnormal stress responses.
- (3)
- There is a need for assistance intended for caregivers and staff of residential facilities to promote better quality sleep at night (i.e., restrict time spent in bed, minimize daytime napping, provide opportunities for exposure to daylight and exercise).
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CBTi | Cognitive Behavioural Therapy for insomnia |
| CCBT-I | Computerized CBTi |
| CPAP | Continuous Positive Airway Pressure |
| ICT | Information and Communication Technologies |
| PSQI | Pittsburgh Sleep Quality Index |
| RCTs | Randomized controlled trials |
| SA | Sleep App |
| SD | Sleep Disorder |
| SE | sleep efficiency |
| SHUTi | Sleep Healthy Using the Internet |
| SL | Sleep latency |
| TI | Technologies Insomnia |
| TST | Total sleep time |
| WHO | World Health Organization |
References
- Foley, D.J.; Mojan, A.A.; Brown, S.L.; Simonsick, E.M.; Wallace, R.B.; Blazer, D.G. Sleep complaints among elderly persons: An epidemiologic study of three communities. Sleep 1995, 18, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Crowley, K. Sleep and sleep disorders in elderly people. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Vitello, M.V.; Moe, K.E.; Prinz, P.N. Sleep complaints cosegregate with illness in elderly people: Clinical research informed by and informing epidemiological studies of sleep. J. Psychosom. Res. 2002, 53, 555–559. [Google Scholar]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in elderly people: Results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.M.; Lee, K.A.; Bliwise, D.L.; Urizar, G.G.; Woodward, S.H.; King, A.C. Sleep patterns and sleep related factors between caregiving and non-caregiving women. Behav. Sleep Med. 2009, 7, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K. Daytime activity and risk factors for late-life insomnia. J. Sleep Res. 2003, 12, 231–238. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. State of the Science Conference Statement on manifestations and management of chronic insomnia in people. Nih Consens State. Sci. Statements 2005, 22, 1–30. [Google Scholar]
- Gureje, O.; Oladeji, B.D.; Abiona, T.; Makanjuola, V.; Esan, O. The natural history of insomnia in the Ibadan study of ageing. Sleep 2011, 34, 965–973. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stenholm, S.; Kronholm, E.; Sainio, P.; Borodulin, K.; Era, P.; Fogelholm, M.; Partonen, T.; Porkka-Heiskanen, T.; Koskinen, S. Sleep-related factors and mobility in elderly men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.P.; Covinsky, K.; Rebok, G.W.; Punjabi, N.M.; Stone, K.L.; Hillier, T.A.; Ensrud, K.E.; Yaffe, K. Poor sleep quality and functional decline in elderly women. J. Am. Geriatr. Soci. 2012, 60, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.A.; Coulouvrat, C.; Fitzgerald, T.; Hajak, G.; Roth, T.; Shahly, V.; Shillington, A.C.; Stephenson, J.J.; Walsh, J.K. Insomnia, comorbidity, and risk of injury among insured Americans: Results from the America Insomnia Survey. Sleep 2012, 35, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Roth, T.; Ancoli-Israel, S. Daytime consequences and correlates of insomnia in the United States: Results of the 1991 National Sleep Foundation Survey II. Sleep 1999, 22, S354–S358. [Google Scholar] [PubMed]
- Szelenberger, W.; Niemcewicz, S. Severity of insomnia correlates with cognitive impairment. Acta Neurobiol. Exp. (Wars) 2000, 60, 373. [Google Scholar] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Troxel, W.M.; Buysse, D.J.; Matthews, K.A.; Kip, K.E.; Strollo, P.J.; Hall, M.; Drumheller, O.; Reis, S.E. Sleep symptoms predict the development of the metabolic syndrome. Sleep 2010, 33, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.P.; Kaufmann, C.N.; Kasper, J.D.; Ohayon, M.M.; Rebok, G.W.; Skidmore, E.; Parisi, J.M.; Reynolds, C.F. Association between insomnia symptoms and functional status in U.S. elderly people. J Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, S35–S41. [Google Scholar] [CrossRef]
- Reynolds, C.F., III; Regestein, Q.; Nowell, P.D.; Neylan, T.C. Treatment of insomnia in the elderly. In Clinical Geriatric Psychopharmacology, 3rd ed.; Salzman, C., Ed.; Williams & Wilkins: Baltimore, MD, USA, 1998; pp. 395–416. [Google Scholar]
- Ancoli-Israel, S. Insomnia in the elderly: A review for the primary care practitioner. Sleep 2000, 23, S23–S30. [Google Scholar]
- Morin, C.M.; Colecchi, C.; Stone, J.; Sood, R.; Brink, D. Behavioural and pharmacological therapies for late-life insomnia: A randomized controlled trial. JAMA 1999, 281, 991–999. [Google Scholar] [CrossRef]
- Pitkala, K.H.; Strandberg, T.E.; Tilvis, R.S. Inappropriate drug prescribing in home-dwelling, elderly patients: A population-based survey. Arch Intern. Med. 2002, 162, 1707–1712. [Google Scholar] [CrossRef]
- Morin, C.M.; Culbert, J.P.; Schwartz, S.M. Nonpharmacological interventions for insomnia: A meta-analysis of treatment efficacy. Am. J. Psychiatry 1994, 151, 1172–1180. [Google Scholar]
- Sivertsen, B.; Omvik, S.; Pallesen, S.; Bjorvatn, B.; Havik, O.E.; Kvale, G.; Nielsen, G.H.; Nordhus, I.H. Cognitive behavioural therapy vs. zopiclone for treatment of chronic primary insomnia in elderly people: A randomized controlled trial. JAMA 2006, 295, 2851–2858. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, G.D.; Pace-Schott, E.F.; Stickgold, R.; Otto, M.W. Cognitive behaviour therapy and pharmacotherapy for insomnia: A randomized controlled trial and direct comparison. Arch Intern. Med. 2004, 164, 1888–1896. [Google Scholar] [CrossRef] [PubMed]
- Bootzin, R.R.; Epstein, D.; Wood, J.M. Stimulus control instructions. In Critical Issues in Psychiatry; Hauri, P.J., Ed.; Springer: Boston, MA, USA, 1991; pp. 19–28. [Google Scholar]
- Spielman, A.J.; Saskin, P.; Thorpy, M.J. Treatment of chronic insomnia by restriction of time in bed. Sleep 1987, 10, 45–56. [Google Scholar] [PubMed]
- Morin, C.M.; Hauri, P.J.; Espie, C.A.; Spielman, A.J.; Buysse, D.J.; Bootzin, R.R. Nonpharmacologic treatment of chronic insomnia: An American Academy of Sleep Medicine review. Sleep 1999, 22, 1134–1156. [Google Scholar] [CrossRef] [PubMed]
- Hauri, P.J. Sleep hygiene, relaxation therapy, and cognitive interventions. In Critical Issues in Psychiatry; Hauri, P.J., Ed.; Springer: Boston, MA, USA, 1991; pp. 65–84. [Google Scholar]
- McClusky, H.Y.; Milby, J.B.; Switzer, P.K.; Williams, V.; Wooten, V. Efficacy of behavioural versus triazolam treatment in persistent sleep-onset insomnia. Am. J. Psychiatry 1991, 148, 121–126. [Google Scholar] [PubMed]
- Smith, M.T.; Perlis, M.L.; Park, A.; Smith, M.S.; Pennington, J.; Giles, D.E.; Buysse, D.J. Comparative meta-analysis of pharmacotherapy and behaviour therapy for persistent insomnia. Am. J. Psychiatry 2002, 159, 5–11. [Google Scholar] [CrossRef]
- Kaynak, H.; Kaynak, D.; Gozukirmizi, E.; Guilleminault, C. The effects of trazodone on sleep in patients treated with stimulant antidepressants. Sleep Med. 2004, 5, 15–20. [Google Scholar] [CrossRef]
- Hauri, P.J. Can we mix behavioural therapy with hypnotics when treating insomniacs? Sleep 1997, 20, 1111–1118. [Google Scholar] [CrossRef][Green Version]
- Baillargeon, L.; Landreville, P.; Verreault, R.; Beauchemin, J.P.; Gregoire, J.P.; Morin, C.M. Discontinuation of benzodiazepines among elderly insomniac people treated with cognitive-behavioural therapy combined withgradual tapering: A randomized trial. CMAJ 2003, 169, 1015–1020. [Google Scholar]
- Morin, C.M.; Bastien, C.; Guay, B.; RadoucoThomas, M.; Leblanc, J.; Vallieres, A. Randomized clinical trial of supervised tapering and cognitive behaviour therapy to facilitate benzodiazepine discontinuation in elderly people with chronic insomnia. Am. J. Psychiatry 2004, 161, 332–342. [Google Scholar] [CrossRef]
- Chesson, A.L., Jr.; Anderson, W.M.; Littner, M.; Davila, D.; Hartse, K.; Johnson, S.; Wise, M.; Rafecas, J. Practice parameters for the nonpharmacologic treatment of chronic insomnia: An American Academy of Sleep Medicine report: Standards of Practice Committee of the American Academy of Sleep Medicine. Sleep 1999, 22, 1128–1133. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Silber, M.H. Chronic Insomnia. N. Engl. J. Med. 2005, 353, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Agarwal, S.; Jones, D.; Young, B.; Sutton, A. Synthesising qualitative and quantitative evidence: A review of possible methods. J. Health Serv. Res. Policy 2005, 10, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Hannes, K.; Macaitis, K. A move to more systematic and transparent approaches in qualitative evidence synthesis: Update on a review of published papers. Qual. Res. 2012, 12, 402–442. [Google Scholar] [CrossRef]
- Barnett-Page, E.; Thomas, J. Methods for the synthesis of qualitative research: A critical review. Bmc Med. Res. Methodol. 2009, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Info Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Andersson, G. The promise and pitfalls of the Internet for cognitive behavioural therapy. Bmc Med. 2010, 8, 82. [Google Scholar] [CrossRef]
- Ritterband, L.M.; Thorndike, F.P.; Gonder-Frederick, L.A.; Magee, J.C.; Bailey, E.T.; Saylor, D.K.; Morin, C.M. Efficacy of an Internet-based behavioural intervention for people with insomnia. Arch Gen. Psychiatry 2009, 66, 692–698. [Google Scholar] [CrossRef]
- Thorndike, F.P.; Saylor, D.K.; Bailey, E.T.; Gonder-Frederick, L.; Morin, C.M.; Ritterband, L.M. Development and perceived utility and impact of an Internet intervention for insomnia. E. J. Appl. Psychol. 2008, 4, 32–42. [Google Scholar] [CrossRef]
- Ritterband, L. An Internet intervention for insomnia: Efficacy and dissemination. Project Information. US Department of Health and Human Services. Available online: http://projectreporter.nih.gov/project_info_description.cfm?aid=7887402&icde=6416813. (accessed on 15 December 2010).
- Morin, C.M.; Bootzin, R.R.; Buysse, D.J.; Edinger, J.D.; Espie, C.A.; Lichstein, K.L. Psychological and behavioural treatment of insomnia: Update of the recent evidence (1998–2004). Sleep 2006, 29, 1398–1414. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.D.; Gehrman, P.; Perlis, M.; Umscheid, C.A. Comparative effectiveness of cognitive behavioural therapy for insomnia: A systematic review. Bmc. Fam. Pr. 2012, 25, 40. [Google Scholar]
- Belleville, G.; Cousineau, H.; Levrier, K.; St-Pierre-Delorme, M.È. Meta-analytic review of the impact of cognitive behavioural therapy for insomnia on concomitant anxiety. Clin. Psychol. Rev. 2011, 31, 638–652. [Google Scholar] [CrossRef] [PubMed]
- Kapella, M.C.; Herdegen, J.J.; Perlis, M.L.; Shaver, J.L.; Larson, J.L.; Law, J.A.; Carley, D.W. Cognitive behavioural therapy for insomnia comorbid with COPD is feasible with preliminary evidence of positive sleep and fatigue effects. Int. J. Chron. Obs. Pulmon Dis. 2011, 6, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Pigeon, W.R.; Moynihan, J.; Matteson-Rusby, S.; Jungquist, C.R.; Xia, Y.; Tu, X.; Perlis, M.L. Comparative effectiveness of CBT interventions for co-morbid chronic pain & insomnia: A pilot study. Behav. Res. 2012, 50, 685–689. [Google Scholar]
- Anderson, K.N.; Goldsmith, P.; Gardiner, A. A pilot evaluation of an online cognitive behavioral therapy for insomnia disorder – targeted screening and interactive Web design lead to improved sleep in a community population. Nat. Sci. Sleep. 2014, 6, 43–49. [Google Scholar] [CrossRef]
- Espie, C.A.; Kyle, S.D.; Williams, C.; Ong, J.C.; Douglas, N.J.; Hames, P.; Brown, J.S.L. A randomized, placebo-controlled trial of online cognitive behavioural therapy for chronic insomnia disorder delivered via an automated media-rich web application. Sleep 2012, 35, 769–781. [Google Scholar] [CrossRef]
- Cheng, S.K.; Dizon, J. Computerised cognitive behavioural therapy for insomnia: A systematic review and meta-analysis. Psychother Psychosom 2012, 81, 206–216. [Google Scholar] [CrossRef]
- Ström, L.; Pettersson, R.; Andersson, G. Internet-based treatment for insomnia: A controlled evaluation. J. Consult Clin. Psychol. 2004, 72, 113–120. [Google Scholar] [CrossRef]
- Lancee, J.; van den Bout, J.; van Straten, A.; Spoormaker, V.I. Internet delivered or mailed self help treatment for insomnia?: A randomized waiting-list controlled trial. Behav. Res. 2012, 50, 22–29. [Google Scholar] [CrossRef]
- Ritterband, L.M.; Bailey, E.T.; Thorndike, F.P.; Lord, H.R.; Farrell-Carnahan, L.; Baum, L.D. Initial evaluation of an Internet intervention to improve the sleep of cancer survivors with insomnia. Psychooncology 2012, 21, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Morin, C.M.; Beaulieu-Bonneau, S.; LeBlanc, M.; Savard, J. Self-help treatment for insomnia: A randomized controlled trial. Sleep 2005, 28, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Beun, R.J. Persuasive strategies in mobile insomnia therapy: Alignment, adaptation, and motivational support. Pers Ubiquit. Comput. 2012, 17, 1187–1195. [Google Scholar] [CrossRef]
- Donkin, L.; Christensen, H.; Naismith, S.L.; Neal, B.; Hickie, I.B.; Glozier, N. A systematic review of the impact of adherence on the effectiveness of e-therapies. J. Med. Int. Res. 2011, 13, e52. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. The law of attrition. J. Med. Int. Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- World Health Organization Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization 2003 URL. Available online: http://apps.who.int/iris/bitstream/10665/42682/1/9241545992.pdf (accessed on 30 August 2015).
- Beun, R.; Griffioen-Both, F.; Ahn, R.; Fitrianie, S.; Lancee, J. Modeling interaction in automated e-coaching: A case from insomnia therapy. In Proceedings of the Sixth International Conference on Advanced Cognitive Technologies and Applications, Venice, Italy, 25 May–9 June 2014. [Google Scholar]
- Horsch, C.; Brinkman, W.; van Eijk, R.; Neerincx, M. Towards the usage of persuasive strategies in a virtual sleep coach. In Proceedings of the UK HCI 2012 Workshop on People, Computers & Psychotherapy, Birmingham, UK, 10 September 2012. [Google Scholar]
- Baylor, A.; Ebbers, S. The pedagogical agent split-persona effect: When two agents are better than one. In Proceedings of the World Conference on Educational Media and Technology, Waynesville, NC, USA, 2003; pp. 459–462. [Google Scholar]
- Horsch, C.; Lancee, J.; Beun, R.J.; Neerincx, M.A.; Brinkman, W.P. Adherence to Technology-Mediated Insomnia Treatment: A Meta-Analysis, Interviews, and Focus Groups. J. Med. Int. Res. 2015, 17, e214. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.; Elbaz, M.; Piednoir, B.; Carron, A.; Texereau, J. Evaluation of the add-on NOWAPI® medical device for remote monitoring of compliance to Continuous Positive Airway Pressure and treatment efficacy in obstructive sleep apnea. Biomed. Eng. Online 2016, 15, 26. [Google Scholar] [CrossRef] [PubMed]
- Ko, P.T.; Kientz, J.A.; Choe, E.K.; Kay, M.; Landis, C.A.; Watson, N.F. Consumer Sleep Technologies: A Review of the Landscape. J. Clin. Sleep Med. 2015, 22, 1455–1461. [Google Scholar] [CrossRef]


{kind=link}
| Studies | Methods | Outcomes |
|---|---|---|
| Ström L et al., 2004 | IBTi | Improve total sleep time, total wake time in bed and sleep efficiency |
| Morin CM V et al., 2005 | SHTi | Significant but modest improvements were obtained on subjective sleep parameters |
| Thorndike FP et al., 2008 | SHUTi | Improve sleep, sleep efficiency and overall quality of life |
| Ritterband LM et al., 2009 | IBBI | Considerable potential in delivering a structured behavioural program for insomnia |
| Kapella MC et al., 2011 | CBTi | Significant positive effects were noted in people with COPD for insomnia severity, global sleep quality, wake after sleep onset, sleep efficiency, fatigue, beliefs, attitudes about sleep and depressed mood |
| Pigeon WR et al., 2012 | CBTp + CBTi | Improve sleep, disability from pain, depression and fatigue |
| Lancee J et al., 2012 | EPPC | EPPC were superior compared to the waiting-list condition on most daily sleep measures, global insomnia symptoms, depression and anxiety symptoms |
| Espie CA et al., 2012 | Web-based CBT | Improve the sleep and associated daytime functioning of adults with insomnia disorder |
| Beun RJ et al., 2014 | Sleepcare project | Improve the individual’s adherence to exercises for insomnia therapy |
| Ko PT et al., 2015 | CST | Facilitation of sleep induction or wakening, self-guided sleep assessment, entertainment, social connection, information sharing and sleep education |
| Leger et al., 2016 | NOWAPI® | Monitor duration of CPAP which improves the quality of sleep. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvemini, A.; D’Onofrio, G.; Ciccone, F.; Greco, A.; Tullio, A.; Addante, F.; Sancarlo, D.; Vendemiale, G.; Serviddio, G.; Ricciardi, F.; et al. Insomnia and Information and Communication Technologies (ICT) in Elderly People: A Systematic Review. Med. Sci. 2019, 7, 70. https://doi.org/10.3390/medsci7060070
Salvemini A, D’Onofrio G, Ciccone F, Greco A, Tullio A, Addante F, Sancarlo D, Vendemiale G, Serviddio G, Ricciardi F, et al. Insomnia and Information and Communication Technologies (ICT) in Elderly People: A Systematic Review. Medical Sciences. 2019; 7(6):70. https://doi.org/10.3390/medsci7060070
Chicago/Turabian StyleSalvemini, Arianna, Grazia D’Onofrio, Filomena Ciccone, Antonella Greco, Anita Tullio, Filomena Addante, Daniele Sancarlo, Gianluigi Vendemiale, Gaetano Serviddio, Francesco Ricciardi, and et al. 2019. "Insomnia and Information and Communication Technologies (ICT) in Elderly People: A Systematic Review" Medical Sciences 7, no. 6: 70. https://doi.org/10.3390/medsci7060070
APA StyleSalvemini, A., D’Onofrio, G., Ciccone, F., Greco, A., Tullio, A., Addante, F., Sancarlo, D., Vendemiale, G., Serviddio, G., Ricciardi, F., Giuliani, F., & Greco, A. (2019). Insomnia and Information and Communication Technologies (ICT) in Elderly People: A Systematic Review. Medical Sciences, 7(6), 70. https://doi.org/10.3390/medsci7060070