The Coming Age of Flavonoids in the Treatment of Diabetic Complications

 , , , and
, , , and
Abstract
:1. Introduction
2. Pathogenesis of Diabetic Complications
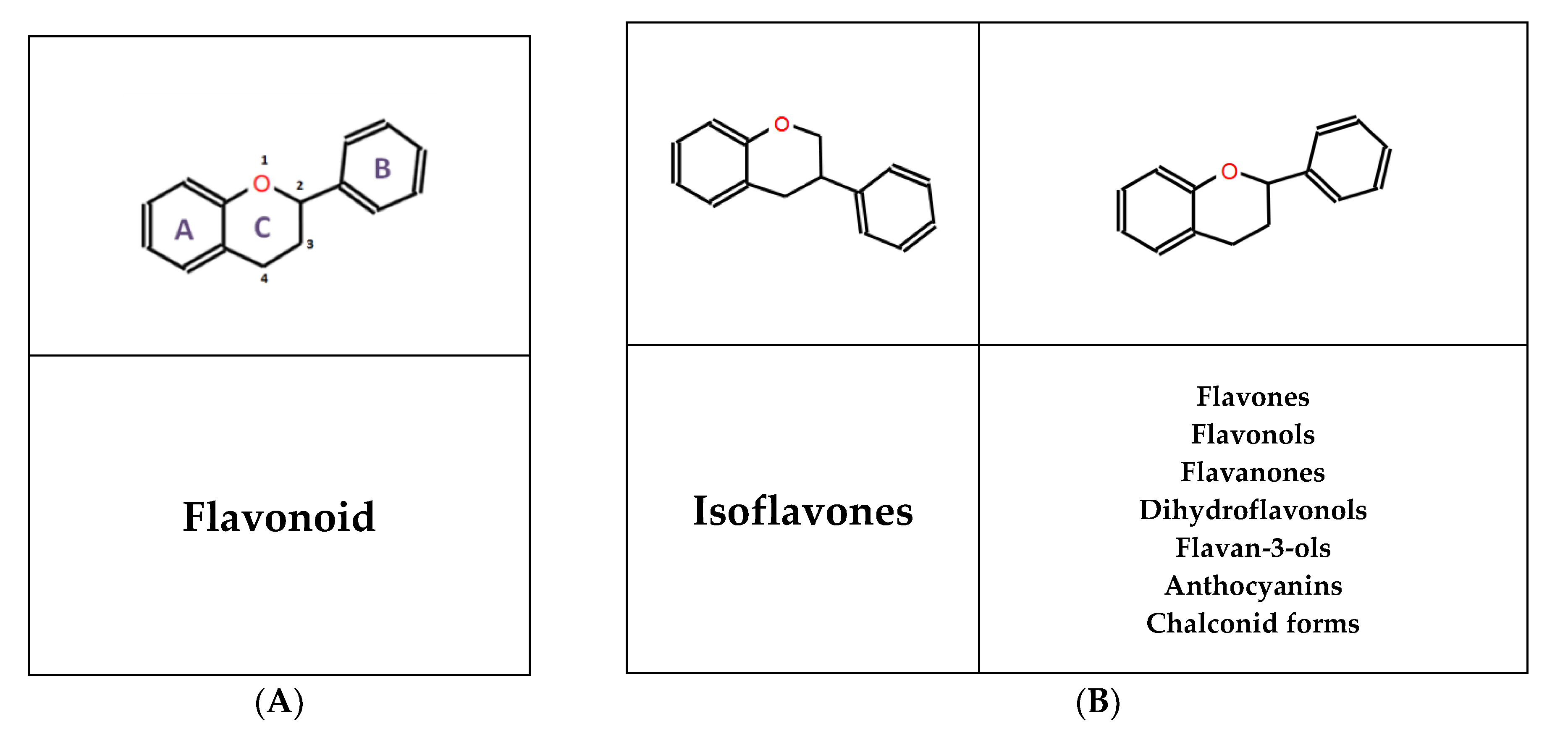
3. General Aspects of Flavonoids
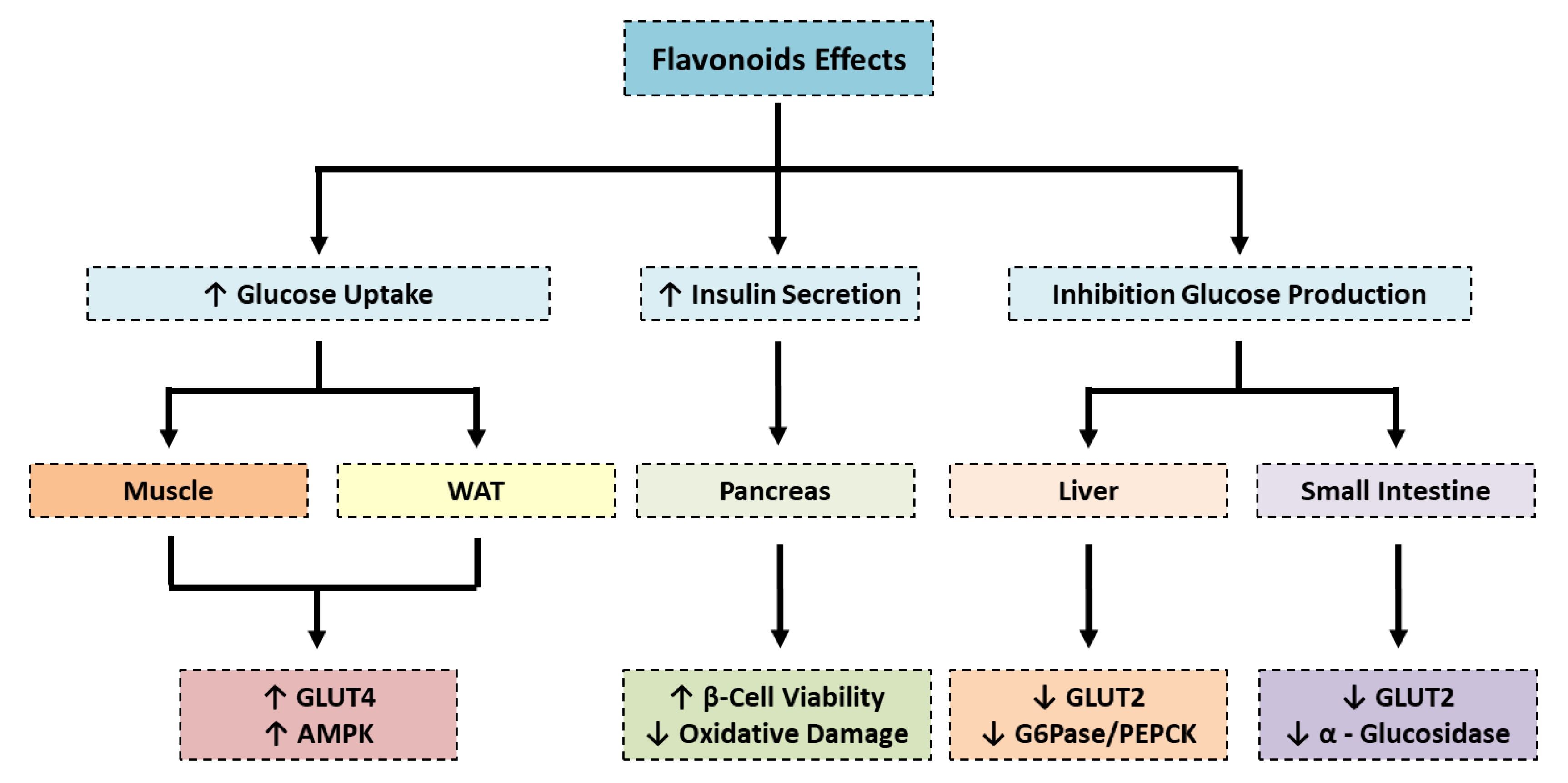
4. Recent Preclinical Advances in the Anti-Diabetic Actions of Flavonoids
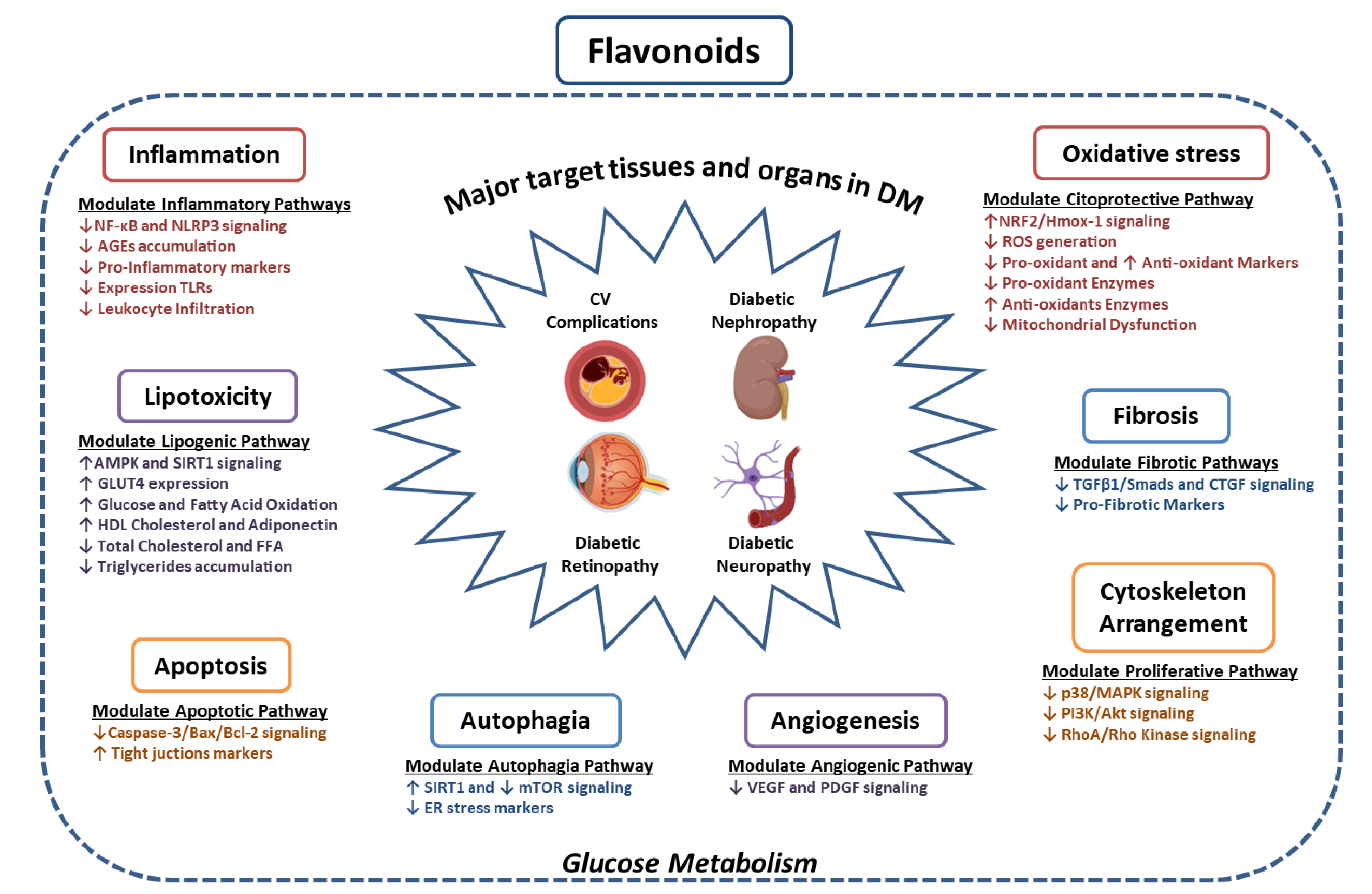
5. Current Status of Experimental Research on Flavonoids in Chronic Complications of Diabetes
5.1. Diabetic Nephropathy
5.2. Diabetic Retinopathy
5.3. Diabetic Neuropathy
5.4. Diabetic Macrovascular Complications
6. Clinical Studies on Flavonoids in Diabetes
6.1. Diabetic Nephropathy
6.2. Diabetic Retinopathy
6.3. Diabetic Neuropathy
6.4. Cardiovascular Complications
7. Ongoing Clinical Trials
8. Toxicity and Adverse Effects of Flavonoids
9. Future Perspectives and Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- International Diabetes Federation. Eighth Edition. Lancet 2017, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global estimates of undiagnosed diabetes in adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef]
- Currie, C.J.; Poole, C.D.; Evans, M.; Peters, J.R.; Morgan, C.L. Mortality and other important diabetes-related outcomes with insulin vs other antihyperglycemic therapies in type 2 diabetes. J. Clin. Endocrinol. Metab. 2013, 98, 668–677. [Google Scholar] [CrossRef]
- Dall, T.M.; Yang, W.; Gillespie, K.; Mocarski, M.; Byrne, E.; Cintina, I.; Beronja, K.; Semilla, A.P.; Iacobucci, W.; Hogan, P.F. The Economic Burden of Elevated Blood Glucose Levels in 2017: Diagnosed and Undiagnosed Diabetes, Gestational Diabetes Mellitus, and Prediabetes. Diabetes Care 2019, 42, 1661–1668. [Google Scholar] [CrossRef] [Green Version]
- Fioretto, P.; Bruseghin, M.; Berto, I.; Gallina, P.; Manzato, E.; Mussap, M. Renal protection in diabetes: role of glycemic control. J. Am. Soc. Nephrol. JASN 2006, 17, S86–S89. [Google Scholar] [CrossRef] [Green Version]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Gregg, E.W.; Li, Y.; Wang, J.; Burrows, N.R.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in diabetes-related complications in the United States, 1990-2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Kern, M.; Kloting, N.; Mark, M.; Mayoux, E.; Klein, T.; Bluher, M. The SGLT2 inhibitor empagliflozin improves insulin sensitivity in db/db mice both as monotherapy and in combination with linagliptin. Metab. Clin. Exp. 2016, 65, 114–123. [Google Scholar] [CrossRef]
- Gnudi, L.; Coward, R.J.M.; Long, D.A. Diabetic Nephropathy: Perspective on Novel Molecular Mechanisms. Trends Endocrinol. Metab. TEM 2016, 27, 820–830. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Sugiura, Y.; Saito, H.; Sugahara, M.; Higashijima, Y.; Yamaguchi, J.; Inagi, R.; Suematsu, M.; Nangaku, M.; Tanaka, T. Sodium-glucose cotransporter 2 inhibition normalizes glucose metabolism and suppresses oxidative stress in the kidneys of diabetic mice. Kidney Int. 2018, 94, 912–925. [Google Scholar] [CrossRef]
- Nolen-Doerr, E.; Stockman, M.C.; Rizo, I. Mechanism of Glucagon-Like Peptide 1 Improvements in Type 2 Diabetes Mellitus and Obesity. Curr. Obes. Rep. 2019, 8, 284–291. [Google Scholar] [CrossRef]
- Sedeek, M.; Montezano, A.C.; Hebert, R.L.; Gray, S.P.; Di Marco, E.; Jha, J.C.; Cooper, M.E.; Jandeleit-Dahm, K.; Schiffrin, E.L.; Wilkinson-Berka, J.L.; et al. Oxidative stress, Nox isoforms and complications of diabetes--potential targets for novel therapies. J. Cardiovasc. Transl. Res. 2012, 5, 509–518. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef]
- Barrett, E.J.; Liu, Z.; Khamaisi, M.; King, G.L.; Klein, R.; Klein, B.E.K.; Hughes, T.M.; Craft, S.; Freedman, B.I.; Bowden, D.W.; et al. Diabetic Microvascular Disease: An Endocrine Society Scientific Statement. J. Clin. Endocrinol. Metab. 2017, 102, 4343–4410. [Google Scholar] [CrossRef]
- Fowler, M.J. Microvascular and macrovascular complications of diabetes. Clin. Diabetes. 2011, 29, 116–122. [Google Scholar] [CrossRef] [Green Version]
- IDF Diabetes Atlas, 9th edition 2019. Available online: https://www.diabetesatlas.org (accessed on 3 February 2020).
- Cerf, M.E. Beta cell dysfunction and insulin resistance. Front. Endocrinol. 2013, 4, 37. [Google Scholar] [CrossRef] [Green Version]
- Sandholm, N.; Salem, R.M.; McKnight, A.J.; Brennan, E.P.; Forsblom, C.; Isakova, T.; McKay, G.J.; Williams, W.W.; Sadlier, D.M.; Makinen, V.P.; et al. New susceptibility loci associated with kidney disease in type 1 diabetes. PLoS Genetics 2012, 8, e1002921. [Google Scholar] [CrossRef] [Green Version]
- Ahlqvist, E.; van Zuydam, N.R.; Groop, L.C.; McCarthy, M.I. The genetics of diabetic complications. Nat. Rev. Nephrol. 2015, 11, 277–287. [Google Scholar] [CrossRef]
- Mueller, P.W.; Rogus, J.J.; Cleary, P.A.; Zhao, Y.; Smiles, A.M.; Steffes, M.W.; Bucksa, J.; Gibson, T.B.; Cordovado, S.K.; Krolewski, A.S.; et al. Genetics of Kidneys in Diabetes (GoKinD) study: a genetics collection available for identifying genetic susceptibility factors for diabetic nephropathy in type 1 diabetes. J. Am. Soc. Nephrol. JASN 2006, 17, 1782–1790. [Google Scholar] [CrossRef]
- Chang, Y.C.; Chang, E.Y.; Chuang, L.M. Recent progress in the genetics of diabetic microvascular complications. World J. Diabetes 2015, 6, 715–725. [Google Scholar] [CrossRef]
- Van Zuydam, N.R.; Ahlqvist, E.; Sandholm, N.; Deshmukh, H.; Rayner, N.W.; Abdalla, M.; Ladenvall, C.; Ziemek, D.; Fauman, E.; Robertson, N.R.; et al. A Genome-Wide Association Study of Diabetic Kidney Disease in Subjects With Type 2 Diabetes. Diabetes 2018, 67, 1414–1427. [Google Scholar] [CrossRef] [Green Version]
- Anders, H.J.; Huber, T.B.; Isermann, B.; Schiffer, M. CKD in diabetes: diabetic kidney disease versus nondiabetic kidney disease. Nat.Rev. Nephrol. 2018, 14, 361–377. [Google Scholar] [CrossRef]
- Obrosova, I.G.; Kador, P.F. Aldose reductase / polyol inhibitors for diabetic retinopathy. Curr. Pharm. Biotechnol. 2011, 12, 373–385. [Google Scholar] [CrossRef]
- Jenkins, A.J.; Joglekar, M.V.; Hardikar, A.A.; Keech, A.C.; O’Neal, D.N.; Januszewski, A.S. Biomarkers in Diabetic Retinopathy. Rev. Diabetic Stud. RDS 2015, 12, 159–195. [Google Scholar] [CrossRef] [Green Version]
- Veron, D.; Reidy, K.J.; Bertuccio, C.; Teichman, J.; Villegas, G.; Jimenez, J.; Shen, W.; Kopp, J.B.; Thomas, D.B.; Tufro, A. Overexpression of VEGF-A in podocytes of adult mice causes glomerular disease. Kidney Int. 2010, 77, 989–999. [Google Scholar] [CrossRef] [Green Version]
- Zoja, C.; Benigni, A.; Remuzzi, G. The Nrf2 pathway in the progression of renal disease. Nephrol. Dial. Transpl. Off. Pub. Eur. Dial. Transpl. Assoc. Eur. Renal Assoc. 2014, 29 (Suppl. 1), i19–i24. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.M.; de Haan, J.B. Combating oxidative stress in diabetic complications with Nrf2 activators: how much is too much? Redox Rep. Commun. Free Radic. Res. 2014, 19, 107–117. [Google Scholar] [CrossRef]
- Uruno, A.; Yagishita, Y.; Yamamoto, M. The Keap1-Nrf2 system and diabetes mellitus. Arch. Biochem. Biophys. 2015, 566, 76–84. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Harris, R.C. Renal endothelial dysfunction in diabetic nephropathy. Cardiovasc. Hematol. Disord. Drug Targ. 2014, 14, 22–33. [Google Scholar] [CrossRef] [Green Version]
- Capellini, V.K.; Celotto, A.C.; Baldo, C.F.; Olivon, V.C.; Viaro, F.; Rodrigues, A.J.; Evora, P.R. Diabetes and vascular disease: basic concepts of nitric oxide physiology, endothelial dysfunction, oxidative stress and therapeutic possibilities. Curr. Vasc. Pharm. 2010, 8, 526–544. [Google Scholar] [CrossRef] [PubMed]
- Santiago, A.R.; Boia, R.; Aires, I.D.; Ambrosio, A.F.; Fernandes, R. Sweet Stress: Coping With Vascular Dysfunction in Diabetic Retinopathy. Front. Physiol. 2018, 9, 820. [Google Scholar] [CrossRef] [PubMed]
- Lindblom, R.; Higgins, G.; Coughlan, M.; de Haan, J.B. Targeting Mitochondria and Reactive Oxygen Species-Driven Pathogenesis in Diabetic Nephropathy. Rev. Diabetic Stud. RDS 2015, 12, 134–156. [Google Scholar] [CrossRef] [Green Version]
- Miranda-Diaz, A.G.; Pazarin-Villasenor, L.; Yanowsky-Escatell, F.G.; Andrade-Sierra, J. Oxidative Stress in Diabetic Nephropathy with Early Chronic Kidney Disease. J. Diabetes Res. 2016, 2016, 7047238. [Google Scholar] [CrossRef] [Green Version]
- Santilli, F.; Cipollone, F.; Mezzetti, A.; Chiarelli, F. The role of nitric oxide in the development of diabetic angiopathy. Hormone and Metabolic Research = Hormon- und Stoffwechselforschung = Hormones et metabolisme 2004, 36, 319–335. [Google Scholar] [CrossRef]
- Shikata, K.; Makino, H. Microinflammation in the pathogenesis of diabetic nephropathy. J. Diabetes Invest. 2013, 4, 142–149. [Google Scholar] [CrossRef] [Green Version]
- Moreno, J.A.; Gomez-Guerrero, C.; Mas, S.; Sanz, A.B.; Lorenzo, O.; Ruiz-Ortega, M.; Opazo, L.; Mezzano, S.; Egido, J. Targeting inflammation in diabetic nephropathy: a tale of hope. Expert Opin. Invest. Drugs 2018, 27, 917–930. [Google Scholar] [CrossRef]
- Tesch, G.H. Diabetic nephropathy—Is this an immune disorder? Clin. Sci. 2017, 131, 2183–2199. [Google Scholar] [CrossRef]
- Qiu, A.W.; Liu, Q.H.; Wang, J.L. Blocking IL-17A Alleviates Diabetic Retinopathy in Rodents. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2017, 41, 960–972. [Google Scholar] [CrossRef]
- Garibotto, G.; Carta, A.; Picciotto, D.; Viazzi, F.; Verzola, D. Toll-like receptor-4 signaling mediates inflammation and tissue injury in diabetic nephropathy. J. Nephrol. 2017, 30, 719–727. [Google Scholar] [CrossRef]
- Elmarakby, A.A.; Sullivan, J.C. Relationship between oxidative stress and inflammatory cytokines in diabetic nephropathy. Cardiovasc. Ther. 2012, 30, 49–59. [Google Scholar] [CrossRef]
- Vinayagam, R.; Xu, B. Antidiabetic properties of dietary flavonoids: a cellular mechanism review. Nutr. Metab. 2015, 12, 60. [Google Scholar] [CrossRef] [Green Version]
- Santos-Buelga, C.; Feliciano, A.S. Flavonoids: From Structure to Health Issues. Molecules 2017, 22. [Google Scholar] [CrossRef]
- Testa, R.; Bonfigli, A.R.; Genovese, S.; De Nigris, V.; Ceriello, A. The Possible Role of Flavonoids in the Prevention of Diabetic Complications. Nutrients 2016, 8. [Google Scholar] [CrossRef]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: an overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Wang, J.; Zhao, H.; Luo, Y. Effects of three flavonoids from an ancient traditional Chinese medicine Radix puerariae on geriatric diseases. Brain Circ. 2018, 4, 174–184. [Google Scholar] [CrossRef]
- CIMA. Available online: https://cima.aemps.es (accessed on 24 May 2019).
- Al-Ishaq, R.K.; Abotaleb, M.; Kubatka, P.; Kajo, K.; Busselberg, D. Flavonoids and Their Anti-Diabetic Effects: Cellular Mechanisms and Effects to Improve Blood Sugar Levels. Biomolecules 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Burton-Freeman, B.; Brzezinski, M.; Park, E.; Sandhu, A.; Xiao, D.; Edirisinghe, I. A Selective Role of Dietary Anthocyanins and Flavan-3-ols in Reducing the Risk of Type 2 Diabetes Mellitus: A Review of Recent Evidence. Nutrients 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Ghorbani, A.; Rashidi, R.; Shafiee-Nick, R. Flavonoids for preserving pancreatic beta cell survival and function: A mechanistic review. Biomedicine Pharmacotherapy = Biomedecine & pharmacotherapie 2019, 111, 947–957. [Google Scholar] [CrossRef]
- Alkhalidy, H.; Wang, Y.; Liu, D. Dietary Flavonoids in the Prevention of T2D: An Overview. Nutrients 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Eid, H.M.; Haddad, P.S. The Antidiabetic Potential of Quercetin: Underlying Mechanisms. Curr. Med. Chem. 2017, 24, 355–364. [Google Scholar] [CrossRef]
- Prasad, C.N.; Anjana, T.; Banerji, A.; Gopalakrishnapillai, A. Gallic acid induces GLUT4 translocation and glucose uptake activity in 3T3-L1 cells. FEBS letters 2010, 584, 531–536. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, Y.; Kishida, H.; Nakagawa, K.; Yoshioka, Y.; Ashida, H. Liquorice flavonoid oil suppresses hyperglycaemia accompanied by skeletal muscle myocellular GLUT4 recruitment to the plasma membrane in KK-A(y) mice. Int. J. Food Sci. Nutr. 2019, 70, 294–302. [Google Scholar] [CrossRef]
- Wang, T.; Jiang, H.; Cao, S.; Chen, Q.; Cui, M.; Wang, Z.; Li, D.; Zhou, J.; Wang, T.; Qiu, F.; et al. Baicalin and its metabolites suppresses gluconeogenesis through activation of AMPK or AKT in insulin resistant HepG-2 cells. Eur. J. Med. Chem. 2017, 141, 92–100. [Google Scholar] [CrossRef]
- Li, X.; Chen, Y.; Shen, J.Z.; Pan, Q.; Yang, W.; Yan, H.; Liu, H.; Ai, W.; Liao, W.; Guo, S. Epigallocatechin Gallate Inhibits Hepatic Glucose Production in Primary Hepatocytes via Downregulating PKA Signaling Pathways and Transcriptional Factor FoxO1. J. Agricult. Food Chem. 2019, 67, 3651–3661. [Google Scholar] [CrossRef]
- Yadollah, S.; Kazemipour, N.; Bakhtiyari, S.; Nazifi, S. Palmitate-induced insulin resistance is attenuated by Pioglitazone and EGCG through reducing the gluconeogenic key enzymes expression in HepG2 cells. J. Med. Life 2017, 10, 244–249. [Google Scholar]
- Lima-Fontes, M.; Costa, R.; Rodrigues, I.; Soares, R. Xanthohumol Restores Hepatic Glucolipid Metabolism Balance in Type 1 Diabetic Wistar Rats. J. Agricult. Food Chem. 2017, 65, 7433–7439. [Google Scholar] [CrossRef]
- Alzaid, F.; Cheung, H.M.; Preedy, V.R.; Sharp, P.A. Regulation of glucose transporter expression in human intestinal Caco-2 cells following exposure to an anthocyanin-rich berry extract. PLoS ONE 2013, 8, e78932. [Google Scholar] [CrossRef] [Green Version]
- Kwon, O.; Eck, P.; Chen, S.; Corpe, C.P.; Lee, J.H.; Kruhlak, M.; Levine, M. Inhibition of the intestinal glucose transporter GLUT2 by flavonoids. FASEB J. 2007, 21, 366–377. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Jo, S.H.; Kwon, Y.I.; Hwang, J.K. Effects of onion (Allium cepa L.) extract administration on intestinal alpha-glucosidases activities and spikes in postprandial blood glucose levels in SD rats model. Int. J. Mol. Sci. 2011, 12, 3757–3769. [Google Scholar] [CrossRef] [Green Version]
- Jayachandran, M.; Vinayagam, R.; Ambati, R.R.; Xu, B.; Chung, S.S.M. Guava Leaf Extract Diminishes Hyperglycemia and Oxidative Stress, Prevents beta-Cell Death, Inhibits Inflammation, and Regulates NF-kB Signaling Pathway in STZ Induced Diabetic Rats. BioMed Res. Int. 2018, 2018, 4601649. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.J.; Kim, J.H.; Pan, J.H.; Kim, J.K.; Park, T.S.; Kim, Y.J.; Lee, J.H.; Kim, J.H. Naringin Protects Pancreatic beta-Cells Against Oxidative Stress-Induced Apoptosis by Inhibiting Both Intrinsic and Extrinsic Pathways in Insulin-Deficient Diabetic Mice. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef]
- Wang, L.P.; Gao, Y.Z.; Song, B.; Yu, G.; Chen, H.; Zhang, Z.W.; Yan, C.F.; Pan, Y.L.; Yu, X.Y. MicroRNAs in the Progress of Diabetic Nephropathy: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. eCAM 2019, 2019, 3513179. [Google Scholar] [CrossRef]
- Pichler, R.; Afkarian, M.; Dieter, B.P.; Tuttle, K.R. Immunity and inflammation in diabetic kidney disease: translating mechanisms to biomarkers and treatment targets. Am. J. Physiol. Renal Physiol. 2017, 312, F716–F731. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Liu, J.; Zhou, Z.; Liu, K.; Liu, C. Diosmetin Attenuates Akt Signaling Pathway by Modulating Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells (NF-kappaB)/Inducible Nitric Oxide Synthase (iNOS) in Streptozotocin (STZ)-Induced Diabetic Nephropathy Mice. Med. Sci. Monitor Int. Med. J. Exp. Clin. Res. 2018, 24, 7007–7014. [Google Scholar] [CrossRef]
- Liu, X.L.; Liu, W.P.; Wang, L.L.; Feng, L. Effects of flavonoids from Pyrrosiae folium on pathological changes and inflammatory response of diabetic nephropathy. Zhongguo Zhong yao za zhi = Zhongguo zhongyao zazhi = China J. Chin. Mater. Med. 2018, 43, 2352–2357. [Google Scholar] [CrossRef]
- Wang, K.J.; Zhao, J.L. Corn silk (Zea mays L.), a source of natural antioxidants with alpha-amylase, alpha-glucosidase, advanced glycation and diabetic nephropathy inhibitory activities. Biomed. Pharmacother. Biomed. Pharmacother. 2019, 110, 510–517. [Google Scholar] [CrossRef]
- Zhu, X.; Shi, J.; Li, H. Liquiritigenin attenuates high glucose-induced mesangial matrix accumulation, oxidative stress, and inflammation by suppression of the NF-kappaB and NLRP3 inflammasome pathways. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 106, 976–982. [Google Scholar] [CrossRef]
- Chen, F.; Wei, G.; Xu, J.; Ma, X.; Wang, Q. Naringin ameliorates the high glucose-induced rat mesangial cell inflammatory reaction by modulating the NLRP3 Inflammasome. BMC Complement. Altern. Med. 2018, 18, 192. [Google Scholar] [CrossRef]
- Kashihara, N.; Haruna, Y.; Kondeti, V.K.; Kanwar, Y.S. Oxidative stress in diabetic nephropathy. Curr. Med. Chem. 2010, 17, 4256–4269. [Google Scholar] [CrossRef] [Green Version]
- Bloch-Damti, A.; Bashan, N. Proposed mechanisms for the induction of insulin resistance by oxidative stress. Antioxid. Redox Signal. 2005, 7, 1553–1567. [Google Scholar] [CrossRef]
- Oza, M.J.; Kulkarni, Y.A. Formononetin attenuates kidney damage in type 2 diabetic rats. Life Sci. 2019, 219, 109–121. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, S.; Li, H.; Chen, F.; Shi, J. Naringin ameliorates diabetic nephropathy by inhibiting NADPH oxidase 4. Eur. J. Pharm. 2017, 804, 1–6. [Google Scholar] [CrossRef]
- Jiang, W.; Wang, R.; Liu, D.; Zuo, M.; Zhao, C.; Zhang, T.; Li, W. Protective Effects of Kaempferitrin on Advanced Glycation End Products Induce Mesangial Cell Apoptosis and Oxidative Stress. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef] [Green Version]
- Fukami, K.; Yamagishi, S.; Ueda, S.; Okuda, S. Role of AGEs in diabetic nephropathy. Curr. Pharm. Des. 2008, 14, 946–952. [Google Scholar] [CrossRef]
- Lee, E.J.; Kang, M.K.; Kim, D.Y.; Kim, Y.H.; Oh, H.; Kang, Y.H. Chrysin Inhibits Advanced Glycation End Products-Induced Kidney Fibrosis in Renal Mesangial Cells and Diabetic Kidneys. Nutrients 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Al-Hussaini, H.; Kilarkaje, N. Trans-resveratrol mitigates type 1 diabetes-induced oxidative DNA damage and accumulation of advanced glycation end products in glomeruli and tubules of rat kidneys. Toxicol. Appl. Pharm. 2018, 339, 97–109. [Google Scholar] [CrossRef]
- Semeraro, F.; Morescalchi, F.; Cancarini, A.; Russo, A.; Rezzola, S.; Costagliola, C. Diabetic retinopathy, a vascular and inflammatory disease: Therapeutic implications. Diabetes Metab. 2019. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, Y.; Jin, W.; Xing, Y.; Yang, A. Catechin Weakens Diabetic Retinopathy by Inhibiting the Expression of NF-kappaB Signaling Pathway-Mediated Inflammatory Factors. Ann. Clin. Lab. Sci. 2018, 48, 594–600. [Google Scholar]
- Mehrabadi, M.E.; Salemi, Z.; Babaie, S.; Panahi, M. Effect of Biochanin A on Retina Levels of Vascular Endothelial Growth Factor, Tumor Necrosis Factor-Alpha and Interleukin-1Beta in Rats With Streptozotocin-Induced Diabetes. Can. J. Diab. 2018, 42, 639–644. [Google Scholar] [CrossRef]
- Mahmoud, A.M.; Abd El-Twab, S.M.; Abdel-Reheim, E.S. Consumption of polyphenol-rich Morus alba leaves extract attenuates early diabetic retinopathy: the underlying mechanism. Eur. J. Nutr. 2017, 56, 1671–1684. [Google Scholar] [CrossRef] [PubMed]
- Al-Dosari, D.I.; Ahmed, M.M.; Al-Rejaie, S.S.; Alhomida, A.S.; Ola, M.S. Flavonoid Naringenin Attenuates Oxidative Stress, Apoptosis and Improves Neurotrophic Effects in the Diabetic Rat Retina. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Mei, X.; Ouyang, H.; Lu, B.; Yu, Z.; Wang, Z.; Ji, L. Natural flavonoid galangin alleviates microglia-trigged blood-retinal barrier dysfunction during the development of diabetic retinopathy. J. Nutr. Biochem. 2019, 65, 1–14. [Google Scholar] [CrossRef]
- Huang, W.; Yan, Z.; Li, D.; Ma, Y.; Zhou, J.; Sui, Z. Antioxidant and Anti-Inflammatory Effects of Blueberry Anthocyanins on High Glucose-Induced Human Retinal Capillary Endothelial Cells. Oxid. Med. Cel. Long. 2018, 2018, 1862462. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, B.; Palanisamy, U.D.; Chua, K.H.; Kuppusamy, U.R. Protective effect of myricetin derivatives from Syzygium malaccense against hydrogen peroxide-induced stress in ARPE-19 cells. Mol. Vis. 2019, 25, 47–59. [Google Scholar] [PubMed]
- Lv, P.; Yu, J.; Xu, X.; Lu, T.; Xu, F. Eriodictyol inhibits high glucose-induced oxidative stress and inflammation in retinal ganglial cells. J. Cell. Biochem. 2019, 120, 5644–5651. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Jiang, S.; Chu, C.; Xin, M.; Song, X.; Zhao, B. Baicalin protects human retinal pigment epithelial cell lines against high glucose-induced cell injury by up-regulation of microRNA-145. Exp. Mol. Pathol. 2019, 106, 123–130. [Google Scholar] [CrossRef]
- Kang, M.K.; Lee, E.J.; Kim, Y.H.; Kim, D.Y.; Oh, H.; Kim, S.I.; Kang, Y.H. Chrysin Ameliorates Malfunction of Retinoid Visual Cycle through Blocking Activation of AGE-RAGE-ER Stress in Glucose-Stimulated Retinal Pigment Epithelial Cells and Diabetic Eyes. Nutrients 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Pop-Busui, R.; Boulton, A.J.; Feldman, E.L.; Bril, V.; Freeman, R.; Malik, R.A.; Sosenko, J.M.; Ziegler, D. Diabetic Neuropathy: A Position Statement by the American Diabetes Association. Diabetes Care 2017, 40, 136–154. [Google Scholar] [CrossRef] [Green Version]
- Vincent, A.M.; Brownlee, M.; Russell, J.W. Oxidative stress and programmed cell death in diabetic neuropathy. Ann. N. Y. Acad.Sci. 2002, 959, 368–383. [Google Scholar] [CrossRef]
- Schmidt, R.E. Neuropathology and pathogenesis of diabetic autonomic neuropathy. Int. Rev. Neurobiol. 2002, 50, 257–292. [Google Scholar] [CrossRef] [PubMed]
- Addepalli, V.; Suryavanshi, S.V. Catechin attenuates diabetic autonomic neuropathy in streptozotocin induced diabetic rats. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 108, 1517–1523. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Liu, W.; Yi, H.; Hu, X.; Peng, L.; Yang, F. The Natural Rotenoid Deguelin Ameliorates Diabetic Neuropathy by Decreasing Oxidative Stress and Plasma Glucose Levels in Rats via the Nrf2 Signalling Pathway. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2018, 48, 1164–1176. [Google Scholar] [CrossRef] [PubMed]
- Balaha, M.; Kandeel, S.; Kabel, A. Phloretin either alone or in combination with duloxetine alleviates the STZ-induced diabetic neuropathy in rats. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 101, 821–832. [Google Scholar] [CrossRef]
- Ferreira, P.E.B.; Beraldi, E.J.; Borges, S.C.; Natali, M.R.M.; Buttow, N.C. Resveratrol promotes neuroprotection and attenuates oxidative and nitrosative stress in the small intestine in diabetic rats. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 105, 724–733. [Google Scholar] [CrossRef]
- Chis, I.C.; Clichici, A.; Nagy, A.L.; Oros, A.; Catoi, C.; Clichici, S. Quercetin in association with moderate exercise training attenuates injuries induced by experimental diabetes in sciatic nerves. J. Physiol. Pharmacol. 2017, 68, 877–886. [Google Scholar]
- Shi, Y.; Liang, X.C.; Zhang, H.; Sun, Q.; Wu, Q.L.; Qu, L. Combination of quercetin, cinnamaldehyde and hirudin protects rat dorsal root ganglion neurons against high glucose-induced injury through Nrf-2/HO-1 activation and NF-kappaB inhibition. Chin. J. Integr. Med. 2017, 23, 663–671. [Google Scholar] [CrossRef]
- Shi, Y.; Liang, X.C.; Zhang, H.; Wu, Q.L.; Qu, L.; Sun, Q. Quercetin protects rat dorsal root ganglion neurons against high glucose-induced injury in vitro through Nrf-2/HO-1 activation and NF-kappaB inhibition. Acta Pharm. Sin. 2013, 34, 1140–1148. [Google Scholar] [CrossRef] [Green Version]
- Xue, B.; Wang, L.; Zhang, Z.; Wang, R.; Xia, X.X.; Han, P.P.; Cao, L.J.; Liu, Y.H.; Sun, L.Q. Puerarin may protect against Schwann cell damage induced by glucose fluctuation. J. Nat. Med. 2017, 71, 472–481. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Wu, J.H.Y. Flavonoids, Dairy Foods, and Cardiovascular and Metabolic Health: A Review of Emerging Biologic Pathways. Circ. Res. 2018, 122, 369–384. [Google Scholar] [CrossRef]
- Bharat, D.; Cavalcanti, R.R.M.; Petersen, C.; Begaye, N.; Cutler, B.R.; Costa, M.M.A.; Ramos, R.; Ferreira, M.R.; Li, Y.; Bharath, L.P.; et al. Blueberry Metabolites Attenuate Lipotoxicity-Induced Endothelial Dysfunction. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wu, Q.H.; Sui, Y.; Wang, Y.; Qiu, X. Rutin protects endothelial dysfunction by disturbing Nox4 and ROS-sensitive NLRP3 inflammasome. Biomed. Pharmacother. Biomed. Pharmacother. 2017, 86, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.W. Liquiritigenin attenuates cardiac injury induced by high fructose-feeding through fibrosis and inflammation suppression. Biomed. Pharmacother. Biomed. Pharmacother. 2017, 86, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.J.; Fan, Y.L.; Liao, H.H.; Liu, Y.; Chen, S.; Ma, Z.G.; Zhang, N.; Yang, Z.; Deng, W.; Tang, Q.Z. Apigenin alleviates STZ-induced diabetic cardiomyopathy. Mol. Cell. Biochem. 2017, 428, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Huang, Y.; Zheng, W.; Yan, J.; Cheng, M.; Zhao, R.; Chen, L.; Hu, C.; Jia, W. Resveratrol reduces intracellular reactive oxygen species levels by inducing autophagy through the AMPK-mTOR pathway. Front. Med. 2018, 12, 697–706. [Google Scholar] [CrossRef]
- Huo, X.; Zhang, T.; Meng, Q.; Li, C.; You, B. Resveratrol Effects on a Diabetic Rat Model with Coronary Heart Disease. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 540–546. [Google Scholar] [CrossRef]
- Kaya, S.T.; Bozdogan, O.; Ozarslan, T.O.; Taskin, E.; Eksioglu, D.; Erim, F.; Firat, T.; Yasar, S. The protection of resveratrol and its combination with glibenclamide, but not berberine on the diabetic hearts against reperfusion-induced arrhythmias: the role of myocardial KATP channel. Arch. Physiol. Biochem. 2019, 125, 114–121. [Google Scholar] [CrossRef]
- Copeland, L.A.; Swendsen, C.S.; Sears, D.M.; MacCarthy, A.A.; McNeal, C.J. Association between triglyceride levels and cardiovascular disease in patients with acute pancreatitis. PLoS ONE 2018, 13, e0179998. [Google Scholar] [CrossRef] [Green Version]
- Mohammed Yusof, N.L.; Zainalabidin, S.; Mohd Fauzi, N.; Budin, S.B. Hibiscus sabdariffa (roselle) polyphenol-rich extract averts cardiac functional and structural abnormalities in type 1 diabetic rats. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2018, 43, 1224–1232. [Google Scholar] [CrossRef]
- Jayachandran, M.; Wu, Z.; Ganesan, K.; Khalid, S.; Chung, S.M.; Xu, B. Isoquercetin upregulates antioxidant genes, suppresses inflammatory cytokines and regulates AMPK pathway in streptozotocin-induced diabetic rats. Chem. Biol. Interact. 2019, 303, 62–69. [Google Scholar] [CrossRef]
- Aloud, A.A.; Chinnadurai, V.; Govindasamy, C.; Alsaif, M.A.; Al-Numair, K.S. Galangin, a dietary flavonoid, ameliorates hyperglycaemia and lipid abnormalities in rats with streptozotocin-induced hyperglycaemia. Pharm. Biol. 2018, 56, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, J.; Zhang, X.; Wang, L.; Hao, T.; Cheng, Y.; Wang, D. Scutellarin Exerts Hypoglycemic and Renal Protective Effects in db/db Mice via the Nrf2/HO-1 Signaling Pathway. Oxid. Med. Cell. Long. 2019, 2019, 1354345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallahzadeh, M.K.; Dormanesh, B.; Sagheb, M.M.; Roozbeh, J.; Vessal, G.; Pakfetrat, M.; Daneshbod, Y.; Kamali-Sarvestani, E.; Lankarani, K.B. Effect of addition of silymarin to renin-angiotensin system inhibitors on proteinuria in type 2 diabetic patients with overt nephropathy: a randomized, double-blind, placebo-controlled trial. Am. J. Kidney Dis. 2012, 60, 896–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, S.A. Silymarin as an adjunct to glibenclamide therapy improves long-term and postprandial glycemic control and body mass index in type 2 diabetes. J. Med. Food 2007, 10, 543–547. [Google Scholar] [CrossRef]
- Huseini, H.F.; Larijani, B.; Heshmat, R.; Fakhrzadeh, H.; Radjabipour, B.; Toliat, T.; Raza, M. The efficacy of Silybum marianum (L.) Gaertn. (silymarin) in the treatment of type II diabetes: a randomized, double-blind, placebo-controlled, clinical trial. Phytother. Res. PTR 2006, 20, 1036–1039. [Google Scholar] [CrossRef]
- Borges, C.M.; Papadimitriou, A.; Duarte, D.A.; Lopes de Faria, J.M.; Lopes de Faria, J.B. The use of green tea polyphenols for treating residual albuminuria in diabetic nephropathy: A double-blind randomised clinical trial. Sci. Rep. 2016, 6, 28282. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, S.R.; Tappenden, K.A.; Carson, L.; Jones, R.; Prabhudesai, M.; Marshall, W.P.; Erdman, J.W., Jr. Isolated soy protein consumption reduces urinary albumin excretion and improves the serum lipid profile in men with type 2 diabetes mellitus and nephropathy. J. Nutr. 2004, 134, 1874–1880. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Xu, W.; Zhou, Z.; Liu, J.; Li, X.; Chen, L.; Weng, J.; Yu, Z. Curcumin attenuates urinary excretion of albumin in type II diabetic patients with enhancing nuclear factor erythroid-derived 2-like 2 (Nrf2) system and repressing inflammatory signaling efficacies. Exp. Clin. Endocrinol. Diabetes 2015, 123, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Sattarinezhad, A.; Roozbeh, J.; Shirazi Yeganeh, B.; Omrani, G.R.; Shams, M. Resveratrol reduces albuminuria in diabetic nephropathy: A randomized double-blind placebo-controlled clinical trial. Diabetes Metab. 2019, 45, 53–59. [Google Scholar] [CrossRef]
- Liu, X.; Yao, L.; Sun, D.; Zhu, X.; Liu, Q.; Xu, T.; Wang, L. Effect of breviscapine injection on clinical parameters in diabetic nephropathy: A meta-analysis of randomized controlled trials. Exp. Ther. Med. 2016, 12, 1383–1397. [Google Scholar] [CrossRef] [Green Version]
- Steigerwalt, R.; Belcaro, G.; Cesarone, M.R.; Di Renzo, A.; Grossi, M.G.; Ricci, A.; Dugall, M.; Cacchio, M.; Schonlau, F. Pycnogenol improves microcirculation, retinal edema, and visual acuity in early diabetic retinopathy. J. Ocul. Pharmacol. Ther. 2009, 25, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Forte, R.; Cennamo, G.; Bonavolonta, P.; Pascotto, A.; de Crecchio, G.; Cennamo, G. Long-term follow-up of oral administration of flavonoids, Centella asiatica and Melilotus, for diabetic cystoid macular edema without macular thickening. J. Ocul. Pharmacol. Ther. 2013, 29, 733–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, S.E.; Loprinzi, P.D. Influence of flavonoid-rich fruit and vegetable intake on diabetic retinopathy and diabetes-related biomarkers. J. Diabetes Complic. 2014, 28, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Domanico, D.; Fragiotta, S.; Cutini, A.; Carnevale, C.; Zompatori, L.; Vingolo, E.M. Circulating levels of reactive oxygen species in patients with nonproliferative diabetic retinopathy and the influence of antioxidant supplementation: 6-month follow-up. Indian J. Ophthalmol. 2015, 63, 9–14. [Google Scholar] [CrossRef]
- Zhang, H.W.; Zhang, H.; Grant, S.J.; Wan, X.; Li, G. Single herbal medicine for diabetic retinopathy. Cochrane Database Syst. Rev. 2018, 12, CD007939. [Google Scholar] [CrossRef]
- Valensi, P.; Le Devehat, C.; Richard, J.L.; Farez, C.; Khodabandehlou, T.; Rosenbloom, R.A.; LeFante, C. A multicenter, double-blind, safety study of QR-333 for the treatment of symptomatic diabetic peripheral neuropathy. A preliminary report. J. Diabetes Complic. 2005, 19, 247–253. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, X.; Zhang, B. Efficacy and safety of puerarin injection in treatment of diabetic peripheral neuropathy: a systematic review and meta-analysis of randomized controlled trials. J. Trad. Chin. Med. Chung i tsa chih ying wen pan 2014, 34, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Zheng, C.; Ou, W.; Shen, H.; Zhou, Z.; Wang, J. Combined therapy of diabetic peripheral neuropathy with breviscapine and mecobalamin: a systematic review and a meta-analysis of Chinese studies. BioMed Res. Int. 2015, 2015, 680756. [Google Scholar] [CrossRef]
- Grassi, D.; Necozione, S.; Lippi, C.; Croce, G.; Valeri, L.; Pasqualetti, P.; Desideri, G.; Blumberg, J.B.; Ferri, C. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension 2005, 46, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Taubert, D.; Roesen, R.; Lehmann, C.; Jung, N.; Schomig, E. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide: a randomized controlled trial. JAMA 2007, 298, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Ried, K.; Fakler, P.; Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst. Rev. 2017, 4, CD008893. [Google Scholar] [CrossRef] [PubMed]
- Curtis, P.J.; Sampson, M.; Potter, J.; Dhatariya, K.; Kroon, P.A.; Cassidy, A. Chronic ingestion of flavan-3-ols and isoflavones improves insulin sensitivity and lipoprotein status and attenuates estimated 10-year CVD risk in medicated postmenopausal women with type 2 diabetes: a 1-year, double-blind, randomized, controlled trial. Diabetes Care 2012, 35, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, P.J.; Potter, J.; Kroon, P.A.; Wilson, P.; Dhatariya, K.; Sampson, M.; Cassidy, A. Vascular function and atherosclerosis progression after 1 y of flavonoid intake in statin-treated postmenopausal women with type 2 diabetes: a double-blind randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 936–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The FLAVO Trial: Dietary Flavonoids and Cardiovascular Disease Risk Reduction in Postmenopausal Women With Type 2 Diabetes (FLAVO); Identifier: NCT00677599. Available online: https://clinicaltrials.gov/ct2/show/NCT00677599 (accessed on 23 December 2019).
- Homayouni, F.; Haidari, F.; Hedayati, M.; Zakerkish, M.; Ahmadi, K. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phytother. Res. PTR 2018, 32, 1073–1079. [Google Scholar] [CrossRef]
- Vitale, M.; Vaccaro, O.; Masulli, M.; Bonora, E.; Del Prato, S.; Giorda, C.B.; Nicolucci, A.; Squatrito, S.; Auciello, S.; Babini, A.C.; et al. Polyphenol intake and cardiovascular risk factors in a population with type 2 diabetes: The TOSCA.IT study. Clin. Nutr. 2017, 36, 1686–1692. [Google Scholar] [CrossRef]
- Green Tea Extract on Soluble RAGE in Patients With Diabetic Nephropathy. 2019. Identifier: NCT03622762. Available online: https://clinicaltrials.gov/ct2/show/NCT03622762 (accessed on 23 December 2019).
- Inflammation and Stem Cells in Diabetic and Chronic Kidney Disease. 2019. Identifier: NCT03325322. Available online: https://clinicaltrials.gov/ct2/show/NCT03325322 (accessed on 23 December 2019).
- Evaluate the Efficacy and Safety of WH-1 Ointment for the Treatment of Chronic Diabetic Foot Ulcers (WH-1). 2019. Identifier: NCT01898923. Available online: https://clinicaltrials.gov/ct2/show/NCT01898923 (accessed on 23 December 2019).
- Metabolic Benefits of Drinking Blueberry Tea in Type 2 Diabetes. 2019. Identifier: NCT02629952. Available online: https://clinicaltrials.gov/ct2/show/NCT02629952 (accessed on 23 December 2019).
- Effects of Mediterranean Diet Intervention in Diabetic Heart Disease. Identifier: NCT03757845. Available online: https://clinicaltrials.gov/ct2/show/NCT03757845 (accessed on 23 December 2019).
- Nanshan Elderly Cohort Study (NECS). 2019; Identifier: NCT03569735. Available online: ClinicalTrials.gov (accessed on 23 December 2019).
- Guangzhou Nutrition and Health Study (GNHS) (GNHS). 2019; Identifier: NCT03179657. Available online: https://clinicaltrials.gov/ct2/show/NCT03179657 (accessed on 23 December 2019).
- Galati, G.; O’Brien, P.J. Potential toxicity of flavonoids and other dietary phenolics: significance for their chemopreventive and anticancer properties. Free Radic. Biol. Med. 2004, 37, 287–303. [Google Scholar] [CrossRef]
- Bugel, S.M.; Bonventre, J.A.; Tanguay, R.L. Comparative Developmental Toxicity of Flavonoids Using an Integrative Zebrafish System. Toxicol Sci. 2016, 154, 55–68. [Google Scholar] [CrossRef] [Green Version]
- Aiello, P.; Consalvi, S.; Poce, G.; Raguzzini, A.; Toti, E.; Palmery, M.; Biava, M.; Bernardi, M.; Kamal, M.A.; Perry, G.; et al. Dietary flavonoids: Nano delivery and nanoparticles for cancer therapy. Semin Cancer Biol. 2019. [Google Scholar] [CrossRef]
- Bunkar, N.; Shandilya, R.; Bhargava, A.; Samarth, R.M.; Tiwari, R.; Mishra, D.K.; Srivastava, R.K.; Sharma, R.S.; Lohiya, N.K.; Mishra, P.K. Nano-engineered flavonoids for cancer protection. Front. Biosci (Landmark Ed.) 2019, 24, 1097–1157. [Google Scholar]
- Hussain, T.; Tan, B.; Murtaza, G.; Liu, G.; Rahu, N.; Saleem Kalhoro, M.; Hussain Kalhoro, D.; Adebowale, T.O.; Usman Mazhar, M.; Rehman, Z.U.; et al. Flavonoids and type 2 diabetes: Evidence of efficacy in clinical and animal studies and delivery strategies to enhance their therapeutic efficacy. Pharmacol. Res. 2020, 152, 104629. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| In vivo Studies | |||||||
| Disease | Animal | DM | Model | Treatment | Results | Effect | PMID |
| Diabetic Nephropathy | Rat | T1D | STZ | Hesperidin 100 mg/kg/day 2 weeks | ↓FGF-23; ↑α-Klotho | Anti-toxic in liver/kidney | 30551370 |
| Rat | T1D | Alloxan | Ramipril 5 mg/kg + Rutin 50 mg/kg/day 6 weeks | Prevented podocyte injury, ↓TGF-β ↓ GRP78 and CHOP (ER stress markers) | Anti-oxidant and anti-fibrotic | 30372836 | |
| Rat | T1D | STZ | Resveratrol 5 mg/kg/day 45/90 days | ↓Renal hypertrophy and structural changes. ↓AGEs accumulation; ↓oxidative stress | Renoprotective, anti-fibrotic and anti-oxidant | 29229234 | |
| Rat | T1D | STZ | Naringin 20–80 mg/kg/day 12 weeks | ↓ROS: ↑SOD and ↓NOX4 | Renoprotective and anti-oxidant | 28395989 | |
| Rat | T2D | HFD/STZ | Pyrrosiae folium 50–200 mg/kg/day 12 weeks | ↓ renal IL-6, TNF-α and IL-1β | Renoprotective and anti-inflammatory | 29945390 | |
| Rat | T2D | HFD/STZ | Formononetin 10–40 mg/kg/day. 16 weeks | ↑ creatinine clearance; ↑SIRT1; ↑SOD; ↑catalase | Renoprotective, anti-diabetic and anti-oxidant | 30641085 | |
| Mouse | T1D | STZ | Diosmetin 25–100 mg/kg/day 8 weeks | Reduced serum FBG, BUN and creatinine and albuminuria.↓ Akt and NF-κB expression. ↑ iNOS | Renoprotective, anti-diabetic, anti-inflammatory and anti-oxidant | 30278036 | |
| Mouse | T2D | db/db mouse | Chrysin 10 mg/kg/day 10 weeks | ↓ Collagen fiber accumulation ↓ AGEs accumulation | Anti-fibrotic | 29987200 | |
| Diabetic Retinopathy | Rat | T1D | STZ | Catechin 50–200 mg/kg/day 8 weeks | Modulation NF-κB pathway ↓ IL-1β, IL-6, and TNF-α | Anti-inflammatory | 30373863 |
| Rat | T1D | STZ | Biochanin A 10–15 mg/kg/day. 6 weeks | ↓ TNFα, IL-1β and VEGF | Anti-inflammatory and anti-angiogenic | 30054234 | |
| Rat | T1D | STZ | Trans-Resveratrol 5 mg/kg/day. 2–4 weeks | ↑ Cyp26b1 and Cyp3a9 transcription levels | Anti-oxidant | 30030988 | |
| Rat | T1D | STZ | Morus alba extract 100 mg/kg/day 16 weeks | ↓ Caspase-3, Bax and ↑ Bcl2; ↓TNF-α and IL-1β; ↑CAT, SOD and GPx. ↓VEGF | Anti-apoptotic, anti-oxidant, anti-inflammatory and anti-angiogenic | 27059477 | |
| Rat | T1D | STZ | Naringenin 50 mg/kg/day 5 weeks | ↑GSH; ↓Caspase-3, Bax and ↑ Bcl2; ↓pro-BDNF and ↑BDNF | Neuroprotective, anti-oxidant and anti-apoptotic | 29064407 | |
| Mouse | T1D | STZ | Galangin 10 mg/kg/day 30 days | ↑Occludin and claudin1; ↓Iba-1 ↓ TNFα, IL-1β and IL-6 ↓p65, IκB and IKK phosphorylation | Neuroprotective and anti-inflammatory | 30597356 | |
| Mouse | T2D | db/db mouse | Chrysin 10 mg/kg/day 10 weeks | Increasing retinoid binding proteins (RPE65, LRAT, RDH5, and rhodopsin) | Anti-oxidant | 30096827 | |
| Diabetic Neuropathy | Rat | T1D | STZ | Catechin 25/50 mg/kg/day 4 weeks | ↑SOD and CAT ↓MDA and lymphocyte infiltration | Neuroprotective and antioxidant | 30372853 |
| Rat | T1D | STZ | Deguelin 4–8 mg/kg/day 2 weeks | ↑Nrf2; ↓ caspase-3 in neurons ↑ (Na+-K+) ATPase activity | Neuroprotective, anti-oxidant and anti-inflammatory | 30045011 | |
| Rat | T1D | STZ | Resveratrol 10 mg/kg/day 120 days | ↑ SOD and GSH; ↓ nitrosative stress and MPO | Anti-oxidant and anti-inflammatory effect | 29906751 | |
| Rat | T1D | STZ | Phloretin 25–50 mg/kg/day 4 weeks | ↑ SOD and GSH ↓ IL-6 and TNF-α; ↓ MDA | Neuroprotective, anti-oxidant and anti-inflammatory | 29635891 | |
| Cardiovascular complications | Rat | T2D | HGI | Rutin 25–50 mg/kg/day 12 weeks | ↓ inflammasome pathway in aortic tissue; ↓ROS generation | Anti-inflammatory and anti-oxidant | 27936392 |
| Rat | T2D | HFD/STZ | Resveratrol 10 mg/kg/day 8 weeks | ↓ TLR4/MyD88/NF-κB signaling pathway. | Cardioprotective and anti-inflammatory | 30658350 | |
| Rat | T1D | STZ | Apigenin 100 mg/kg/day 7 months | ↓ cardiomyocyte enlargement; ↑SOD and GPx ↓ NF-κB/p65 signaling pathway activation ↓ Col-I, Col-III, CTGF, TGFβ | Cardioprotective, anti-oxidant, anti-inflammatory and anti-fibrotic | 28176247 | |
| Rat | T1D | STZ + IRIA | Resveratrol 5 mg/kg/day + Glibenclamide 5 mg/kg/day 6 weeks | ↑ Kir6.2 expression (subunit of KATP channel) | Anti-arrhythmic | 28176247 | |
| Rat | T1D | STZ | Heracleum Persicum 100 mg/kg/day; 8 weeks | ↓MDA; ↑GSH, CAT and SOD | Anti-oxidant | 29726706 | |
| Rat | T1D | STZ | Isoquecertin 40 mg/kg/day 45 days | ↓ TG, PPL and FFA | Anti-hyperlipidemic | 30817903 | |
| Rat | T1D | STZ | Galangin 40 mg/kg 45 days | ↓ TG, PPL, total cholesterol and FFA | Anti-hyperlipidemic | 29952676 | |
| Mouse | T2D | db/db mouse | Scutellarin 25–100 mg/kg 8 weeks | ↑ high-density lipoprotein cholesterol ↓ TG and cholesterol | Anti-hyperlipidemic | 30881587 | |
| Mouse | T2D | HFI | Liquiritigenin 4–16 mg/kg/day | ↓NF-κB signaling pathway ↓α-SMA, Col-I, Col-II, TGF-β1 | Anti- inflammatory and anti-fibrotic | 28039849 | |
| Mouse | T2D | HFI | Liquiritin 10/20 mg/kg/day | ↓α-SMA, Col I and Col II | Anti-fibrotic | 27810791 | |
| In vitro Studies | |||||||
| Disease | Cell type | Stimulus | Treatment | Results | Effect | PMID | |
| Diabetic Nephropathy | Human embryonic kidney cells | HG | Combretum micranthum 10–25 µg/mL | Hydrogen peroxide and nitric oxide scavenging activity | Anti-oxidant | 30976670 | |
| Rat mesangial cells | HG | Marein 100–400 µM | Regulating AMPK, TGF-β1/Smads pathway ↓ NF-κB signaling pathway | Anti-inflammatory and anti-fibrotic | 30630477 | ||
| Rat/human renal tubular epithelial cells | HG | Kaempferol 5–50 μM | ↓ RhoA/Rho Kinase signaling | Anti-inflammatory, anti-oxidant and anti-fibrotic | 30551415 | ||
| Mesangial cells | HG | Corn silkextract 200 µg/mL | ↓ α-glucosidase and α-amylase, IL-6, AGEs, Col IV and fibronectin | Anti-inflammatory, anti-oxidant and anti-fibrotic | 30530231 | ||
| Rat mesangial cells | AGEs | Kaempferitrin 10–35 µM | ↑SOD activity ↓MDA, Col IV and TGF-β1 | Anti-oxidant and anti-fibrotic | 30373106 | ||
| Rat mesangial cells | HG | Liquiritigenin 20–40 µM | ↓ NOX4 and ↑SOD Decrease collagen IV fibronectin, Il-6 and IL-1β | Anti-oxidant, anti-inflammatory and anti-fibrotic | 30119269 | ||
| Human proximal tubular epithelial cells | HG | Astilbin 10–20 µM | Modulating PI3K/Akt pathway | Anti-proliferative | 30119185 | ||
| Mouse podocyte cell line | HG | Genistein 20 µM | Inactivating mTOR signaling | Autophagia | 29999001 | ||
| Human mesangial cells | HG | Chrysin 1–20 µM | ↓ Collagens, α-SMA, fibroblast-specific protein-1, MMPs | Anti-fibrotic | 29987200 | ||
| Rat mesangial cells | HG | Naringin 5–80 μmol/L | Modulating NLRP3 signaling pathway ↓IL-1β, IL-18 and caspase-1 | Anti-inflammatory and anti-apoptotic | 29929501 | ||
| Rat mesangial cells | AGEs | Kaempferitrin 10–35 μM | ↓MDA levels; ↑SOD and ROS generation. ↓ Collagen IV and TGF-β1 | Anti-oxidant and anti-fibrotic | 30373106 | ||
| Human mesangial cells | AGEs | Chrysin 1–20 µM | ↓ Collagens, α-SMA, fibroblast-specific protein-1, MMPs | Anti-fibrotic | 29987200 | ||
| Diabetic Retinopathy | Human retinal pigment epithelial cell line | Glucose oxidase | Myricetin 40 μg/mL | Activation of Nrf2 ↑ SOD ↓ NOS2 | Anti-oxidant | 30820141 | |
| Human retinal pigment epithelial/endothelial cells | HG | Baicalin 2.5–100 μM | Inhibition of NF-κB and p38 MAPK pathways | Anti-apoptotic and anti-inflammatory | 30625293 | ||
| Human retinal pigment epithelial cell line | H2O2 | Kaempferol 20–100 nM | Modulation Bax/Bcl-2/caspase-3 pathway; ↑ SOD and ↓VEGF | Anti-apoptotic, anti-oxidant, and anti-angiogenic | 30584457 | ||
| Human retinal pigment epithelium cells | HG | Chrysin 1–20 µM | ↓VEGF and PDGF, AGEs and ER stress | Anti-angiogenic | 30096827 | ||
| Human retinal capillary endothelial cells | HG | Blueberry Anthocyanin 10 μg/mL | ↑CAT, SOD, ↓ Nox4 and eNOS levels ↓ICAM-1 and NF-κB; ↓VEGF | Anti-oxidant, anti-inflammatory and anti-angiogenic | 29682153 | ||
| Rat retinal ganglial cells | HG | Eriodictyol 5–20 μM | ↓ROS and ↑ SOD, GPx, catalase ↓ TNFα, IL-8 | Anti-oxidant and anti-inflammatory | 30317656 | ||
| Mice microglia retinal cells | HG | Galangin 20/50 µM | ↓IL-1β, TNFα;↓ NF-κB activation | Anti-inflammatory | 30597356 | ||
| Diabetic Neuropathy | Rat dorsal root ganglion neurons | HG | Quercetin 10 mmol/L + other flavonoids | ↑ Nrf-2/HO-1 pathway; scavenging ROS ↓NF-κB activation | Anti-oxidant and anti-inflammatory | 28861887 | |
| Schwann cells | HG | Puerarin 10 µmol/L | ↓Caspase-3; ↓ROS production and mitochondria depolarization | Anti-apoptotic and anti-oxidant | 28181078 | ||
| Rat dorsal root ganglion neurons | HG | Quercetin 2.5–10 mmol/L | ↑ Nrf-2/HO-1; ↓ NF-κB inhibition | Anti-oxidant and anti-inflammatory | 23770986 | ||
| Cardiovascular complications | Human aortic endothelial cells | Palmitic acid | Blueberry Anthocyanins 12–16 nmol | ↓Nox-mediated ROS production | Anti-oxidant | 29024402 | |
| Human umbilical vein endothelial cells | HG | Rutin 30–100 µM | ↓Nox2 and Nox4 | Anti-oxidant | 27936392 | ||
| Human aortic endothelial cells | Palmitic acid | Resveratrol 50–100 µM | ↓ ROS production via AMPK-mTOR pathway | Autophagia and anti-oxidant | 30421395 | ||
| Objective to Study | Treatment | Duration | Results | PMID | |
|---|---|---|---|---|---|
| Diabetic Nephropathy | Renoprotective effect of milk thistle extract on T2D patients with macroalbuminuria. | n = 30; 3 × 140 mg silymarin n = 30; Placebo | 3 months | Significant decrease in UACR levels, urinary TNF-α and urinary and serum MDA in the silymarin group. | 22770926 NCT01003236 |
| Effect of silymarin on glycemic control and body mass index in T2D patients with insulin resistance and poor glycemic control with oral hypoglycemic agents | n = 18; 200 mg silymarin + 10 mg Glibenclamide n = 21; Placebo + 10mg Glibenclamide | 4 months | Silymarin treatment significantly reduced fasting and postprandial plasma glucose, HbA1c levels and body mass index. | 17887949 | |
| Effects silymarin administration on the glycemic state in T2D patients. | n = 25; 3 × 200 mg silymarin n = 26; Placebo | 4 months | Decreased significantly FBG, HbA1c, total cholesterol, LDL, triglyceride, GOT and GPT after treatment with silymarin. | 17072885 | |
| Safety and effect of green tea (epigallocatechin gallate, EGCG) in patients with DN. | n = 24; ACEi/ARBs + 800 mg EGCG n = 23; ACEi/ARBs + Placebo | 3 months | Treatment with green tea extract reduced UACR by 41%. | 27320846 NCT01923597 | |
| Effects of isolated soy protein consumption on urinary albumin excretion and blood lipid profile in early stages of DN. | n = 14; 0.5 g/kg/day of the dietary protein was provided as either isolated soy protein | 2 × 8 weeks | Soy protein consumption reduced UACR levels by 9,55%. | 15284369 | |
| Efficacy of curcumin for blocking DN development in T2D patients (short time). | n = 14; 500 mg curcumin | 1 month | Curcumin attenuated microalbuminuria and reduced plasma MDA and LPS levels content. Maintaining gut barrier integrity and function. | 25875220 | |
| Diabetic Retinopathy | Effects of pycnogenol in early stages of DR. | n = 24; 150 mg pycnogenol n = 22; Placebo | 2 months | Visual improvement was subjectively perceived by 18 of 24 patients in the pycnogenol group. Significant improvement visual acuity from baseline. | 19916788 |
| Evaluate long-term follow-up of the orally administered combination of flavonoids for treatment of diabetic cystoid macular edema without macular thickening. | n = 35; 300 mg Diosmin, 15 mg C. asiatica 160 mg Melilotus n = 35; Placebo | 3 years | Retinal sensitivity reduced in control group only from month 6 until month 36. In the treatment group, a greater retinal sensitivity was present at month 12, 24, and 36. | 23844756 | |
| Determine the relationship between dietary flavonoid-rich fruit and vegetable consumption on DM-related biomarkers and DR. | Data from 381 participants with DM from the NHANES 2003–2006. | - | Greater high-flavonoid fruit and vegetable consumption was associated with lower levels of CRP, HbA1c and glucose, with reducing the odds of having diabetic retinopathy by 30%. | 25055729 | |
| Efficacy of anti-oxidant dietary supplementation reducing the ROS levels in patients with non-proliferative DR. | n = 34; 50 mg pycnogenol, 30 mg Vit. E, 20 mg CoQ n = 34; Placebo | 6 M | In the group receiving antioxidant therapy the levels of free oxygen radicals and retinal thickness were significantly reduced over three times. Conversely, in the control group a significant increase was observed. | 25686055 | |
| Diabetic Neuropathy | Efficacy and safety of QR-333 (quercetin, ascorbyl palmitate and vitamin D3) in the treatment of diabetic neuropathy. | n = 23; three topical applications QR-333 n = 11; Placebo | 1 M | QR-333 produced significant relief of some symptoms of diabetic neuropathy and was safe and well tolerated. | 16112498 NCT16112498 |
| Cardiovascular complications | Effect of flavanol-rich chocolate in patients with hypertension. | n = 20; Cross-over 100 mg Dark Chocolate (88 mg flavanols) 90 mg flavanol-free White Chocolate | 15 d per treatment | Dark chocolate decreased blood pressure and serum LDL cholesterol, improved FMD, and ameliorated insulin sensitivity in hypertensive patients. | 16027246 |
| Evaluate whether regular ingestion of an unsweetened, strongly defatted and flavanol-rich cocoa powder might improve BP and glucose and lipid metabolism in stably treated T2D subjects. | n = 17; Five × 0.5 g cocoa powder capsules n = 18; Placebo | 3 M | Daily intake of 2.5 g of flavanol-rich, unsweetened and strongly defatted cocoa powder does not affect BP, glucose and lipid metabolism in stably-treated patients with T2D and hypertension in a fasting state. | 30301127 | |
| Effect of dietary flavonoids on CVD risk in postmenopausal women with T2D on established statin and hypoglycemic therapy. | n = 59; 27 g flavonoid-enriched chocolate n= 59; Placebo | 12 M | Improvement in insulin sensitivity was observed. Reductions in total cholesterol, HDL-cholesterol ratio and LDL cholesterol. Estimated 10 year total coronary heart disease risk was attenuated after flavonoid intervention. | 22250063 NCT00677599 | |
| Effect of combined isoflavone and flavan-3-ol intake on vascular function in postmenopausal women with T2D. | The flavonoid intervention did not significantly change the intima-media thickness of the common carotid artery, augmentation index, or BP, but pulse pressure variability improved. | ||||
| Effect of oral Hesperidin supplementation in hemodynamic changes in T2D patients. | n = 32; 500 mg Hesperidin n = 32; Placebo | 1.5 M | Significant difference in mean percent change of SBP, diastolic blood pressure, mean arterial BP, serum TAC, and inflammatory markers between Hesperidin and control groups. | 29468764 | |
| Association between the intake of total polyphenols and polyphenol classes with the major CV risk factors in a T2D population. TOSCA.IT study. | n = 2573 people with T2D | 10 years | A diet characterized by a higher intake of total polyphenols was associated with a better cardiovascular risk factors profile and a lower grade of subclinical inflammation. | 27890487 NCT00700856 |
| Title | Design | Objective | Patients | Treatment | Duration |
|---|---|---|---|---|---|
| Green tea extract on Soluble RAGE in Patients with DN (NCT03622762) | Double blind, randomized and placebo controlled | Evaluate effect of administration of green tea extract on soluble RAGE and renal damage in patients with T2D. | 30 patients | Twice daily: 400 mg green tea extract vs. 400 mg placebo | 3 months |
| Inflammation and Stem Cells in Diabetic and CKD (NCT03325322) | Randomized, parallel | Study the efficacy of fisetin on stem/stromal cell function, kidney function, inflammation and physical activity in advanced CKD patients. | 30 patients | Fisetin 20 mg/kg/day, orally for 2 consecutive days vs. placebo | 1 year |
| Randomized controlled study to evaluate the efficacy and safety of WH-1 ointment for the treatment of chronic diabetic foot ulcers (NCT01898923) | Randomized, evaluator blinded, active-controlled, multicentric | Evaluate efficacy and safety of WH-1 ointment compared to Aquacel hydrofiber dressing. | 236 patients | WH-1 ointment (1,25%) twice daily for up to 16 weeks vs. Aquacel hydrofiber dressings changed daily, on alternate days or three times a week | 4 months |
| Metabolic Benefits of Drinking Blueberry Tea in T2D (NCT02629952) | Open, randomized, crossover assigned. | Determine whether chronic consumption of blueberry tea improve metabolic and vascular health in people with and without T2D. | 36 patients | Three cups of blueberry tea per day vs. non treatment | 1 month |
| Effects of Mediterranean Diet Intervention in Diabetic Heart Disease (NCT03757845) | Randomized, parallel, double-blind | Examine short-term effects of modified Mediterranean diet on lipogenic signaling pathway in T2D patients. | 48 patients | Mediterranean diet vs. control diet | 9 days |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caro-Ordieres, T.; Marín-Royo, G.; Opazo-Ríos, L.; Jiménez-Castilla, L.; Moreno, J.A.; Gómez-Guerrero, C.; Egido, J. The Coming Age of Flavonoids in the Treatment of Diabetic Complications. J. Clin. Med. 2020, 9, 346. https://doi.org/10.3390/jcm9020346
Caro-Ordieres T, Marín-Royo G, Opazo-Ríos L, Jiménez-Castilla L, Moreno JA, Gómez-Guerrero C, Egido J. The Coming Age of Flavonoids in the Treatment of Diabetic Complications. Journal of Clinical Medicine. 2020; 9(2):346. https://doi.org/10.3390/jcm9020346
Chicago/Turabian StyleCaro-Ordieres, Teresa, Gema Marín-Royo, Lucas Opazo-Ríos, Luna Jiménez-Castilla, Juan Antonio Moreno, Carmen Gómez-Guerrero, and Jesús Egido. 2020. "The Coming Age of Flavonoids in the Treatment of Diabetic Complications" Journal of Clinical Medicine 9, no. 2: 346. https://doi.org/10.3390/jcm9020346